![Ruby on Rails [ Ruby On Rails.ppt ] - [Ruby - [Ruby-Doc.org ...](https://static.fdocuments.net/doc/165x107/5491e450b479597e6a8b57d5/ruby-on-rails-ruby-on-railsppt-ruby-ruby-docorg-.jpg)
Ruby on Rails [ Ruby On Rails.ppt ] - [Ruby - [Ruby-Doc.org ...
Upload
drruby-binilCategory
view
242download
5
Ruby RajPG-First year
Department of Orthodontics

Introduction
Why to study growth
Relevance of growth
Definition of growth and development
Factors affecting growth
Terminologies
Characteristics of bone growth
Theories
Prenatal growth
Post natal
Growth movements
Growth rotations
Conclusion


growth
How
and
where
direction
Environme
nt
0rthodont
ics
remaining
genetics


•skeletal
•malocclusionDisproportionate
growth
•Treatment
•plangrowth

Definition
Growth is an increase in size.
Development is progress towards
maturity .”
TODD

quantitative aspect of biological development
per unit of time
MOYERS
GROWTH

development
growth
differentiation
translocation

all the naturally occuring unidirectional changes in
life of as individual from its existence as a single
cell to its elaboration as a multifunctional unit
terminating in death
MOYERSDEVELOPMENT
Change in any morphological
parameter which is measurable
GROWTH
MOSS
genetic
• genotype
• racial
Environmental factors
• nutrition
• Physical changes like temperature pressure
,hydration
Functional forces
• Extrinsic and intrinsic muscle activities-exercises
• Space occupying organs and cavities
• Growth expansion
F
A
C
T
O
R
S

Growth fields
The outside and inside surface of a bone are
blanketed by mosaic like pattern of soft
tissue , cartilage or osteogenic membrane
called as growth fields .
These when altered are capable of
producing an alteration in the growth of
particular bone.
Growth site:
are growth fields that have a specific
significance in the growth of particular bone
.(location)
eg: Md condyle, Max tuberosity, sutures
between membrane bones of cranium and jaws
.
The growth site may posses an intrinsic
potential to grow.
Growth centre :
special growth site
Control overall bone growth
which has a genetic potential to grow.
Eg: epiphyseal plate, cartilage from speno
occipital synchondrosis.

Remodelling
Differential growth activity involving deposition
and resorption in the inner and outer surfaces of
the bone
ex,-posterior movement of ramus

CHARACTERISTICS OF BONE GROWTH
INTRAMEMBRANOUS
ENDOCHONDRAL
Intramembranous
Rapid apposition without
cartilaginous model
Mesenchymal connective tisssue osseous tisssue

Endochondral
Hyaline cartilage bone
Deeply seated and slowly expanding structures-cartilage
Favours a directed prototype cartilaginous growth
Replaced by bone(indirect bone growth)

GENETIC THEORY
SUTURAL THEORY
CARTILAGINOUS THEORY
FUNCTIONAL MATRIX THEORY

Van LIMBORGH’S THEORY
ENLOW’S EXPANDING ‘V’ PRINCIPLE
ENLOW’S COUNTERPART PRINCIPLE
NEUROTROPHISM IN ORO-FACIAL GROWTH

Genetic
BASED ON THE LOCATION OF GENETIC
CONTROL THERE ARE 3 DETERMINANTS
OF GROWTH
Bone is the primary determinant of its own growth
Cartilage is the primary determinant of skeletal
growth
Soft tissue matrix in which the skeletal elements are
embedded is the primary determinant of growth

SUTURAL THEORY
Sicher and Weinmann 1952
SICHER AND WEINMANN
1952

Proliferation of osteogenictissues
Create space for oppositional growth

points raised against this theory are
1)suture reimplanted
2)growth in cleft cases

SYCHONDROSIS OF CRANIAL
BASE

Spheno-ethmoidal –terminates by 6 yrs
Inter-sphenoidal---disappears at birth
Spheno-occipital---upto adult life
Intra-occipital --closes at 3rd to 5th year of life

CARTILAGINOUS THEORY-JAMES .H.SCOTT
Nasal septal cartilage is the
pacemaker for the
nasomaxillary complex.
Points in favor of this theory
1) in many bones cartilaginous growth
occurs
2) transplantation of epiphyseal plate
3) nasal septal cartilage



FUNCTIONAL MATRIX THEORY
By Melvin Moss(1960)
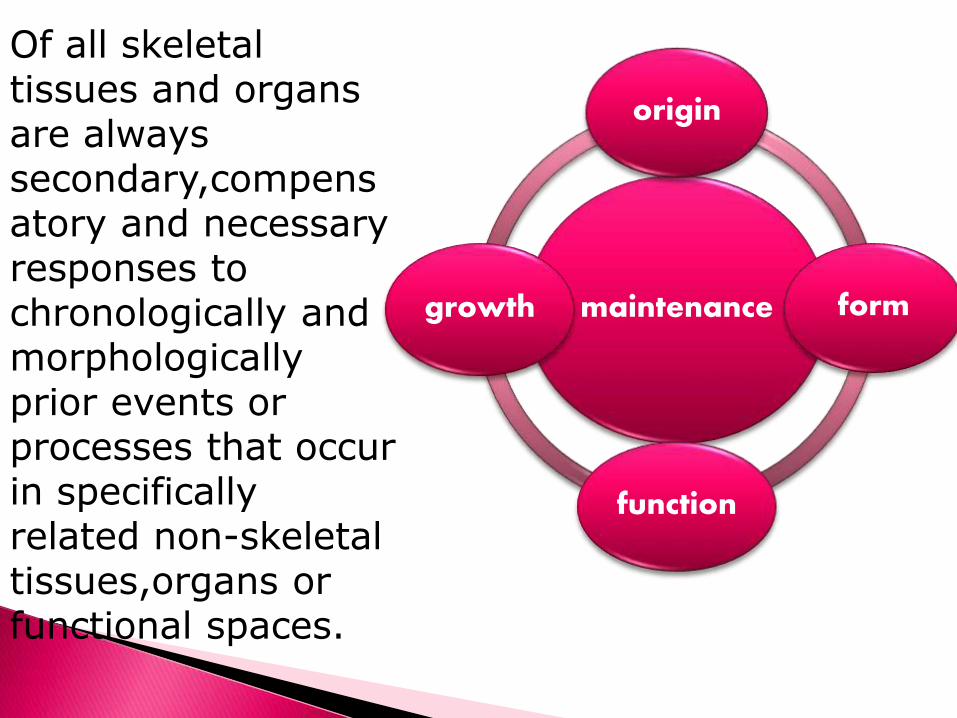
Of all skeletal tissues and organs are always secondary,compensatory and necessary responses to chronologically and morphologically prior events or processes that occur in specifically related non-skeletal tissues,organs or functional spaces.
maintenance
origin
form
function
growth
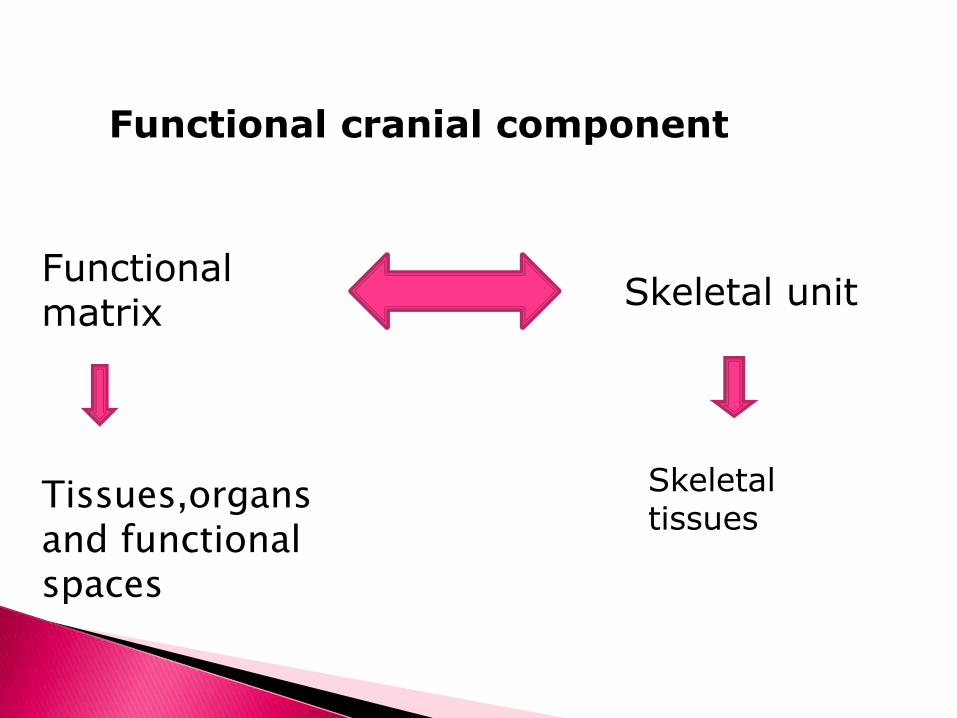
Functional cranial component
Functional matrix
Skeletal unit
Tissues,organsand functional spaces
Skeletal tissues

A change in size ,shape,spatial position
and maintanence of all skeletal units is
due to their activity of their respective
functional matrices.

Functional matrix
Periostealmatrix
Capsular matrix

Periosteal matrix
Consist of muscles, blood vessels, nerves,glands etc
Direct action on their skeletal units-leading to bone
deposition and resorption-lead to transformation in size
and shape.

Capsular matrix
Act indirectly and passively-expansion of the
oro-facial capsule(facial bones arise, grow and
maintained)-secondarily compensatory
translation in space.
No deposition and resorption.

Neuro- cranial capsule
Skin and duramater
Protects the neuro cranial capsular functional matrix
Comprises of brain ,leptomeninges and C.S.F

Oro-facial capsule
Skin and mucosa
Protects the orofacial
pharyngeal spaces
Volume and patency of
these spaces influence
the growth of facial
skull

van Limborgh’s theory
1. Intrinsic genetic factor
2. Local epigenic factors
3. General epigenic factors
4. Local environmental factors
5. General environmental factors
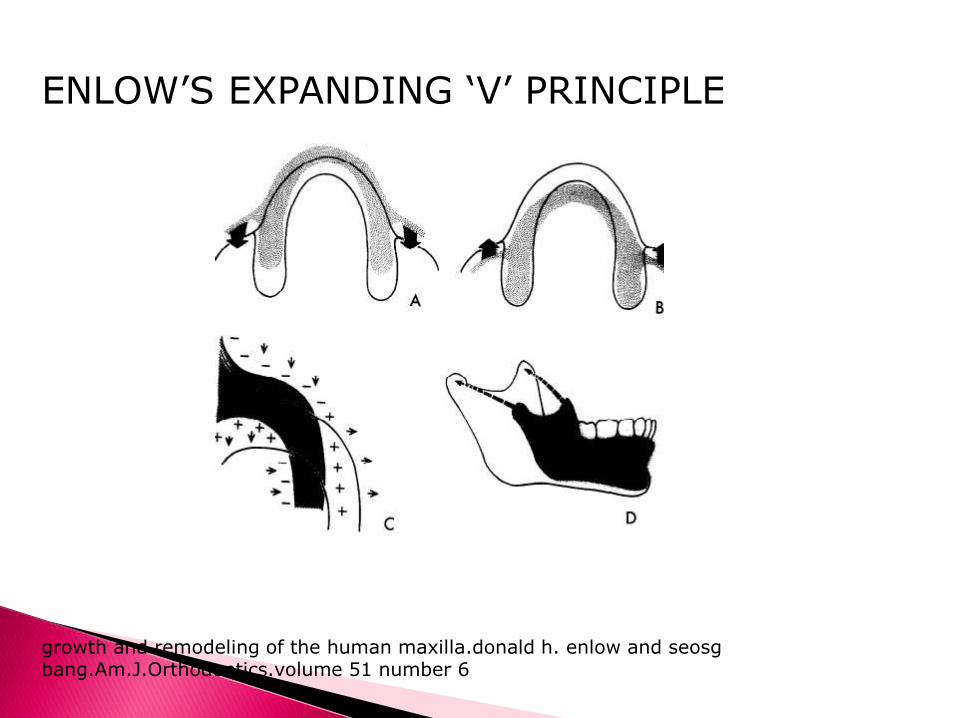
ENLOW’S EXPANDING ‘V’ PRINCIPLE
growth and remodeling of the human maxilla.donald h. enlow and seosgbang.Am.J.Orthodontics.volume 51 number 6


ENLOW’S COUNTERPART PRINCIPLE
Growth of any facial or cranial part is related to
their counterparts.
Imbalanced growth occurs if there is change in
amount,time and direction of growth
Nasomaxillary complex-anterior cranial
fossa
Pharyngeal space-middle cranial fossa
Maxilla-mandible
Maxilla-corpus
Maxillary tuberosity –lingual tuberosity

NEUROTROPHISM IN ORO-FACIAL GROWTH
Neutrotrophism is a non impulse transmitting
neural function
involves axoplasmic transport
provides long term interaction between
neurons and innervative tissues that regulates
the morphological,compositional and functional
integrity of those tissues.

SERVO SYSTEM THEORY (Stutzmann and Petrovic )

• Influence of STH
• Gives a cybernetic form of
command
• Proprioceptives in muscle
• Get activated
• Stretching of muscle
• Increase cartilage vascular supply
• Growth

GROWTH
prenatal postnatal
Period of ovum
Period of embryo
Period of fetus
PRENATAL
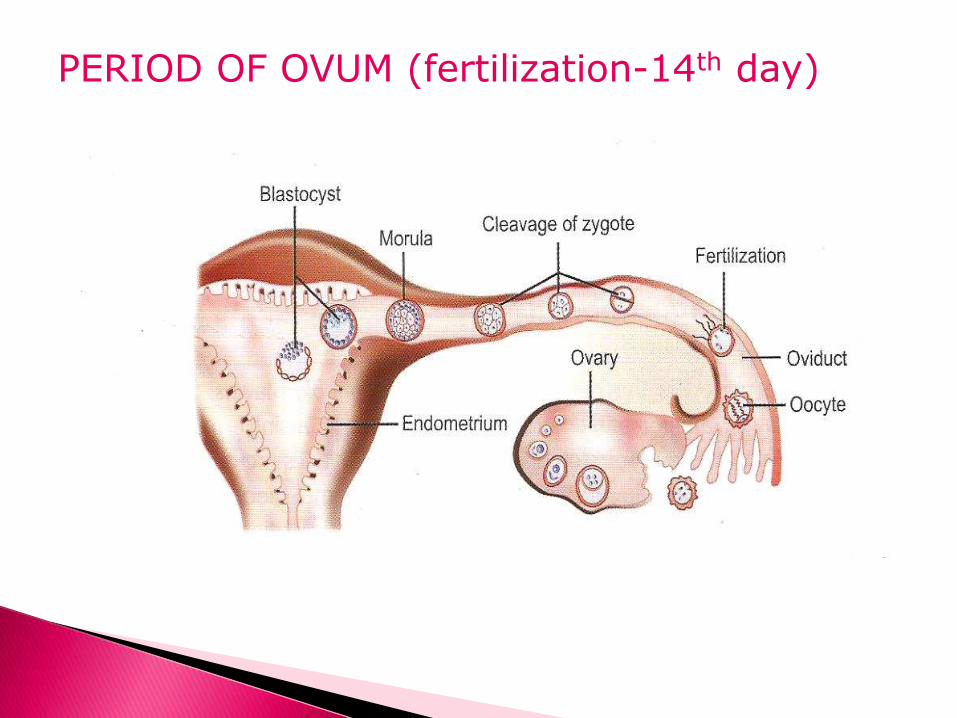
PERIOD OF OVUM (fertilization-14th day)


PERIOD OF EMBRYO (14-56th day)
presomite
somite
postsomite
PRESOMITE(2-3rd week of IUL)
Formation of amnion and chorion-nutrition-end
of 2nd week
Formation of primary germ layers-3rd
week(gastrulation and neurulation)
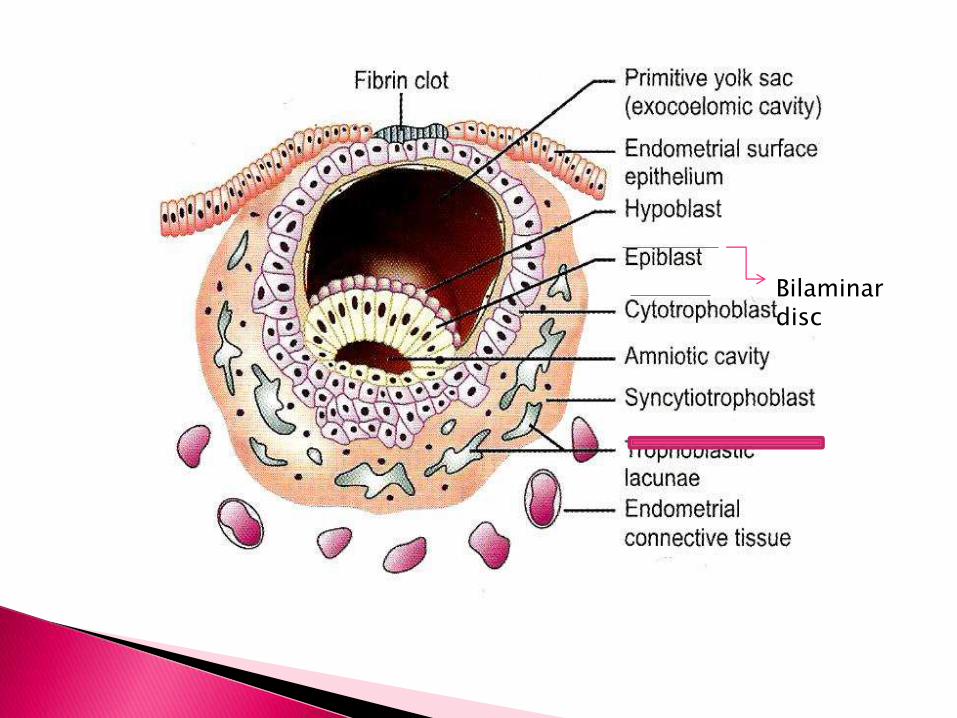
Bilaminardisc
During gastrulation
Bilaminar disc – trilaminar disc.
Middle of epiblast layer-primitive streak
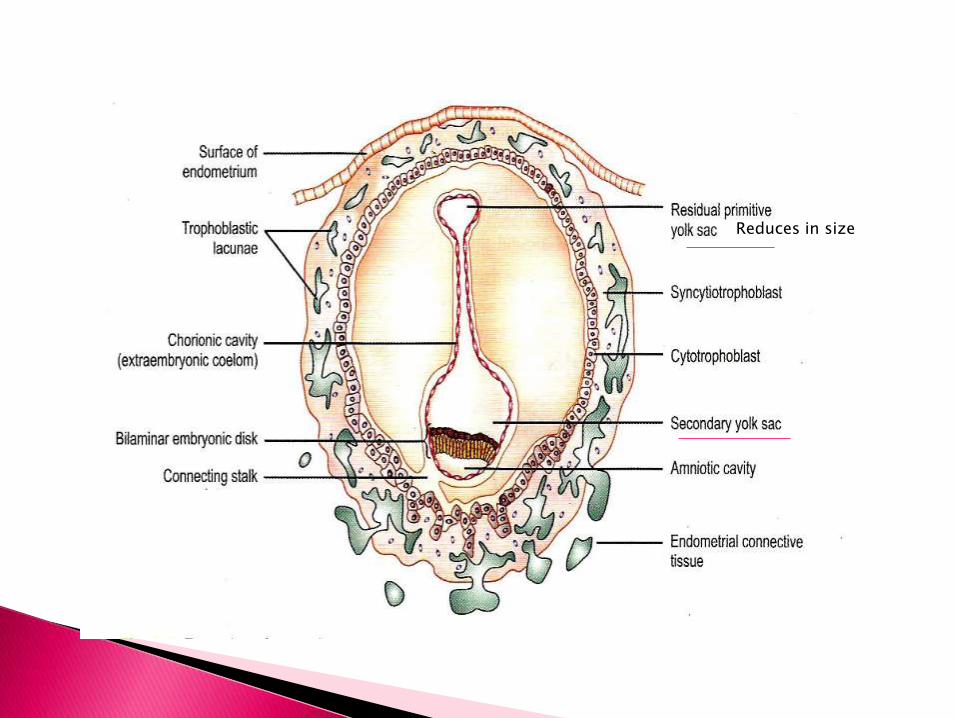
Reduces in size
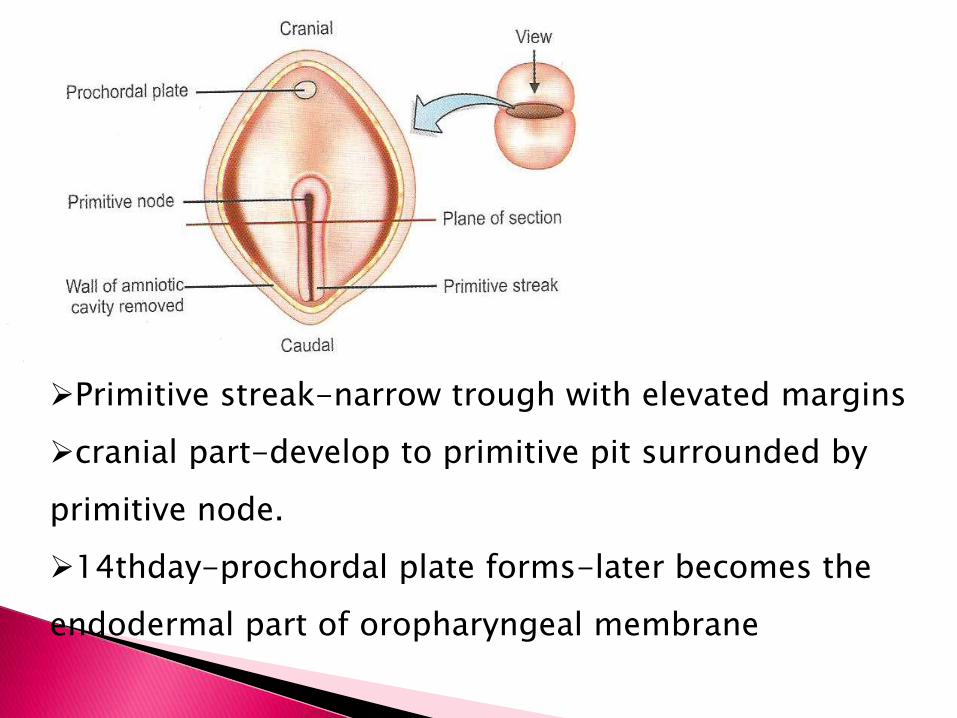
Primitive streak-narrow trough with elevated margins
cranial part-develop to primitive pit surrounded by
primitive node.
14thday-prochordal plate forms-later becomes the
endodermal part of oropharyngeal membrane

3 germ layers

Notochord and Neural tube formation
SOMITE PERIOD
Period of organogenesis.
21-31 day of IUL
Anomalies
Formation of visceral organs from endoderm and
mesoderm
Rapid growth of cranial and caudal part lags behind.


Neural tube
ProchordalPlate

4th week of IUL
Prominent bulge –at ventral aspect of embryo-developing brain
Below bulge-shallow depression-primitive mouth-stomodeum
Floor of stomodeum –buccopharyngeal membrane that
separates stomodeum from the foregut.

Neck elongation of the region between the stomatodeum and
the pericardium
Elongation due to
Appearance of mesodermal
thickenings in the wall of
cranial most part of foregut
called pharyngeal arches
Descend of the
developing heart


FOREGUT
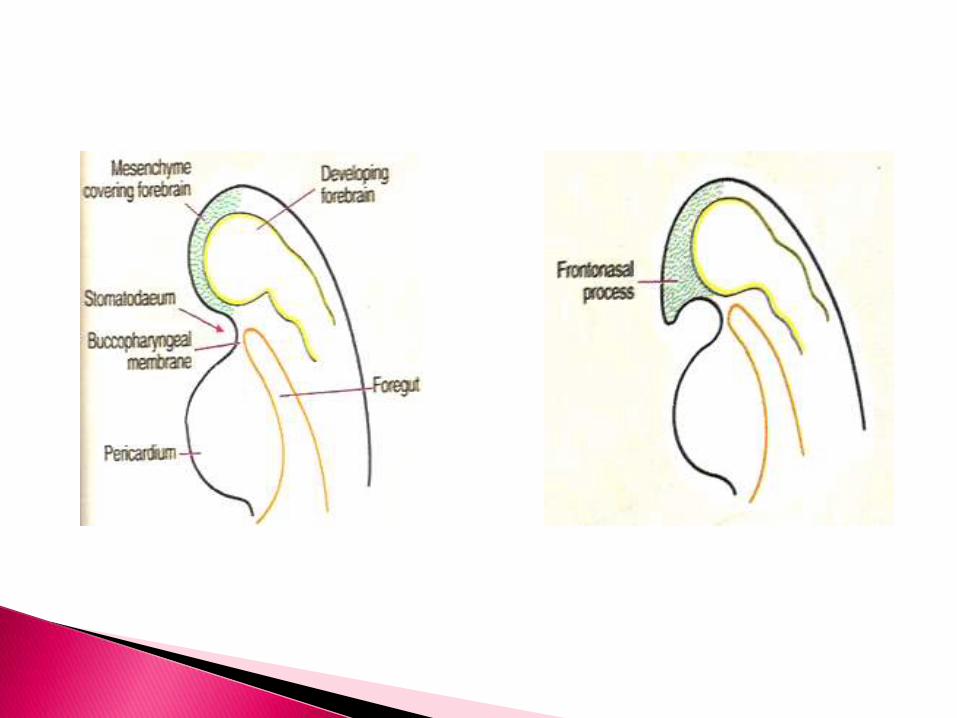

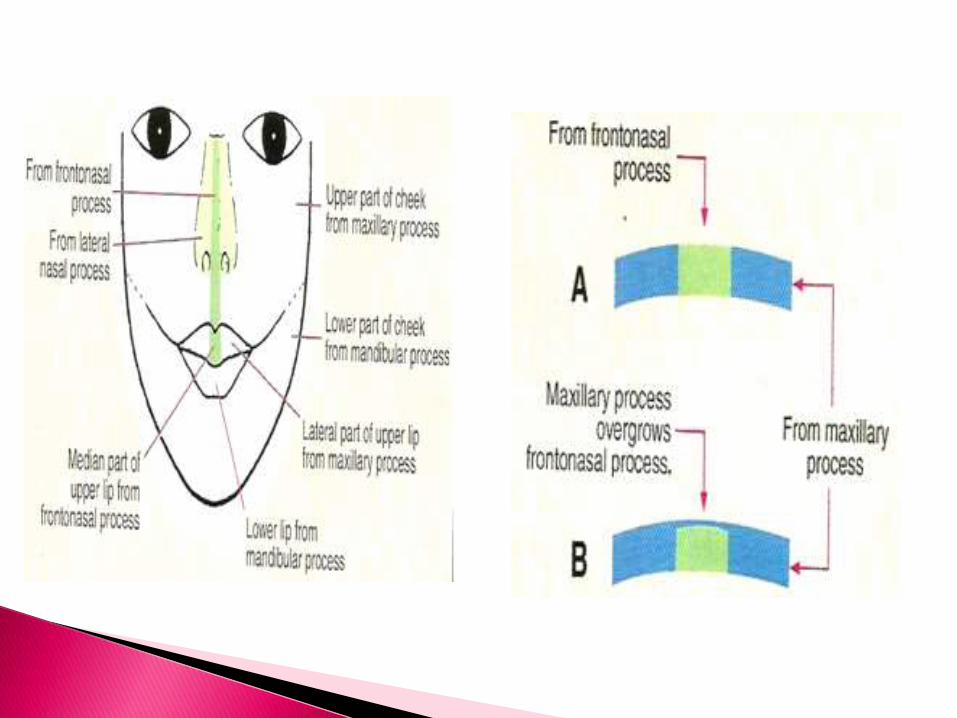
Face-FNP and first pharyngeal arch

Forebrain induces ectoderm



POST SOMITE PERIOD
4-8th week IUL
Maxillary process fuses with MNP and two mandibular process-
narrow the stomodeum
Mouth-continous with oral cavity –due to # of buccopharyngeal
membrane.

Lateral palatal shelves(future secondary palate) –from internal
aspect of maxillary process.
Oral cavity is small and occupied by developing tongue.

6th
week IUL

tongue
Lateral
palatal
shelves
7-8th week of IUL

Head bend over
heart
prominence
Elevation of
face
Growth of
mandible
Increase
volume of oral
cavity
Tongue
descends
Elevation of
palatal shelves

Physical
changes
Blood
flow
Rapid
mitosis
Pressure
changes
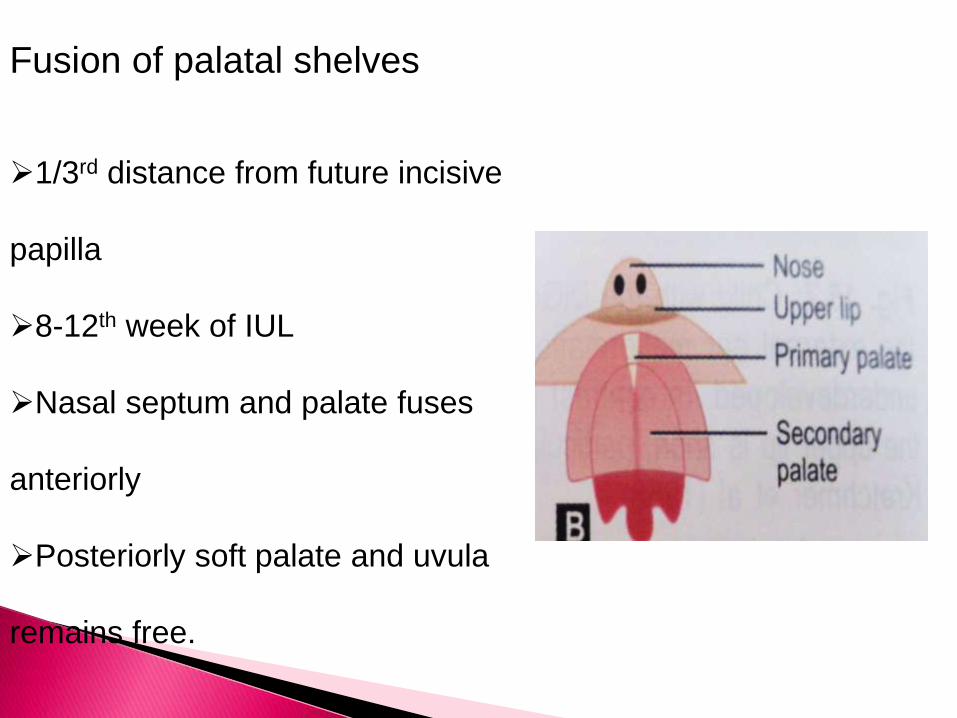
Fusion of palatal shelves
1/3rd distance from future incisive
papilla
8-12th week of IUL
Nasal septum and palate fuses
anteriorly
Posteriorly soft palate and uvula
remains free.

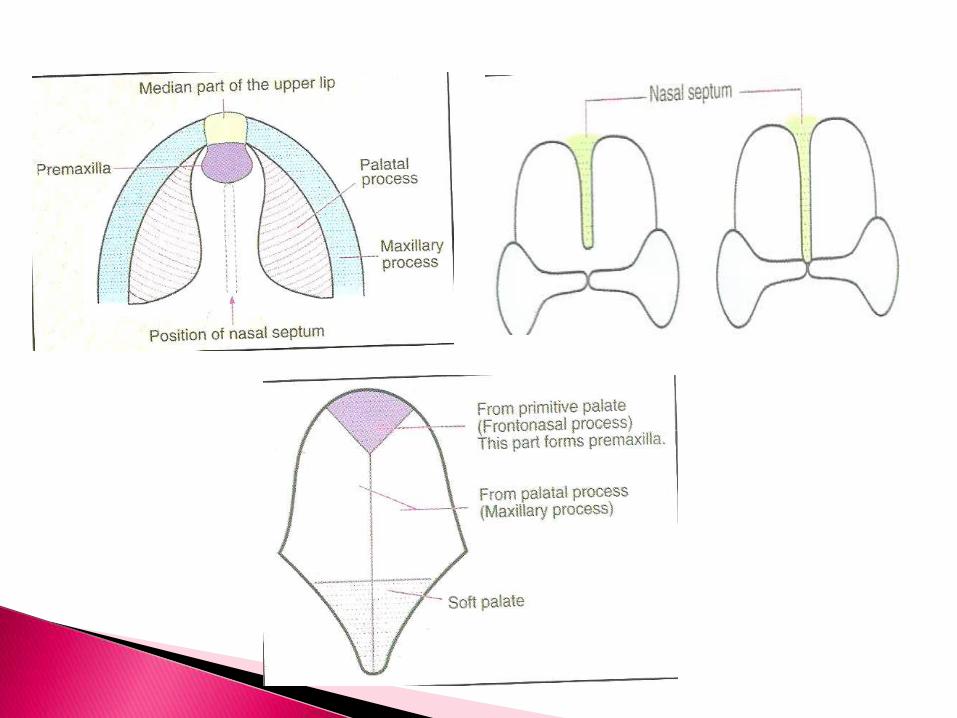
primary
secondary


A cleft palate occurs if the palatal shelves fail to fuse
together or may happen if the tongue fails to descent
due to under-development of the mandible
4th ----8 th weekof IUL ------cleft in primary palate
8th ----12th week of IUL -------cleft between hard
and soft palate
CLEFT
Defective growth of palatine shelves
Failure of elevation of shelves
Failure of fusion of shelves
Post fusion rupture of shelves
Micrognathia as in robin complex
REASONS

Palatal elevation
approximation
contact
adherencefusionDisintegrati
on of epithelium
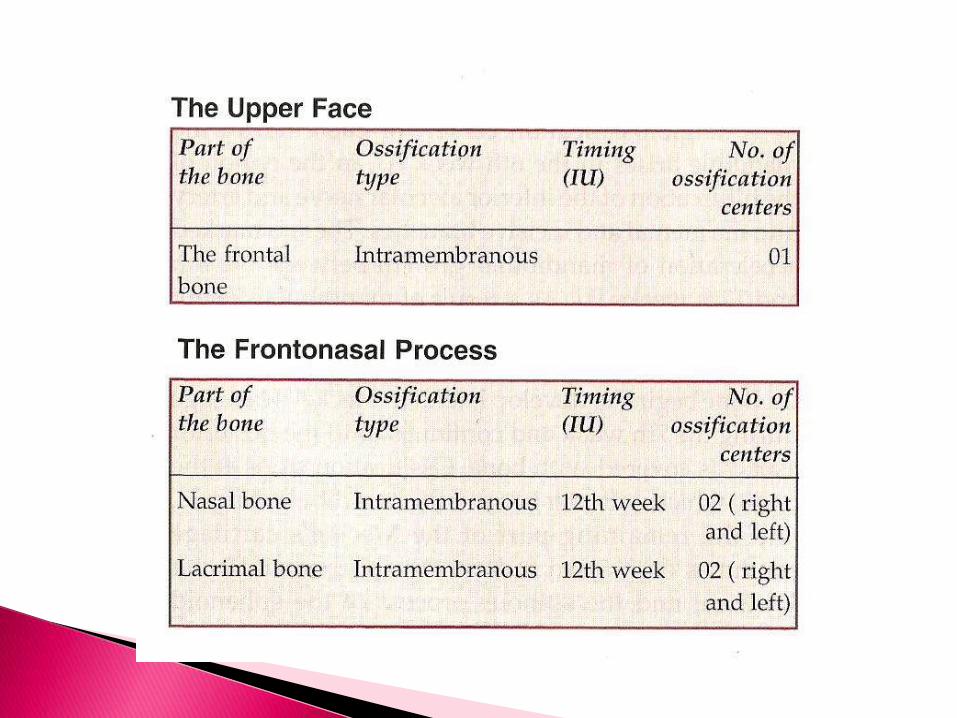
Invasion of mesenchymal cells
Primary intramembraneous ossification centre at 8th
week of IUL at the termination of infra orbital nerve just
above the canine tooth dental lamina
Secondary cartilage ---end of 8th week of IUL in the
region of zygomatic and alveolar process, that fuses with
primary intramembraneous centre .
Premaxillary centre appear anteriorly in each side by 8th
week of IUL fuse with primary maxillary centre
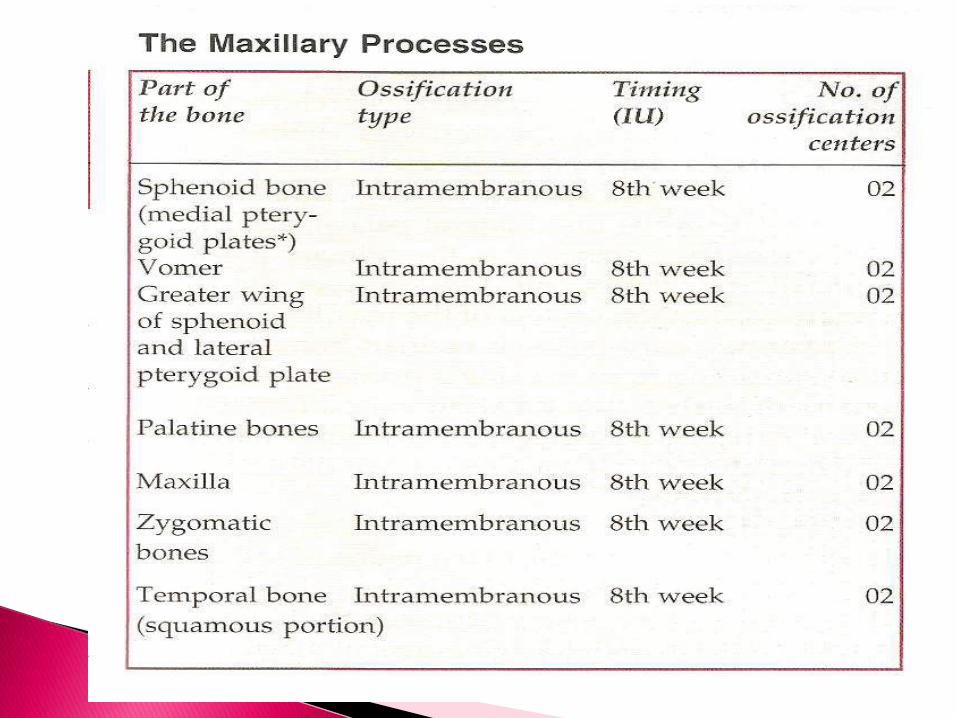
OSSIFICATION

8th
week
4th month(7-18 wks)
Palate undergoes a increase in width than length along
the Mid palatal suture



Median part of upper lip
Position of nasal septum
Nasal septum

DISPLACEMENTGROWTH AT
SUTURES
SURFACE REMODELLING

maxilla
Nasomaxillary complex
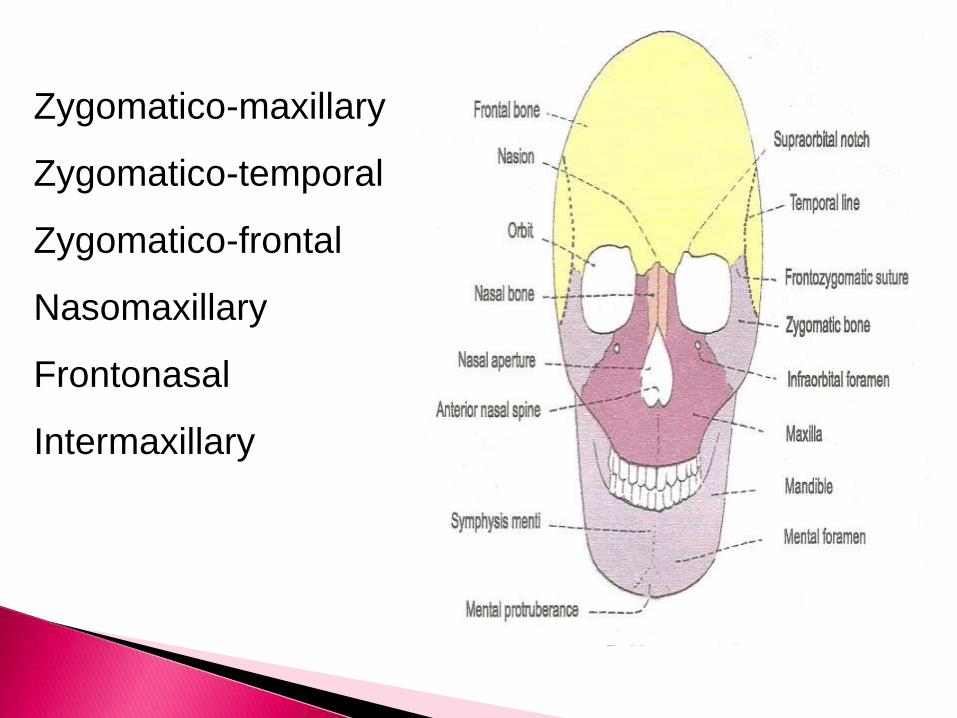
Zygomatico-maxillary
Zygomatico-temporal
Zygomatico-frontal
Nasomaxillary
Frontonasal
Intermaxillary

Zygomatic process
Frontal process
Alveolar process
Palatine process
NMC-
Zygomatic bone
Maxilla
Palate
Nasal bone
Orbital roof

•Cortical remodelling
•Selective apposition and
resorption of cortical
surfaces
drift
•Movement of entire
bone
•Primary displacement
•Secondary displacement
displacement

PRIMARY DISPLACEMENT

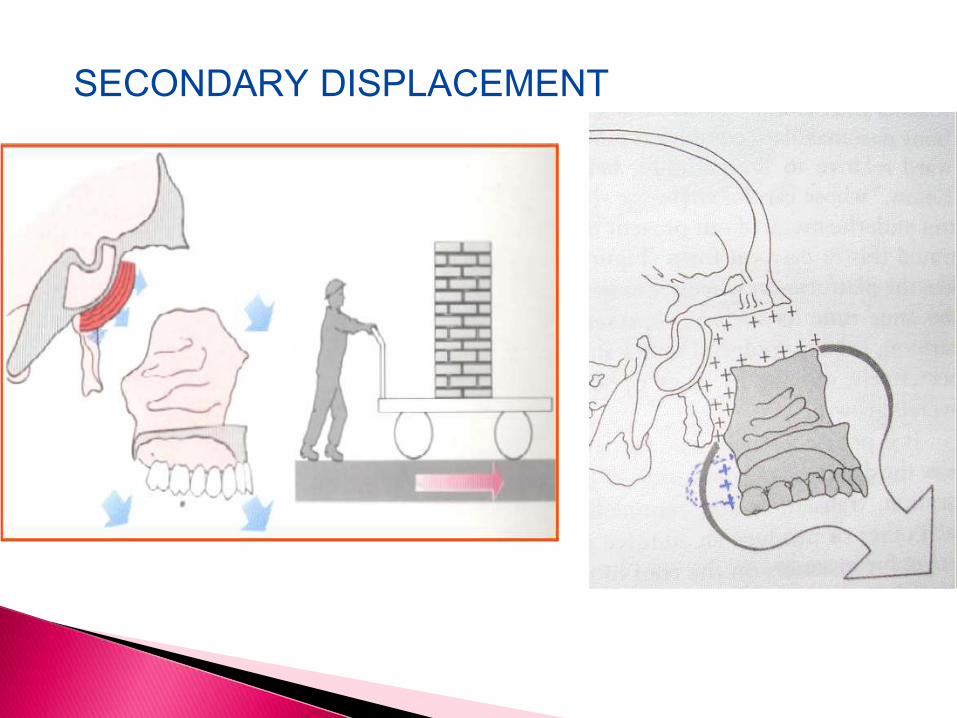
SECONDARY DISPLACEMENT
ENLOW and BANG
As maxilla grows forward the posterior end is depository to
maintain contact with the adjacent bones but the entire anterior surface of maxilla be
comes resorptive to maintain its shape and configuration

KEY
RIDGE
reversal and remodelling
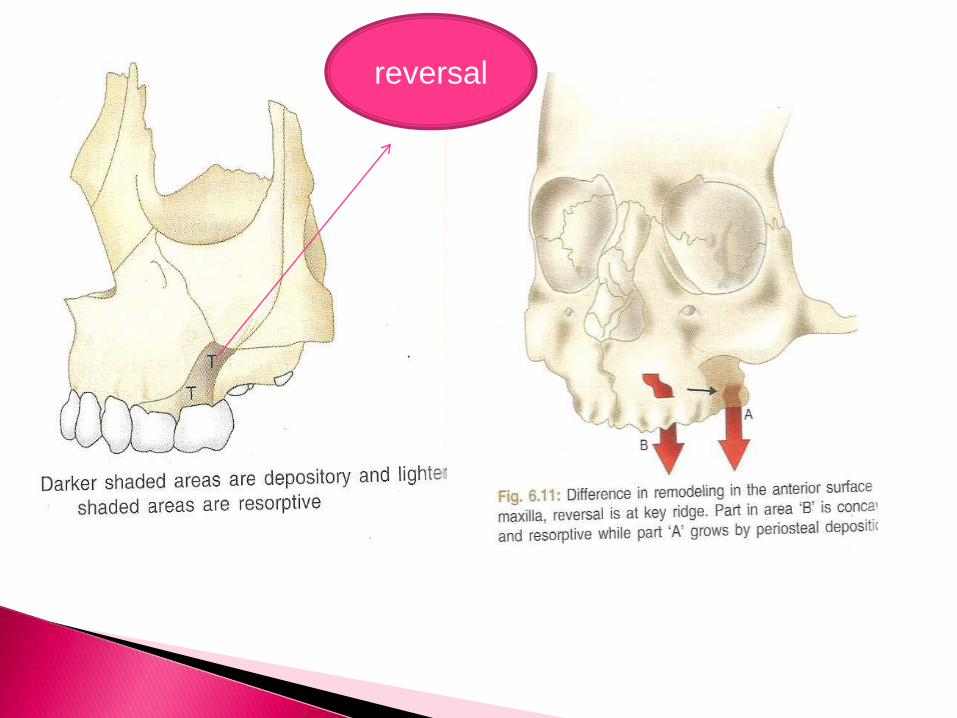
reversal

deposition resorption
AnteriormaxillaAnterior nasal bone
Pyriform rim
Orbit-medial Orbit-lateral
Sinus-medial Sinus rest surfaces
Tuberosityposteriorlyand laterally
Location of
tuberosity is
marked by the
posterior limit of
ACB
PM plane
Posterior limit of
ACB
tuberosity
Junction of corpus
and ramus

Tooth eruption
Vertical drift
Downward displacement

Downward growth and expansion of palate
deposition resorption
Palate roof,nasalroof
Nasal floor

eruption
Vertical
height of
alveolar bone
Depth of
palate
Width of
bone
laterally

V principle and apposition
at intermaxillary suture
Increase maxillary
width
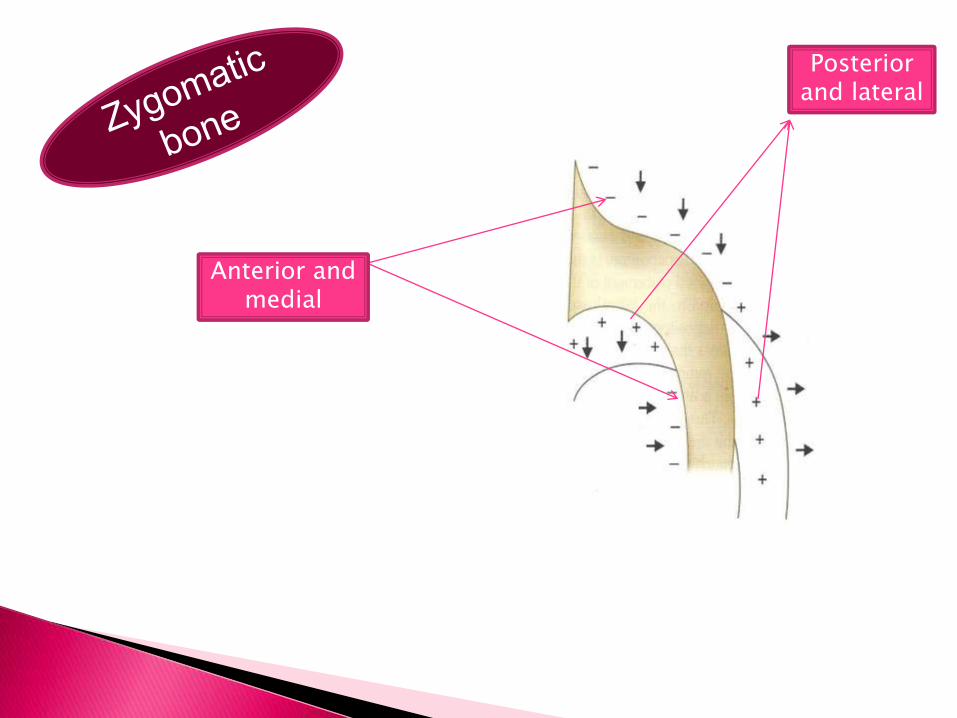
Anterior and medial
Posterior and lateral

nasalFloor and lateral
sinus
roof

ROTATIONS
growth
Passive
displacement
Active
growth

Extreme variations in
rotational pattern leads to
canting and mislift of the
palate and maxillary arch

Bjork and Skeiller..(1972)
Lateral implants placed on anterior and posterior contour of zygomatic process

rotation
internal
external foward
backward

Internal rotation

External rotation
nasal
deposition
Variations in eruption

internal external
Palatal Plane

FORWARD ROTATION
Excessive I.R
Lack of compensatory E.R
Both
Anteinclination
Psuedo-protrusion

The angle formed between the SpP plane and the Pn plane is called the inclination angle or the “J”angle .Mean-85º
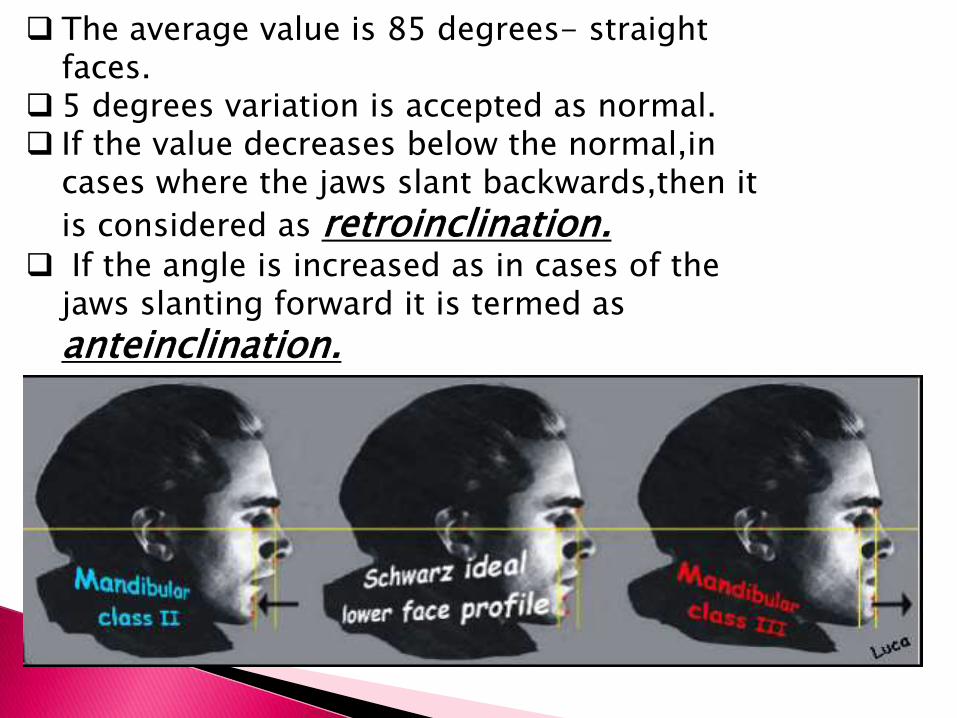
The average value is 85 degrees- straight faces.
5 degrees variation is accepted as normal. If the value decreases below the normal,in
cases where the jaws slant backwards,then it
is considered as retroinclination. If the angle is increased as in cases of the
jaws slanting forward it is termed as
anteinclination.

BACKWARD ROTATION
Retroinclination
Downward and backward tipping of
anterior end of palatal plane and maxillary
base
Jaw bases are translated posteriorly
Upper incisors are lingually tipped
Angle less than 85 degree
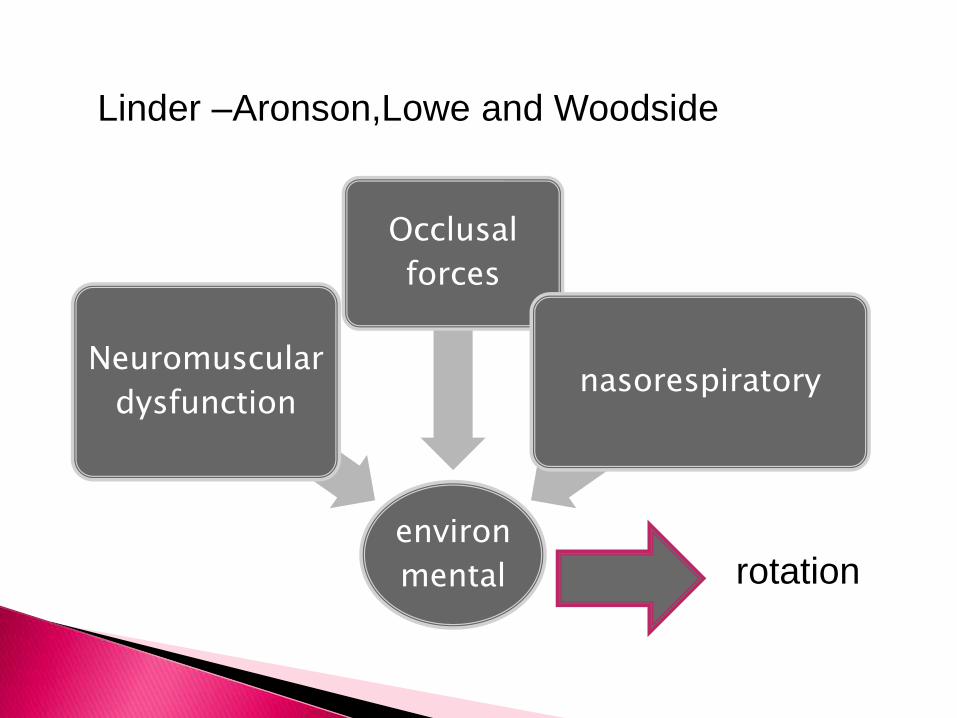
Linder –Aronson,Lowe and Woodside
environ
mental
Neuromuscular
dysfunction
Occlusal
forces
nasorespiratory
rotation


CONCLUSION
Inclination of maxilla can be influenced by fixed mechanotherapy
and functional therapy.
Orthopedic treatment measures should be carefully monitored
during active treatment

Degree of maxillary rotation show variations in
direction and intensity each year.
Its smaller than the mandibular rotation
The rotations of both jaws are not always same
Therefore the interactions between the maxillary and the
mandibular rotations play an important role in the vertical
and sagittal relationships of both jaws