
Growth Hormone Releasing Hormone Receptor Mutations
35
Growth Hormone Releasing Hormone Receptor Mutations Gerhard P. Baumann Northwestern University International Symposium on IGF-1, GH and Ghrelin/GHS, Orlando, March 2011
Transcript of Growth Hormone Releasing Hormone Receptor Mutations

Growth Hormone Releasing Hormone Receptor Mutations
Gerhard P. Baumann
Northwestern University
International Symposium on IGF-1, GH and Ghrelin/GHS, Orlando, March 2011

NH2
Extracellular
Intracellular
COOH
Human GHRH ReceptorGPCR Class B

GHRHR Expression
- Pituitary somatotrophs
- Kidney
- Placenta
- Gonads
- Gut
- Hypothalamus
- Widely expressed at low levels in numerous tissues
Several splice variants exist in tumors and some non-tumorous
tissues. Their biological role is unclear.

Regulation of GHRHR Expression
- Pit-1- NF-1
- AP-1
- CREB
- glucocorticoids
- T3
- estrogen (negative)

GHRHR Signaling Pathways
- Gsa - adenylyl cyclase - cAMP - PKA
- Ca2+ - calmodulin
- PLC - DAG - PKC
- Arachidonic acid - eicosanoid

Human Growth Hormone Releasing Hormone (GHRH)
amide -
amide -
GHRH 1-44
GHRH 1-40
GHRH 1-29- amide

Effects of GHRH in somatotropes
- ProliferationResponsible for the major expansion of the somatotrope
population late in pituitary development
- GH biosynthesis
- GH release

The human GHRHR gene (15,511 bp)
Exon 1 2 3 4 5 6 7 8 9 10 11 12 13
3’5’
3’5’
Exon bp 105 103 108 98 98 133 154 61 70 92 130 42 413
Intron bp 4708 126 696 1154 746 1889 290 481 736 560 722 1796
AAAA
5’ 3’
TM # I II III IV V VI VII
1 2 3 4 5 6 7 8 9 10 11 12
7
p
q
14
ATG TAG
13
Signal


NH2
COOH
Asp Glymouse GHRHR


Mutations in human GHRHR (n = 21 mutant alleles, Feb 2011)
1 2 3 4 5 6 7 8 9 10 11 12 13
3’5’
3’5’
5’ 3’
TM # I II III IV V VI VII
1 2 3 4 5 6 7 8 9 10 11 12 13
Signal
–166(ATG) t > c
–164(ATG) t > c
–124(ATG) a > c
IVS1+1 g > a
IVS1+2 t > c IVS3+1 g > a IVS7+1 g > c
c.1146 G > A
( E322E ) IVS12+2 t > a
V10G
Q43X E72X
H137L L144H
A176V
A222E F242C K329E R357C
D4 D5

I I Y
H G V T
S I S
L A V I
F AV
L T II
V A L
R
RL H C
P
R
K
D
W
L
C S V
T T
F V
G W
L
F
G P
G A
W L V
AW
L
V
T
S
R
W
Y
Q
S
Q
TH
R
I
L
V
R
K
L
E
P
AQ
GS L
S
C
L
L
AS T S
P
S
R
R
A
A
F
L
F
H
SD
DT D H
C
S
A
L
K
D
F
E
IA C W
T
D
D
L
D
N
L
A
GL G I
R
P
L
G
K
SM TC
I
V
Y
Y W W
I
G K I
P V
G V S L
N F
F L G
N I I
L
A K
LV
T
L F
G R V
L
T F L
H Q
NY
V
T
S
F
Y
S
E
E
E
A
L
L
E
LP
V P C A V PY
PP
F PE S
W GT I
TC D R
K VA G S
SES F H S F F D P C
PL
T
V
G
S
C
L
K
S
T
L
V S V
Y
N
H A A
F A
LV
A E A
F T S
W L
M
S
S
T F I
S
P
K
S
L
F
L
F
L
L
N
I I Y
G I H
F L P
F I
T S
P
D
COOH
WW
E
G
A
T
P
W
C
L
L
G
D
WT
APCGLT
TN
PM
EE
AA
QLCASEDE
RL
Q
T
I
F
DC
EP
H M H NH2
SM TC SM TC
E L G
L
Q
L
F
A
C
L
G
V
S
I F
I
F Y
QN
E
R
V
T
E
I
S
R
K
W
H
PW A
GH
DP
ELLRTRAKWTTPSRSAAKL VTSMC
Gln StopCanada
Little
GlyAsp
Sindh
Glu StopCanada
HisLeu
Spain
USA
Brazil
GluAla
Pakistan CysPhe
USA
Morocco
GluLys
Portugal
Arg Cys
Israel
D4
Japan
D5
Canada
Glu Glu
Japan
Pakistan
Japan, Portugal, Brazil, Morocco, ItalyPromoter, , Val Gly
Splice donor site mutation
Splice silencer mutation
LeuHis
Canada

GHRHR mutations: Mechanism of inactivation
Nonsense mutations (n=2) Truncation, nonsense-mediated mRNA decay
Splice site mutations (n=5) Intronic readthrough, premature stop
Exonic splicing silencer mutation (n=1) Exon skipping
Promoter mutations (n=3) Decreased Pit-1 binding to P1 or P2 elements
Missense mutations (n=8) Loss of GHRH binding activity (n=6)
Retention in ER (V10G)
Not determined (R357E)
Alba & Salvatori, J Endo 2005

Activating mutations in human GHRHR ?
To date, no gain of function mutations in the GHRHR have
been described.
Extensive screening of over 130 somatotrope tumors for
somatic activating mutations in GHRHR, as a potential
basis for constitutive proliferative drive, has not discovered
any such mutations.
However, two somatic inactivating mutations (W250X and
G294R) have been described in GH-producing pituitary
tumors.
A number of polymorphisms without clinical significance are
known to exist.

Clinical manifestations

Dr. Aguiar-Oliveira and the Itabaianinha cohort

Clinical manifestations (cont.)
Mode of inheritance: autosomal recessive (homozygous or compound heterozygous).
Very high penetrance
Two large kindreds with high degrees of consanguinity exist in
Pakistan (Dwarfs of Sindh) and in Itabaianinha, Brazil.
Founder mutations are implicated in both.
Heterozygous carriers are physically normal and biochemically
intermediate to near-normal.
Phenotype: Isolated GH deficiency type IB
– postnatal growth retardation → dwarfism
– some basal GH production
– other pituitary functions normal
– delayed puberty, menopause at normal age
– other features typical for GH deficiency (some exceptions)
Pituitary hypoplasia (anterior lobe)
Relative microcephaly (Head circumference -4.1 ± 0.2 SDS)
No. of cases reported: ~ 180 (~100 in Itabaianinha; ~45 in Pakistan/India)

Clinical manifestations (cont.)
Short stature: Full impact of mutation seen only in adults
Adult height (Sindh): Male 130 ± 10.6 cm (118-148) -8.9 ± 1.2 SDS
Female 113.5 cm (113-114) -8.4 SDS
(Brazil): Male 127 ± 7.6 cm (110-140) -7.6 ± 0.9 SDS
Female 119 ± 8.5 cm (107-129) -7.8 ± 0.9 SDS
Upper-lower segment and height-arm span ratio: Normal
Waist-hip ratio (Sindh): 0.92 ± 0.05 (elevated)
(Brazil): 0.97 ± 0.02 (controls 0.90 ± 0.02)
Bone age delayed
Anthropometric and clinical data
- No or minimal dysmorphism
- No microphallus
- No hypoglycemia
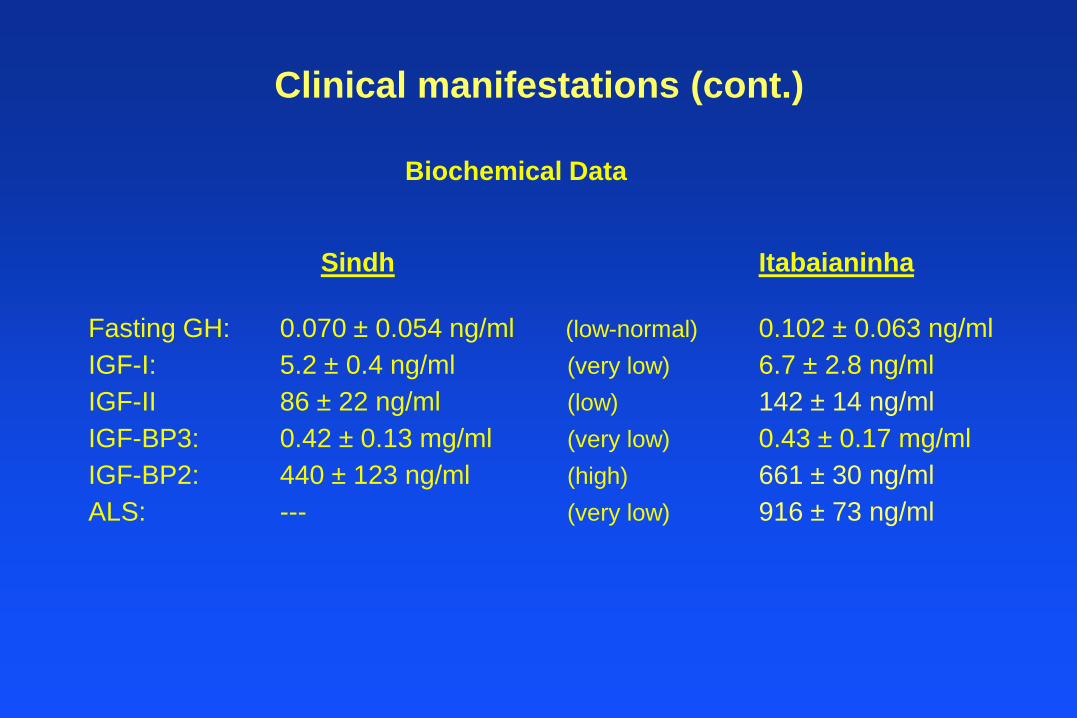
Biochemical Data
Sindh Itabaianinha
Fasting GH: 0.070 ± 0.054 ng/ml (low-normal) 0.102 ± 0.063 ng/ml
IGF-I: 5.2 ± 0.4 ng/ml (very low) 6.7 ± 2.8 ng/ml
IGF-II 86 ± 22 ng/ml (low) 142 ± 14 ng/ml
IGF-BP3: 0.42 ± 0.13 mg/ml (very low) 0.43 ± 0.17 mg/ml
IGF-BP2: 440 ± 123 ng/ml (high) 661 ± 30 ng/ml
ALS: --- (very low) 916 ± 73 ng/ml
Clinical manifestations (cont.)

Anterior Pituitary Hypoplasia
Lin & Rosenfeld, Nature 1993
Little mouse
Ant. pituitary volume
330 ± 96 mm3
103 ± 21 mm3
normal

Is there a genotype-phenotype relationship?
Insufficient data
- Extensive information only available for 2 severely inactivating
(null) mutations
- Other, potentially milder mutations only phenotyped in 1-3 patients
- Patients phenotyped at varying ages are difficult to compare
- Functional differences shown in vitro (e.g., cAMP generation)
not always borne out in vivo
Probably

Novel insights gained into GH biology
Regulation of GH secretion
- Generation of secretory pulses
- Role of GHS
Natural history of life-long, severe, untreated, isolated GH deficiency
- Cardiovascular disease
- Bone and skeletal disease
- Quality of life
- Life span

Clock Time
8:00 14:00 20:00 2:00 8:00
Pla
sm
a G
H (
µg
/L)
0.00
0.04
0.08
0.12
0.16
0.20
Patient 1
SLEEP
Plasma GH
8:00 14:00 20:00 2:00 8:00
Pla
sm
a G
H (
µg
/L)
0.00
0.02
0.04
0.06
0.08
0.10
Patient 4
8:00 14:00 20:00 2:00 8:00
GH
se
cre
tio
n r
ate
(µ
g/L
/min
)
0.00
0.02
0.04
0.06
0.08
0.10
Patient 4
8:00 14:00 20:00 2:00 8:00
GH
se
cre
tio
n r
ate
(µ
g/L
/min
)
0.00
0.04
0.08
0.12
0.16
0.20
Patient 1
GH Secretion Rate
GH Secretion Profiles in GHRH-Receptor Deficiency

GH Secretion in GHRH-Receptor Deficiency
Patient 24 h mean Number of Half-life GH productionnumber plasma GH peaks/24 h rate
( ng/ml) (min) (ng/ml/24 h)
1 0.052 18 14.6 3.41
2 0.020 --- ---- ----
3 0.021 16 16.1 1.42
4 0.046 12 15.7 2.95
Mean 0.035 15.3 15.5 2.59
Normal mean 1.394 19.0 16.5 80.2

Response to hexarelin in GHRH-R Deficiency
Minutes
-15 0 15 30 45 60 90 120
Co
rtis
ol (
g/d
l)
0
5
10
15
20
25
30
Minutes
-15 0 15 30 45 60 90 120
AC
TH
(p
g/m
l)
0
50
100
150
200
Hex Hex
-15 0 15 30 45 60 90 120
GH
(n
g/m
l)
0
5
10
15
20
-15 0 15 30 45 60 90 120
Pro
lacti
n (
ng
/ml)
0
5
10
15
20
25
HexHex
Minutes
-15 0 15 30 45 60 90 120
Pla
sm
a G
H (
µg
/L)
0.00
0.25
0.50
0.75
1.00
1.25
1.50
#1
#4
#3
#2
Hexarelin

Cardiovascular risk factors in Itabaianinha cohort
Abdominal fat increased
Blood pressure increased
LDL-cholesterol increased
C-reactive protein increased
No carotid intima-media thickening
No increased cardiovascular deaths
GH treatment increases carotid intima-media thickening

Bone mineral density
Areal BMD at lumbar spine, femoral neck, forearm and total body
is decreased by DEXA (mean Z scores -1.7 to – 3.7) (Sindh)
BMD at calcaneus is decreased by quantitative ultrasound (mean Z score -1.15)
(Itabaianinha).
No evidence for an increased fracture rate.
GH therapy for 6 months mildly improved BMD (Z score -0.78)
Potential artifact due to small bone size is not accounted for.
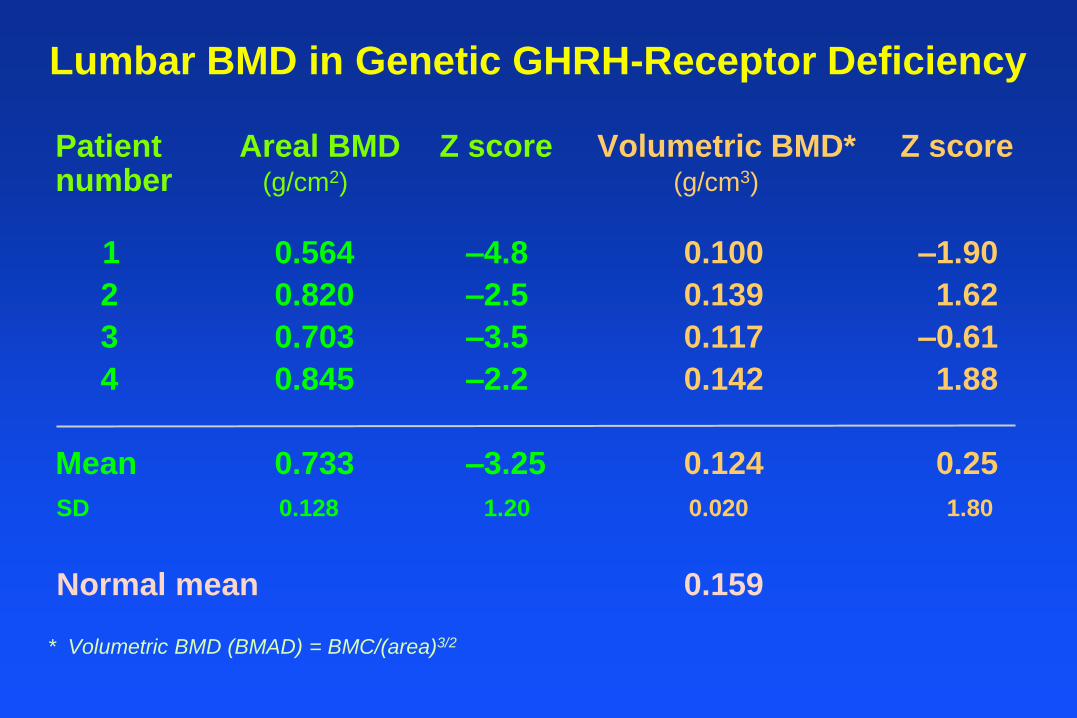
Lumbar BMD in Genetic GHRH-Receptor Deficiency
Patient Areal BMD Z score Volumetric BMD* Z scorenumber (g/cm2) (g/cm3)
1 0.564 –4.8 0.100 –1.90
2 0.820 –2.5 0.139 1.62
3 0.703 –3.5 0.117 –0.61
4 0.845 –2.2 0.142 1.88
Mean 0.733 –3.25 0.124 0.25
SD 0.128 1.20 0.020 1.80
Normal mean 0.159
* Volumetric BMD (BMAD) = BMC/(area)3/2

Quality of Life in Itabaianinha cohort
QoL measured by Life Satisfaction Hypopituitarism Module (QLS-H)
- No difference between GH deficient and control subjects
- No improvement in QoL after 6 months of GH treatment
(exception: satisfaction with improved physical endurance)
- No difference after 12 months washout time

Life span in GH deficiency
- GH-deficient and GH-resistant rodents have a prolonged life span.
(little mouse, GHR-KO mouse, Snell, Ames mouse, spontaneous dwarf rat, etc.)
- The Krk dwarfs (harboring a PROP-1 mutation) are said to live to unusually old age.
- Acquired adult GH deficiency is associated with a shortened life span.
- GH is frequently portrayed as an anti-aging agent → beneficial?
- A Swiss patient cohort with a GH-1 gene deletion had a shortened life span.
- How to reconcile these different observations?

Longevity in untreated GHRHR Deficiency
Aguiar-Oliveira et al, JCEM 2010
All ages Age >20

Summary: Genetic GHRH-Receptor Deficiency
Twenty-one mutant alleles reported, all are inactivating
Recessive inheritance, 100% penetrance
May account for ~10% of familial isolated GH deficiency
Heterozygotes show normal height and mild biochemical and body composition abnormalities
Phenotype:
- Isolated GH deficiency type IB
- Ultradian GH rhythm persists, with severely decreased pulse amplitudes, but normal pulse frequency
- Good response to GH therapy
- Proportionate short stature
- Relative eumorphism
- Relative microcephaly, apparent normal intelligence

Summary: Genetic GHRH-Receptor Deficiency
Phenotype, continued:
- Anterior pituitary hypoplasia (somatotrope deficiency)
- Absence of childhood hypoglycemia
- Characteristic high-pitched, raspy voice in males
- Absence of microphallus
- Delayed puberty (2-3 years)
- Fertility and lactation appear normal
Parity is low, possibly because of late pairing and obstetricalconsiderations
- Probably normal or near-normal bone mineral density
- Systolic hypertension (Itabaianinha people)

Summary: Genetic GHRH-Receptor Deficiency
Phenotype, continued:
- Increased % fat (abdominal), low lean body mass
- Increased LDL cholesterol, C-reactive protein
- Normal carotid intima/media thickness
- No phenotypic evidence of GHRH resistance in extrapituitary tissues, despite widespread expression of GHRH and the GHRH-receptor (exception: relative microcephaly)


















