
GUIDELINES FOR DIAGNOSIS, TREATMENT AND … · Guidelines for diagnosis, treatment and prevention...
82
Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia 2012 Somali Federal Government Ministry of Health
Transcript of GUIDELINES FOR DIAGNOSIS, TREATMENT AND … · Guidelines for diagnosis, treatment and prevention...

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
2012
Somali Federal Government Ministry of Health


Contents
Acronyms ...................................................................................................................... 4
Acknowledgements ............................................................................................................ 5
1. Introduction .............................................................................................................. 7
1.1 Background information ............................................................................................................. 7
1.2 Life-cycle and transmission patterns .......................................................................................... 8
1.3 Human infection and disease ..................................................................................................... 8
2. Diagnosis ................................................................................................................. 9
2.1 Clinical diagnosis ........................................................................................................................ 9
2.2 Laboratorydiagnosis ................................................................................................................. 10
2.3 Diagnosis of primary kala-azar ................................................................................................ 13
2.4 Diagnosis of relapse ................................................................................................................ 15
2.5 Diagnosis of PKDL ................................................................................................................... 15
3. Treatment .............................................................................................................. 15
3.1 Treatment of primary kala-azar (new cases) ........................................................................... 15
3.2 Treatment of relapse of kala-azar ............................................................................................ 18
3.3. Treatment of PKDL .................................................................................................................. 19
3.4 Other treatment related issues and special situations ............................................................ 20
3.5. Treatment of concurrent infection and malnutrition ................................................................. 22
4. Information system ................................................................................................... 32
5. Prevention and control .............................................................................................. 32
6. Annexes ................................................................................................................ 33
Annex 1. rK39 rapid diagnostic test procedure ....................................................................................... 33
Annex 3. Lymph node aspirate procedure ............................................................................. 42
Annex 4. Bone marrow aspiration procedures ........................................................................ 43
Annex 5. Procedures for splenic aspiration ............................................................................ 45
Annex 6. Preparation and examination of aspirates. Grading of parasites ..................................... 47
Annex 7. Kala-azar laboratory register book (left page) ............................................................ 51
Annex 8. Kala-azar treatment register book (left page) ............................................................. 53
Annex 9. Kala-azar patient treatment card (front) .................................................................... 55
Annex 10. Kala-azar patient discharge card ........................................................................... 57
Annex 11. Dosage and precautions for the use of sodium stibogluconate (SSG) ............................ 58
Annex 12. Dosage and precautions for the use of paromomycin (aminosidine). .................................... 60
Annex 13. Dosage, administration and precautions for meglumine antimoniate. .................................... 62
Annex 14. Anthropometry and nutrition therapy look-up tables. .............................................................. 64
Annex 15. Overview of treatment for concurrent illnesses in kala-azar. .................................................. 73
Annex 16. Drug guidelines for kala-azar .................................................................................................. 75
Annex 17. Kala-azar monthly reporting forms.......................................................................................... 76
Annex 18. Kala-azar weekly reporting forms .......................................................................... 81
Annex 19. Kala-azar line listing file (to be sent to central database on regular basis) ....................... 82

Acronyms
DAT Direct agglutination test
FDA Freeze – dried antigen
IM Intramuscular
IV Intravenous
KA Kala-azar
ME Mercapto-ethanol
ORS Oral rehydration salt
PKDL Post kala-azar dermal leishmaniasis
RBC Red blood cells
RDT Rapid diagnostic test
RR Respiratory rate
SSG Sodium stibogluconate
TFC Therapeutic feeding centre
TOC Test of cure
VL Visceral leishmaniasis
WBC White blood cells
WHO World Health Organization

Acknowledgements
The Visceral Leishmaniasis (VL) guideline for Somalia has been updated through a highly participatory process involving officials from the Ministry of Health, Non-governmental Organizations supporting the various endemic kala-azar treatment centres, World Health Organization representatives from Somalia and EMRO, and national partners.
I sincerely appreciate and commend the role of the World Health Organization in supporting the Ministry of Health technically and logistically without which this document would have not been materialized.
I would like to thank health workers in kala-azar treatment facilities and the various INGOs supporting those facilities. I am fully cognizant that without their commitments and continuous daily efforts in diagnosing, treating and monitoring patients, no progress on kala-azar guidelines would have been possible.
A special thank you is extended to Dr Marthe Everard, WR for Somalia, for her support, to Dr José Postigo of WHO EMRO, and Dr Mohamed M Fuje and Godela von Döhren of WHO Somalia for valuable comments, guidance and effective assistance during the guidelines preparation and printing process.
The guidance provided in this document has been drawn from vast experience and lessons learnt from global, regional and local level. We hope the guideline will standardize and unify kala-azar management in the endemic regions and will be able to significantly reduce the high burden of kala-azar in the endemic states.
Mr. Duale Adam Mohamed
Director General
Ministry of Health, TFG Somalia
Mogadishu 23rd
July, 2012.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
7
1. Introduction
1.1 Background information
Leishmaniases are caused by over 20 species of parasitic protozoa of the genus Leishmania. The disease, transmitted to humans by sandflies (Phlebotomus and Lutzomyia species), is endemic in 98 countries or territories, affecting around two million people each year.
Depending on the species of the parasite and the immune response of the host the disease spectrum of leishmaniasis ranges from self-healing skin lesions to a fatal systemic disease called visceral leishmaniasis (VL) which is also known as kala-azar (KA), a Hindi term meaning ‘black fever’.
Human leishmanial infections can result in 3 main forms of disease:
Cutaneous leishmaniasis
Muco-cutaneous leishmaniasis
Visceral leishmaniasis (kala-azar)
Visceral leishmaniasis (kala-azar) is a deadly disease caused by the protozoan Leishmania parasite, transmitted through the bite of Phlebotomus sandflies.
The World Health Organization (WHO) estimates that globally about 500,000 new cases and over 50,000 deaths of kala-azar occur every year, over 90 % of these cases are from six countries: Bangladesh, Brazil, Ethiopia, India, Nepal and the Sudan. In Africa, there are five countries endemic for VL, namely Ethiopia, Kenya, Somalia, Uganda and the Sudan. Kala-azar generally affects poor and neglected populations living in remote rural areas. If not treated more than 95% of kala-azar cases will eventually die.
Eastern Africa is one of the world’s main kala-azar endemic areas, with the majority of the burden being concentrated in focal areas in the east and south-east of Sudan.
In Somalia, kala-azar is caused by Leishmania donovani. Phlebotomus martinii is the predominant vector in Somalia, but also P. vansomerenae was reported as possible vector (Trans R Soc Trop Med Hyg. 2003 Nov–Dec;97(6):667–71) . Man is believed to be the only reservoir and transmission is believed to be anthroponotic.
Anecdotal cases were described as early as 1935, but VL was first officially reported in 1943, with the first outbreak reported in 1952 from Daarbuluk, Hargeisa.
An endemic focus was described in 1965, with 12 cases diagnosed in Middle Shabele region, the majority of which occurred in young age groups and originated from the province capital Jowhar. Further VL cases were reported in 1995‐6 from the Lower Juba region by MSF‐B (Belgian Section) and a case was identified in 1995 in Baidoa, Bay region.
In 2001, an outbreak on the borders of Kenya, Ethiopia and Somalia began, with the majority of cases occurring in ethnic Somalis from nomadic tribes grazing cattle in the border area. Cases first occurred in Lower Juba, Bakool and Gedo regions, although VL in Gedo may have been introduced by the arrival of people displaced from Bakool in 1998.
Cases continued to occur in Bakool, with approximately 140 cases reported annually from 2002 to 2004. A marked increase to 1,002 patients was observed in 2006, 80% of which came from two districts, Hoddur and Tiyeglow, in Bakool region and this outbreak continued up to 2008.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
8
1.2 Life-cycle and transmission patterns
Kala-azar is transmitted to human through the inoculation, during a blood meal, of the promastigotes by an infected female Phlebotomus sandfly. The form of the parasite that infects man is called a promastigote. The promastigotes are injected into the skin of a healthy person through the bite of an infected female sandfly. Following inoculation, the promastigotes are taken up by the phagocytic cells and develop into amastigotes. The amastigotes spread in the blood and multiply in the macrophages of the spleen, liver, bone marrow, lymph nodes, and the mucosa of the small intestines. Intracellular & free forms of amastigotes are ingested by a female sandfly while taking a blood meal. After about 72 hours, the amastigotes become flagellated promastigotes in the mid-gut of the sandfly. The promastigotes continue to multiply and fill up the sandfly gut. Subsequent migration to the mouthparts follows in 4 to 6 days time making promastigotes ready for inoculation when the vector takes the next blood meal (Figure 1).
Different species of sandflies need different habitats to survive and have different biting patterns (in and outdoors, forest or village, day or night preferences). This has important implications for the transmission and possible control measures.
Termite hills and acacia trees are assumed to be breeding and resting sites for P martinae. The sandfly is active throughout the dry season and it bites at night (from dusk to dawn).
Figure 1. Life cycle of the leishmania parasite.
1.3 Human infection and disease
Most individuals infected by Leishmania donovani will not develop the disease (90% of asymptomatic or sub-clinical infections). When the host immune system is not able to suppress the parasite, VL will develop. After an incubation period of 2 to 6 months, sometimes longer, patients will present with fever, anorexia, headache, sometimes with cough, abdominal pain, diarrhoea, vomiting, epistaxis (nose bleeding) and symptoms of anaemia. After several weeks of illness, splenomegally develops and weight loss becomes prominent, sometimes leading to severe malnutrition. If left untreated, the disease leads to death in more than 95% of the cases often from superimposed bacterial infection, severe anaemia or bleeding.
Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
9
2. Diagnosis
2.1 Clinical diagnosis
A patient will be considered as a clinical suspect of VL if she/he presents with a history of prolonged fever (2 weeks or more) associated with clinical splenomegaly or wasting (weight loss).
NO ONE SHOULD BE TESTED FOR KALA-AZAR UNLESS THEY HAVE A FEVER. CHECK THE TEMPERATURE – you may need to check in the afternoon.
EXCEPTION: Occasionally you will clinically diagnose a severely malnourished patient with kala-azar without finding a fever because they are too sick.
As only 50–60 % of patients meeting this clinical case definition have kala-azar, the diagnosis needs to be confirmed serologically or parasitologically. The main differential diagnoses for KA patients are:
Malaria
Hyperactive malarial splenomegaly (HMS): formerly called Tropical Splenomegaly Syndrome (TSS). This condition results from multiple partially treated malaria episodes
Schistosomiasis: the splenomegaly is caused by portal hypertension and the fever is usually caused by another condition (e.g. pneumonia)
Brucellosis: the splenomegaly is usually not massive; hepatomegaly; joint, bone and occasionally neurological involvement
Typhoid fever: high grade fever, bradycardia, duration of illness less than one month, impaired mental status, constipation
Tuberculosis: usually no splenomegaly, but possible in case of milliary tuberculosis; respiratory symptoms are present.
Splenic abscess
Myeloproliferative diseases
Malignancies of lymphoid origin (leukemias and lymphomas)
Chronic haemolytic anaemia
A kala-azar patient can have primary kala-azar, or relapse or PKDL. The definitions for each are as follows:
Primary kala-azar: This refers to a patient who is diagnosed with KA for the first time. The patient had not been treated for KA before.
Relapse: This refers to a patient who has completed full treatment course and then returns with proven kala-azar. If a patient was treated for at least 15 days with appropriate amount of antimonial as single therapy more than one month ago and then returns with proven KA
Case definition of a clinical suspicion of VL
History of prolonged fever (more than 2 weeks)
AND splenomegaly or wasting (weight loss)

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
10
she/he is also considered as a relapse. Relapses are diagnosed parasitologically and are mainly observed within 6 months after treatment.
Post kala-azar dermal leishmaniasis (PKDL): PKDL is a recognized complication, occurring in a very mild form in about 50% of kala-azar cases, and in severe forms in few cases. Usually, skin lesions develop months after the clinical cure of kala-azar, but sometimes PKDL occurs during treatment or even before kala-azar. In most of these cases however a previous infection occurred sub-clinically. In some cases no history of previous KA is known.
The lesions of PKDL start on the face as small scattered hyper-pigmented macules and papules. The rash can become nodular and spread to the trunk and limbs. It is symmetrical and non – itching. A grading system is used to describe the spread of the skin lesions:
Grade 1: Scattered macular, rash on the face around the mouth with some lesions on the upper chest and upper arms.
Grade 2: Dense macular, or nodular rash covering most of the face and extending to the chest, back and upper arms and legs. If extensive or black nodules, it is severe grade 2.
Grade 3: Dense macular, rash, covering most of the body, including hands and feet. In grade 3 crusting ulcers, scaling and spreading to the mucosa of the lips and the palate occurs.
PKDL might persist for years (up to 10 years have been reported). It is speculated that PKDL patients could form a reservoir of the parasite in the community. Bed nets should be given to PKDL patients to prevent transmission.
Majority of PKDL cases are self limiting so treatment is not needed, only severe grade 2 and grade 3 are treated with specific medicines.
PKDL is diagnosed clinically therefore none of the kala-azar laboratory tests (rapid tests, DAT and aspirates) should be done.
2.2 Laboratory diagnosis
Before proceeding to any blood testing for primary visceral leishmaniasis (DAT or rapid diagnostic test) first exclude malaria by doing a blood test and treating if positive, or if no testing is possible simply treat and evaluate after 4 days. If the patient still has a clinical diagnosis of kala-azar do a blood test. A patient who is severely ill can be tested for kala-azar at the same time the person gets treatment for malaria.
If the patient has been treated for kala-azar before with SSG for 15 days or more and is sick again they do NOT need a DAT test. That may have a relapse.
Diagnostic techniques involve serological and parasitological tests:
Serological tests:
Rapid diagnostic test (RDT) (rK39 dipsticks- Inbios® and DiaMed – IT LEISH® also known as Opti-Leish®
Direct agglutination test (DAT)
Parasitological tests:
Lymph node aspirate
Splenic aspirate
Bone marrow aspirate

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
11
Serological tests
Several tests have been developed to detect antibodies against Leishmania in the blood or serum of VL patients. The most common serological tests used in diagnosis of kala-azar are the DAT and the rk39 dipstick tests. These tests indicate the presence of antibodies against Leishmania and so confirming the parasite (antigen) is or was present in the body.
Inbios® and DiaMed – IT LEISH® test are the commonly used and recommended rapid diagnostic tests in a dipstick format. The rapid tests allow diagnostic confirmation of kala-azar at the peripheral health facilities leading to early treatment and better prognosis.
DAT is a robust and well-validated test that requires more material and training. The procedure is a bit complex, thus requires health facilities with a laboratory, cold chain and well trained staff.
Serological tests can only be used for the diagnosis of primary kala-azar (patients with no prior history of kala-azar, the ones who had not been treated for kala-azar before). For patients with a prior history of KA who present with a suspicion of relapse one cannot rely on a serological test for diagnostic confirmation, as specific anti-leishmania antibodies can persist for several years.
Rapid diagnostic (rK39 antigen-based) tests
The rapid diagnostic rK39-based tests (RDT) are easy to perform, quick, cheap and give reproducible results. They can therefore be used for early diagnosis of visceral leishmaniasis at both peripheral and central levels. The RDTs detect specific antibodies against the kinesin-related antigen that is present in Leishmania donovani.
The procedure of the rK39 dipstick is simple with results available within 20–25 minutes (annex 1). They do not require extra-material and results are stable overtime, allowing for quality control.
The rK39 rapid tests are therefore the recommended tests for use in Somalia for confirmation of the diagnosis of kala-azar among clinical suspects with no prior history of the disease.
Direct agglutination test
The DAT can be performed using either blood (dried blood on filter paper) or serum. The DAT antigen is prepared from formalin-killed promastigote stages of L. donovani cultures and stained blue for visibility. The test is semi-quantitative and gives antibody titres ranging from 1:100 up to 1:151200. It is a highly sensitive (>95 %) and specific (>85 %) test when performed according to standardized procedures (annex 2). It requires a well-trained laboratory technician to undertake the process over a period of 2 to 3 days to obtain results. The DAT should be performed in a health facility with a laboratory, cold chain and well trained staff.
Interpretation of Dipstick Results
POSITIVE:
This patient needs admission (if they were never treated before) and treatment.
NEGATIVE:
This patient must await the result of the DAT test. Do not let that person leave.
Treat for all other illnesses while they wait. Give ferrous and folic acid while
waiting.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
12
The DAT cut-off points vary between the types of antigen used either freeze–dried antigen (FDA) or liquid antigen. The freeze–dried antigen is more preferred in the field due to its stability during transportation and is therefore recommended for Somalia. The positive cut-off titre for freeze–dried antigen is 1:3200 (well 7). Other cut-off points for FDA are as follows:
DAT negative (< 1: 400): VL is very unlikely. Alternative diagnoses (e.g. malaria, disseminated tuberculosis, brucellosis, typhoid fever, etc.) should be looked for and treated. If there is no response to treatment for a proven or suspected alternative diagnosis and if clinical suspicion of kala-azar is high (i.e. much enlarged spleen), the tests can be repeated within a month or a parasitological test (lymph node/bone marrow/spleen aspiration) is performed to search for the Leishmania parasites.
If the DAT is positive (≥ 1:3200): Kala-azar is very likely and appropriate treatment should be initiated.
If the DAT is borderline (1: 400, 1:800 and 1:1600), the test should be repeated within one month or alternatively a parasitological test (lymph node/bone marrow/spleen aspiration) should be performed in the absence of contra-indication (s).
Parasitological diagnosis
Visceral leishmaniasis can be confirmed by microscopical examination of stained slides of lymph node, bone marrow, or spleen aspirates (annexes 3–6). Specificity of these tests is near 100% provided that slide staining is done properly and that the laboratory technicians are well trained. Spleen aspirate is more sensitive (96 %) than bone marrow (70 %) or lymph nodes (58%) aspirates. Bone marrow aspirate is a very painful and invasive medical procedure that needs expertise and optimal sterilization of the puncture material. The procedure of lymph node aspiration is also quite painful.
Spleen aspiration should be limited to hospital settings or health facilities where there is adequate equipment and trained staff to manage complications appropriately. Transfusion facilities should be present. Provided that the test is performed properly, the rate of life threatening bleeding after a spleen puncture is very low. The patient must strictly rest in bed for at least eight hours after the procedure and remain under close nursing observation. Spleen aspiration is contra-indicated in the following situations:
Spleen barely or not palpable
Jaundice (a sign of possible liver dysfunction)
Signs of active bleeding (nose, skin, digestive, etc…). A history of recent nose bleeding without active bleeding is not a contra-indication for spleen aspiration
Severe anaemia (Haemoglobin < 5.5 mg/dl)
Pregnancy
Patient in very poor general condition
The clinical indications for parasitological diagnosis (spleen, bone marrow or lymph node
aspiration) are the following:
Clinical suspect with a prior history of kala-azar (suspicion of relapse)
VL patient not responding to anti-Leishmania treatment (test of cure)
Clinical suspect with a borderline DAT result (1:400 – 1:1600)
Clinical suspect with a negative rK39 dipstick or DAT results but with strong clinical
suspicion of kala-azar AND absence of alternative diagnosis or no response to treatment
of alternative diagnosis

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
13
Low blood pressure
Uncooperative patient or caretaker
Lack of informed consent from patient or caretaker
In patients with contra-indication(s) to spleen puncture, bone marrow or lymph node aspirates can be done, provided that enlarged lymph nodes are present. Figure 2 (below) shows the diagnostic algorithm to guide you when to use each of the tests mentioned above and how to interpret the result in terms of treatment decisions. All diagnostic tests must be properly recorded on the laboratory register book (annex 7).
KA testing is done to clinically VL suspect patients since most people infected by Leishmania do not develop the disease (KA). It is crucial to enquire about any previous treatment for KA because serological tests will test positive even several years after a successful treatment.
The first test to be used in a clinically VL suspect never treated before is the RDT and treatment should start when the RDT is positive. In case of a negative RDT result, then blood should be tested for DAT.
If DAT result is positive the patient should be treated. If DAT result is borderline, the test should be repeated not earlier than one week later or to perform a parasitological test. If DAT result is negative another disease has to be considered.
If a person shows a borderline DAT result and the parasitological test is positive the person has to be treated for KA. If the parasitological test is negative then re-test for DAT or search another diagnosis.
In health facilities where either RDTs or DAT is not available the following is recommended:
2.3 Diagnosis of primary kala-azar
RDT not available: Take a blood sample using filter paper to perform DAT either in your health facility or at the referral laboratory.
At the same time you can do a parasitological test. If the parasitological test shows Leishmania parasites then treatment can be started. If parasites are not observed wait for the DAT results.
DAT not available and RDT is negative or not available: Take a blood sample using filter paper to perform DAT at the referral laboratory.
At the same time you can do a parasitological test. If the parasitological test shows Leishmania parasites then treatment can be started. If parasites are not observed wait for the DAT results.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
14
Figure 2. Diagnostic algorithm of primary visceral leishmaniasis (VL) in Somalia
Clinical VL suspect
Rapid diagnostic test
Negative Positive
VL treatment
LN: lymph node aspirate
BM: Bone marrow aspirate
SP: spleen aspirate
(1) Rarely DAT negative patients would
need LN/SP/BM
Fever > 2 weeks
with splenomegaly or wasting (malaria
and previous VL ruled out).
Send blood for DAT
DAT RESULT
Positive
Borderline
Negative
Search for other diagnosis and treat OR
refer (1)
Re-test in 1 week
OR
perform LN/BM/SP aspirate
Lymph node, bone marrow or spleen
aspirates
VL treatment
Negative
Positive
Search for other diagnosis and treat OR
refer OR Re-test DAT in 1 week
VL treatment
DAT Freeze Dried
Positive: ≥ 1:3200
Borderline (BL): 1:1600; 1:800;
1:400
Negative: ≤ 1:200

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
15
2.4 Diagnosis of relapse
A relapse of kala-azar means that a person has kala-azar but has already been treated before. Relapses usually occur within 6 months after treatment. If a patient comes with fever for more than 2 weeks and a palpable spleen ask if they have been treated for kala-azar before. A serological test cannot diagnose a relapse because it can still be positive for months to 2–3 years after treatment even if a person is feeling well. If the serological test was done and was negative, there is usually no relapse!
2.5 Diagnosis of PKDL
Post kala-azar dermal leishmaniasis is usually known as PKDL.
This is a rash that starts on the face. This rash may sometimes spread to the whole body but it always starts on the face.
This rash usually starts within 6 months of having kala-azar. Sometimes it starts at the end of kala-azar treatment. Rarely the person was not previously treated for kala-azar.
PKDL usually heals by itself. Sometimes it comes and goes for years. Sometimes it gets worse and worse. Sometimes it affects the mucous membranes.
The diagnosis of PKDL is easier if you study the pictures. Note that people can die with severe PKDL and that PKDL itself may be a reservoir for kala-azar infection.
NB: In Somalia PKDL cases have not been detected and it seems that it is very rare.
3. Treatment
The treatment regimens should follow these national guidelines in all treatment centers in Somalia. All patients treated for KA must be registered in the designated KA treatment register book (Annex 8). On admission all patients should be screened for acute malnutrition and referred as necessary.
On admission the KA treatment card will be also filled in so the data can be entered in the national data base of the Ministry of Health (annex 9). At discharge the patient will be given a card which will be useful for his/her reference, especially when the person visits another health facility or health personnel (annex 10).
Patients must be encouraged to return for a follow-up visit six months after discharge to make sure the treatment was successful. The date of that post-treatment visit is the final cure date to be recorded in the KA treatment card.
3.1 Treatment of primary kala-azar (new cases)
Treatment should normally be given only after confirmation of disease based on the clinical examination and the laboratory tests. At the same time, the presence and extent of concomitant infection should be ascertained, as this may influence the choice of therapy or supportive treatment. In many cases, supportive treatment, for example rehydration or nutritional supplementation, may be required before the start of therapy. Treatment should be given under the supervision of medical personnel.
The objectives of kala-azar treatment are:
to reduce parasites to “below the level of detection”;
to support the patient’s nutrition and hydration;
to treat complications;
to prevent development of drug resistance, and

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
16
to reduce or interrupt transmission of infection in the community
Hence, daily monitoring of signs and symptoms of each VL patient is necessary. Obtaining important baseline information such as, spleen size, hemoglobin, and body weight is also crucial. Weight should be taken weekly and drug dosage adjusted accordingly.
Treatment on the spot is important since some patients need treatment for other illnesses. Treat all the illnesses while waiting for the DAT result. Give ferrous and folic acid tablets while waiting for the results (except if patient is undergoing inpatient treatment of severe acute malnutrition, please refer to IMAM guidelines)
Treatment regimens (options) for primary kala-azar
First line regimens for primary kala-azar
Sodium stibogluconate (SSG) and paromomycin (combination therapy)
In this combination therapy sodium stibogluconate, 20mg/kg body weight /day, and paromomycin injection, 15mg/kg body weight /day are given intramuscularly for 17 days (annex 11–12).
This combination treatment is the first choice and line of therapy as the safety and efficacy is similar to the pentavalent antimonials monotherapy and considerably shortens the treatment duration.
Sodium stibogluconate (monotherapy)
SSG in monotherapy is administered as intramuscular injections 20 mg/ kg/day for 30 days .
In the absence or stock ruptures of paramomycin the pentavalent antimonials sodium stibogluconate and meglumine antimoniate can be used in monotherapy (Annex 13).
Remember that:
There is no upper limit for SSG, but doses above 10 ml should be given in 2 separate
injections.
The smallest dose is 2 ml for everyone over 5 kg in weight.
For severe vomiting the SSG should be stopped for 2 to 5 days until the vomiting stops.
If a child weighs 5 kg or less she/he is usually severely ill. Give 1 ml daily and follow
closely.
Patients with severe ascites may need a lower dose. If the patient has severe ascites:
Subtract 5 kg from the weight of an adult
Subtract 2 kg from the weight of a patient weighing between 24–40 kg
Subtract 1 kg from the weight of a patient weighting between 10–23 kg
Then calculate the dose of SSG.
Weigh the patient weekly and recalculate the dose accordingly.
HOW TO CALCULATE THE DOSE OF SSG
SSG vials contain 100 mg / ml so it is calculated as follows:
Dose in ml = Body Weight in kg x 0.2
EXAMPLES:
If your patient weighs 50 kg
50 x 0.2 =10 - so give 10 ml
If your patient weighs 9 kg
9 x 0.2 = 1.8 - but give 2 ml (the lowest dose)

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
17
Conditions for withdrawal of SSG:
Acute pancreatitis
Aberrations of creatinine
Jaundice developing during treatment
Excessively high LFT values, i.e. > 5x normal values of SGPT/SGOT
Any evidence of cardiotoxicity (prolonged QT interval, cardiac arrhythmia)
Declining hematological measurements (HCT, total WBT counts)
Uninterrupted vomiting
Failure to respond favorably during the first 2 weeks of treatment
If SSG needs to be withdrawn, then Ambisome® can be used as second line option.
Contraindications:
Patients with known cardiac diseases. Co-administration of quinine or any other drug known to cause cardiac toxicity is contraindicated.
Liposomal amphotericin B (Ambisome®)
Liposomal amphotericin B is the safest antileishmanial drug and needs to be available at the referral sites. It is presented as 50 mg per vial. Liposomal amphotericin B: 3–5 mg/kg per day intravenous by infusion over 6–10 days up to a total dose of 30 mg/kg. Ambisome® requires cold chain.
How to calculate the dose of PAROMOMYCIN
Paromomycin is 500 mg/ml in a 2 ml vial so it is calculated as follows:. Dose of paromomycin in ml = (weight in kg x 15) divided by 500 EXAMPLES: If your patient is 7 kg: (7 x 15) / 500 = 105 / 500 = 0.21 ml If your patient is 15 kg: (15 x 15) / 500 = 225 / 500 = 0.45 ml If your patient is 50 kg
(50x 15) / 500 = 705 / 500 = 1.41 ml
Remember that:
To administer paromomycin:
You must have 1 ml and 2 ml syringes to give this drug.
The recommended dose is 15 mg/kg sulfate (equivalent to 11 mg/kg base); no maximum
dose; monotherapy should not be used.
Patients must remain well hydrated because paromomycin can affect the kidneys.
Tell patients to drink enough that they pass urine 4 times a day.
If patients have too much vomiting and diarrhea, do not give the injections.
Patients over 60 years may have problems with their kidneys so should not get this.
This medicine may NOT be given intravenously
Weigh the patient weekly and recalculate the dose.
Do not give during pregnancy unless there is no choice

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
18
Ambisome® in VL is the first line treatment for pregnancy, severe patients and HIV co-infected patients.
3.2. Treatment of relapse of kala-azar
First relapse
A definitive or final cure is defined as an absence of signs and symptoms 6 months after initial cure (which was at the time of discharge). Therefore, to establish definite cure, active follow up should be done as part of the treatment centre activities. For definitive cure one looks at the clinical picture. No aspirate is necessary at follow-up unless relapse is clinically suspected. Patients should be instructed to return for follow-up 6 months after discharge or earlier in case they feel sick.
If a person returns with a clinical suspicion of kala-azar, after having received full treatment and discharged with a negative test of cure (TOC), the patient has a relapse. It is impossible to differentiate a relapse from a new infection. Therefore, all are considered relapses and treated as such under this scenario.
Relapses can occur in up to 5% of the treated patients. In HIV+ patients the relapse can go up to 50%. Most relapses occur within 6 months of initial discharge and these are called first relapses. A patient who had a first relapse, re-treated for that, and got cured again, can get a second relapse. Relapses tend to have a higher parasite load (but not necessarily so) and are difficult to treat.
There must be two negative TOC’s before discharging relapsed patients, because any further relapses will be more difficult to cure. The likelihood for a positive TOC after treating a relapse is higher than 10%. So, in every relapse case TOC’s have to be done. To ensure that there is at least a week of treatment after the first negative TOC, two consecutive TOC’s are performed one week apart. Relapse cases need close monitoring. Longer SSG therapy is associated with more side effects: kidney toxicity, pancreatitis, and arrhythmias are known complications. In-patient treatment (if feasible) is always preferred for relapse treatments. Usually, it is better to refer a relapsed patient for treatment in a hospital.
The clinician should check each week or even more frequently whether the relapsed patient is clinically responding. Good signs of response are the clearance of fever, well-being of the patient (e.g. able to walk, appetite improving), spleen size reducing, hemoglobin increasing, weight stable or increasing.
First line regimens for first relapse
In case of first relapses, a new treatment schedule is started, and the following are acceptable:
SSG 20 mg/kg/day IM
PLUS paromomycin 15 mg/kg/day IM for 17–30 days
If parasitology is available, end of treatment should be guided by clinical assessment and test of cure aspirates. TOC aspirates can start on day 17 for two drug (SSG plus paromomycin) combination therapy. TOC aspirates should be done weekly. When TOC is available, the minimum days of SSG is 30 for combination therapy. Paromomycin is given for only 17 days (more than 21 days may be toxic).
Sodium stibogluconate 20 mg/kg/day IM for 40 to 60 days
If parasitology is available, end of treatment should be guided by clinical assessment and test of cure aspirates. TOC aspirates can start on day 30 for single drug (SSG) therapy. Then TOC aspirates should be done weekly. When TOC is available, the minimum number of days of

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
19
SSG is 40 for monotherapy. After 60 days of SSG, it is clear that the parasite is unresponsive to SSG and 2
nd line treatment should be instituted as stated below.
Second line regimens for first relapse
Liposomal amphotericin B (Ambisome®)
Liposomal amphotericin B is the safest antileishmanial drug and needs to be available at the referral sites. It is presented as 50 mg per vial. Liposomal amphotericin B: 3–5 mg/kg per day intravenous by infusion over 6–10 days up to a total dose of 30 mg/kg. Ambisome requires cold chain.
Ambisome® in VL is mainly used for relapses, pregnancy, severe patients, HIV-co-infected patients and when SSG toxicity is not tolerated by the patient.
Amphotericin B deoxycholate
Dose: 0.75–1.0 mg/kg/d intravenous for 30 alternate days (15 mg/kg total dose)- infused with 1 liter of 5% dextrose in 2-12 hrs. Before the full treatment course, the patient is given an initial test dose, which is the first 1 mg of the first dose to be infused over 20 to 30 minutes; and the patient observed for 1 hour. The remaining doses are given as 1 mg/kg body weight IV once per day every other day for 30 days (total of 15 treatment doses).
Administration
Amphotericin B is infused in 1 litre of dextrose 5% infusion running over 2–12 hours. The slower infusions decrease infusion related side-effects (chills, fever). Before starting therapy, hydrate the patient and maintain hydration with ORS and, if needed, IV fluids. This is important to decrease the risk of renal toxicity.
Give potassium supplementation (1 tablet 3×/day for adults); if potassium tablets are not available, give one banana every eight hours (1 banana = 8 mmol KCl = 1 tablet KCl).
Management of fever: give paracetamol before infusion or at the onset of symptoms. Avoid gentamycin, streptomycin, paromomycin or other drugs that can cause renal toxicity.
Second relapses
Second relapses are not very common but occur especially in immune suppressed patients. The treatment option for those cases is to administer amphotericin formulations at the highest dose.
3.3. Treatment of PKDL
When to treat PKDL
The rash shows blackening especially around the nose
The rash is dense – the skin is almost covered with bumps that are almost touching
The rash includes mucous membranes – especially the nose, eyes or mouth
The rash is pealing or scaling
The patient with this rash is also ill with fever (after treatment for possible concurrent illnesses) and has a big spleen
Any patient who develops PKDL during kala-azar treatment: This patient should be continued on treatment until the PKDL is cured.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
20
The rare patient who has a new decrease in vision and eye pain with the rash. Iritis is rarely part of PKDL.
End of treatment of PKDL
Treatment of PKDL can be completed when the rash is no longer palpable. Feel the rash with your finger. If the skin is smooth you can stop treatment even if you can still see the rash. Everyone must have at least 30 days of SSG.
The treatment regimen consists of SSG 20 mg/kg/day IM for 30 – 120 days OR SSG 20 mg/kg/day IM for 30 to 60 days plus paromomycin 15 mg/kg/day IM for 17 days.
3.4 Other treatment related issues and special situations
Interruption of SSG treatment
Interruption during treatment can occur in two conditions: medically initiated interruption or severe vomiting and defaulting by the patient:
If interruption is less than 5 days, continue the treatment from where the patient stopped taking the treatment and continue until the full course of treatment is given.
If interruption is 5–14 days, the patient should continue from where they stopped but must have an adequate test of cure parasitologically at the end of treatment.
If interruption is 15 days or more, irrespective of the number of days of previous treatment, the patient needs readmission for parasitology testing; if positive, restart treatment as day one and do a test of cure before discharge. If negative, follow up is necessary and parasitological test if need be.
Evaluating cure
At the end of treatment with combination or monotherapy, the patient should be re-assessed. This usually includes clinical and laboratory examinations as described below:
Clinical response
Many patients get worse during the first few days of treatment. Patients, at the extremes of age, with severe anaemia, severely malnourished, in a state of collapse, and presenting with vomiting, pneumonia, or bleeding are at high risk during the first 10 days of treatment. After 7 to 10 days the patients become afebrile, and begin to look stronger, become more mobile, with increased alertness and appetite.
By day 14 the spleen size regresses, hemoglobin rises and there is weight gain (note: loss of oedema may mask weight gain during treatment). By the end of successful treatment, patients are afebrile, usually have a smaller spleen than on admission, and have an increased hemoglobin level (though most remain anaemic). All the patient conditions get improved.
Initial parasitological cure – the role of TOC
Splenic aspirate is more sensitive for diagnosis and for TOC. Lymph node aspirate (LNA) has been used for TOC when splenic aspirate is not possible.
There is no clinical sign that correlates with a positive test-of-cure aspirate (TOC) or that predicts increased risk of relapse. The exceptions are signs of co-existing TB or HIV, both of which will increase the risk of treatment failure. TOC is done for assurance that discharge is appropriate for patients who may have difficulty returning for care/follow-up. When done systematically it is also a way to monitor the emergence of drug resistance.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
21
Non-response is defined as no decrease in the grade of parasitology from before treatment to after adequate treatment. For those patients who are not aspirated on admission, use 4+ at TOC as defining primary unresponsiveness. Anyone with any TOC of 4+ (or a TOC that does not become negative by 60 days of SSG) should get second line treatment.
Clinical judgment will always play the final role in any decision-making process given the variability of individual VL cases.
Kala-azar treatment in pregnancy
Kala-azar treatment during pregnancy cannot be differed as untreated VL during pregnancy may lead to severe disease, characterized by high grade anaemia, spontaneous loss of the fetus, and congenital VL because of transplacental transfer of parasites, even in apparently low symptomatic cases. Unfortunately, no drug of VL is proven to be safe in pregnancy – however, none are known to be harmful. Pregnant women should therefore be treated with the safest available anti-leishmanial drugs.
Amphotericin B deoxycholate or its liposomal formulation is safe and effective for pregnant women and their fetuses, and is therefore recommended as first-line treatment for these patients. The dosage and administration is the same as other patients.
Pentavalent antimonials are less safe in pregnancy, as they can result in spontaneous abortion, preterm deliveries and hepatic encephalopathy in the mother and vertical transmission.
Paromomycin: Ototoxicity in the fetus is the main concern and hence should be avoided as much as possible.
Leishmania–HIV coinfection
Visceral leishmaniasis is an AIDS-defining condition and a valid entry point for starting antiretroviral treatment, irrespective of CD4+ count. The baseline CD4+ count is lower in visceral leishmaniasis–HIV co-infected patients, as visceral leishmaniasis itself causes a reduction in CD4+ cells. The impact of antiretroviral treatment on visceral leishmaniasis in co-infected patients includes reduction of incidence of VL, higher survival rates, a reduction in relapse rate and possible immune reconstitution inflammatory syndrome.
HIV and Leishmania infection reinforce each other. HIV patients are more likely to develop visceral leishmaniasis (due to reactivation of a dormant infection or clinical manifestation after primary infection). Patients characteristically have high disseminated parasite loads. Visceral leishmaniasis negatively affects the response to antiretroviral treatment and is difficult to cure in co-infected patients.
The prognosis of co-infected patients is characterized by a high mortality rate during the first episode, increased anti-leishmanial drug toxicity (predominantly with antimonials), poor long-term clinical response, parasitological cure and a high relapse rate over a lifetime. The risk factors for relapse are: no antiretroviral treatment, low CD4+ cell count, previous visceral leishmaniasis episode, failure to achieve clinical or parasitological cure during the first episode and no secondary prophylaxis.
Antimonials are more toxic in HIV patients, necessitating careful monitoring for pancreatitis and cardiotoxicity.
Treatment of VL in HIV co-infected patient
Amphotericin B deoxycholate or lipid formulations should be considered first and pentavalent antimonials only in areas of no significant resistance and when lipid formulations of amphotericin B are unavailable.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
22
Lipid formulations (e.g., Liposomal Amphotericin B, Ambisome) infused at a dose of 3–5 mg/kg daily or intermittently for 10 doses (days 1–5, 10, 17, 24, 31 and 38) up to a total dose of 40 mg/kg are recommended.
3.5. Treatment of concurrent infection and malnutrition
General kala-azar patient management
Because infection with Leishmania depresses the immune system, patients with kala-azar are at increased risk for other infections. Additionally, the severity of such infections in kala-azar patients may be greater than in patients without kala-azar. All concurrent illnesses should be treated immediately and aggressively.
Many kala-azar patients are severely malnourished. Because of this and their immune depression, these guidelines include routine treatments similar to those given in therapeutic feeding centers.
Kala-azar patients can die during treatment. Those at most risk are those who are very young (< 3 years), those who are old, those severely malnourished, those severely anemic, those with prolonged disease (more than 2 month history), and those with vomiting. Please give special care for these patients!
All kala-azar patients should be screened for malaria and managed promptly following the national treatment guidelines:
If treated with Artemisinin Plus Fansidar in the previous 7 days no more treatment is needed.
If not treated and not tested, the patient must be tested for malaria or treated.
If the test is positive give Artemisinine plus Fansidar.
NB: Remember not to use Fansidar in the first 2 months of pregnancy, use Quinine instead.
On admission give Vitamin A to all VL patients except pregnant women:
Vitamin A - 200,000 IU –
if 6 months to 1 year use 100,000 IU;
if < 6 months, use 50,000 IU
do not give to pregnant women until after delivery.
Amoxicillin for 5 days
Tinidazole for 3 days or metronidazole for 7 days
Daily tablets if not being treated for acute malnutrition
Vit C and multivitamins – not needed if there is good food available
Ferrous plus folic acid
Remember
to also treat all other illnesses and complaints on admission to send children for measles vaccination if not previously vaccinated

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
23
* If severely malnourished, give folic acid alone for first 7 days. If the patient is pregnant give 2 ferrous each day
Discharge tablets
Ferrous plus folic acid 30 tablets for daily use
Fansidar* to all patients with a palpable or visible pregnancy that is less than 9 months.
Albendazole* for non-pregnant patients if your area has round worms.
Note that most severely malnourished patients have iron stored in their body, but kala-azar patients may have none. For this reason we add the ferrous to the folic acid on day 7 rather than waiting for day 14 as in many stabilization centre (SC) protocols.
Treatment of malnutrition
Promoting good nutritional status of patients is key in the management of kala-azar. Experience has shown that 70–75% of the diagnosed cases are severely or moderately malnourished and in desperate need of nutritional supplements.
The latest round of nutrition and mortality surveys conducted in October 2011 indicate extremely high levels of global acute malnutrition and mortality compared to normal levels for this time of year, yet show some improvements from the round of surveys from August 2011. In most of the regions the rates of acute malnutrition remain near or above 30%, and depict a Very Critical nutrition phase.
Therefore, these guidelines include the treatment of acute malnutrition in line with the National Guidelines for Integrated Management of Acute Malnutrition (IM-SAM).

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
24
Admission criteria for moderately and severely malnourished Kala-azar cases:
Admission criteria for children from 6 to 59 months of age
SC OTP TSFP
SAM with complications SAM no-complications MAM
New
ad
mis
sio
ns
W/H (Z-score) < - 3 < - 3 < - 2
MUAC (mm) < 115 < 115 < 125
Oedema
Bilateral oedema +++ Marasmus with
any oedema
No oedema, or
Bilateral oedema + , ++ No oedema
Appetite NO APPETITE Pass appetite test N/A
Complications
Uncontrollable vomiting
No complications No complications
Fever > 39 ºC
Hypothermia < 35 ºC
Lower respiratory tract infection
Severe anaemia
Extensive skin infection
Very weak, apathetic
unconscious, convulsions
Admission criteria for other categories
Indicator SAM MAM
Infants less than 6 months
W/H (W/L Z-scores) < - 3
Static weight or loosing weight at
home
Oedema Present Absent
Clinical presentation To weak to suckle breast Poor feeding
Older Children and Adolescents (5–18 years)
W/H (Z-scores) < - 3 < - 2
MUAC (mm)
<145 for children 5–10 years and < 160 for
children 10–18 years N/A
Oedema Present Absent
Adults (oder than 18 years)
BMI and clinical signs < 16 with weight loss in the last 4 weeks < 16 but no weight loss
Oedema Present Absent
Pregnant and lactating women
MUAC (mm) < 210 with weight loss in the last 4 weeks
< 210 with no weight loss in the last 4
weeks
SAM-Severe Acute Malnutrition; MAM-Moderate Acute Malnutrition
See annex 14 for Anthropometry look-up tables
Nutritional treatment for severely malnourished kala-azar cases
Severely malnourished patients can be treated as inpatients (in Stabilization Centres) or outpatients (in Outpatient Therapeutic Feeding Centres) depending on whether or not they present with medical complications. It is likely that most patients with kala-azar will need to be treated as inpatients due to the daily injections that they must receive. However, once the

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
25
need for injections is over than they can be transferred to outpatient treatment to complete their nutrition rehabilitation.
Infants should always be treated as inpatients. Infants 0-5 months with SAM who are not breastfed are particularly at risk and require protection and support to reduce the risks of artificial feeding. For these infants and their caregivers, the potential for restoring or establishing breastfeeding should always be explored to the maximum. Further, it is not appropriate to provide infants 0-5 months with RUTF because the reflex of swallowing semi-solid foods is not yet present.
Nutritional rehabilitation of severely malnourished patients uses several specialized products. F-75 Therapeutic milk is used in the first phase of inpatient care to stabilize the patient. Once the patient is stabilized they can be moved to transition phase which uses either F-100 therapeutic milk or Ready-to-Use Therapeutic Food (RUTF). From their they move to a rapid weight gain phase which almost always uses RUTF unless the patient is an infant or has other complications. F-75, F-100, and RUTF are all given based on body weight and look-up tables for quantities can be seen in Annex 14.
Nutritional treatment for moderate malnourished Kala-azar cases
The treatment of moderately malnourished patients should use Ready-to-Use Supplementary Food (RUSF) or fortified flour porridge. RUSF is the preferred treatment.
Target group Treatment
Children 6–59 months Provide 3 sachets of RUTF per day for the duration
of the treatment
Above 5 years (older children 5-9 yrs, adolescents
10–18yrs and Adults)
Provide 2 sachets of RUTF per day for the duration
of the treatments
Basic food rations
Food rations should be provided to all kala-azar patients for the duration of treatment except for the initial inpatient treatment of severely malnourished patients who should only consume the specialized nutritional products.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
26
BENEFICIARY
CATEGORY
Daily food ration (per person/grams)
Eligible
beneficiaries)
Cereal Pulses Oil Salt Sugar CSB Total Duration
1) IFP
inpatient
HIV, TB, Kalazar,
Leprosis inpatient
450 50 30 10 30 50 620 During hospitalization
2) IFP outpatient HIV, TB, Kalazar,
Leprosis outpatient
450 50 30 10 30 50 620 During ambulatory
treatment period (ARV,
DOTS)
3) IFP caretaker One caretaker for
one HIV, TB,
Kalazar, Leprosis
inpatient
450 50 30 10 540 When accompanying
inpatients for treatment in
hospitals
4) IFP
family ration
Two family
members for one
HIV, TB, Kalazar,
Leprosis outpatient
450 50 30 10 540 During ambulatory
treatment period (ARV,
DOTS)
5) TFP caretaker One caretaker for
one SAM child 6-59
months
450 50 30 10 540 During therapeutic
treatment at TF center
Systematic medicine for severe malnutrition
Name of Product When Age / Weight Prescription Dose
VITAMIN A* AT ADMISSION
6 months to
< 1 year 100 000 IU
Single dose on
admission ≥ 1 year 200 000 IU
DO NOT GIVE TO CHILDREN WITH
OEDEMA
AMOXICILLIN AT ADMISSION All beneficiaries See protocol 3 times a day for 7
days
MEASLES VACCINATION AT ADMISSION From 9 months (standard) Single dose on
admission
ALBENDAZOLE SECOND VISIT
< 1 year Do not give None
12–23 months 200 mg (1/2
tablet) Single dose on day
7 ≥ 2 years
400 mg (1
tablet)
* VITAMIN A: do not give if child has already received within last 3 months.
DO NOT provide to patients with oedema. Wait for oedema to fully subside.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
27
Treatment of diarrhea ORS, made with boiled water, left to cool, or with borehole water.
Zinc supplements, 10mg/day for infants below 6 months and 20mg/day for patients 6 months and over.
Tinidazole for 3 days, then continue tablets to 5 days if diarrhea continues (no more than 10 days total) OR Albendazole single dose.
ask if they have nausea or vomiting and treat if they do
Diarrhea 4 times or more in 24 hours OR any diarrhea with blood OR any diarrhea with fever:
ORS, made with boiled water, left to cool or with borehole water.
Ciprofloxacin AND Tinidazole for 3 days – to 5 days if diarrhea persists.. (Tindazole for persistent diarrhea may be given for a total of 10 days.)
ask if they have nausea or vomiting and treat if they do
Second line treatment:
substitute metronidazole for 7-10 days for the tinidazole
Unresponsive diarrhea:
Consider sending a stool specimen to the laboratory.
Consider potassium supplement (slow K) for patients with severe diarrhea and vomiting.
This protocol is for use with kala-azar patients only. Viruses cause most diarrhea in the world and there is no medicine other than oral rehydration salt (ORS) and zinc supplementation. Kala-azar patients are different; they get more dysentery and they are too weak. Note that zinc supplementation and ORS is not recommended if the patient is undergoing treatment for severe acute. Diarrhea with associated weight loss in a patient with severe acute malnutrition should be treated with ReSoMal as per IMAM guidelines. If the diarrhea is not causing weight loss than rehydration should be done with potable water alone. ORS is contraindicated in the treatment of diarrhea or vomiting when there is severe acute malnutrition.
Any diarrhea:
Causes of diarrhea
Syndromic diagnosis (diagnosis based on history and physical) is good. The syndromic diagnosis is based on evidence from well-equipped hospitals and on knowing what diseases are in your area. Sometimes there are confusing cases. If you have a lab this can sometimes help sort out these confusions. Remember though, one stool specimen is not sensitive – it is simply a help. You may need multiple specimens. Remember too that patients can have more than one germ. Use the below table as a quick reference for treatment of various pathogens causing diarrhoea:
People do not usually die of the germ causing diarrhea, they die because they lost too much
water or they are starving. Anyone with diarrhea must eat and drink more than normal or they
may die. ORS, local made with safe water, and high energy biscuits are good choices.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
28
Treatment of vomiting
Patients who vomit only with cough do not need medication for vomiting.,
Give paracetamol if they have a fever
Give promethazine tablets for 2 days but patient has difficulty of taking orally, give IM.
Tell the patient to take the tablet and then wait 1 hour before taking any other tablets or eating.
Tell the caretaker that the patient will get a little sleepy from promethazine, but they should be awakened to drink.
Give ORS and asses hydration status frequently.
Continue breastfeeding
Consider stopping the SSG for 2 to 5 days.
Any patient who has nausea or vomiting should continue eating and drinking but in small amounts 5 to 7 or more times a day.
Any patient taking tinidazole or metronidazole should be asked about vomiting. Both these drugs are common causes of vomiting. You may treat with promethazine.
Severe vomiting
Be careful of these patients who cannot stop vomiting, patients who vomit too much to keep down water, ORS or milk.
Stop the SSG for 2 to 5 days until the vomiting is gone. If the vomiting stops within 5 days, continue the SSG from the dose you stopped.
Give promethazine injection.
Pathogen Fever
common
Stool exam Other symptoms Treatment
ORS for all!
Viral No Normal ORS
Giardia No Giardia Nausea, vomiting, burping, bloating,
abdominal cramp, May or may not
have diarrhea
Albendazole or
Tinidazole or
Metronidazole
Ameba No RBC
<5 WBC
Ameba Trophs
abdominal pain, tenesmus,
sometimes with blood mixed with
mucus
Tinidazole or
Metronidazole
Bacterial Yes WBC
RBC
Many times a day diarrhea, may be
bloody, may be very ill
Ciprofloxin or co-
trimoxazole
SSG can cause nausea and vomiting. Vomiting is associated with death
in kala-azar patients. Please give close attention to these patients.
Remember that malaria and meningitis cause also cause vomiting;
check your patients carefully!
Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
29
Always start promethazine tablets following the injection. Start the promethazine tablet 1/2 hour after the injection so they do not vomit it; the effect of the injection will stop in one or two hours. The effect of the tablets lasts 3 to 6 hours.
Always give ORS, give small amounts every 15 minutes. They may need an IV of Saline or Ringers Lactate if they are dehydrated. Please refer them to help!
Special notes for children < 12kg who are vomiting
Take the temperature and make sure the child has no other disease such as malaria or meningitis. Try giving small amounts of ORS every 5-10 minutes. Give paracetamol if needed. You may give promethazine syrup after you have checked for other illnesses. Patients who vomit only when coughing do not need promethazine.
Treatment of malaria
Every one with a documented fever after the first 7 days of kala-azar treatment with no obvious source of the fever should repeat a blood film or RDT for malaria if possible. Consider malaria treatment if there is no other source of fever and no laboratory test is available.
Remember that pregnant mothers and young children get malaria easily.
Treat with ACT and paracetamol if more than 2 weeks from the last malaria treatment for uncomplicated malaria. Treat with Quinine for severe malaria (severe vomiting, a seizure in an adult, repeated seizures in a child, talking crazy, hypoglycemia, jaundice, pulmonary edema, Hb < 5, or any altered mental status).
Note that SSG should not be used with quinine (due to prolonged QT interval and cardio-toxicity).
If treatment with quinine is inevitable, stop SSG for VL while quinine is being given. After quinine treatment is finished, resume SSG injections, starting 24hrs after the last dose of quinine. Consider shortening quinine usage for 3-5 days and finish with other antimalaria medicines. This helps to resume SSG within short period.
NB: refer to the national Malaria guideline for detailed dosage and duration of treatment.
Treatment of pneumonia
The diagnosis follows the health worker guidelines so check the last version of the integrated management childhood illness (IMCI) guidelines in use in Somalia:
kala-azar patients can get a dry cough that does not need antibiotics
kala-azar patients commonly get a pneumonia that does need antibiotics
adults as well as children get pneumonia
fever, productive cough, chest pain with breathing, and fast breathing are all part of a diagnosis of pneumonia
WHO-IMCI guidelines for diagnosing pneumonia in children
based on respiratory rate (RR):
Diagnose pneumonia if a child
2 – 12 months has RR > 50;
NOTE: normal RR is up to 60 for 0-2mo, 40 for infants, 30 for 12 months–5 years

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
30
Treatment of mild to moderate pneumonia
amoxicillin for 7 days.
Amoxicillin is preferred over cotrimoxazole. Amoxicillin but not cotrimoxazole will treat most pneumonia from aspiration that occurs with vomiting or seizures or a concurrent ginigivitis. Erythromycin is a reasonable first line drug for older children and adults who do not have the aspiration risks. Erythromycin can cause vomiting which is already a problem for kala-azar patients.
Treatment of pneumonia not improving by day 3 or 4
ceftriaxone injection, chloramphenicol capsules
Initial treatment of all serious pneumonia
ceftriaxone once daily injection
second line treatment, chloramphenicol oral or by injection 3 or 4 times a day
Signs of serious pneumonia
infants breathing too fast to breast feed
pneumonia patients with significant vomiting, unable to keep down medicines
patients with respiratory distress (retractions, flaring nose, grunting)
unexplained abnormal mental status
Please refer these seriously ill patients to the senior medical staff. They may be acidotic from dehydration or sepsis, they may have severe malaria or meningitis with the pneumonia.
Treatment of tooth or gum pain - with or without bleeding
clean teeth twice a day
Procain penicillin or amoxicillin for 5 days
paracetamol as needed (never aspirin)
Treatment of bleeding
Nose bleeding: Pinch the nose at the end of the bony part for 10 minutes.
Patients treated successfully for pneumonia will usually have their fever subside in 3 days and
their cough and crepitations usually subside in 8 days.
Patients who have pneumonia all through their kala-azar treatment and/or who are unresponsive
to antibiotics may have tuberculosis (TB). Document any fever. Take the temperature in the
evening. Adults may need a sputum test. Ask children with continuing pneumonia if there is a
family history of pulmonary TB.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
31
If the nose bleeding will not stop with pinching: pack the nose with petroleum jelly on gauze and leave the pack in for at least 2 days. If you pack the nose, treat with amoxicillin (for prevention of sinusitis).
Gum bleeding: treat with penicillin or amoxicillin for 5 days.
Give vitamin C
Occasionally you will need epinephrine on gauze compresses to stop the bleeding
If the patient has jaundice: give vitamin K___ IM for 5 days.
Treatment of conjunctivitis
Tetracycline eye ointment is used for red conjunctiva especially if there is drainage. Any sign of trachoma should be treated with tetracycline eye ointment.
Gentamicin or chloramphenicol eye drops for abundant pus discharge or for failure of tetracycline ointment. Use until 2 days after pus discharge is gone.
Make sure this patient got vitamin A on admission! Patients who are severely malnourished can have a second dose of vitamin A.
Iritis is a rare disease that can accompany PKDL. There is eye pain and the vision is blurry – like looking through a cloud. There is usually little or no pus. Please notify a doctor. The patient needs to continue the SSG. They may also need steroid eye drops.
3.5.10. Treatment of infected wounds
Clean and treat with penicillin for 5 days, they may need gentian violet.
If the wound is not improving consider cloxacillin.
If they have an injection abscess it may need draining and cloxacillin.
Treatment of herpes zoster
This is an extremely painful rash that can occur at the end of, or just after kala-azar treatment. It is only on one side of the body and usually covers only a small area. The skin is red and develops blisters.
This is NOT associated with HIV when it occurs at the end or after kala-azar treatment (or if it occurs in the elderly).
Treat with 5 to 10 days with paracetamol or ibuprophen (ibuprophen is OK to use ONLY at the end of kala-azar treatment).
If the wounds are open you can use gentian violet
Treatment of pain
Treat with paracetamol (for severe pain consider tramadol).
Never use aspirin for kala-azar patients, this can cause bleeding
* Ibuprophen and indometacin may cause bleeding so should be avoided
See treatment and medicines for concomitant diseases in annexes 15–16.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
32
4. Information system
This is a crucial aspect to allow data collection and analysis for monitoring and evaluation of the activities.
In addition to the register books and patient’s forms, data should be summarized in the monthly report forms and then submitted to MOH. When an outbreak is declared a weekly report form is also to be filled in (annex 17–18).
5. Prevention and control
Leishmaniasis control in general is primarily based on finding and treating cases, combined where feasible with vector control and, in some zoonotic foci, control of animal reservoirs.
In practice, providing access to sensitive diagnostics and quality treatment, and prevention of sandfly bites are currently the only feasible options in Somalia.
Active case finding is may be opted for as it becomes essential if patients have difficulties and delays in reaching treatment.
Prevention should aim at reducing the number of bites by wearing appropriate clothes (long sleeved) and repellents (ash, neem oil, commercial) during the evenings, especially during the dry season when kala-azar is transmitted.
The use of long lasting insecticide- treated nets (LLINs) provides personal protection in areas of transmission. Fine mesh (jersey fabric) bed nets with or without impregnation will also protect, but are hot. Impregnated bed nets should be distributed to all Kala-azar patients at treatment centre.
Health education should focus on;
Appropriate usage of LLINs, including the mode of transmission of kala-azar
The danger of sleeping outside without being protected by a mosquito net
The signs and symptoms of kala-azar, and the availability and location of treatment centres, aiming at improving early reporting of symptomatic cases.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
33
6. Annexes
Annex 1. rK39 rapid diagnostic test procedure
The utility of a rapid diagnostic test for visceral leishmaniasis lies in its simplicity. Several brands of test with rK39 antigen are available. Operators should always read the package insert carefully, and follow the manufacturer’s instructions. This is especially important with regard to the type of specimen used: serum or whole blood. Some brands can be used only with serum, while others can be used with whole blood collected by finger prick.
Test procedure
In general, the test procedure is as follows (figure 3):
1. Remove the test strip from the pouch and place it on a flat surface.
2. Place a specified amount of patient specimen (serum or finger-prick blood) on the absorbent pad on the bottom of the strip.
3. Add the specified amount of buffer provided.
4. Read the result after 10–20 min, according to the manufacturer’s instructions.
Some brands require a slightly different procedure, for example:
1. Take a test tube or a U-bottom microtitre plate.
2. Add a specified amount of buffer to the tube or well.
3. Add a specified amount of specimen (blood or serum) to the tube or well and mix.
4. Immerse the test strip into the buffer–specimen mixture.
5. Read the result after 10–20 min, according to the manufacturer’s instructions.
Points to consider for optimizing use of rapid diagnostic tests
Have a clear management plan to deal with positive and negative results.
Follow biosafety standards and precautions for handling blood and other body fluids.
Ensure proper storage conditions.
Do not use damaged or expired tests.
Adhere strictly to the manufacturer’s instructions.
Use test kits within 1 h of removal from pouch.
Read the results within the time specified by the manufacturer.
Do not reuse a test.
Interpretation of the test
Positive result: When both control and test lines appear, the sample tested has antibodies against recombinant K39 antigen of Leishmania. Even a faint line should be considered positive.
Negative result: When only the control line appears, there are no antibodies against recombinant K39 antigen of Leishmania present in the patient’s sample.
Invalid result: When no control line appears, a fresh patient sample should be tested with a new strip.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
34
Advantages and disadvantages of the rK39 test
Advantages
Simple to perform with minimal training.
Does not require a laboratory.
Can be performed with finger-prick whole blood, serum or plasma.
Kits can be transported and stored at ambient temperature (up to 30 °C).
Results are available within 10–20 min.
Disadvantages
Cannot distinguish between active cases and relapse in previously treated cases. Therefore, interpretation must always be accompanied by clinical case definition.
In patients with advanced HIV infection, a negative result does not rule out a diagnosis of visceral leishmaniasis.
A. diamed-it leish
This is a ready-made kit, and so follow strictly the instructions provided by the manufacturers. The test can be used either on finger prick blood or plasma/serum. The kit is provided with a device containing 2 wells: that of conjugate well (red line) and wash well. The device should be used within 15 minutes of opening the packet.
Figure 3. Procedures for the DiaMed-IT LEISH test

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
35
Test procedure
Take out the device from its package and place it horizontally on a flat surface.
Write the name and an identifying number of the patient on the space provided.
Tear open the ampoule of buffer, add 1 drop to the conjugate well and 4 drops to the wash well, and allow to stand for 1 minute.
Add 8-12 l blood/serum/plasma to the conjugate well by squeezing the pipette gently. Stir gently with the upper end of the pipette and allow to stand for 1 minute
Pull the device apart by holding the device with wells between thumb and forefinger, and with the other hand pulling out the dipstick holder (with label). Then place the wells on a flat surface, and insert the legs of the dipstick holder into the holes besides the conjugate well (with red line) so that the dipstick end reaches the bottom of the conjugate well. Allow to stand 10 minutes (5-10 minutes for serum/plasma).
Transfer the dipstick to the second well (wash well) and allow to stand 10 minutes (5 minutes for serum/plasma). N.B. – the reaction field should then be completely cleared of blood or serum/plasma, and the control band should be clearly visible.
Remove the dipstick from the wash well and click it back into the clear plastic piece. Close the wells with the well cover, break them off, and break the two legs off from the clear plastic piece (to be discarded).
Read the reaction and interpret the results. Keep the dipstick slide for future reference.
The appearance of dark purple bands on the dipstick demonstrates a positive reaction in the presence of a control band. The test is invalid if the control band is not visible.
A very faint line/band must be considered as positive reaction.
DiaMed -IT LEISH Set.
Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
36
B. Inbios kalazar detect test
This is also a ready-made kit, and so follow strictly the instructions provided by the manufacturers. The test can be used either on finger prick blood or plasma/serum. The kit is provided in pouches containing strips and appropriate buffers.
Test procedure
Take out the test strips from its package and allow reach room temperature.
Add 20-30 l blood/serum/plasma to the area beneath the arrows shown in the strips.
Place the test strip into a test tube or well of a 96 well tissue culture plate so that the end of the strip is facing downward.
Add two to three drops (150 l) of the chase buffer provided with the test kit
Read the results in 10 minutes

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
37
Annex 2. Direct agglutination test procedure
Principle of DAT
Infection with L. donovani results in production of antibodies against the parasite. These antibodies can be demonstrated in blood or serum by agglutination test.
The DAT antigen is a whole, killed, promastigotes from cultures of L. donovani which have been stained blue for visibility. These are suspended in solution, and when left in a V-shaped well, will slowly fall to the tip of the V, giving a dense blue dot. If anti-Leishmania antibodies are present from the blood or serum, the blue-stained parasites (DAT antigen), will become cross-linked by the antibodies (directly agglutinated) and will settle to the bottom of the well as a hazy blue mat or a cloud, NOT a dot.
By diluting the serum 2-fold in each well starting at 100x dilution, the titer (quantity of antibody) can be measured.
These procedures are for freeze-dried presentation of DAT.
Collection of blood specimen for DAT
Collect capillary blood from the finger or the toe or heel in infants.
Method
Requirements
DAT request form
DAT registration book
Whatman No.3 filter paper
Sterile lancet
Disinfectant e.g. iodine, alcohol etc.
Cotton wool
Scissors
Plastic bag
Pen (ball point)
Paper clips
Procedure
Cut the circular filter paper into 8-16 segments depending on the size. Each segment can be used for one patient’s test only.
Draw a circle of approximately 1cm in radius on the segment of the filter paper.
Record the patient’s details in the laboratory registration book (annex 7).
Write the DAT number on the patient’s request form and also write this number on the segment.
Soak a piece cotton wool in iodine or alcohol and disinfect finger, toe or heel thoroughly. Allow the skin to dry.
Using the sterile lancet, prick the finger firmly so that blood flows freely without excessive squeezing.
Wipe the first drop of blood with a plug of dry cotton wool. The first drop of blood is normally contaminated with dirt and tissue fluid.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
38
Squeeze the finger gently and collect the next drop of blood into the circle on the segment of the filter paper. Check the DAT number on the filter paper before collecting the blood.
Make sure the blood soaks through both sides of the filter paper and fills the circle
Allow the filter paper to dry.
Apply pressure to the finger prick with a dry cotton wool.
Discard the used cotton wool into the waste bucket and the lancet into the sharps container.
When dry, very dry, clip the filter paper with the request form and put into a plastic bag.
Store in a fridge or cool box until ready to send for testing or until ready for performing the test.
Elution of samples – Day 1
Requirements
Laboratory register
Microtitre plates (V-shaped)
Sample (dry in filter paper)
Micropipette to measure 125 µl
Normal saline
Paper punch (5mm)
Scissors
Marker (permanent)
Forceps
Refrigerator
Procedure
Write the number of the samples in order in the laboratory register. The list should be labeled to show which row of which microtitre plate corresponds to which sample. e.g. The list can be labeled A, B, C, D, E, F, G, and H in order.
The samples need to be grouped by 8 samples in each group or less. Group one is called Plate I, group two is called Plate II and so on.
Label the microtitre plates to correspond with the laboratory register. i.e. Get out the microtiter plates and write on the plate itself the plate number. The first one is plate I.
Using the paper punch, punch out a sample of filter-paper blood.
Using the forceps, put the punched sample of filter-paper blood into the well of the first column of the microtitre plates corresponding to the position recorded on the patient laboratory register. Ensure that the punched filter paper blood is properly inserted in the well. e.g. The sample listed as A should go in the first row labeled A. The sample listed as B should go in the second row labeled B, and so on.
Take the micropipette and adjust it to measure 125ul, fix the pipette tip firmly and pipette 125 ml of normal saline. Add the 125ul of normal saline to each well with a sample paper. Make sure that the punched filter paper blood is completely immersed in the saline.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
39
Cover the plates with another microtire plate incubate in the fridge (at 40C) overnight for at least 8 hours.
Dilution and titration – Day 2
Requirements
Measuring cylinder
50ml container (plastic or glass bottle or conical tubes)
Research (Repetitive) pipette 100-1000l, adjustable; brand Handy-Step or Eppendorf with volume display, Combitip ejection.
Multipipette 100 – 1000 μl Eppendorf or Handy-Step adjustable with Volume display and tip ejection.
Multichannel pipette, 8 channels, 5 – 50 l Eppendorf, adjustable volume and tip ejection.
Micropipette tips (yellow tips for 100ul Multipette and the Multichannel pipette, blue tips for up to 1000ul Research pipette, combitips standard 1.25ml and combitips plus 2.5 ml)
5 – 10 ml syringe
2-mercaptoethanol (2-ME)
Normal saline
DAT antigen (Freeze dried antigen OR Liquid antigen)
Freeze dried control sera
Preparation of diluent
1. To be used with Freeze dried antigen (FDA)
Measure 50ml of normal saline and put in the container
Adjust the multipipette to measure 390ul, pipette 390ul of 2-ME and add to the normal saline then mix gently.
Reconstitution of the Freeze dried antigen (FDA)
Add 5ml of fresh normal saline to the vial of the antigen
Mix gently by rotating and tilting the vial. Do not shake
Let it stand for about 10 minutes before use.
Freeze dried antigen is kept at room temperature.
Reconstitution of the freeze dried control
Use a new set of control sera with every new batch of DAT antigen. Make sure all the freeze dried powder is on the bottom of the vial. (The control kits made in Amsterdam contain 2ul of serum each)
Strictly follow the manufacturers’ instructions on the procedure for reconstitution especially the amount of normal saline or diluent to be added to the vial.
Either add 100ul or 200ul of normal saline or diluent to the vial of the control sera depending on the manufacturers’ instructions.
Mix gently by rotating.
Let it stand for at least 10 minutes before use.
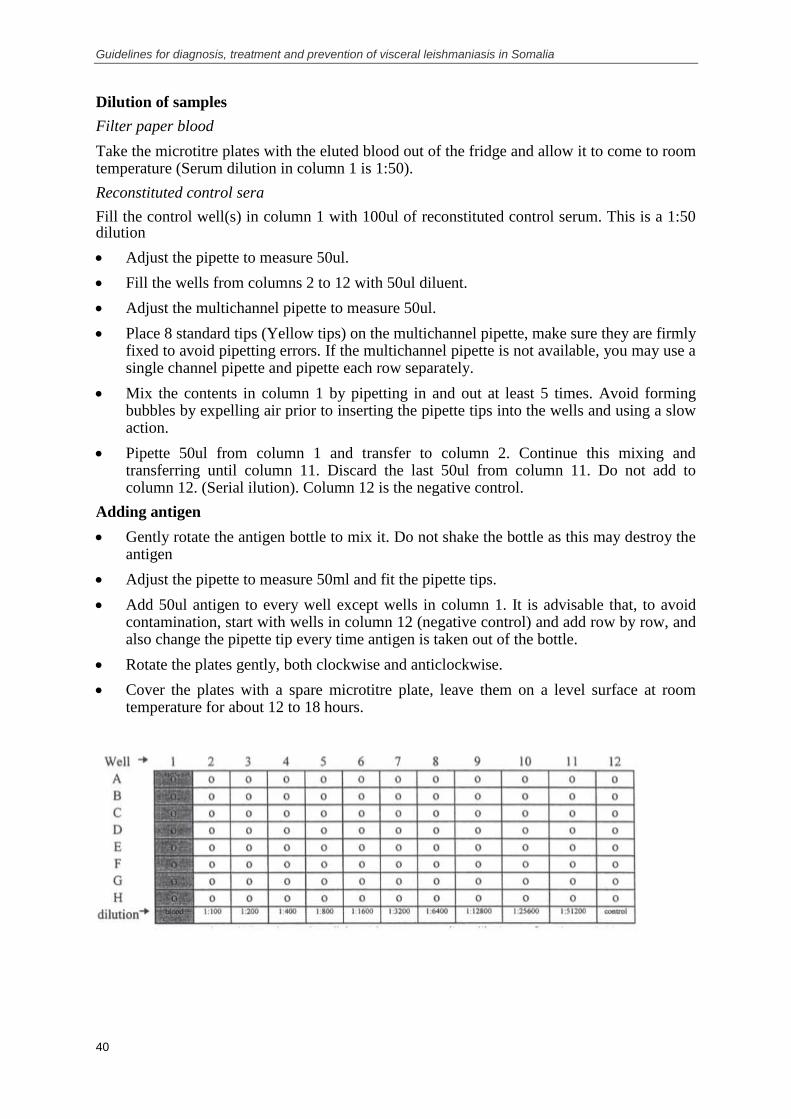
Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
40
Dilution of samples
Filter paper blood
Take the microtitre plates with the eluted blood out of the fridge and allow it to come to room temperature (Serum dilution in column 1 is 1:50).
Reconstituted control sera
Fill the control well(s) in column 1 with 100ul of reconstituted control serum. This is a 1:50 dilution
Adjust the pipette to measure 50ul.
Fill the wells from columns 2 to 12 with 50ul diluent.
Adjust the multichannel pipette to measure 50ul.
Place 8 standard tips (Yellow tips) on the multichannel pipette, make sure they are firmly fixed to avoid pipetting errors. If the multichannel pipette is not available, you may use a single channel pipette and pipette each row separately.
Mix the contents in column 1 by pipetting in and out at least 5 times. Avoid forming bubbles by expelling air prior to inserting the pipette tips into the wells and using a slow action.
Pipette 50ul from column 1 and transfer to column 2. Continue this mixing and transferring until column 11. Discard the last 50ul from column 11. Do not add to column 12. (Serial ilution). Column 12 is the negative control.
Adding antigen
Gently rotate the antigen bottle to mix it. Do not shake the bottle as this may destroy the antigen
Adjust the pipette to measure 50ml and fit the pipette tips.
Add 50ul antigen to every well except wells in column 1. It is advisable that, to avoid contamination, start with wells in column 12 (negative control) and add row by row, and also change the pipette tip every time antigen is taken out of the bottle.
Rotate the plates gently, both clockwise and anticlockwise.
Cover the plates with a spare microtitre plate, leave them on a level surface at room temperature for about 12 to 18 hours.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
41
Reading the DAT results – Day 3
Put the plates against a white background.
Estimate the titre by comparing the dots in column 12 (negative control) to those of the samples in the other columns.
The titre is expressed as the last dilution that shows a difference compared to the negative control. A dark blue dot indicates that the result is negative and no reaction took place whereas a hazy blue mat or cloudy appearance indicates that reaction took place. The highest titre will be last dilution that still shows a hazy blue mat or cloud.
Record the result in the lab book by titer and meaning. For example record well 9, 12800 positive. If you are not sure of the meaning (positive, negative or borderline) simply record the titer. Currently the positive titer is well 7 or 3200 with the FD antigen.
Report the results in the patients’ request form.
The titres are as follows.
Column: 1 2 3 4 5 6 7 8 9 10 11
Dilution: 1:50 1:100 1:200 1:400 1:800 1:1600 1:3200 1:6400 1:12800 1:25600 1:51200
See below an example of positive result:
sample E: well 11, titre 1:51200, positive

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
42
Annex 3. Lymph node aspirate procedure
Collection of lymph node aspirate
The most common site for collection of the lymph node aspirate for diagnosis of kala-azar is the inguinal glands. Infected glands will be swollen.
Method
Items required:
Sterile needle (21G )
Syringe (10ml)
Clean glass slide
Iodine (disinfectant) or sterile cotton swabs
Cotton wool
Procedure
Allow the patient to lie comfortably. Prepare the syringe by pulling the piston back as far as possible.
Feel both sides of the inguinal area to locate a swollen gland.
Disinfect the chosen site with swollen glands using a piece of cotton wool soaked in iodine or suitable disinfectant.
Take the gland between the thumb and index finger of the left hand. Hold it steady, at the same time making it stand out.
Introduce the needle at right angle into the centre of the gland in two stages:-
a) First pierce the skin
b) Second penetrate the gland
With your left hand, gently knead the gland. With your right hand, revolve the needle in both directions. The glandular fluid will ooze into the needle.
Withdraw the needle in one rapid movement, holding the thumb over the hub. Then apply a swab dipped in iodine to the point of entry.
Attach the syringe (piston pulled back) to the needle. Place the needle on the slide. Push the piston gently down the barrel to discharge the glandular fluid contained in the needle onto the slide
Make a thin film using the fluid on the slide. The fluid can be discharged in more than one slide.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
43
Annex 4. Bone marrow aspiration procedures
Materials needed
Sterile BM needle
10 ml syringe
Clean microscope slides
NNN or any other suitable culture medium
Wooden applicator or tooth picks
Spirit lamp with sufficient flame
Drapes
Sterile gloves
Sterile cotton and gauze
Plaster
Labels
Pen and pencil/marker
Biopsy aspiration needles (recommended sizes):
Regular/Adults: 4-inch, 11-gauge
Adults: 4-inch, 8-gauge
Orthopaedic: 6-inch, 10/11-gauge
Paediatric: 3 ½ -inch, 13-gauge
Infant: 2-inch, 13-gauge
Pre-operative procedures
No specific procedures are needed.
Aspiration procedures
1. Place the patient in a right or left lateral decubitus position with the back comfortably flexed and the top knee drawn toward the chest.
2. Locate the posterior iliac spine and mark with ink or thumb nail pressure
3. Using sterile technique, prepare the skin with anti-septics and drape
4. Using sterile syringe, apply/infiltrate the marked area with local anaesthetic especially the periosteum
5. Make a 3-mm skin incision with a scalpel blade over the marked area.
6. Hold the needle with the proximal end in the palm and the index finger against the shaft near the tip.
7. With the stylet locked in place, introduce the needle through the incision pointing toward the anterior superior iliac spine and bring it into contact with the posterior iliac spine.
8. Using gentle but firm pressure, advance the needle to bore through the iliac spine.
9. Rotate the needle in an alternating clock-wise and counter-clockwise motion. Entrance into the marrow cavity is generally detected by decreased resistance.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
44
10. Remove the stylet, and check for presence/absence of marrow material. If not, proceed to bore until marrow is found in the tips of the stylet.
11. With a syringe locked into the proximal portion, apply a negative pressure.
12. The material can then be expelled on to clean slides and also inoculated into appropriate culture medium (preferably NNN medium)
N.B. For cultures, insert needle into a tube containing culture medium and push the plunger into the barrel to expel contents of the needle on to the side walls of the tube or directly into the liquid phase of the medium. You may repeat this once or twice until the LN material is visible in the tube. For safety purposes, inoculate 2 culture tubes.
For smears, expel any remaining material gently on clean glass slides holding tip of needle on the surface of slide, and spread evenly into a smear immediately using a linear motion. More material can be obtained at the end of the plunger or the needle (or tip of syringe) after removing the plunger and needle. Tooth picks or wooden applicators may be used for this purpose. It is important that culture tubes are not over loaded by large amounts of inoculum, which is not uncommon with BM aspirates.
13. Slides can be stained with Leishman, Giemsa or Wright’s stain (See Annex 4). NNN cultures should be incubated at 25
0C for up to 2 weeks.
Post-operative procedures
No specific procedures are needed

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
45
Annex 5. Procedures for splenic aspiration
Splenic aspiration should be performed only if the following conditions are met:
absence of clinical contraindication(s): - signs of active bleeding (e.g. epistaxis, rectal bleeding, skin bruises)
- jaundice (a potential marker of liver dysfunction) - pregnancy - spleen barely palpable - bad general condition (e.g. cardiovascular shock, altered consciousness)
absence of biological contraindication(s): - severe anaemia (haemoglobin count ≤ 5 g/l) - difference in prothrombin time between patient and control > 5 s - platelet count < 40 000/ml
rapid access to blood transfusion in case of bleeding
The two important prerequisites for the safety of the procedure are rapidity, so that the needle remains within the spleen for less than l s; and precision, so that the entry and exit axes of the aspirating needle are identical to avoid tearing the splenic capsule.
The procedure is as follows:
1. Clean three glass slides and label them with patient´s name, date and the words ‘splenic aspirate’. Have culture medium ready (if available) and labelled in the same way as the slides. Attach a 1
1/4-inch 21-gauge (32 0.8-mm) needle to a 5-ml syringe. Place all
items on a table at the bedside.
2. Inform the patient about the procedure. Check all clinical and biological contraindications again. Palpate the spleen and outline its margins on the patient´s abdomen with a pen. For safety, the spleen should be palpable at least 3 cm below the costal margin on expiration. Use an alcohol swab to clean the skin at the site of aspiration, and allow the skin to dry.
3. With the 21-gauge (0.8-mm) needle attached to the 5-ml syringe, just penetrate the skin, midway between the edges of the spleen, 2–4 cm below the costal margin. Aim the needle cranially at an angle of 45° to the abdominal wall. The actual aspiration is done as follows: pull the syringe plunger back to approximately the 1-ml mark to apply suction, and with a quick in-and-out movement push the needle into the spleen to the full needle depth and then withdraw it completely, maintaining suction throughout.
4. For young, restless children, have two assistants hold the child (arms folded across the chest, with shirt raised to obstruct the line of vision, and pelvis held firmly). Carry out the aspiration as a single-stage procedure, using the same landmarks, angles and suction as in step 3, all in one quick motion. The insertion should be timed with the patient´s breathing so that the diaphragm is not moving; this should be done during fixed expiration if the child is crying. Only a minute amount of splenic material is obtained, but this is sufficient for culture and smear.
5. If culture is available: slowly pull the plunger back to the 2–3-ml mark, and, using sterile techniques, insert the needle into a tube containing culture medium and briskly push the plunger into the barrel to expel the contents of the needle onto the side walls of the tube. lf necessary, repeat once or twice until splenic material is visible in the tube. Replace the cap on the tube and invert to wash splenic material on the side of the tube. Repeat the procedure for the second tube of culture medium. Sterile techniques are essential throughout.
6. Expel material (or additional material if culture is available) gently onto glass slides, holding the needle tip on the surface of the slide. Immediately spread evenly with the needle, using a linear (not circular) motion. The smear should be slightly thinner than a

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
46
thick blood film for malaria. Remove the needle, and use the end of it to obtain additional material from the tip of the syringe and spread it on slides. Further material found on the end of the plunger may be dabbed directly onto a slide and spread. Allow the slides to dry.
7. Write the time of aspiration on the patient´s chart, with the instructions: "Record pulse and blood pressure every half hour for 4 h, then every hour for 6 h. Patient must remain in bed for 12 h." Ensure that the patient understands the instructions. Enter the procedure in the notes, and sign.
8. Take the slides (and medium) to the laboratory for preparation and microscopic examination.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
47
Annex 6. Preparation and examination of aspirates. Grading of parasites
Preparation of the aspirates
Prepare thin films of the splenic aspirate material or lymph gland fluid.
Spread the films on a clean glass slide immediately after collection, before the material clots.
Slides are stained with Giemsa as for a thin malaria film and examined under oil immersion
Items required:
Methanol
Glass slide
Slide rack
Giemsa
Buffer solution pH 7.2
Microscope
Thin films
Collect a drop of the aspirate/fluid on one end of the slide; about 1-2 cm from one end.
Place the slide horizontally on a flat surface.
Hold the sides of second slide (spreader) or coverslip on to the center of the specimen slide and move it backwards until it touches the drop of the fluid. Let the fluid spread along its base.
At an angle of between 30-450, move the spreader firmly and steadily across the specimen slide to make a film. A good film should have a conical ‘tail’ and should cover about two-thirds of the slide.
Let the film dry.
Fix the dried smear by dipping in absolute methanol for a few seconds and allow to air-dry on a drying/draining rack.
Fixation
Place the slides horizontally on the slides rack and leave to air dry.
Fix the slides by dipping them in 100% methanol for 1minute. The methanol must be stored in a tightly closed bottle to prevent absorption of water.
Staining:
Stain the slides with Giemsa stain 1: 10 concentration; 1ml of stock Giemsa stain to 9ml buffer solution pH 7.2. The slides can either be stained in a staining trough or on a staining rack.
Staining in trough
Place the slides in a staining trough
Pour the stain gently into the trough until the slides are totally covered. Avoid pouring the stain directly onto the film
Leave the slides to stain for 10 - 15 minutes.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
48
Pour clean water into the trough to float off the scum on the surface of the stain. The water should be poured into the end of the trough.
Gently pour off the stain and rinse again in clean water. Then pour off the water.
Remove the slides one by one and place them in vertical position on a slides rack to dry
Staining on a rack
Use a test tube or a small container to hold the prepared stain
Gently pour the stain onto the slide or use a pipette to drop the stain on to the slide
Leave the slides to stain for 10 – 15 minutes
Gently flush the stain off the slide by adding drops of clean water. Never pour the stain off the slides, otherwise the surface scum will stick to the film and spoil if for microscopic examination
Place the slides in vertical position on a slides rack to dry
Microscopic examination of stained aspirates
Method
Place the microscope on a firm bench, free from vibration.
Switch on the light source. If there is no inbuilt light source, adjust the flat side of the mirror to reflect the light up through the condenser.
Adjust the eyepieces by sliding them horizontally until they fit both eyes comfortably and the two fields merge.
Centre the condenser if applicable.
Prepare the slide for examination by putting a drop of oil immersion on the smear.
Clean and dry underneath of the slide by wiping with cotton gauze/wool or tissue paper.
Rotate the nosepiece until the low power objective is in position (x10). A slight resistance and a click are felt as the objective moves to the correct position.
Place the slide carefully on the stage. Never place the slide on the stage when the x40 or x100 (oil immersion) objectives are in position as this may scratch the lenses.
Adjust the illumination.
Focus the specimen by racking the stage up to the top and then while observing through the eyepiece, rack the stage down slowly using the coarse adjustment knob, until the image comes into view. Use the fine adjustment knob to focus the image sharply. Scan the film and select a part that is well stained, free of staining debris and well populated with white blood cells.
Swing the required objective into position i.e. oil immersion (x100) objective. Focus using the fine adjustment knob. Never use the coarse adjustment knob because the objectives are perfocal.
Adjust the illumination by opening the iris diaphragm as required, for oil immersion objective open the iris diaphragm fully.
Examine the specimen systematically, moving from field to field using the knobs that control the mechanical stage. For example, start at the selected site and move horizontally to the top right hand corner. Move the slide down by one field and then horizontally in the other direction to the end of the smear. Continue until the whole specimen has been examined.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
49
After examination, lower the stage or swing the lowest power objective into position before removing the slide from the stage. Never remove the slide from the stage when x40 or x100 objectives are in position, as this may scratch the lenses.
Wipe the oil immersion objective using lens cleaning tissue.
Switch off the microscope.
Identification of the Leishmania parasite
Leishmania amastigotes are oval or round and are usually seen in the cytoplasm of monocytes. Free parasites may be seen if the host cells are ruptured during preparation of the film. In stained preparations, Leishmania amastigotes contain two visible structures:
Nucleus
Kinetoplast
The nucleus and kinetoplast stain dark reddish. The cytoplasm stains pale pink. The nucleus of the host cell may be pushed to one side by the multiplying parasites.
Leishmania amastigotes are sometimes referred to as L.D. bodies.
Free amastigotes Intra-cellular amastigotes
If Leishmania amastigotes are seen, report the slide as:
Lymphnode or splenic aspirate: Leishmania amastigotes seen and indicate the grade.
Examine at least 1000 fields before declaring a film to be negative.
Grading of slides
Parasite grading has several uses. It increases the sensitivity of parasite detection, provides an objective measure of the speed of response to treatment, distinguishes quickly between slow responders and nonresponders, and provides an indication of parasite load that is useful in research.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
50
The average amastigote density is graded as follows:1
6+: > 100 parasites per field (viewed with a 10 eyepiece and 100 oil-immersion lens)
5+: 10–100 parasites per field
4+: 1–10 parasites per field
3+: 1–10 parasites per 10 fields
2+: 1–10 parasites per 100 fields
1+: 1–10 parasites per 1000 fields
0: 0 parasite per 1000 fields
Parasite grading has several uses. It increases the sensitivity of parasite detection, provides an objective measure of the speed of response to treatment, distinguishes quickly between slow responders and nonresponders, and provides an indication of parasite load that is useful in research.
1 Adapted from Chulay JD, Bryceson AD. Quantitation of amastigotes of Leishmania donovani in smears of
splenic aspirates from patients with visceral leishmaniasis. American Journal of Tropical Medicine and
Hygiene, 1983; 32:475–9.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
51
Annex 7. Kala-azar laboratory register book (left page)
Patient information Patient origin
Serial No. Date Name Age Sex Region District Village/ Town Patient category

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
52
Kala-azar laboratory register book (right page)
Laboratory results Reference laboratory results
rapid test (rk39) DAT LN aspirate BM aspirate SP aspirate
Date DAT
samples sent to
Ref. Lab
Date DAT results
received from Ref.
Lab
Ref. Lab DAT
results COMMENT
DAT = direct agglutination test
LN = lymph node
BM = bone marrow
SP = spleen
Aspirate results:
+ (scarcely positive)
++ (moderately positive)
+++ (highly positive)
- (negative)
ND (not done)

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
53
Annex 8. Kala-azar treatment register book (left page)
Patient information Patient origin
Admission No. Date Patient Name Age Sex Region District Village/ Town
No. of months
sick before
treatment

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
54
Kala-azar treatment register book (right page)
Laboratory tests Treatment
Date Test type Result Patient
category Pregnancy
Treatment
start date Medication
Adverse side
effects
Treatment
end date
Treatment
outcome Comment
Test type: RDT (rapid diagnostic test)/ DAT (direct agglutination test)/ Aspirate (LN/ BM/ SP)
Patient category: NC (New Case)/ PDKL (Post Kalaazar Dermal Leishmaniasis)/ R (Relapse)
Pregnancy: Y (yes)/ N (no)/ NA (not known)
Treatment outcome: discharged/default/referred/died

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
55
Annex 9. Kala-azar patient treatment card (front)

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
56
Kala-azar patient treatment card (back)

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
57
Annex 10. Kala-azar patient discharge card
NAME:_______________________________NO:_____
AGE:_______ SEX: M F
VILLAGE:_____________________
DISTRICT____________________
1oKA RELAPSE-KA PKDL
SSG/Glucantime PAROMO AMBISOME
Other drugs (specify)
ADMISSION DATE:
DISCHARGE DATE:
Weight: SPLEEN: LIVER:
TOC:

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
58
Annex 11. Dosage and precautions for the use of sodium stibogluconate (SSG)
Presentation:
Solution for injection, vials 30ml.
Contains 33% (= 9.9g/30ml) SSG corresponding to 10% Sb5+
which is 100mg Sb5+
/1ml or 3000mg Sb
5+/30ml.
Table of SSG volume per body weight (20mg Sb5+
/kg/day)
Weight in
kg
SSG dose in ml Weight in
kg
SSG dose in ml Weight in
kg
SSG dose in ml
1 2 26 5.2 51 10.2
2 2 27 5.4 52 10.4
3 2 28 5.6 53 10.6
4 2 29 5.8 54 10.8
5 2 30 6 55 11
6 2 31 6.2 56 11.2
7 2 32 6.4 57 11.4
8 2 33 6.6 58 11.6
9 2 34 6.8 59 11.8
10 2 35 7 60 12
11 2.2 36 7.2 61 12.2
12 2.4 37 7.4 62 12.4
13 2.6 38 7.6 63 12.6
14 2.8 39 7.8 64 12.8
15 3 40 8 65 13
16 3.2 41 8.2 66 13.2
17 3.4 42 8.4 67 13.4
18 3.6 43 8.6 68 13.6
19 3.8 44 8.8 69 13.8
20 4 45 9 70 14
21 4.2 46 9.2 71 14.2
22 4.4 47 9.4 72 14.4
23 4.6 48 9.6 73 14.6
24 4.8 49 9.8 74 14.8
25 5 50 10 75 15
No upper limit for SSG!! If the patient’s weight is higher than 75 then calculate accordingly.
Contraindications
There are no absolute contraindications to its use - but under ideal circumstances patients with underlying renal, hepatic or cardiac disease should be well monitored. Elder may have age related decreased kidney function so may be at risk of increased toxicity..

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
59
Toxicity and side effects
Prevention of SSG toxicity:
The most important way to prevent SSG accumulation between doses is to ensure adequate hydration. SSG is cleared in the urine. Patients should repeatedly be told to drink enough fluids so they pass urine at least 4 times a day. Babies should pass urine every hour or so while awake.
Minor side effects:
Symptoms: nausea, anorexia, arthralgias, myalagias, injection site pain, fatigue, and abdominal pain.
Laboratory toxicity: elevated amylase (biochemical pancreatitis), elevated liver enzymes (biochemical hepatitis), leukopenia / anaemia / thrombocytopenia. Occasionally, renal failure occurs.
Electrocardiograph changes (ST segment and T wave).
Nausea and anorexia are substantial problems where patients are already malnourished and dehydrated. The nausea and anorexia subside somewhat in the later weeks of treatment.
Serious toxicity:
Severe vomiting and abdominal pain (pancreatitis?): Vomiting is relatively common and should be treated aggressively. Treat with anti-emetic medications, and push sips of fluids. When anti-emetic treatment fails the SSG should be withheld for 2 to 5 days as needed.
If vomiting is associated with other risk factors especially extremes of age, low Hb, severe malnutrition, withholding of SSG is even more imperative.
In hospitals with chemistry available, patients vomiting from known pancreatitis also should get SSG withheld. Note that when the pancreatic enzymes return to normal and the patient is re-challenged with SSG, the amylase may remain normal.
Electrocardiograph abnormalities (QT prolongation), and sudden death (rare): Sudden death occurs rarely - possible explanations are cardiac arrhythmias or intra-cerebral bleeds. ECG changes are common. Sudden death is associated with high doses of SSG (over 30mg/kg/day). However, cardiotoxicity and sudden deaths are not seen in PKDL patients, so toxicity may be a combination of SSG and a weak individual.
Other points of interest:
Blindness is NOT a toxicity of SSG - if a patient complains of loss of vision after treatment then it could be iritis (which can occur in isolation or with PKDL) and this iritis requires further treatment with SSG. Apparently retinal haemorrhages occur with KA (not associated with SSG) as well.
Injection abscesses from the IM route have been uncommon - but when present need aggressive treatment (antibiotics, drainage of pus).
Neurological toxicity: not reported elsewhere as a toxic effect of SSG. Before or during treatment some patients have ataxia and severe tremors with or without headache. Neuropathy, psychosis and epilepsy are other occasional neurological features. It is unclear whether any of these are an effect of SSG in patients with KA (it never occurs in patients undergoing treatment for PKDL), if it is KA itself, or if it represents bleeding into areas of the brain. The ataxia, tremor and neuropathy may all remain for months after cure.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
60
Annex 12. Dosage and precautions for the use of paromomycin (aminosidine).
Presentation
Solution for injection vials of 500 mg/ml, 2 ml (1 gr).
Table of paromomycin (PM) volume per body weight (15mg/kg/day)
Weight in
kg
PM dose in ml Weight in
kg
PM dose in ml Weight in
kg
PM dose in ml
1 0.03 26 0.78 51 1.53
2 0.06 27 0.81 52 1.56
3 0.09 28 0.84 53 1.59
4 0.12 29 0.87 54 1.62
5 0.15 30 0.9 55 1.65
6 0.18 31 0.93 56 1.68
7 0.21 32 0.96 57 1.71
8 0.24 33 0.99 58 1.74
9 0.27 34 1.02 59 1.77
10 0.3 35 1.05 60 1.8
11 0.33 36 1.08 61 1.83
12 0.36 37 1.11 62 1.86
13 0.39 38 1.14 63 1.89
14 0.42 39 1.17 64 1.92
15 0.45 40 1.2 65 1.95
16 0.48 41 1.23 66 1.98
17 0.51 42 1.26 67 2.01
18 0.54 43 1.29 68 2.04
19 0.57 44 1.32 69 2.07
20 0.6 45 1.35 70 2.1
21 0.63 46 1.38 71 2.13
22 0.66 47 1.41 72 2.16
23 0.69 48 1.44 73 2.19
24 0.72 49 1.47 74 2.22
25 0.75 50 1.5 75 2.25
Toxicity and side effects
PM is an aminoglycoside and as such has renal and oto-toxicity. The toxic effects of SSG and PM do not overlap.
Oto-toxicity: All aminoglycosides can cause damage to hearing and balance. PM is probably less toxic than streptomycin, amikacin or gentamicin. PM should be avoided in patients who complain of deafness before treatment – this occasionally occurs in KA.
Renal toxicity: Renal toxicity is increased in patients who are dehydrated, hypokalemic [= low serum potassium - e.g. patients with vomiting or profuse diarrhea], or who have underlying renal impairment. All patients should be encouraged to remain orally well hydrated when on PM or SSG. Patients should be told to drink until they have passed urine at

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
61
least 4 times a day; babies should pass urine about each hour. Old patients are more vulnerable to renal toxicity.
Pregnancy: Like streptomycin, PM could theoretically affect the hearing of the newborn. The survival benefits of PM in pregnant women in Somalia are thought to out-weigh this theoretical risk.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
62
Annex 13. Dosage, administration and precautions for meglumine antimoniate.
Dosage
Meglumine antimoniate and sodium stibogluconate are the pentavalent antimony (Sb5+
) compounds used to treat leishmaniasis;
Meglumine antimoniate is commercialized by SANOFI-AVENTIS as solution for injection in 5ml ampoules (Glucantime®) containing 405mg of pentavalent antimony (Sb
5+), it means
81mg of Sb5+
/1 ml. The dose of meglumine antimoniate is based on the amount of pentavalent antimony the presentation contains and is 20mg/kg/day.
The minimum dose is 2ml (162mg) for children weighing less than 10 kg.
Weight
in kg
Meglumine
antimoniate dose in
ml
Weight in
kg
Meglumine
antimoniate dose in
ml
Weight in
kg
Meglumine
antimoniate dose in
ml
< 10 2 34 8.4 59 14.6
10 2.6 35 8.6 60 14.8
11 2.8 36 9.0 61 15.0
12 3.0 37 9.2 62 15.4
13 3.2 38 9.4 63 15.6
14 3.4 39 9.6 64 15.8
15 3.8 40 9.8 65 16.0
16 4.0 41 10.2 66 16.2
17 4.2 42 10.4 67 16.6
18 4.4 43 10.6 68 16.8
19 4.8 44 10.8 69 17.0
20 5.0 45 11.2 70 17.2
21 5.2 46 11.4 71 17.6
22 5.4 47 11.6 72 17.8
23 5.8 48 11.8 73 18.0
24 6.0 49 12.2 74 18.2
25 6.2 50 12.4 75 18.6
26 6.4 51 12.6 76 18.8
27 6.6 52 12.8 77 19.0
28 7.0 53 13.0 78 19.4
29 7.2 54 13.4 79 19.6
30 7.4 55 13.6 80 19.8
31 7.6 56 13.8 >80 20
32 8.0 57 14.0
33 8.2 58 14.4

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
63
Table of Meglumine antimoniate volume of injection to give 20mg/kg/day
Route of administration
Intravenous or intramuscular.
Sb5+
pharamcokinetics are almost identical by the IM and IV routes. Choice of IV or IM depends on the setting. IM is most logical in the bush. The drug may be given by deep intramuscular injection. Consider also the big volume that should be injected (if the volume of injection exceeds 10 ml, it should be divided in 2 doses: one in each buttock or thigh). During a polio outbreak consider giving all the children less than 3 years of age IV injections (IM injections increase the rate of paralytic disease in those incubating with polio). IV is much less painful. It should be given slowly = over 5-10 minutes or longer, using a small butterfly style needles. Other possibility is to dilute the drug in 5% glucose solution 500 ml in adults and give it slowly (30min-1hour). In children between 10–25 kg body weight use 100 ml and if less than 10 kg use 50 ml.
Contra-indications
Severe cardiac, liver and kidney disorders and breastfeeding.
Precautions
The risk of serious, even fatal, toxicity of pentavalent antimonials is increased in patients who concomitantly present with: cardiac disease, in particular arrhythmia; renal failure, liver disease, severe malnutrition/severely impaired general condition; advanced HIV infection; pregnancy. If one of these conditions are present, provide protein-rich diet and a good hydration throughout treatment and, if possible, correct iron and other nutritional deficiencies; renal and hepatic impairment; monitor cardiac, renal and hepatic function; treat concomitant infection (for example pneumonia), and check regularly the patient (ECG and renal, liver, pancreatic function). And if possible an alternative drug should be used.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
64
Annex 14. Anthropometry and nutrition therapy look-up tables.
Look-up table for inpatient care of severely malnourished individuals, for breastfed infants and older children, adolescents and adults
Phase 1 Transition phase
Transition
phase Phase 2
F75 F100 Plumpy'nut F100
Class of weight
(Kg)
8 feeds
per day
6 feeds
per day
8 feeds
per day
6 feeds
per day
6 feeds per
day
6 feeds
per day
ml per feed
ml per feed
sachets per
day
ml per
feed
2 – 2.1 40 50
F100
diluted
F100
diluted
F100 diluted
F100
diluted
2.2 – 2.4 45 60
2.5 – 2.7 50 65
2.8 – 2.9 55 70
3.0 – 3.4 60 75 60 75 1 ¼ 110
3.5 – 3.9 65 80 65 80
1 ½
120
4.0 – 4.4 70 85 70 85 150
4.5 – 4.9 80 95 80 95
5.0 – 5.4 90 110 90 110
2
180
5.5 – 5.9 100 120 100 120
6 – 6.9 110 140 110 140 210
7 – 7.9 125 160 125 160
3
240
8 – 8.9 140 180 140 180 270
9 – 9.9 155 190 155 190 300
10 – 10.9 170 200 170 200
4
350
11 – 11.9 190 230 190 230
12 – 12.9 205 250 205 250
450 13 – 13.9 230 275 230 275
14 – 14.9 250 290 250 290
15 – 19.9 260 300 260 300 5 550
20 – 24.9 290 320 290 320 6
650
25 – 29.9 300 350 300 350 750
30 – 39.9 320 370 320 370 7 850
40 – 60 350 400 350 400 8 1000

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
65
Look-up table for therapeutic milk amounts to be given to infants without the prospect of being breastfed
Diluted F100 or F75
(kwash) Dilute F100 Diluted F100
Class of Weight (kg) 8 feeds per day 8 feeds per day 6 to 8 feeds per day
ml per feed ml per feed ml per feed
Below 1.5 30 45 60
1.6–1.8 35 53 70
1.9–2.1 40 60 80
2.2 –2.4 45 68 90
2.5–2.7 50 75 100
2.8–2.9 55 85 110
3.0–3.4 60 90 120
3.5–3.9 65 98 130
4.0–4.4 140
Look-up table for amounts of RUTF to give to a child per day or week based on a dose of 200 kcal/kg bodyweight/day using 92 g packets containing 500 kcal
Weight of
the child
Packets
per day
Packets
per 1 week
3.5 – 3.9 1.5 11
4.0 – 5.4 2 14
5.5 – 6.9 2.5 18
7.0 – 8.4 3 21
8.5 – 9.4 3.5 25
9.5 – 10.4 4 28
10.5 – 11.9 4.5 32
>= 12 5 35

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
66
Appetite test
For children meeting the anthropometric criteria for admission for treatment of SAM, the appetite test, in addition to the
presence or absence of severe medical complications, forms one of the most important criteria for deciding whether to
treat a child with SAM in outpatient care or inpatient care.
The pathophysiological responses to nutrient depletion in children with SAM are such that liver and metabolic functions
are disturbed and dysfunctional, leading to poor appetite. In addition, children with a significant infection also lose
appetite, especially in the acute phase. This puts children with SAM with poor appetite at higher risk of death.
The appetite is tested upon admission and is repeated at each follow-up visit to the health facility.
Points to consider when conducting an appetite test:
Conduct the appetite test in a quiet separate area.
Provide an explanation regarding the purpose of the test to the caregiver and describe the procedure.
Observe the child eating the RUTF during 30 minutes, and decide if the child passes or fails the test.
Advise the caregiver to:
o Wash hands before giving the RUTF
o Sit with the child in lap and gently offer the RUTF
o Encourage the child to eat the RUTF without force-feeding
o Offer plenty of clean water to drink from a cup when child is eating the RUTF
Appetite test:
Pass Appetite Test Fail Appetite Test
The child eats at least one third of a packet of
RUTF (92 g) or three teaspoons from a pot.
The child does NOT eat one third of a packet of
RUTF (92 g) or three teaspoons from a pot.
Note: If necessary, arrange a quiet corner where the child and caregiver can take their time to get accustomed to
eat the RUTF. Usually the child eats the RUTF in 30 minutes.
A child who fails the appetite test should be admitted to inpatient care.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
67
Transition phase look-up table for amounts of RUTF to give to a child per day based on a dose of 150
kcal/kg bodyweight/day using 92 g packets containing 500 kcal
Child’s Weight (kg) Packets per Day
3.5 – 3.9 1.2
4.0 – 4.9 1.5
5.0 – 6.9
Anthropometry Look-Up
Tables 2.1
7.0 – 8.4 2.5
8.5 – 9.4 2.8
9.5 – 10.4 3.1
10.5 – 11.9 3.6
12 4
Weight-for-length look-up table, children 6–23 months, WHO 2006 child growth standards
Boys' Weight (kg) Length a Girls' Weight (kg)
-3 SD -2 SD -1 SD Median (cm) Median -1 SD -2 SD -3 SD
1.9 2.0 2.2 2.4 45 2.5 2.3 2.1 1.9
2.0 2.2 2.4 2.6 46 2.6 2.4 2.2 2.0
2.1 2.3 2.5 2.8 47 2.8 2.6 2.4 2.2
2.3 2.5 2.7 2.9 48 3.0 2.7 2.5 2.3
2.4 2.6 2.9 3.1 49 3.2 2.9 2.6 2.4
2.6 2.8 3.0 3.3 50 3.4 3.1 2.8 2.6
2.7 3.0 3.2 3.5 51 3.6 3.3 3.0 2.8
2.9 3.2 3.5 3.8 52 3.8 3.5 3.2 2.9
3.1 3.4 3.7 4.0 53 4.0 3.7 3.4 3.1
3.3 3.6 3.9 4.3 54 4.3 3.9 3.6 3.3
3.6 3.8 4.2 4.5 55 4.5 4.2 3.8 3.5
3.8 4.1 4.4 4.8 56 4.8 4.4 4.0 3.7
4.0 4.3 4.7 5.1 57 5.1 4.6 4.3 3.9
4.3 4.6 5.0 5.4 58 5.4 4.9 4.5 4.1
4.5 4.8 5.3 5.7 59 5.6 5.1 4.7 4.3
4.7 5.1 5.5 6.0 60 5.9 5.4 4.9 4.5
4.9 5.3 5.8 6.3 61 6.1 5.6 5.1 4.7
5.1 5.6 6.0 6.5 62 6.4 5.8 5.3 4.9
5.3 5.8 6.2 6.8 63 6.6 6.0 5.5 5.1
5.5 6.0 6.5 7.0 64 6.9 6.3 5.7 5.3
5.7 6.2 6.7 7.3 65 7.1 6.5 5.9 5.5
5.9 6.4 6.9 7.5 66 7.3 6.7 6.1 5.6
6.1 6.6 7.1 7.7 67 7.5 6.9 6.3 5.8
6.3 6.8 7.3 8.0 68 7.7 7.1 6.5 6.0
6.5 7.0 7.6 8.2 69 8.0 7.3 6.7 6.1
6.6 7.2 7.8 8.4 70 8.2 7.5 6.9 6.3
6.8 7.4 8.0 8.6 71 8.4 7.7 7.0 6.5
7.0 7.6 8.2 8.9 72 8.6 7.8 7.2 6.6
7.2 7.7 8.4 9.1 73 8.8 8.0 7.4 6.8
7.3 7.9 8.6 9.3 74 9.0 8.2 7.5 6.9
7.5 8.1 8.8 9.5 75 9.1 8.4 7.7 7.1
7.6 8.3 8.9 9.7 76 9.3 8.5 7.8 7.2
7.8 8.4 9.1 9.9 77 9.5 8.7 8.0 7.4
7.9 8.6 9.3 10.1 78 9.7 8.9 8.2 7.5

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
68
Boys' Weight (kg) Length a Girls' Weight (kg)
-3 SD -2 SD -1 SD Median (cm) Median -1 SD -2 SD -3 SD
8.1 8.7 9.5 10.3 79 9.9 9.1 8.3 7.7
8.2 8.9 9.6 10.4 80 10.1 9.2 8.5 7.8
8.4 9.1 9.8 10.6 81 10.3 9.4 8.7 8.0
8.5 9.2 10.0 10.8 82 10.5 9.6 8.8 8.1
8.7 9.4 10.2 11.0 83 10.7 9.8 9.0 8.3
8.9 9.6 10.4 11.3 84 11.0 10.1 9.2 8.5
9.1 9.8 10.6 11.5 85 11.2 10.3 9.4 8.7
9.3 10.0 10.8 11.7 86 11.5 10.5 9.7 8.9
9.5 10.2 11.1 12.0 87 11.7 10.7 9.9 9.1
9.7 10.5 11.3 12.2 88 12.0 11.0 10.1 9.3
9.9 10.7 11.5 12.5 89 12.2 11.2 10.3 9.5
10.1 10.9 11.8 12.7 90 12.5 11.4 10.5 9.7
10.3 11.1 12.0 13.0 91 12.7 11.7 10.7 9.9
10.5 11.3 12.2 13.2 92 13.0 11.9 10.9 10.1
10.7 11.5 12.4 13.4 93 13.2 12.1 11.1 10.2
10.8 11.7 12.6 13.7 94 13.5 12.3 11.3 10.4
11.0 11.9 12.8 13.9 95 13.7 12.6 11.5 10.6
11.2 12.1 13.1 14.1 96 14.0 12.8 11.7 10.8
11.4 12.3 13.3 14.4 97 14.2 13.0 12.0 11.0
11.6 12.5 13.5 14.6 98 14.5 13.3 12.2 11.2
11.8 12.7 13.7 14.9 99 14.8 13.5 12.4 11.4
12.0 12.9 14.0 15.2 100 15.0 13.7 12.6 11.6
a Length is measured for children under 2 years or less than 87 cm height. For children 2 years or older or 87 cm height or
greater, height is measured. Recumbent length is, on average, 0.7 cm greater than standing height; although the difference is
of no importance to individual children, a correction may be made by subtracting 0.7 cm from all lengths above 86.9 cm if
standing height cannot be measured.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
69
Weight-for-height look-up table, children 24–59 months, WHO 2006 child growth standards
Boys' Weight (kg) Height a Girls' Weight (kg)
-3 SD -2 SD -1 SD Median (cm) Median -1 SD -2 SD -3 SD
5.9 6.3 6.9 7.4 65 7.2 6.6 6.1 5.6
6.1 6.5 7.1 7.7 66 7.5 6.8 6.3 5.8
6.2 6.7 7.3 7.9 67 7.7 7.0 6.4 5.9
6.4 6.9 7.5 8.1 68 7.9 7.2 6.6 6.1
6.6 7.1 7.7 8.4 69 8.1 7.4 6.8 6.3
6.8 7.3 7.9 8.6 70 8.3 7.6 7.0 6.4
6.9 7.5 8.1 8.8 71 8.5 7.8 7.1 6.6
7.1 7.7 8.3 9.0 72 8.7 8.0 7.3 6.7
7.3 7.9 8.5 9.2 73 8.9 8.1 7.5 6.9
7.4 8.0 8.7 9.4 74 9.1 8.3 7.6 7.0
7.6 8.2 8.9 9.6 75 9.3 8.5 7.8 7.2
7.7 8.4 9.1 9.8 76 9.5 8.7 8.0 7.3
7.9 8.5 9.2 10.0 77 9.6 8.8 8.1 7.5
8.0 8.7 9.4 10.2 78 9.8 9.0 8.3 7.6
8.2 8.8 9.6 10.4 79 10.0 9.2 8.4 7.8
8.3 9.0 9.7 10.6 80 10.2 9.4 8.6 7.9
8.5 9.2 9.9 10.8 81 10.4 9.6 8.8 8.1
8.7 9.3 10.1 11.0 82 10.7 9.8 9.0 8.3
8.8 9.5 10.3 11.2 83 10.9 10.0 9.2 8.5
9.0 9.7 10.5 11.4 84 11.1 10.2 9.4 8.6
9.2 10.0 10.8 11.7 85 11.4 10.4 9.6 8.8
9.4 10.2 11.0 11.9 86 11.6 10.7 9.8 9.0
9.6 10.4 11.2 12.2 87 11.9 10.9 10.0 9.2
9.8 10.6 11.5 12.4 88 12.1 11.1 10.2 9.4
10.0 10.8 11.7 12.6 89 12.4 11.4 10.4 9.6
10.2 11.0 11.9 12.9 90 12.6 11.6 10.6 9.8
10.4 11.2 12.1 13.1 91 12.9 11.8 10.9 10.0
10.6 11.4 12.3 13.4 92 13.1 12.0 11.1 10.2
10.8 11.6 12.6 13.6 93 13.4 12.3 11.3 10.4
11.0 11.8 12.8 13.8 94 13.6 12.5 11.5 10.6
11.1 12.0 13.0 14.1 95 13.9 12.7 11.7 10.8
11.3 12.2 13.2 14.3 96 14.1 12.9 11.9 10.9
11.5 12.4 13.4 14.6 97 14.4 13.2 12.1 11.1
11.7 12.6 13.7 14.8 98 14.7 13.4 12.3 11.3
11.9 12.9 13.9 15.1 99 14.9 13.7 12.5 11.5
12.1 13.1 14.2 15.4 100 15.2 13.9 12.8 11.7
12.3 13.3 14.4 15.6 101 15.5 14.2 13.0 12.0
12.5 13.6 14.7 15.9 102 15.8 14.5 13.3 12.2
12.8 13.8 14.9 16.2 103 16.1 14.7 13.5 12.4
13.0 14.0 15.2 16.5 104 16.4 15.0 13.8 12.6
13.2 14.3 15.5 16.8 105 16.8 15.3 14.0 12.9
13.4 14.5 15.8 17.2 106 17.1 15.6 14.3 13.1
13.7 14.8 16.1 17.5 107 17.5 15.9 14.6 13.4
13.9 15.1 16.4 17.8 108 17.8 16.3 14.9 13.7
14.1 15.3 16.7 18.2 109 18.2 16.6 15.2 13.9
14.4 15.6 17.0 18.5 110 18.6 17.0 15.5 14.2
14.6 15.9 17.3 18.9 111 19.0 17.3 15.8 14.5
14.9 16.2 17.6 19.2 112 19.4 17.7 16.2 14.8
15.2 16.5 18.0 19.6 113 19.8 18.0 16.5 15.1
15.4 16.8 18.3 20.0 114 20.2 18.4 16.8 15.4
15.7 17.1 18.6 20.4 115 20.7 18.8 17.2 15.7
16.0 17.4 19.0 20.8 116 21.1 19.2 17.5 16.0
16.2 17.7 19.3 21.2 117 21.5 19.6 17.8 16.3
16.5 18.0 19.7 21.6 118 22.0 19.9 18.2 16.6
16.8 18.3 20.0 22.0 119 22.4 20.3 18.5 16.9
17.1 18.6 20.4 22.4 120 22.8 20.7 18.9 17.3 a Length is measured for children under 2 years or less than 87 cm height. For children 2 years or older or 87 cm height or
more, height is measured. Recumbent length is, on average, 0.7 cm greater than standing height; although the difference is
of no importance to individual children, a correction may be made by subtracting 0.7 cm from all lengths greater than 86.9
cm if standing height cannot be measured.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
70
BMI look-up tables
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38
95 9.0 9.9 10.8 11.7 12.6 13.5 14.4 15.3 16.2 17.1 18.1 19.0 19.9 20.8 21.7 22.6 23.5 24.4 25.3 26.2 27.1 28.0 28.9 29.8 30.7 31.6 32.5 33.4 34.3 95
96 9.2 10.1 11.1 12.0 12.9 13.8 14.7 15.7 16.6 17.5 18.4 19.4 20.3 21.2 22.1 23.0 24.0 24.9 25.8 26.7 27.6 28.6 29.5 30.4 31.3 32.3 33.2 34.1 35.0 96
97 9.4 10.3 11.3 12.2 13.2 14.1 15.1 16.0 16.9 17.9 18.8 19.8 20.7 21.6 22.6 23.5 24.5 25.4 26.3 27.3 28.2 29.2 30.1 31.0 32.0 32.9 33.9 34.8 35.8 97
98 9.6 10.6 11.5 12.5 13.4 14.4 15.4 16.3 17.3 18.2 19.2 20.2 21.1 22.1 23.0 24.0 25.0 25.9 26.9 27.9 28.8 29.8 30.7 31.7 32.7 33.6 34.6 35.5 36.5 98
99 9.8 10.8 11.8 12.7 13.7 14.7 15.7 16.7 17.6 18.6 19.6 20.6 21.6 22.5 23.5 24.5 25.5 26.5 27.4 28.4 29.4 30.4 31.4 32.3 33.3 34.3 35.3 36.3 37.2 99
100 10.0 11.0 12.0 13.0 14.0 15.0 16.0 17.0 18.0 19.0 20.0 21.0 22.0 23.0 24.0 25.0 26.0 27.0 28.0 29.0 30.0 31.0 32.0 33.0 34.0 35.0 36.0 37.0 38.0 100
101 10.2 11.2 12.2 13.3 14.3 15.3 16.3 17.3 18.4 19.4 20.4 21.4 22.4 23.5 24.5 25.5 26.5 27.5 28.6 29.6 30.6 31.6 32.6 33.7 34.7 35.7 36.7 37.7 38.8 101
102 10.4 11.4 12.5 13.5 14.6 15.6 16.6 17.7 18.7 19.8 20.8 21.8 22.9 23.9 25.0 26.0 27.1 28.1 29.1 30.2 31.2 32.3 33.3 34.3 35.4 36.4 37.5 38.5 39.5 102
103 10.6 11.7 12.7 13.8 14.9 15.9 17.0 18.0 19.1 20.2 21.2 22.3 23.3 24.4 25.5 26.5 27.6 28.6 29.7 30.8 31.8 32.9 33.9 35.0 36.1 37.1 38.2 39.3 40.3 103
104 10.8 11.9 13.0 14.1 15.1 16.2 17.3 18.4 19.5 20.6 21.6 22.7 23.8 24.9 26.0 27.0 28.1 29.2 30.3 31.4 32.4 33.5 34.6 35.7 36.8 37.9 38.9 40.0 41.1 104
105 11.0 12.1 13.2 14.3 15.4 16.5 17.6 18.7 19.8 20.9 22.1 23.2 24.3 25.4 26.5 27.6 28.7 29.8 30.9 32.0 33.1 34.2 35.3 36.4 37.5 38.6 39.7 40.8 41.9 105
106 11.2 12.4 13.5 14.6 15.7 16.9 18.0 19.1 20.2 21.3 22.5 23.6 24.7 25.8 27.0 28.1 29.2 30.3 31.5 32.6 33.7 34.8 36.0 37.1 38.2 39.3 40.4 41.6 42.7 106
107 11.4 12.6 13.7 14.9 16.0 17.2 18.3 19.5 20.6 21.8 22.9 24.0 25.2 26.3 27.5 28.6 29.8 30.9 32.1 33.2 34.3 35.5 36.6 37.8 38.9 40.1 41.2 42.4 43.5 107
108 11.7 12.8 14.0 15.2 16.3 17.5 18.7 19.8 21.0 22.2 23.3 24.5 25.7 26.8 28.0 29.2 30.3 31.5 32.7 33.8 35.0 36.2 37.3 38.5 39.7 40.8 42.0 43.2 44.3 108
109 11.9 13.1 14.3 15.4 16.6 17.8 19.0 20.2 21.4 22.6 23.8 25.0 26.1 27.3 28.5 29.7 30.9 32.1 33.3 34.5 35.6 36.8 38.0 39.2 40.4 41.6 42.8 44.0 45.1 109
110 12.1 13.3 14.5 15.7 16.9 18.2 19.4 20.6 21.8 23.0 24.2 25.4 26.6 27.8 29.0 30.3 31.5 32.7 33.9 35.1 36.3 37.5 38.7 39.9 41.1 42.4 43.6 44.8 46.0 110
111 12.3 13.6 14.8 16.0 17.2 18.5 19.7 20.9 22.2 23.4 24.6 25.9 27.1 28.3 29.6 30.8 32.0 33.3 34.5 35.7 37.0 38.2 39.4 40.7 41.9 43.1 44.4 45.6 46.8 111
112 12.5 13.8 15.1 16.3 17.6 18.8 20.1 21.3 22.6 23.8 25.1 26.3 27.6 28.9 30.1 31.4 32.6 33.9 35.1 36.4 37.6 38.9 40.1 41.4 42.6 43.9 45.2 46.4 47.7 112
113 12.8 14.0 15.3 16.6 17.9 19.2 20.4 21.7 23.0 24.3 25.5 26.8 28.1 29.4 30.6 31.9 33.2 34.5 35.8 37.0 38.3 39.6 40.9 42.1 43.4 44.7 46.0 47.2 48.5 113
114 13.0 14.3 15.6 16.9 18.2 19.5 20.8 22.1 23.4 24.7 26.0 27.3 28.6 29.9 31.2 32.5 33.8 35.1 36.4 37.7 39.0 40.3 41.6 42.9 44.2 45.5 46.8 48.1 49.4 114
115 13.2 14.5 15.9 17.2 18.5 19.8 21.2 22.5 23.8 25.1 26.4 27.8 29.1 30.4 31.7 33.1 34.4 35.7 37.0 38.4 39.7 41.0 42.3 43.6 45.0 46.3 47.6 48.9 50.3 115
116 13.5 14.8 16.1 17.5 18.8 20.2 21.5 22.9 24.2 25.6 26.9 28.3 29.6 30.9 32.3 33.6 35.0 36.3 37.7 39.0 40.4 41.7 43.1 44.4 45.8 47.1 48.4 49.8 51.1 116
117 13.7 15.1 16.4 17.8 19.2 20.5 21.9 23.3 24.6 26.0 27.4 28.7 30.1 31.5 32.9 34.2 35.6 37.0 38.3 39.7 41.1 42.4 43.8 45.2 46.5 47.9 49.3 50.6 52.0 117
118 13.9 15.3 16.7 18.1 19.5 20.9 22.3 23.7 25.1 26.5 27.8 29.2 30.6 32.0 33.4 34.8 36.2 37.6 39.0 40.4 41.8 43.2 44.6 45.9 47.3 48.7 50.1 51.5 52.9 118
119 14.2 15.6 17.0 18.4 19.8 21.2 22.7 24.1 25.5 26.9 28.3 29.7 31.2 32.6 34.0 35.4 36.8 38.2 39.7 41.1 42.5 43.9 45.3 46.7 48.1 49.6 51.0 52.4 53.8 119
120 14.4 15.8 17.3 18.7 20.2 21.6 23.0 24.5 25.9 27.4 28.8 30.2 31.7 33.1 34.6 36.0 37.4 38.9 40.3 41.8 43.2 44.6 46.1 47.5 49.0 50.4 51.8 53.3 54.7 120
121 14.6 16.1 17.6 19.0 20.5 22.0 23.4 24.9 26.4 27.8 29.3 30.7 32.2 33.7 35.1 36.6 38.1 39.5 41.0 42.5 43.9 45.4 46.9 48.3 49.8 51.2 52.7 54.2 55.6 121
122 14.9 16.4 17.9 19.3 20.8 22.3 23.8 25.3 26.8 28.3 29.8 31.3 32.7 34.2 35.7 37.2 38.7 40.2 41.7 43.2 44.7 46.1 47.6 49.1 50.6 52.1 53.6 55.1 56.6 122
123 15.1 16.6 18.2 19.7 21.2 22.7 24.2 25.7 27.2 28.7 30.3 31.8 33.3 34.8 36.3 37.8 39.3 40.8 42.4 43.9 45.4 46.9 48.4 49.9 51.4 53.0 54.5 56.0 57.5 123
124 15.4 16.9 18.5 20.0 21.5 23.1 24.6 26.1 27.7 29.2 30.8 32.3 33.8 35.4 36.9 38.4 40.0 41.5 43.1 44.6 46.1 47.7 49.2 50.7 52.3 53.8 55.4 56.9 58.4 124
125 15.6 17.2 18.8 20.3 21.9 23.4 25.0 26.6 28.1 29.7 31.3 32.8 34.4 35.9 37.5 39.1 40.6 42.2 43.8 45.3 46.9 48.4 50.0 51.6 53.1 54.7 56.3 57.8 59.4 125
126 15.9 17.5 19.1 20.6 22.2 23.8 25.4 27.0 28.6 30.2 31.8 33.3 34.9 36.5 38.1 39.7 41.3 42.9 44.5 46.0 47.6 49.2 50.8 52.4 54.0 55.6 57.2 58.7 60.3 126
127 16.1 17.7 19.4 21.0 22.6 24.2 25.8 27.4 29.0 30.6 32.3 33.9 35.5 37.1 38.7 40.3 41.9 43.5 45.2 46.8 48.4 50.0 51.6 53.2 54.8 56.5 58.1 59.7 61.3 127
128 16.4 18.0 19.7 21.3 22.9 24.6 26.2 27.9 29.5 31.1 32.8 34.4 36.0 37.7 39.3 41.0 42.6 44.2 45.9 47.5 49.2 50.8 52.4 54.1 55.7 57.3 59.0 60.6 62.3 128
129 16.6 18.3 20.0 21.6 23.3 25.0 26.6 28.3 30.0 31.6 33.3 34.9 36.6 38.3 39.9 41.6 43.3 44.9 46.6 48.3 49.9 51.6 53.3 54.9 56.6 58.2 59.9 61.6 63.2 129
130 16.9 18.6 20.3 22.0 23.7 25.4 27.0 28.7 30.4 32.1 33.8 35.5 37.2 38.9 40.6 42.3 43.9 45.6 47.3 49.0 50.7 52.4 54.1 55.8 57.5 59.2 60.8 62.5 64.2 130
131 17.2 18.9 20.6 22.3 24.0 25.7 27.5 29.2 30.9 32.6 34.3 36.0 37.8 39.5 41.2 42.9 44.6 46.3 48.1 49.8 51.5 53.2 54.9 56.6 58.3 60.1 61.8 63.5 65.2 131
132 17.4 19.2 20.9 22.7 24.4 26.1 27.9 29.6 31.4 33.1 34.8 36.6 38.3 40.1 41.8 43.6 45.3 47.0 48.8 50.5 52.3 54.0 55.8 57.5 59.2 61.0 62.7 64.5 66.2 132
133 17.7 19.5 21.2 23.0 24.8 26.5 28.3 30.1 31.8 33.6 35.4 37.1 38.9 40.7 42.5 44.2 46.0 47.8 49.5 51.3 53.1 54.8 56.6 58.4 60.1 61.9 63.7 65.4 67.2 133
134 18.0 19.8 21.5 23.3 25.1 26.9 28.7 30.5 32.3 34.1 35.9 37.7 39.5 41.3 43.1 44.9 46.7 48.5 50.3 52.1 53.9 55.7 57.5 59.3 61.1 62.8 64.6 66.4 68.2 134
135 18.2 20.0 21.9 23.7 25.5 27.3 29.2 31.0 32.8 34.6 36.5 38.3 40.1 41.9 43.7 45.6 47.4 49.2 51.0 52.9 54.7 56.5 58.3 60.1 62.0 63.8 65.6 67.4 69.3 135
136 18.5 20.3 22.2 24.0 25.9 27.7 29.6 31.4 33.3 35.1 37.0 38.8 40.7 42.5 44.4 46.2 48.1 49.9 51.8 53.6 55.5 57.3 59.2 61.0 62.9 64.7 66.6 68.4 70.3 136
137 18.8 20.6 22.5 24.4 26.3 28.2 30.0 31.9 33.8 35.7 37.5 39.4 41.3 43.2 45.0 46.9 48.8 50.7 52.6 54.4 56.3 58.2 60.1 61.9 63.8 65.7 67.6 69.4 71.3 137
138 19.0 20.9 22.9 24.8 26.7 28.6 30.5 32.4 34.3 36.2 38.1 40.0 41.9 43.8 45.7 47.6 49.5 51.4 53.3 55.2 57.1 59.0 60.9 62.8 64.7 66.7 68.6 70.5 72.4 138
139 19.3 21.3 23.2 25.1 27.0 29.0 30.9 32.8 34.8 36.7 38.6 40.6 42.5 44.4 46.4 48.3 50.2 52.2 54.1 56.0 58.0 59.9 61.8 63.8 65.7 67.6 69.6 71.5 73.4 139
140 19.6 21.6 23.5 25.5 27.4 29.4 31.4 33.3 35.3 37.2 39.2 41.2 43.1 45.1 47.0 49.0 51.0 52.9 54.9 56.8 58.8 60.8 62.7 64.7 66.6 68.6 70.6 72.5 74.5 140
141 19.9 21.9 23.9 25.8 27.8 29.8 31.8 33.8 35.8 37.8 39.8 41.8 43.7 45.7 47.7 49.7 51.7 53.7 55.7 57.7 59.6 61.6 63.6 65.6 67.6 69.6 71.6 73.6 75.5 141
142 20.2 22.2 24.2 26.2 28.2 30.2 32.3 34.3 36.3 38.3 40.3 42.3 44.4 46.4 48.4 50.4 52.4 54.4 56.5 58.5 60.5 62.5 64.5 66.5 68.6 70.6 72.6 74.6 76.6 142
143 20.4 22.5 24.5 26.6 28.6 30.7 32.7 34.8 36.8 38.9 40.9 42.9 45.0 47.0 49.1 51.1 53.2 55.2 57.3 59.3 61.3 63.4 65.4 67.5 69.5 71.6 73.6 75.7 77.7 143
144 20.7 22.8 24.9 27.0 29.0 31.1 33.2 35.3 37.3 39.4 41.5 43.5 45.6 47.7 49.8 51.8 53.9 56.0 58.1 60.1 62.2 64.3 66.4 68.4 70.5 72.6 74.6 76.7 78.8 144
145 21.0 23.1 25.2 27.3 29.4 31.5 33.6 35.7 37.8 39.9 42.1 44.2 46.3 48.4 50.5 52.6 54.7 56.8 58.9 61.0 63.1 65.2 67.3 69.4 71.5 73.6 75.7 77.8 79.9 145
146 21.3 23.4 25.6 27.7 29.8 32.0 34.1 36.2 38.4 40.5 42.6 44.8 46.9 49.0 51.2 53.3 55.4 57.6 59.7 61.8 63.9 66.1 68.2 70.3 72.5 74.6 76.7 78.9 81.0 146
147 21.6 23.8 25.9 28.1 30.3 32.4 34.6 36.7 38.9 41.1 43.2 45.4 47.5 49.7 51.9 54.0 56.2 58.3 60.5 62.7 64.8 67.0 69.1 71.3 73.5 75.6 77.8 80.0 82.1 147
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
71
BMI look-up tables (continued)
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38
148 21.9 24.1 26.3 28.5 30.7 32.9 35.0 37.2 39.4 41.6 43.8 46.0 48.2 50.4 52.6 54.8 57.0 59.1 61.3 63.5 65.7 67.9 70.1 72.3 74.5 76.7 78.9 81.0 83.2 148
149 22.2 24.4 26.6 28.9 31.1 33.3 35.5 37.7 40.0 42.2 44.4 46.6 48.8 51.1 53.3 55.5 57.7 59.9 62.2 64.4 66.6 68.8 71.0 73.3 75.5 77.7 79.9 82.1 84.4 149
150 22.5 24.8 27.0 29.3 31.5 33.8 36.0 38.3 40.5 42.8 45.0 47.3 49.5 51.8 54.0 56.3 58.5 60.8 63.0 65.3 67.5 69.8 72.0 74.3 76.5 78.8 81.0 83.3 85.5 150
151 22.8 25.1 27.4 29.6 31.9 34.2 36.5 38.8 41.0 43.3 45.6 47.9 50.2 52.4 54.7 57.0 59.3 61.6 63.8 66.1 68.4 70.7 73.0 75.2 77.5 79.8 82.1 84.4 86.6 151
152 23.1 25.4 27.7 30.0 32.3 34.7 37.0 39.3 41.6 43.9 46.2 48.5 50.8 53.1 55.4 57.8 60.1 62.4 64.7 67.0 69.3 71.6 73.9 76.2 78.6 80.9 83.2 85.5 87.8 152
153 23.4 25.7 28.1 30.4 32.8 35.1 37.5 39.8 42.1 44.5 46.8 49.2 51.5 53.8 56.2 58.5 60.9 63.2 65.5 67.9 70.2 72.6 74.9 77.2 79.6 81.9 84.3 86.6 89.0 153
154 23.7 26.1 28.5 30.8 33.2 35.6 37.9 40.3 42.7 45.1 47.4 49.8 52.2 54.5 56.9 59.3 61.7 64.0 66.4 68.8 71.1 73.5 75.9 78.3 80.6 83.0 85.4 87.7 90.1 154
155 24.0 26.4 28.8 31.2 33.6 36.0 38.4 40.8 43.2 45.6 48.1 50.5 52.9 56.3 57.7 60.1 62.5 64.9 67.3 69.7 72.1 74.5 76.9 79.3 81.7 84.1 86.5 88.9 91.3 155
156 24.3 26.8 29.2 31.6 34.1 36.5 38.9 41.4 43.8 46.2 48.7 51.1 53.5 56.0 58.4 60.8 63.3 65.7 68.1 70.6 73.0 75.4 77.9 80.3 82.7 85.2 87.6 90.0 92.5 156
157 24.6 27.1 29.6 32.0 34.5 37.0 39.4 41.9 44.4 46.8 49.3 51.8 54.2 56.7 59.2 61.6 64.1 66.6 69.0 71.5 73.9 76.4 78.9 81.3 83.8 86.3 88.7 91.2 93.7 157
158 25.0 27.5 30.0 32.5 34.9 37.4 39.9 42.4 44.9 47.4 49.9 52.4 54.9 57.4 59.9 62.4 64.9 67.4 69.9 72.4 74.9 77.4 79.9 82.4 84.9 87.4 89.9 92.4 94.9 158
159 25.3 27.8 30.3 32.9 35.4 37.9 40.4 43.0 45.5 48.0 50.6 53.1 55.6 58.1 60.7 63.2 65.7 68.3 70.8 73.3 75.8 78.4 80.9 83.4 86.0 88.5 91.0 93.5 96.1 159
160 25.6 28.2 30.7 33.3 35.8 38.4 41.0 43.5 46.1 48.6 51.2 53.8 56.3 58.9 61.4 64.0 66.6 69.1 71.7 74.2 76.8 79.4 81.9 84.5 87.0 89.6 92.2 94.7 97.3 160
161 25.9 28.5 31.1 33.7 36.3 38.9 41.5 44.1 46.7 49.2 51.8 54.4 57.0 59.6 62.2 64.8 67.4 70.0 72.6 75.2 77.8 80.4 82.9 85.5 88.1 90.7 93.3 95.9 98.5 161
162 26.2 28.9 31.5 34.1 36.7 39.4 42.0 44.6 47.2 49.9 52.5 55.1 57.7 60.4 63.0 65.6 68.2 70.9 73.5 76.1 78.7 81.4 84.0 86.6 89.2 91.9 94.5 97.1 99.7 162
163 26.6 29.2 31.9 34.5 37.2 39.9 42.5 45.2 47.8 50.5 53.1 55.8 58.5 61.1 63.8 66.4 69.1 71.7 74.4 77.1 79.7 82.4 85.0 87.7 90.3 93.0 95.6 98.3 101 163
164 26.9 29.6 32.3 35.0 37.7 40.3 43.0 45.7 48.4 51.1 53.8 56.5 59.2 61.9 64.6 67.2 69.9 72.6 75.3 78.0 80.7 83.4 86.1 88.8 91.4 94.1 96.8 99.5 102 164
165 27.2 29.9 32.7 35.4 38.1 40.8 43.6 46.3 49.0 51.7 54.5 57.2 59.9 62.6 65.3 68.1 70.8 73.5 76.2 79.0 81.7 84.4 87.1 89.8 92.6 95.3 98.0 101 104 165
166 27.6 30.3 33.1 35.8 38.6 41.3 44.1 46.8 49.6 52.4 55.1 57.9 60.6 63.4 66.1 68.9 71.6 74.4 77.2 79.9 82.7 85.4 88.2 90.9 93.7 96.4 99.2 102 105 166
167 27.9 30.7 33.5 36.3 39.0 41.8 44.6 47.4 50.2 53.0 55.8 58.6 61.4 64.1 66.9 69.7 72.5 75.3 78.1 80.9 83.7 86.5 89.2 92.0 94.8 97.6 100 103 106 167
168 28.2 31.0 33.9 36.7 39.5 42.3 45.2 48.0 50.8 53.6 56.4 59.3 62.1 64.9 67.7 70.6 73.4 76.2 79.0 81.8 84.7 87.5 90.3 93.1 96.0 98.8 102 104 107 168
169 28.6 31.4 34.3 37.1 40.0 42.8 45.7 48.6 51.4 54.3 57.1 60.0 62.8 65.7 68.5 71.4 74.3 77.1 80.0 82.8 85.7 88.5 91.4 94.3 97.1 100 103 106 109 169
170 28.9 31.8 34.7 37.6 40.5 43.3 46.2 49.1 52.0 54.9 57.8 60.7 63.6 66.5 69.4 72.2 75.1 78.0 80.9 83.8 86.7 89.6 92.5 95.4 98.3 101 104 107 110 170
171 29.2 32.2 35.1 38.0 40.9 43.9 46.8 49.7 52.6 55.6 58.5 61.4 64.3 67.3 70.2 73.1 76.0 79.0 81.9 84.8 87.7 90.6 93.6 96.5 99.4 102 105 108 111 171
172 29.6 32.5 35.5 38.5 41.4 44.4 47.3 50.3 53.3 56.2 59.2 62.1 65.1 68.0 71.0 74.0 76.9 79.9 82.8 85.8 88.8 91.7 94.7 97.6 101 104 107 110 112 172
173 29.9 32.9 35.9 38.9 41.9 44.9 47.9 50.9 53.9 56.9 59.9 62.9 65.8 68.8 71.8 74.8 77.8 80.8 83.8 86.8 89.8 92.8 95.8 98.8 102 105 108 111 114 173
174 30.3 33.3 36.3 39.4 42.4 45.4 48.4 51.5 54.5 57.5 60.6 63.6 66.6 69.6 72.7 75.7 78.7 81.7 84.8 87.8 90.8 93.9 96.9 99.9 103 106 109 112 115 174
175 30.6 33.7 36.8 39.8 42.9 45.9 49.0 52.1 55.1 58.2 61.3 64.3 67.4 70.4 73.5 76.6 79.6 82.7 85.8 88.8 91.9 94.9 98.0 101 104 107 110 113 116 175
176 31.0 34.1 37.2 40.3 43.4 46.5 49.6 52.7 55.8 58.9 62.0 65.0 68.1 71.2 74.3 77.4 80.5 83.6 86.7 89.8 92.9 96.0 99.1 102 105 108 112 115 118 176
177 31.3 34.5 37.6 40.7 43.9 47.0 50.1 53.3 56.4 59.5 62.7 65.8 68.9 72.1 75.2 78.3 81.5 84.6 87.7 90.9 94.0 97.1 100 103 107 110 113 116 119 177
178 31.7 34.9 38.0 41.2 44.4 47.5 50.7 53.9 57.0 60.2 63.4 66.5 69.7 72.9 76.0 79.2 82.4 85.5 88.7 91.9 95.1 98.2 101 105 108 111 114 117 120 178
179 32.0 35.2 38.4 41.7 44.9 48.1 51.3 54.5 57.7 60.9 64.1 67.3 70.5 73.7 76.9 80.1 83.3 86.5 89.7 92.9 96.1 99.3 103 106 109 112 115 119 122 179
180 32.4 35.6 38.9 42.1 45.4 48.6 51.8 55.1 58.3 61.6 64.8 68.0 71.3 74.5 77.8 81.0 84.2 87.5 90.7 94.0 97.2 100 104 107 110 113 117 120 123 180
181 32.8 36.0 39.3 42.6 45.9 49.1 52.4 55.7 59.0 62.2 65.5 68.8 72.1 75.4 78.6 81.9 85.2 88.5 91.7 95.0 98.3 102 105 108 111 115 118 121 125 181
182 33.1 36.4 39.7 43.1 46.4 49.7 53.0 56.3 59.6 62.9 66.2 69.6 72.9 76.2 79.5 82.8 86.1 89.4 92.7 96.1 99.4 103 106 109 113 116 119 123 126 182
183 33.5 36.8 40.2 43.5 46.9 50.2 53.6 56.9 60.3 63.6 67.0 70.3 73.7 77.0 80.4 83.7 87.1 90.4 93.8 97.1 101 104 107 111 114 117 121 124 127 183
184 33.9 37.2 40.6 44.0 47.4 50.8 54.2 57.6 60.9 64.3 67.7 71.1 74.5 77.9 81.3 84.6 88.0 91.4 94.8 98.2 102 105 108 112 115 119 122 125 129 184
185 34.2 37.6 41.1 44.5 47.9 51.3 54.8 58.2 61.6 65.0 68.5 71.9 75.3 78.7 82.1 85.6 89.0 92.4 95.8 99.3 103 106 110 113 116 120 123 127 130 185
186 34.6 38.1 41.5 45.0 48.4 51.9 55.4 58.8 62.3 65.7 69.2 72.7 76.1 79.6 83.0 86.5 89.9 93.4 96.9 100 104 107 111 114 118 121 125 128 132 186
187 35.0 38.5 42.0 45.5 49.0 52.5 56.0 59.4 62.9 66.4 69.9 73.4 76.9 80.4 83.9 87.4 90.9 94.4 97.9 101 105 108 112 115 119 122 126 129 133 187
188 35.3 38.9 42.4 45.9 49.5 53.0 56.6 60.1 63.6 67.2 70.7 74.2 77.8 81.3 84.8 88.4 91.9 95.4 99.0 103 106 110 113 117 120 124 127 131 134 188
189 35.7 39.3 42.9 46.4 50.0 53.6 57.2 60.7 64.3 67.9 71.4 75.0 78.6 82.2 85.7 89.3 92.9 96.4 100 104 107 111 114 118 122 125 129 132 136 189
190 36.1 39.7 43.3 46.9 50.5 54.2 57.8 61.4 65.0 68.6 72.2 75.8 79.4 83.0 86.6 90.3 93.9 97.5 101 105 108 112 116 119 123 126 130 134 137 190
191 36.5 40.1 43.8 47.4 51.1 54.7 58.4 62.0 65.7 69.3 73.0 76.6 80.3 83.9 87.6 91.2 94.9 98.5 102 106 109 113 117 120 124 128 131 135 139 191
192 36.9 40.6 44.2 47.9 51.6 55.3 59.0 62.7 66.4 70.0 73.7 77.4 81.1 84.8 88.5 92.2 95.8 99.5 103 107 111 114 118 122 125 129 133 136 140 192
193 37.2 41.0 44.7 48.4 52.1 55.9 59.6 63.3 67.0 70.8 74.5 78.2 81.9 85.7 89.4 93.1 96.8 101 104 108 112 116 119 123 127 130 134 138 142 193
194 37.6 41.4 45.2 48.9 52.7 56.5 60.2 64.0 67.7 71.5 75.3 79.0 82.8 86.6 90.3 94.1 97.9 102 105 109 113 117 120 124 128 132 136 139 143 194
195 38.0 41.8 45.6 49.4 53.2 57.0 60.8 64.6 68.4 72.2 76.1 79.9 83.7 87.5 91.3 95.1 98.9 103 107 110 114 118 122 126 129 133 137 141 145 195
196 38.4 42.3 46.1 49.9 53.8 57.6 61.5 65.3 69.1 73.0 76.8 80.7 84.5 88.4 92.2 96.0 99.9 104 108 111 115 119 123 127 131 135 138 142 146 196
197 38.8 42.7 46.6 50.5 54.3 58.2 62.1 66.0 69.9 73.7 77.6 81.5 85.4 89.3 93.1 97.0 101 105 109 113 116 120 124 128 132 136 140 144 148 197
198 39.2 43.1 47.0 51.0 54.9 58.8 62.7 66.6 70.6 74.5 78.4 82.3 86.2 90.2 94.1 98.0 102 106 110 114 118 122 126 129 133 137 141 145 149 198
199 39.6 43.6 47.5 51.5 55.4 59.4 63.4 67.3 71.3 75.2 79.2 83.2 87.1 91.1 95.0 99.0 103 107 111 115 119 123 127 131 135 139 143 147 151 199
200 40.0 44.0 48.0 52.0 56.0 60.0 64.0 68.0 72.0 76.0 80.0 84.0 88.0 92.0 96.0 100 104 108 112 116 120 124 128 132 136 140 144 148 152 200
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
72
BMI-for-age look-up table school-aged children and adolescents 5–19 years - WHO 2007
growth reference
Boys' BMI-for-age Year: Month
Girls' BMI-for-age
-3 SD -2 SD -1 SD Median Median -1 SD -2 SD -3 SD
12.1 13.0 14.1 15.3 5:1 15.2 13.9 12.7 11.8
12.1 13.0 14.1 15.3 5:6 15.2 13.9 12.7 11.7
12.1 13.0 14.1 15.3 6:0 15.3 13.9 12.7 11.7
12.2 13.1 14.1 15.4 6:6 15.3 13.9 12.7 11.7
12.3 13.1 14.2 15.5 7:0 15.4 13.9 12.7 11.8
12.3 13.2 14.3 15.6 7:6 15.5 14.0 12.8 11.8
12.4 13.3 14.4 15.7 8:0 15.7 14.1 12.9 11.9
12.5 13.4 14.5 15.9 8:6 15.9 14.3 13.0 12.0
12.6 13.5 14.6 16.0 9:0 16.1 14.4 13.1 12.1
12.7 13.6 14.8 16.2 9:6 16.3 14.6 13.3 12.2
12.8 13.7 14.9 16.4 10:0 16.6 14.8 13.5 12.4
12.9 13.9 15.1 16.7 10:6 16.9 15.1 13.7 12.5
13.1 14.1 15.3 16.9 11:0 17.2 15.3 13.9 12.7
13.2 14.2 15.5 17.2 11:6 17.6 15.6 14.1 12.9
13.4 14.5 15.8 17.5 12:0 18.0 16.0 14.4 13.2
13.6 14.7 16.1 17.9 12:6 18.4 16.3 14.7 13.4
13.8 14.9 16.4 18.2 13:0 18.8 16.6 14.9 13.6
14.0 15.2 16.7 18.6 13:6 19.2 16.9 15.2 13.8
14.3 15.5 17.0 19.0 14:0 19.6 17.2 15.4 14.0
14.5 15.7 17.3 19.4 14:6 19.9 17.5 15.7 14.2
14.7 16.0 17.6 19.8 15:0 20.2 17.8 15.9 14.4
14.9 16.3 18.0 20.1 15:6 20.5 18.0 16.0 14.5
15.1 16.5 18.2 20.5 16:0 20.7 18.2 16.2 14.6
15.3 16.7 18.5 20.8 16:6 20.9 18.3 16.3 14.7
15.4 16.9 18.8 21.1 17:0 21.0 18.4 16.4 14.7
15.6 17.1 19.0 21.4 17:6 21.2 18.5 16.4 14.7
15.7 17.3 19.2 21.7 18:0 21.3 18.6 16.4 14.7
15.8 17.4 19.4 22.0 18:6 21.3 18.6 16.5 14.7
15.9 17.6 19.6 22.2 19:0 21.4 18.7 16.5 14.7

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
73
Annex 15. Overview of treatment for concurrent illnesses in kala-azar
This is a short listing of diseases common for kala-azar patients. This is a bit different than what is used in general health facilities because kala-azar patients are immune compromised. Please use this only for your kala-azar treatment center.
Disease First line therapy Second line therapy Comments
Pneumonia Amoxicillin for mild to
moderate pneumonia
Ceftriaxone if seriously ill
Chlorampenicol:
For serious pneumonia or treatment failure
oral is as good or better than IV or IM
not a good choice if patient is severely anemic
Cotrimoxazole:
for patients who are allergic
Erythromycin:
for patients > 5 who fail amoxicillin
patients with wheezy pneumonia
Many kala-azar patients especially < 5 years old have aspirated because of
vomiting or a febrile seizure. Amoxicillin, Ceftriaxone and Chloramphenicol will
treat aspiration pneumonia.
Chloramphenicol suppresses blood formation so is not recommended for severely
anemic patients.
Erythromycin can cause stomach pain or vomiting so be careful with KA patients!
Vomiting
with nausea – not
simply with cough
This can be a side effect
of SSG. You may stop
the SSG for 2 to 5 days.
Promethazine – orally or
IM or IV
ORS
Metoclopromide oral or IM or IV
Diazepam oral or IM or IV
Hydration with ORS or by IV
A combination of all the medicines may be
necessary
You must be sure that there is not a diagnosis you are missing. Is there malaria?
Is there meningitis?
Vomiting can be a sign of serious illness especially in children. Be careful.
Young children can easily get an overdose. Make sure older children do not give
their tablets to babies.
The major overdose effect of promethazine and metaclopromide is a stiff neck,
sometimes the tongue sticks out. Treatment with IV or rectal diazepam helps
overdose.
Diarrhea, significant
This means ANY ONE of
the below:
≥4 x per 24 hours
bloody
with fever
the patient is severely
malnourished
Tinidazole 3-10 days
PLUS
Ciprofloxin 3 – 5 days
PLUS
ORS, always give ORS, it
is better if it is already
made up in the correct
way.
Consider KCl (slow K) for
severe disease
Metronidazole 5-10 days
PLUS
Ciprofloxin for 3-5 days PLUS
ORS
Tinidazole causes less vomiting than Metronidazole and is a once a day drug
Bananas are a good source of potassium and if available should be encouraged

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
74
Other common illnesses of kala-azar patients. These are likely to be standard care with only a few comments specific to kala-azar patients
Disease First line therapy Second line therapy Comments
Malaria
Artemisinin plus Fansidar Quinine
for blood film positive malaria within 2 weeks of
treatment with Artemisinine plus Fansidar
for serious malaria
All kala-azar patients are treated for Malaria on or within 1 week of
admission. The first week of kala-azar treatment the patient has
fever from kala-azar so diagnosis is difficult.
Ear infection
Recent infection with or
without draining
Amoxicillin Cotrimoxazole Chronic draining ears need to be cleaned. Saline or vinegar (half
strength) are good for cleaning. Antibiotics are not useful
Gentian violet in the ear canal can be used if there is an ear canal
infection with itching
Fever after childbirth
Amoxicillin plus Metronidazole
Ceftriaxone if seriously ill
Ampicillin, Metronidazole and Gentamycin IM
Jaundice Vitamin K IM (for 5 days)
Gum pain Penicillin and vitamin C Penicillin plus metronidazole for cancrum oris Educate about good oral hygiene
Wounds Penicillin and gentian violet Cloxacillin and drainage if there is an abscess
Penicillin and metronidazole if there is
gangrene
Injections abscesses are common from village injections.
Gangrene can occur with these wounds.
Herpes Zoster Paracetamol for 5 days
minimum
Gentian violet if blisters open
Ibuprophen is first line if the
patient is at the end of kala-azar
treatment.
Tramadol – for severe pain At the end of treatment Ibuprophen is superior to Paracetamol for
treatment as it has more pain relief than paracetamol.
Ibuprophen should not be used early in treatment because of risk of
bleeding.
Eye pain Tetracycline eye ointment
Until 2 days after symptoms
gone
For 1 month if there is trachoma
Vitamin A – if not given, may
need 3 doses if severely
malnourished
Gentamicin or chloramphenicol eye drops
Use first line for excessive pus
Use if tetracycline fails
Pain Paracetamol Tramadol for severe pain
NO aspirin, it increases the risk of bleeding.
Ibuprophen may also increase the risk of bleeding, it may
sometimes be used at the end of treatment

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
75
Annex 16. Drug guidelines for kala-azar
This table is to help with these uncommon medicines you may not be familiar with.
This is not a complete guide to these medicines. If you are not comfortable please use other medicines that you know or ask for help.
Dose Indication Length of tx Side effects Comments
Ciprofloxacin 500 mg
20-30mg/kg/d up to 40mg/kg/d
Sometimes the tablets are 250
mg. LOOK!
4.5-7 kg ¼ tab x 1
8-12 kg ½ tab x 1
13-24 kg ½ tab x 2
25-adult 1-2 tab x 2
Dysentery, shigella (this is
a common illness for kala-
azar patients)
3 to 5 days Multiple uncommon side
effects – nausea, headache,
neurologic complaints,
aches, sun sensitivity
Ciprofloxacin treats many illnesses.
We try to use it rarely as resistance could
develop. Then there would be no
medicine for dysentery epidemics.
Avoid during pregnancy.
Avoid antacids and ferrous for 2 hours
Avoid with aminophylline
May have some effect on children’s cartilage
Ceftriaxone 1 gm vial
50-100 mg/kg/day
for IM, you can mix with 4.6 ml
water to make 5 ml.
Then each ml is 200 mg!
50mg/kg/day – LRTI
100 mg/kg/day -
meningitis
Pneumonia, severe
Meningitis
(Also typhoid, neonatal
sepsis, any age sepsis)
LRTI: 3 days followed by oral
high dose Amoxicillin for 7
days (or, if resistant LRTI, 7
days of chloramphenicol)
Meningitis: 7 – 14 days
Allergic reaction
Painful injection!
Safe
It can be given once a day.
Tinidazole 500 mg
4-7 kg ½ tab x 1
8-13 kg 1 tab x 1
14-17 kg 1½-2 tab x 1
18-23 kg 2 tab x 1
24-33 kg 3 tab x 1
adult 4 tab x 1
Giardia
Amebic dysentery and
amebic liver abscess
(various gynecologic dx)
1 to 3 days
3 to 10 days
Nausea
Metallic taste in mouth
Do not take with alcohol
Tinidazole causes less nausea and vomiting
than metronidazole and it may be taken as
once a day dosing. The 2 drugs treat the
same diseases. They may not be taken
together.
Slow K 500 or 600mg
50mm / kg / day
8-15kg 1 x 1
15-30kg 1 x 2
30-50kg 1 x 3
Severe diarrhea, or
moderate diarrhea with
vomiting
2 days – more if needed Bad taste If the patient cannot pass urine, do not give,
it can be deadly! If the patient urinates it is
not dangerous.

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
76
Annex 17. Kala-azar monthly reporting forms
Treatment activities Kala Azar Year ………. Treatment site ………………
January February March April May June July August September October November December TOTAL
Total cases admitted
Primary KA
Relapses
PKDL
January February March April May June July August September October November December TOTAL
No. of Primary KA cases
Discharged
Defaulters
Deaths
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec TOTAL
No. Of relapses
Discharged
Defaulters
Deaths
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec TOTAL
No. of PKDL (Post Kala azar Dermal Leishmaniasis)
Discharged
Defaulters
Deaths
Demographic characteristics, Primary KA Jan Feb Mar Apr May Jun Jul Aug Sept Oct Nov Dec TOTAL
SEX
Male
Female
AGE GROUP
< 5years
5 - 14 years
15 years and above

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
77
Kala-Azar test performed Year ……………. Treatment centre…………………….
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec TOTAL
No. of rapid tests (rk39) done
rapid tests positive
rapid tests negative
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec TOTAL
No. of DAT collected
DAT positive
DAT negative
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec TOTAL
No. of lymph node aspirates
lymph node aspirate positive
lymph node aspirate negative
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec TOTAL
No. of BM aspirates
BM aspirate positive
BM aspirate negative
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec TOTAL
No. of spleen aspirates
spleen aspirate positive
spleen aspirate negative
DAT - Direct Agglutination Test
BM - bone marrow

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
78
Drugs and reagents for Kala Azar Year …………. Treatment site ……………………….
Glucantime Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec TOTAL
Expiry date(s):
No. of Ampules at the beginning of the month
No. of Ampules at the end of the month
No. of Ampules consumed
SSG (..… ml vials at ….. mg/ml) Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec TOTAL
Expiry date(s):
No. of vials at the beginning of the month
No. of vials at the end of the month
No. of vials consumed
Ambisome (..… mg vials) Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec TOTAL
Expiry date(s):
No. of vials at the beginning of the month
No. of vials at the end of the month
No. of vials consumed
Paromomycin (..… mg vials) Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec TOTAL
Expiry date(s):
No. of vials at the beginning of the month
No. of vials at the end of the month
No. of vials consumed
DAT reagent Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec TOTAL
Expiry date(s):
No. of vials at the beginning of the month
No. of vials at the end of the month
No. of vials consumed
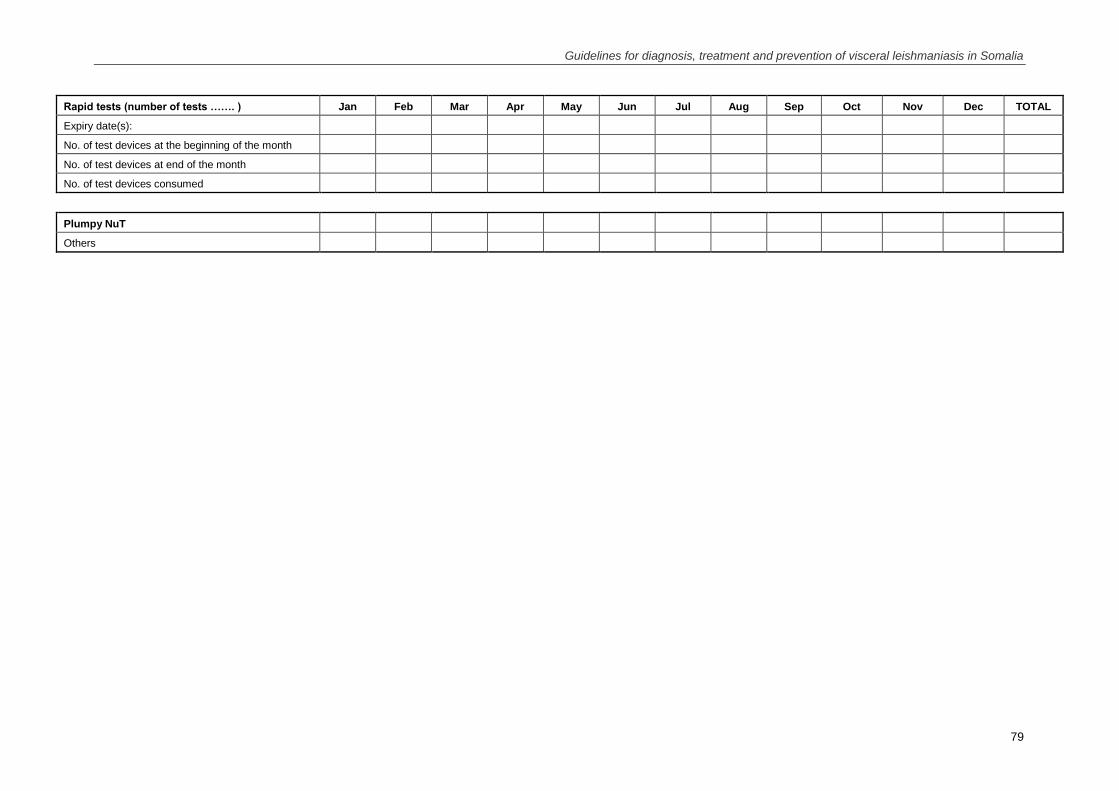
Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
79
Rapid tests (number of tests ……. ) Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec TOTAL
Expiry date(s):
No. of test devices at the beginning of the month
No. of test devices at end of the month
No. of test devices consumed
Plumpy NuT
Others

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
80
Kala Azar screening and diagnosis activities Year …………… Treatment site ………………………….
No. of people screened Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Total
Active (through outreach)
Passive (patient coming to heatlh facility)
Geographical origin of patients Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec TOTAL
(place of infection if known)
Region District Village/Town

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
81
Annex 18. Kala-azar weekly reporting forms
Government of Somalia, Ministry of Health and Human Services
Weekly reporting form
Centre…………………
Year…………………….
Admissions characteristics
Epidemiological
week
PRY KA
(new case)
SEC KA
(PKDL or
relapse) Male Female 0-4 5 to 14 15 and Above Death
Total
admissions
Total
retained
Years Years Years
Summary

Guidelines for diagnosis, treatment and prevention of visceral leishmaniasis in Somalia
82
Annex 19. Kala-azar line listing file (to be sent to central database on regular basis)
Kala Azar line listing file
Date
Treat-
ment
site
Patient
number/
ID
Patient
name Region District
Village
/town Age Sex Pregnant
Months
sick BMI
Z
score
Rapid
test
(rK39)
DAT DAT
titre
LN
aspirate
Spleen
aspirate
Patient
category
Treatment
starting
date
Treatment
regime
Treatment
outcome
Date of
treatment
outcome


















