Granzyme B PET Imaging as a Predictive Biomarker of ... · may be more valuable for predicting...
11
Microenvironment and Immunology Granzyme B PET Imaging as a Predictive Biomarker of Immunotherapy Response Benjamin M. Larimer 1 , Eric Wehrenberg-Klee 1 , Frank Dubois 1 , Anila Mehta 1 , Taylor Kalomeris 1 , Keith Flaherty 2,3 , Genevieve Boland 4 , and Umar Mahmood 1 Abstract While cancer immunotherapy can produce dramatic responses, only a minority of patients respond to treatment. Reliable response biomarkers are needed to identify responders, and conventional imaging modalities have not proved adequate. Here, we provide a preclinical proof of concept for the use of granzyme B, a downstream effector of tumoral cytotoxic T cells, as an early biomarker for tumors responding to immunotherapy. We designed novel PET imaging probes for the murine and human granzyme B isoforms that specifically and quantitatively bind granzyme B. Immunotherapy-treated mice were imaged prior to therapy-induced tumor volume reduction. Imaging distinguished treated responders from nonresponders with excellent predictive ability. To assess the clinical value of a granzyme B imaging paradigm, biopsy specimens from melanoma patients on check- point inhibitor therapy were analyzed. A marked differential in granzyme B expression was observed between treated responders and nonresponders. Additionally, our human probe was able to specifically detect granzyme B expression in human samples, providing a clear candidate for clinical application. Overall, our results suggest granzyme B PET imaging can serve as a quantita- tively useful predictive biomarker for efficacious responses to cancer immunotherapy. Cancer Res; 77(9); 2318–27. Ó2017 AACR. Introduction Cancer immunotherapy, and PD-1 blockade in particular, has represented a significant advance in cancer therapy. While responses to anti–PD-1 monotherapy and combination regi- mens, including anti–PD-1 paired with anti–CTLA-4, have generated well-warranted enthusiasm for the future of cancer immunotherapy, several limitations have yet to be addressed. Of particular importance is predicting which patients will benefit from this novel approach. Efficacies vary widely across tumor and treatment type, with objective response rates ranging between 5% and 60% (1, 2). Immunotherapy is also often associated with severe immune-related adverse events, includ- ing hepatitis, colitis, and even death, with grade III/IV adverse events occurring in up to 50% of patients on PD-1/CTLA-4 inhibitor combination regimens (3, 4). Early differentiation of treated responders from nonresponders would help to triage nonresponding patients away from ineffective therapies, reduc- ing unnecessary side effects and allowing the opportunity for alternative therapeutic strategies. Despite the clear benefit of early identification, it remains highly difficult to differentiate treatment responders from nonresponders using standard imaging techniques (5). PET- CT with 18 F-fluorodeoxyglucose ( 18 F-FDG), an imaging meth- od widely used to assess response to traditional therapy, is unfortunately limited in cancer immunotherapy. This is due in part to a metabolically active tumoral immune cell infil- trate, which can cause expansion in tumor volume, increased glucose uptake, and even the development of new detectable lesions, features indistinguishable from tumor progression (6, 7). In addition to imaging, emphasis has been placed on identifying nonimaging biomarkers for both pretreatment stratification and response assessment. Several of these strate- gies enrich for responding patients, but are insufficient for individual response prediction. For example, tumors with greater than 50% positive staining for PD-L1 have a 30% response rate, compared with an 18% response rate in patients with >1% positive staining, in advanced non–small cell lung cancer treated with pembrolizumab (8). These biopsy-depen- dent measures face several limitations, as biopsy is typically obtained only once prior to therapy, and the collected tissue from an 18-gauge percutaneous biopsy (0.011 cm 3 ) represents only approximately 0.1% of a typical lesion (10 cm 3 ). The small sampling size is unlikely to accurately represent the markedly heterogeneous tumoral immune infiltrate within a single tumor focus or across metastatic sites. Because of the potential limitations of biopsy, alternative imaging approaches monitoring CD8 þ and CD3 þ T-cell infiltration and PD-1/PD- L1 expression have been explored preclinically, with mixed efficacy based on tumor model and therapy utilized (9–11). Factors that may hinder the successful correlation of cytotoxic T-cell infiltration with therapeutic efficacy include a tolero- genic tumor microenvironment that inhibits the activity of cytotoxic T cells, as well as phenomena such as T-cell 1 Athinoula A. Martinos Center for Biomedical Imaging, Department of Radiology, Massachusetts General Hospital, Boston, Massachusetts. 2 Department of Med- icine, Harvard Medical School, Boston, Massachusetts. 3 Department of Medical Oncology, Massachusetts General Hospital, Boston, Massachusetts. 4 Depart- ment of Surgery, Massachusetts General Hospital, Boston, Massachusetts. Note: Supplementary data for this article are available at Cancer Research Online (http://cancerres.aacrjournals.org/). Corresponding Author: Umar Mahmood, Massachusetts General Hospital, 149 13th Street, Room 5.407, Charlestown, MA 02129. Phone: 617-726-6477; Fax: 617-726-7422; E-mail: [email protected] doi: 10.1158/0008-5472.CAN-16-3346 Ó2017 American Association for Cancer Research. Cancer Research Cancer Res; 77(9) May 1, 2017 2318 on June 9, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Transcript of Granzyme B PET Imaging as a Predictive Biomarker of ... · may be more valuable for predicting...

Microenvironment and Immunology
Granzyme B PET Imaging as a PredictiveBiomarker of Immunotherapy ResponseBenjamin M. Larimer1, Eric Wehrenberg-Klee1, Frank Dubois1, Anila Mehta1,Taylor Kalomeris1, Keith Flaherty2,3, Genevieve Boland4, and Umar Mahmood1
Abstract
While cancer immunotherapy can produce dramatic responses,only a minority of patients respond to treatment. Reliableresponse biomarkers are needed to identify responders, andconventional imaging modalities have not proved adequate.Here, we provide a preclinical proof of concept for the use ofgranzyme B, a downstream effector of tumoral cytotoxic T cells, asan early biomarker for tumors responding to immunotherapy.Wedesigned novel PET imaging probes for the murine and humangranzyme B isoforms that specifically and quantitatively bindgranzyme B. Immunotherapy-treated mice were imaged prior totherapy-induced tumor volume reduction. Imaging distinguished
treated responders from nonresponders with excellent predictiveability. To assess the clinical value of a granzyme B imagingparadigm, biopsy specimens from melanoma patients on check-point inhibitor therapy were analyzed. A marked differential ingranzyme B expression was observed between treated respondersand nonresponders. Additionally, our human probe was able tospecifically detect granzyme B expression in human samples,providing a clear candidate for clinical application. Overall, ourresults suggest granzyme B PET imaging can serve as a quantita-tively useful predictive biomarker for efficacious responses tocancer immunotherapy. Cancer Res; 77(9); 2318–27. �2017 AACR.
IntroductionCancer immunotherapy, and PD-1 blockade in particular,
has represented a significant advance in cancer therapy. Whileresponses to anti–PD-1 monotherapy and combination regi-mens, including anti–PD-1 paired with anti–CTLA-4, havegenerated well-warranted enthusiasm for the future of cancerimmunotherapy, several limitations have yet to be addressed.Of particular importance is predicting which patients willbenefit from this novel approach. Efficacies vary widely acrosstumor and treatment type, with objective response rates rangingbetween 5% and 60% (1, 2). Immunotherapy is also oftenassociated with severe immune-related adverse events, includ-ing hepatitis, colitis, and even death, with grade III/IV adverseevents occurring in up to 50% of patients on PD-1/CTLA-4inhibitor combination regimens (3, 4). Early differentiation oftreated responders from nonresponders would help to triagenonresponding patients away from ineffective therapies, reduc-ing unnecessary side effects and allowing the opportunity foralternative therapeutic strategies.
Despite the clear benefit of early identification, it remainshighly difficult to differentiate treatment responders fromnonresponders using standard imaging techniques (5). PET-CT with 18F-fluorodeoxyglucose (18F-FDG), an imaging meth-od widely used to assess response to traditional therapy, isunfortunately limited in cancer immunotherapy. This is duein part to a metabolically active tumoral immune cell infil-trate, which can cause expansion in tumor volume, increasedglucose uptake, and even the development of new detectablelesions, features indistinguishable from tumor progression(6, 7). In addition to imaging, emphasis has been placed onidentifying nonimaging biomarkers for both pretreatmentstratification and response assessment. Several of these strate-gies enrich for responding patients, but are insufficient forindividual response prediction. For example, tumors withgreater than 50% positive staining for PD-L1 have a 30%response rate, compared with an 18% response rate in patientswith >1% positive staining, in advanced non–small cell lungcancer treated with pembrolizumab (8). These biopsy-depen-dent measures face several limitations, as biopsy is typicallyobtained only once prior to therapy, and the collected tissuefrom an 18-gauge percutaneous biopsy (0.011 cm3) representsonly approximately 0.1% of a typical lesion (10 cm3). Thesmall sampling size is unlikely to accurately represent themarkedly heterogeneous tumoral immune infiltrate within asingle tumor focus or across metastatic sites. Because of thepotential limitations of biopsy, alternative imaging approachesmonitoring CD8þ and CD3þ T-cell infiltration and PD-1/PD-L1 expression have been explored preclinically, with mixedefficacy based on tumor model and therapy utilized (9–11).Factors that may hinder the successful correlation of cytotoxicT-cell infiltration with therapeutic efficacy include a tolero-genic tumor microenvironment that inhibits the activity ofcytotoxic T cells, as well as phenomena such as T-cell
1Athinoula A.MartinosCenter for Biomedical Imaging, Department of Radiology,Massachusetts General Hospital, Boston, Massachusetts. 2Department of Med-icine, Harvard Medical School, Boston, Massachusetts. 3Department of MedicalOncology, Massachusetts General Hospital, Boston, Massachusetts. 4Depart-ment of Surgery, Massachusetts General Hospital, Boston, Massachusetts.
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
Corresponding Author: Umar Mahmood, Massachusetts General Hospital, 14913th Street, Room 5.407, Charlestown, MA 02129. Phone: 617-726-6477; Fax:617-726-7422; E-mail: [email protected]
doi: 10.1158/0008-5472.CAN-16-3346
�2017 American Association for Cancer Research.
CancerResearch
Cancer Res; 77(9) May 1, 20172318
on June 9, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

exhaustion or anergy that induce immunotolerance (12, 13). Inthese cases, T cells are present within the tumor, yet remaininactive, allowing for continued tumor progression.
By focusing on active rather than total tumor immuneinfiltrate, an imaging biomarker of cytotoxic T-cell activitymay be more valuable for predicting response to cancerimmunotherapy. Granzyme B is a serine-protease released byCD8þ T cells and natural killer cells during the cellularimmune response and represents one of the two dominantmechanisms by which T cells mediate cancer cell death(14, 15). We set out to design a PET imaging agent capableof detecting the release of this enzyme by actively engagedimmune cells. Such an imaging agent would allow for repeatednoninvasive and systemic interrogation of the tumoralresponse to cancer immunotherapy and provide insight intoa major biochemical mechanism responsible for immune-mediated cell death. We began with development granzymeB–specific PET imaging agent (GZP) designed from the opti-mal cleavage sequence for murine granzyme B with furthermodifications to induce irreversible binding and allow forlabeling with a suitable PET-detectible radiometal (16). Wedemonstrated that GZP has high affinity and specificity forgranzyme B, and showed in a CT26 syngeneic cancer modelthat GZP uptake correlates closely with tumoral granzyme Bexpression. We then sought to demonstrate the utility of GZPas a predictive imaging biomarker for successful immunother-apy. PET imaging was able to differentiate with excellentaccuracy between treated responders and treated nonrespon-ders prior to tumor volume divergence. We extended ourfindings into humans by developing a human-specific gran-zyme B agent and interrogated it in a cohort of biopsy speci-mens obtained from patients on checkpoint inhibitor therapy.Granzyme B expression from these on-treatment specimenswas markedly different between treated responders and treatednonresponders, and our humanized probe was able to detectthese changes in expression with high correlation to anti-granzyme B antibody staining in the same samples. Theseresults suggest that granzyme B PET imaging represents abiomarker of active cytotoxic immune response, with valuablepredictive capability in immune-oncology.
Materials and MethodsSyngeneic colon cancer model of immunotherapy
Mice were housed and maintained by the Center for Com-parative Medicine following animal protocols approved by theMassachusetts General Hospital Institutional Animal Care andUse Committee. CT26 murine colon carcinoma cells wereacquired from ATCC and cultured in RPMI. Monthly myco-plasma testing was performed by PCR screening and cells werediscarded after 15 passages. All cell-based experiments weredone with cells acquired within 6 months from ATCC during2016 in order to ensure fidelity of the cell line identity. CT26cells (1�106) were prepared in a 1:1 (v:v) ratio in Matrigel(Corning) and injected subcutaneously into the right shoulderof Balb/c mice. Anti-mouse PD-1 (clone RMP1-14) and anti-mouse CTLA-4 (clone 9D9) were obtained from Bio X Cell. Allmice were treated by intraperitoneal injection of saline (vehi-cle), 200 mg anti-PD1 (monotherapy), or both 200 mg anti-PD1,and 100 mg anti–CTLA-4 (combination therapy) on days 3, 6,and 9 following CT26 tumor inoculation (17).
Ex vivo tumor biochemical analysisFor ex vivo analysis, mice were sacrificed on the specified
day and the entire tumor excised and either lysed for Westernblot analysis or fixed in 10% formalin and paraffin embeddedfor immunohistochemical or immunofluorescence staining.For Western blot analyses, anti-CD8 (Ab108292, Abcam),anti-CD3 (sc-20047, Santa Cruz Biotechnology), anti-CD4(sc-19643, Santa Cruz), anti-FoxP3 (12653s, Cell SignalingTechnology), anti-pSTAT (700349, ThermoFisher), anti-Gran-zyme B (4275s, Cell Signaling Technology), and anti–b-actin(Cell Signaling Technology 4970S) were used at the manu-facturer's recommended concentration. For immunohis-tochemistry analysis, granzyme B (Ab4059, Abcam) and CD3(Ab56090, Abcam) antibodies were detected using biotiny-lated goat-anti-rabbit antibodies with the Signal Stain BoostIHC Detection Reagent (Abcam). For immunofluorescencestaining, granzyme B was detected with Ab4059 and Alexa-Fluor 488 goat anti-rabbit secondary (Life Technologies);CD3 was detected with anti-CD3 clone PC3/188A (SantaCruz) and AlexaFluor 594 goat anti-mouse secondary (LifeTechnologies).
NOTA-GZP synthesis and 68Ga radiolabellingNOTA–b-Ala–Gly–Gly–Ile–Glu–Phe–Asp–CHO (NOTA-GZP)
and biotin–b-Ala–Gly–Gly–Ile–Glu–Pro–Asp–CHO (hGZP)were synthesized using standard FMOC chemistry (18). Chem-ical purity was analyzed by HPLC and mass spectroscopy. 68Gawas obtained from a 68Ge/68Ga generator (iThemba Labs)eluted with 0.6N HCl. Radiolabeling proceeded as previouslydescribed with minor modifications (19). Briefly, the eluentwas equilibrated to pH 3.5-4.0 with 2 mol/L HEPES followedby addition of 100 mg NOTA-GZP. The labeling reaction pro-ceeded at room temperature for 10 minutes. The reactionproduct was loaded on a reverse-phase C18 Sep-Pak minicartridge and eluted with 200 mL of 70% ethanol. The finalformulation was adjusted to 10% ethanol in saline. The chem-ical and radiochemical purity of 68Ga-NOTA-GZP was mea-sured through radio thin-layer chromatography.
NOTA-GZP affinity and specificity determinationPro-granzyme B (R&D Systems) was activated to granzyme B
using cathepsin B (R&D Systems) following the manufacturer'sprotocol. Enzyme activity was assessed by cleavage of BOC–Ala–Ala–Asp–SBZL (Sigma) and reaction with DTNB (Sigma)with absorbance measurements at 405 nm (NanoDrop 2000Spectrophotometer, Thermo Scientific). Serial dilutions of non-radioactive gallium-labeled NOTA-GZP were used to inhibitgranzyme B by incubation at 37�C for 30 minutes prior toaddition of substrate. Additionally, 68Ga-NOTA-GZP was incu-bated with the activated forms of granzyme B, granzyme A(R&D Systems), granzyme H (R&D Systems), granzyme K(Enzo Life Sciences), and pro–granzyme B to assess the spec-ificity of the peptide. After a 30-minute incubation at 37�C,enzymes were purified by size exclusion chromatography andbound radioactivity assessed by gamma counter (Wizard 2480,Perkin Elmer).
In vivo PET imaging and tumor growth curve analysesFor all imaging studies, Balb/c mice were injected with CT26
cells and treated as described previously. On either day 12 or
Granzyme B PET Imaging Predicts Immunotherapy Response
www.aacrjournals.org Cancer Res; 77(9) May 1, 2017 2319
on June 9, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

14, mice were injected intravenously with �37 MBq of 68Ga-NOTA-GZP and imaged 1 hour following injection. Imageswere acquired on a rodent Triumph PET/CT (GE Healthcare).PET images were obtained for 15 minutes in a single bedposition, followed by CT acquisition. Images were constructedusing 3D-MLEM (4 iterations and 20 subsets) and corrected forscatter and randoms. The mean standard uptake value (SUV-mean) for each tumor was calculated in a 3D region of interestmanually drawn around the tumor using CT-anatomic corre-lation. A region of interest was also drawn around the leftventricle of the heart to calculate blood pool activity as ameasure of nonspecific signal. Images were postprocessedusing VivoQuant software (InviCRO). Dynamic PET Imagingdata were acquired over a 2-hour period, and time activitycurves were generated using the same region of interest meth-od as for static image acquisition. A noncompartmentalPATLAK analysis was performed based on the assumed non-reversible binding of the peptide to granzyme B. For ex vivocorrelation studies, mice were sacrificed immediately follow-ing imaging. For survival and response prediction, mice werereturned to normal housing following radioactive decay.Tumor volumes were measured by caliper every 2 days begin-ning on day 10 until the end of the study or when volumesreached a size greater than 1,500 mm3.
Immunohistochemical analyses of human melanomaspecimens
All specimens were acquired from patients followinginformed consent and according to a Massachusetts GeneralHospital institutional review board–approved clinical proto-col. Immunohistochemistry was performed on formalin-fixedparaffin-embedded sections following standard antigen retriev-al in citrate buffer. Granzyme B expression was detected witheither an anti-Granzyme B antibody (ab5049, Abcam) or abiotinylated and humanized version of GZP (Biotin-bAla-GGG-IEPD-CHO; hGZP). Bound antibody was detected witheither HRP-conjugated goat anti-rabbit antibody and reactedwith DAB substrate for IHC staining or AlexaFluor 488 goatanti-rabbit or AlexaFluor 594 goat anti-rabbit antibodies (LifeTechnologies) for immunofluorescent visualization. Boundpeptide was detected with either HRP-conjugated streptavidin(Abcam) followed by reaction with DAB substrate or Oregongreen conjugated neutravidin (Life Technologies). Patient sam-ples were grouped as either immunotherapy treated or non-treated, and treated specimens were further distinguished asresponders or nonresponders using modified RECIST criteria.Fluorescence quantification was performed using ImageJ soft-ware (National Institutes of Health, Bethesda, MD).
Statistical analysisStatistical analysis was performed using GraphPad Prism Ver-
sion 6 software. For all comparisons between treated and untreat-ed samples, an unpaired Student t test was utilized. A nonlinearregression was used for competitive binding analysis. One-wayANOVA was utilized to assess the specificity of the probe forvarious granzyme enzymes and to comparemean tumor to bloodratio of the monotherapy, combination therapy and vehicletreatment arms, and tumor volumes of the three groups of miceon days 12 and 18. Pearson correlation test was performed tocorrelate total tumoral granzyme B expression determined byWestern blot to tumoral TBR
ResultsWestern blot analysis of immune response in murine cancerimmunotherapy model
To evaluate candidate biomarkers of cancer immunotherapyresponse, we utilized CT26 syngeneic tumors in immunocom-petent Balb/c mice, a model characterized by its moderateresponse to anti–PD-1 and anti–CTLA-4 therapies (17). Micewere treated with anti–PD-1 and anti–CTLA-4 therapy or vehi-cle and tumors excised and evaluated by Western blot on days10, 12, or 14 after tumor inoculation. Neither CD8 nor CD3expression levels differed significantly between treated anduntreated mice at any time point analyzed (Fig. 1A–C; P ¼0.07–0.64, CD8; P ¼ 0.17–1, CD3). In contrast, there was amarked divergence between treated and untreated granzyme Bexpression levels. While granzyme B levels in treated anduntreated mice were equally low on day 10, they sharplyincreased in treated tumors across days 12 and 14, with sig-nificantly higher level of granzyme B in treated tumors (gran-zyme B:b-actin ¼ 20.4 � 4.1) in comparison with untreatedtumors (4.7 � 1.6; P ¼ 0.01) on day 14 (Fig. 1D). This was instark contrast with CD8, where the day 10 expression ratiobetween treated and untreated tumors was 0.52 � 0.3, with nosignificant change occurring over subsequent time points(Fig. 1E). Individual tumor granzyme B expression analysisamong treated tumors revealed separation into two distinctgroups: one group demonstrated low-level expression similarto untreated tumors, the other group had higher expressionthan both the low-level treated and vehicle-treated tumors(Fig. 1C). Furthermore, granzyme B expression among treatedtumors was independent of CD8 expression, as demonstratedby the dichotomous split among individual treated mice ana-lyzed for granzyme B versus CD8 expression (Fig. 1F).
As intratreatment biopsy is used occasionally in clinical trialsto assess change in protein expression, we questioned whetherfocused tumor sampling would be adequate to assess gran-zyme B expression. To visualize the spatial heterogeneity ofgranzyme B expression, a treated tumor was divided by a singlelongitudinal and two axial excisions into six equal mass por-tions. The portions were lysed and subjected to Western blot,which revealed significantly different levels of granzyme Bexpression, indicating a high level of heterogeneity (Supple-mentary Fig. S1). Taken together with the time course analysisof tumor infiltrate protein expression, it was hypothesized thatgranzyme B represented an attractive target for imaging agentdevelopment.
Immunofluorescent and immunohistochemical staining toassess granzyme B localization in tumors followingimmunotherapy
Prior to T-cell activation, granzyme B is contained withincytotoxic granules, and following activation it is secreted intothe immune synapse. A fraction of exocytosed granzyme Benters the target cell, with the remainder being released intothe extracellular space (20). Although Western blot confirmedthat granzyme B expression increased in treated tumors, itremained unclear if the increase in tumoral granzyme Breflected an increase within cytotoxic granules only, an increasein released granzyme B, or both. We sought a more detailedexamination of granzyme B spatial localization with immuno-fluorescence to better inform imaging agent development.
Larimer et al.
Cancer Res; 77(9) May 1, 2017 Cancer Research2320
on June 9, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Tumor samples from treated and untreated mice were analyzedby immunofluorescence for granzyme B and CD3 to assesswhether granzyme B was sequestered within T cells or secreted.Visualization revealed two distinct patterns of granzyme Baccumulation. In the first pattern, seen primarily withinuntreated tumors, a low intensity and small surface area gran-zyme B staining colocalized in regions of CD3 staining withinboth treated and untreated tumors, suggestive of basal gran-zyme B contained within granulocytes (Fig. 2A and B). A secondpattern of granzyme B staining, seen mostly in treated tumors,resulted in much larger and more intense areas of stainingthat often did not colocalize with CD3, suggestive of intensegranzyme B production and release into the extracellular space(Fig. 2C). We similarly demonstrated these distinct spatialpatterns with immunohistochemistry in an independent tu-mor set (Supplementary Fig. 2). The larger intense granzymeB–positive regions were present at a significantly higher fre-quency (P < 0.001) in treated tumors than in untreated tumors(Fig. 2D; Supplementary Fig. S3). These results strongly sug-gested that higher granzyme B expression in treated tumors wasdue to its release from activated cytotoxic T cells and a signif-icant fraction of the enzyme was extracellular, and thus acces-sible to binding by an imaging agent.
Synthesis and in vitro characterization of a novel granzyme BPET imaging probe
In order to assess the feasibility of imaging granzyme Bto predict immunotherapy response, we developed a granzymeB–specific imaging agent. The tetrapeptide Ile–Glu–Phe–Asphas been well characterized as the preferred murine granzymeB substrate, and previous evidence has shown that modi-fication of the C-terminus aspartate residue with an aldehydecreates an electrophilic trap, potently inhibiting granzyme Bwith a Ki of 80 nmol/L (21, 22). Previous structural analy-sis demonstrated the inhibitor forms a covalent bondbetween the aldehyde carbon and the enzyme active-site serineresidue. To generate a PET imaging construct, a small, flexiblelinker (Gly–Gly–Gly) was used to bridge the peptide and theradiometal chelator 2-[4,7-bis(carboxymethyl)-1,4,7-triazo-nan-1-yl]acetic acid (NOTA; Fig. 3A). An in vitro enzymeinhibition assay following conjugation confirmed retainedinhibitory potency with a Ki of 47 � 54 nmol/L (Fig. 3B).The peptide (NOTA-GZP) was labeled with 68Ga (68Ga-NOTA-GZP), a radiometal with a 68-minute half-life that matchesthe rapid pharmacokinetics of small peptides. The radio-labeling occurred with high yield (67% � 11%) and radio-chemical purity of >95% (peptide Rf ¼ 0.9–1.0, free gallium
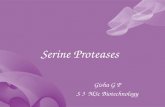
Figure 1.
Ex vivo immunoblot analysis of immunotherapy-treated tumors. Western blot analysis of combination therapy and vehicle-treated tumors on 10 (A), 12(B), and 14 (C) days post-inoculation. D, Quantification of protein expression on day 14 in treated (T) and untreated tumors (U). Bars represent themean of 4 replicates � SEM. E, Ratio of treated to untreated expression of granzyme B and CD8 over time. Each point represents the mean of 3 or 4 micewith error bars representing SEM. � , P < 0.05 by unpaired t test; significance is relative to expression. F, Ratio of granzyme B to CD8 for mice, eachsquare represents a ratio for an individual mouse, with the mean � SEM represented by bars.
Granzyme B PET Imaging Predicts Immunotherapy Response
www.aacrjournals.org Cancer Res; 77(9) May 1, 2017 2321
on June 9, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Rf ¼ 0.0–0.1) and resulted in an average calculated specificactivity of 5,190 � 1,100 MBq/mg. Together, these character-istics demonstrated a highly suitable radioligand for in vivoimaging. We then analyzed the radiolabeled peptide for selec-tivity relative to other granzyme family members and found itto have 5- to 11-fold specificity over all other enzymes assayed(Fig. 3C). As such, the 68Ga-NOTA-GZP peptide represented anovel, high-affinity, and specific peptide suitable for in vivoassessment.
68Ga-NOTA-GZP uptake correlates with granzyme B anddifferentiates therapeutic efficacy
After confirming in vitro affinity and specificity, the ability of68Ga-NOTA-GZP to image granzyme B in vivo was assessed inCT26 tumor–bearing mice treated with anti–PD-1 monotherapy,anti–PD-1 plus anti–CLTA-4 combination therapy regimen, orvehicle control. On day 14 after inoculation, mice were injectedwith �37 MBq of purified 68Ga-NOTA-GZP intravenously andimaged at 1 hour after injection. PET imaging revealed uptake in
Figure 2.
Immunohistochemical analysis ofgranzyme B localizationimmunofluorescent staining of CD3,granzyme B, and DAPI merged toshow spatial relationship anddifferential staining of granzyme B intreated (A) and untreated (B) tumors.Small panels represent the individualchannels, with the large panelrepresenting a composite overlayof allthree. C, Representative imagedemonstrating differential staining ofgranzyme B found in T cells versussecreted enzyme. D, Quantification ofgranzyme B fluorescence in treatedand untreated tumors (P < 0.0001).
Figure 3.
In vitro characterization of novelgranzyme B peptide, A, Chemicalstructure of NOTA-GZP. B, Arepresentative plot of enzyme activityat increasing concentrations of NOTA-GZP. Each point represents the meanof 6 replicates � SEM. A nonlinearregression was fit to the points usingGraphPad Prism.C,Enzyme specificityplot for radiolabeled 68Ga-NOTA-GZP.Bars represent the mean of 4replicates � SEM. ��� , P < 0.0001 byone-way ANOVA with a Bonferroniposttest, comparison to granzyme Bbinding.
Larimer et al.
Cancer Res; 77(9) May 1, 2017 Cancer Research2322
on June 9, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

tumors, kidneys and bladder, the latter of the two consistent withrenal clearance characteristic of small peptides (Fig. 4A–C; Sup-plementary Video S1–S2). Specific 68Ga-NOTA-GZP PET imaginguptake was calculated by dividing total tumor uptake by leftventricle uptake to derive a tumor to blood ratio (TBR) as ameasure of specifically retained signal. Comparison of TBR toWestern blot-quantified granzyme B expression demonstrated ahighly significant correlation (P < 0.0001) with an R2 ¼ 0.71,indicating that GZP PET imaging accurately reflects tumoralgranzyme B expression (Fig. 4D). PET imaging was also used tononinvasively assess granzyme B expression following differentimmunotherapy treatments. Anti–PD-1 treated tumors had anaverage TBR of 1.29 � 0.12 whereas the TBR of combination(anti–PD-1 þ anti–CTLA-4) treated mice was 1.83 � 0.18. Bothmonotherapy and combination therapy granzyme B expressionwere significantly elevated above untreated mice (TBR ¼ 0.96 �0.11). Following imaging, mice were sacrificed and ex vivo radio-activity assessed by gamma counter, which confirmed PET anal-ysis (Supplementary Fig. S4). The specificity of tumoral granzymeB was finally investigated using dynamic PET imaging to analyzethe effects of altered vasculature permeability on peptide reten-tion. Based on the irreversible mechanism of binding, a PATLAKgraphical plot was utilized and tumor influx calculated. Theresulting data were compatible with an irreversible two-compart-ment model, providing further evidence of granzyme B–specificpeptide accumulation (Supplementary Fig. S5).
Granzyme B PET imaging predicts response toimmunotherapy
Having determined that 68Ga-NOTA-GZP represented an accu-rate and noninvasive method to analyze granzyme B expression,the radiolabeled peptidewas next used to image treatedmice priorto tumor size divergence to determine the predictive value of the
peptide. CT26 tumor–bearing mice were treated with anti–PD-1and anti–CTLA-4 combination therapy andGZP PET imagingwasperformedon12 treated and8untreatedmice 12days post-tumorinoculation. This day represented the earliest possible time pointin which our previous studies observed significant differences ingranzyme B expression and was also before repression of tumorgrowth. While the vehicle treated mice had mostly low levels ofGZP PET uptake (mean TBR¼ 0.95� 0.20; range, 0.72–1.28), thetreated mice diverged into two distinct and nonoverlappinggroups of high GZP PET uptake (mean TBR¼ 1.90� 0.55, range,1.25–2.86) and low GZP PET uptake (mean TBR ¼ 0.89 � 0.19,range ¼ 0.57–1.08; Fig. 5). The high GZP-uptake group wassignificantly differentiated from both the low GZP uptake (P <0.05) and untreated control groups (P < 0.001). There was nosignificant difference in uptake between low-GZP uptake treatedtumors and untreated control. These results also stood in agree-ment with the patterns observed by ex vivoWestern blot analysis.
Although at the time of imaging there was no difference intumor volume between any of the three groups (Fig. 6B), alltreated tumors that regressed were identified as high GZP uptakeby PET imaging, while all tumors that significantly increased insize were characterized as having low GZP uptake (Fig. 6C). Assuch, our PET imaging quantification of GZP TBRwas completelypredictive of future tumoral response in the CT26 model. Repre-sentative PET images of each tumor are shown in SupplementaryFig. S6 to demonstrate the striking visual correlation betweentumor response and nonresponse between mice treated in anidentical manner.
Differential human granzyme B probe binding in humanmelanoma patient samples.
Having demonstrated the predictive ability of the murinegranzyme B–specific probe, we set out to develop an analogous
Figure 4.
Quantitative PET imaging of granzyme B following cancer immunotherapy PET images of anti–PD-1 and anti–CTLA-4 combination-treated (A), anti–PD-1—treated (B), and vehicle-treated (C) mice acquired 1 hour post-injection of 68Ga-NOTA-GZP. Top image represents a coronal maximal intensity projectionof whole body uptake, with tumors circled and labeled (T) and kidneys, which are the main route of peptide clearance, marked with a "K". Thebottom image shows an axial slice of the mouse with tumors circled and labeled with a "T" for clarity. D, Plot of TBR versus normalized granzyme Bexpression from mice undergoing PET imaging, followed by subsequent ex vivo protein quantification, r2 ¼ 0.71, P < 0.0001 by Pearson correlation. E,Mice treated with combination, monotherapy, or vehicle control were imaged and PET TBR acquired for each group. Bars represent the mean of N¼ 9–14 mice� SEM. � , P < 0.05; �� , P < 0.01.
Granzyme B PET Imaging Predicts Immunotherapy Response
www.aacrjournals.org Cancer Res; 77(9) May 1, 2017 2323
on June 9, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

human granzyme B–specific probe. The substrate specificity ofhuman granzyme B differs by one amino acid from the murineenzyme (23), with Ile–Glu–Pro–Asp the preferred substrate.We modified this tetrapeptide in a similar fashion as ourmurine imaging agent to create an irreversible inhibitor, andthen biotinylated the N-terminus for purpose of tissue staining(hGZP). We then analyzed a cohort of 9 human melanomabiopsy samples obtained from patients treated with anti–PD-1checkpoint inhibitors (n ¼ 6 nivolumab and n ¼ 3 pembro-lizumab), that were retrospectively correlated with responsebased on modified RECIST criteria. Using an antihuman gran-zyme B antibody, on-treatment biopsy samples demonstrateddistinct differences in the amount and intensity of granzyme Bstaining between treated responders and nonresponders byIHC (Fig. 7A). To quantify the degree and magnitude ofdifference between treated responders and nonresponders,quantitative fluorescent microscopy was performed. Fluores-cent microscopy analysis shows treated-responder specimengranzyme B expression up to �1,000� greater than treatednonresponders and suggests continual increase in treatedgranzyme B expression over time (Fig. 7B). Finally, treatedresponder samples were analyzed by both immunohistochem-istry and immunofluorescence to compare the ability of hGZP
to specifically detect granzyme B in human tissue and compareit to anti–granzyme B antibody. A strong correlation wasobserved by both techniques, indicating highly specific bind-ing of hGZP to human granzyme B (Fig. 7C and D). Theseresults suggest that there are significant differences in tumoralgranzyme B expression between human responders and non-responders and that these differences are recognized by ourhuman granzyme B–specific probe. The magnitude of differ-ence between responders and nonresponders suggests thatfuture clinical imaging studies will be able to readily distin-guish between these two groups.
DiscussionIn this report, we demonstrate that granzyme B represents an
attractive biomarker for early response prediction to cancerimmunotherapy and have developed a novel, translatable gran-zyme B–targeted peptide to allow for repeated, quantitative, andnoninvasive PET imaging assessment. Beginning in a murineimmunotherapy model, we establish that tumoral uptake of68Ga-NOTA-GZP is highly correlated with tumoral granzyme Bexpression across a number of therapeutic strategies. In tumorstreatedwith combined PD-1 andCTLA-4 inhibitors, we show that
Figure 5.
Granzyme B PET imagingdifferentiates treated responders andnonresponders. Mice treated withcombination anti–PD-1 and anti–CTLA-4 therapy or vehicle wereimaged 12 days post-inoculation. A,Representative sagittal images oftreated responders, treatednonresponders, and vehicle-treatedmice. T, tumors. B, Scatter plot ofindividual mice by groups; mean ofeach group are shown by bars � SEM.��� P < 0.001
Figure 6.
Tumor growth of high and lowgranzyme B expression. A, Tumorgrowth curves of treated responder(green circles), treated nonresponders(red squares), and vehicle-treated(black triangles) mice; same groupsas Fig. 5. Eachmeasurement representsthe mean of two individual calipermeasurements. B, Tumor volumes ofeach group of mice on the day ofimaging; no significant difference wasfound between groups. C, Tumorvolumes of mice at end of study,grouped by PET TBR. � , P < 0.05; ��� , P< 0.001
Larimer et al.
Cancer Res; 77(9) May 1, 2017 Cancer Research2324
on June 9, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

68Ga-NOTA-GZP PET imaging prior to tumor volume divergencesegments tumors into high- and low-signal groups. Further mon-itoring of changes in tumor volume revealed that all high-uptaketumors subsequently regressed, and all low-uptake tumors pro-gressed on therapy, with the low-uptake group PET quantificationindistinguishable from vehicle-treated controls. We extended ourfindings by analyzing human melanoma biopsy specimensobtained from patients on checkpoint inhibitor therapy. Usinga human specific version of our granzyme B imaging probe, wedemonstrate marked increased granzyme B expression in treatedresponders in comparison to treated nonresponders. These resultssuggest granzyme B PET imaging may serve as a noninvasiveimaging biomarker for predicting response in immuno-oncology.
Immunotherapy represents a significant advance in cancertreatment, withmany patients experiencing durable tumor remis-sion (2, 7, 24). However, oncologists must balance the benefitsthat are eventually seen in only a minority of patients with a highincidence of severe immune-related adverse events in the treatedpopulation. Moreover, they must weigh the potential increasedtumoricidal benefits of combination immunotherapy with thegreater rate of severe side effects when utilizing these regimens(2, 25). Unfortunately, standard clinical imaging modalities (CT,MRI, 18F-FDG-PET) typically utilized to monitor therapeuticefficacy are of limited value in the setting of immunotherapy,due in part to the tumoral inflammatory infiltrate that can beinduced by treatment (26). This infiltrate is indistinguishablefrom tumor progression, confounding standard imaging diag-
nostics (27, 28). As such, an alternative biomarker formonitoringimmune response is needed. Potential PET imaging biomarkerssuch as CD8 or PD-L1 may provide benefit in certain cases;however, a more global marker of T-cell activation was soughtin order to accurately determine T-cell activity rather than cellpresence.
Granzyme B, a serine protease released primarily by cyto-toxic T cells as a primary tumor killing mechanism, may serveas such a biomarker. Our work and others' have demonstratedit to be differentially expressed among treated respondersand nonresponders (29). Unlike other biomarkers under inves-tigation, expression of tumoral granzyme B represents anincorporation of cytotoxic T cell tumor localization as well astumoricidal activity. Its expression serves as a general responsebiomarker by integrating the activity of multiple convergingpathways of immune-mediated tumor cell killing enhancementor suppression. Moreover, granzyme B–specific imaging pro-vides for an integrated picture of granzyme B expression withina given lesion and allows for simultaneous interrogation ofall tumor sites. This global view stands in contrast to the smallgeographic and temporal perspective of a biopsy specimen,which provides a wealth of data but represents less than 0.1%of the total tumor volume. The inherent marked spatial het-erogeneity of tumors and tumoral immune cell infiltrates,as demonstrated in our and others' data (30, 31), underscoresthe risk of inaccurate assessment when relying on biopsiesrather than complete tumor sampling. Additionally, the rapid
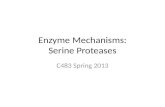
Figure 7.
Human melanoma granzyme B analysis and peptide binding. A, Human melanoma samples from patients treated with an anti–PD-1 checkpoint inhibitorwere grouped as treated responders (TR) or treated nonresponders (TNR) based on modified RECIST criteria. B, Immunofluorescent microscopyquantification of granzyme B in 9 patients at incremental time intervals reveals significant differences in granzyme B expression as early as 16 dayspost-therapy between responding and nonresponding patients. C, Comparison of matched samples using either an anti–granzyme B antibody (Anti-GrB) orhumanized GZP peptide (clinical GZP) reveals similar patterns of staining between the antibody and peptide that are much stronger in treated patientsthan untreated patients. D, Colocalization (yellow) of human GZP (green) and anti-GrB (red) is demonstrated in a treated responder melanoma patient,with nuclear staining (DAPI) in blue.
Granzyme B PET Imaging Predicts Immunotherapy Response
www.aacrjournals.org Cancer Res; 77(9) May 1, 2017 2325
on June 9, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

pharmacokinetics of the peptide-based imaging agent allowsfor repeat, noninvasive quantitation of granzyme B activity,facilitating integration into clinical trials and overcomingthe need for repeat biopsy with the attendant patient risks(32–34). This current lack of global and temporal assessmenthas been one of the limitations to clinical development ofcancer immunotherapies and combination treatments. Gran-zyme B PET imaging may reduce these limitations by providingearly and quantitative verification of successful therapeuticdevelopment.
We anticipate that granzyme B imaging will significantlybenefit several aspects of the evolving cancer immunotherapylandscape. It may be used to distinguish treated respondersfrom treated nonresponders on an individual patient basis attime points much earlier than previously possible, allowing fortriage of nonresponders onto alternative therapeutic regimensearly in the course of treatment. Nonresponders could avoid theoften-severe side effects of an ineffective therapy and wouldhave an opportunity to try other, potentially more effectiveregimens, immunotherapy-based or otherwise. With the abilityto rapidly distinguish effective from ineffective therapy, 68Ga-NOTA-GZP imaging may conversely allow patients to begin onless strenuous single-agent regimens and only move to com-bination regimens if imaging indicates a lack of granzyme Bsecretion. The quantitative signal derived from PET imagingmay also be broadly useful in clinical trial development. As weobserved in this study, combination therapy is associated withhigher mean 68Ga-NOTA-GZP uptake than anti–PD-1 mono-therapy. Further investigation of dose dependency and alter-native combination therapy is required to definitively confirmthis application, but comparison of immunotherapy regimensbased on their 68Ga-NOTA-GZP quantification may allow forrapid comparison of alternative clinical trial regimens in a morenuanced and less time-intensive fashion than tracking overallsurvival.
Our work presented in this report suggests that granzyme B PETmay serve as a much-needed quantitative predictive imagingbiomarker. Multiple 68Ga-labelled peptides are currently in useclinically, and the pharmacokinetic profile of peptides is wellsuited for clinical translation. Given the potential benefits ofincorporation of granzyme B PET imaging into immunotherapy
diagnostics, near term human clinical trials are planned. Initialclinical trials focused inmelanoma patients will allow for humanpharmacokinetic analysis and granzyme B quantification andcorrelation with overall response and progression-free survival.They will also provide the framework for future trials that willpermit a more comprehensive quantitative examination of thepredictive capabilities at both an individual patient level and fornovel therapeutic assessment.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: B.M. Larimer, E. Wehrenberg-Klee, F. Dubois,K. Flaherty, U. MahmoodDevelopment of methodology: B.M. Larimer, E. Wehrenberg-Klee, F. Dubois,G. Boland, U. MahmoodAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): B.M. Larimer, E. Wehrenberg-Klee, F. Dubois,T. Kalomeris, G. BolandAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): B.M. Larimer, E. Wehrenberg-Klee, F. Dubois,A. Mehta, T. Kalomeris, K. Flaherty, U. MahmoodWriting, review, and/or revision of the manuscript: B.M. Larimer, E. Wehren-berg-Klee, F. Dubois, T. Kalomeris, K. Flaherty, U. MahmoodAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): B.M. Larimer, E. Wehrenberg-Klee, F. Dubois,T. KalomerisStudy supervision: B.M. Larimer, U. Mahmood
AcknowledgmentsThe authors would like to thank Hans Vitzhum and Emily Bloch for their
assistance with data collection and manuscript preparation.
Grant SupportThis study was supported by NIHP50-CA127003 and R01-CA166582.The costs of publication of this article were defrayed in part by the
payment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received December 8, 2016; revised December 8, 2016; accepted March 9,2017; published online May 1, 2017.
References1. Royal RE, Levy C, Turner K, Mathur A, Hughes M, Kammula US, et al.
Phase 2 trial of single agent Ipilimumab (anti-CTLA-4) for locallyadvanced or metastatic pancreatic adenocarcinoma. J Immunother2010;33:828–33.
2. PostowMA, Chesney J, Pavlick AC, Robert C, Grossmann K,McDermott D,et al. Nivolumab and ipilimumab versus ipilimumab in untreated mela-noma. N Engl J Med 2015;372:2006–17.
3. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Cowey CL, Lao CD, et al.Combined nivolumab and ipilimumab or monotherapy in untreatedmelanoma. N Engl J Med 2015;373:23–34.
4. Marrone KA, Ying W, Naidoo J. Immune-related adverse events fromimmune checkpoint inhibitors. Clin Pharmacol Therapeut 2016:n/a-n/a.
5. Wolchok JD, Hoos A, O'Day S, Weber JS, Hamid O, Lebb�e C, et al.Guidelines for the evaluation of immune therapy activity in solidtumors: immune-related response criteria. Clin Cancer Res 2009;15:7412–20.
6. Sachpekidis C, Larribere L, Pan L, Haberkorn U, Dimitrakopoulou-StraussA, Hassel JC. Predictive value of early 18F-FDG PET/CT studies for treat-ment response evaluation to ipilimumab in metastatic melanoma: pre-
liminary results of an ongoing study. Eur J Nucl Med Mol Imaging2015;42:386–96.
7. Borghaei H, Paz-Ares L, Horn L, Spigel DR, Steins M, Ready NE, et al.Nivolumab versus docetaxel in advanced nonsquamous non-small-celllung cancer. N Engl J Med 2015;373:1627–39.
8. Herbst RS, Baas P, Kim D-W, Felip E, P�erez-Gracia JL, Han J-Y, et al.Pembrolizumab versus docetaxel for previously treated, PD-L1-positive,advanced non-small-cell lung cancer (KEYNOTE-010): a randomised con-trolled trial. Lancet 2016;387:1540–50.
9. Tavar�e R, Escuin-OrdinasH,Mok S,McCrackenMN, Zettlitz KA, Salazar FB,et al. An effective immuno-PET imaging method to monitor CD8-depen-dent responses to immunotherapy. Cancer Res 2016;76:73–82.
10. Larimer BM, Wehrenberg-Klee E, Caraballo A, Mahmood U. QuantitativeCD3 PET imaging predicts tumor growth response to anti-CTLA-4 therapy.J Nucl Med 2016.
11. Maute RL, Gordon SR, Mayer AT, McCracken MN, Natarajan A, Ring NG,et al. Engineering high-affinity PD-1 variants for optimized immunother-apy and immuno-PET imaging. Proc Natl Acad Sci 2015;112:E6506–E14.
12. Schwartz RH.T cell anergy. Annu Rev Immunol 2003;21:305–34.
Larimer et al.
Cancer Res; 77(9) May 1, 2017 Cancer Research2326
on June 9, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

13. Roychoudhuri R, Eil RL, RestifoNP. The interplay of effector and regulatoryT cells in cancer. Curr Opin Immunol 2015;33:101–11.
14. Podack ER.Execution and suicide: cytotoxic lymphocytes enforce Draco-nian laws through separate molecular pathways. Curr Opin Immunol1995;7:11–6.
15. Nagata S.Apoptosis by death factor. Cell 1997;88:355–65.16. Thornberry NA, Rano TA, Peterson EP, Rasper DM, Timkey T, Garcia-
Calvo M, et al. A combinatorial approach defines specificities of mem-bers of the caspase family and granzyme B. Functional relationshipsestablished for key mediators of apoptosis. J Biol Chem 1997;272:17907–11.
17. Duraiswamy J, Kaluza KM, Freeman GJ, Coukos G. Dual blockade of PD-1and CTLA-4 combined with tumor vaccine effectively restores T-cell rejec-tion function in tumors. Cancer Res 2013;73:3591–603.
18. Stewart JM, Young JD. Solid phase peptide synthesis. Pierce ChemicalCompany; 1984.
19. Heidari P, Wehrenberg-Klee E, Habibollahi P, Yokell D, Kulke M, Mah-mood U. Free somatostatin receptor fraction predicts the antiproliferativeeffect of octreotide in a neuroendocrine tumor model: implications fordose optimization. Cancer Res 2013;73:6865–73.
20. Voskoboinik I, Whisstock JC, Trapani JA. Perforin and granzymes:function, dysfunction and human pathology. Nat Rev Immunol 2015;15:388–400.
21. Willoughby CA, Bull HG, Garcia-Calvo M, Jiang J, Chapman KT,Thornberry NA. Discovery of potent, selective human granzyme Binhibitors that inhibit CTL mediated apoptosis. Bioorg Med Chem Lett2002;12:2197–200.
22. Rotonda J, Garcia-Calvo M, Bull HG, Geissler WM, McKeever BM, Wil-loughby CA, et al. The three-dimensional structure of human granzyme Bcompared to caspase-3, keymediators of cell deathwith cleavage specificityfor aspartic acid in P1. Chem Biol 2001;8:357–68.
23. Casciola-Rosen L, Garcia-Calvo M, Bull HG, Becker JW, Hines T, Thorn-berry NA, et al. Mouse and human granzyme B have distinct tetrapeptidespecificities and abilities to recruit the bid pathway. J Biol Chem 2007;282:4545–52.
24. Motzer RJ, Escudier B, McDermott DF, George S, Hammers HJ, Srinivas S,et al. Nivolumab versus everolimus in advanced renal-cell carcinoma.N Engl J Med 2015;373:1803–13.
25. Naidoo J, Page DB, Li BT, Connell LC, Schindler K, Lacouture ME, et al.Toxicities of the anti-PD-1 and anti-PD-L1 immune checkpoint antibodies.Ann Oncol 2015;26:2375–91.
26. Kubota R, Yamada S, Kubota K, Ishiwata K, Tamahashi N, Ido T. Intratu-moral distribution of fluorine-18-fluorodeoxyglucose in vivo: high accu-mulation in macrophages and granulation tissues studied by microautor-adiography. J Nucl Med 1992;33:1972–80.
27. Wolchok JD, Hoos A, O'Day S, Weber JS, Hamid O, Lebbe C, et al.Guidelines for the evaluation of immune therapy activity in solid tumors:immune-related response criteria. Clin Cancer Res 2009;15:7412–20.
28. Okada H, Weller M, Huang R, Finocchiaro G, Gilbert MR, Wick W, et al.Immunotherapy response assessment in neuro-oncology: a report of theRANO working group. Lancet Oncol 2015;16:e534–42.
29. Tumeh PC, Harview CL, Yearley JH, Shintaku IP, Taylor EJ, Robert L, et al.PD-1 blockade induces responses by inhibiting adaptive immune resis-tance. Nature 2014;515:568–71.
30. Galon J, Costes A, Sanchez-Cabo F, Kirilovsky A, Mlecnik B, Lagorce-Pages C, et al. Type, density, and location of immune cells withinhuman colorectal tumors predict clinical outcome. Science 2006;313:1960–4.
31. Nawaz S,HeindlA, KoelbleK, YuanY. Beyond immunedensity: critical roleof spatial heterogeneity in estrogen receptor-negative breast cancer. ModPathol 2015;28:1621.
32. Manno C, Strippoli GF, Arnesano L, Bonifati C, Campobasso N, GesualdoL, et al. Predictors of bleeding complications in percutaneous ultrasound-guided renal biopsy. Kidney Int 2004;66:1570–7.
33. Myers RP, Fong A, Shaheen AA. Utilization rates, complications and costsof percutaneous liver biopsy: a population-based study including 4275biopsies. Liver Int 2008;28:705–12.
34. Heck SL, Blom P, Berstad A. Accuracy and complications in computedtomography fluoroscopy-guided needle biopsies of lung masses. EurRadiol 2006;16:1387–92.
www.aacrjournals.org Cancer Res; 77(9) May 1, 2017 2327
Granzyme B PET Imaging Predicts Immunotherapy Response
on June 9, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

2017;77:2318-2327. Cancer Res Benjamin M. Larimer, Eric Wehrenberg-Klee, Frank Dubois, et al. Immunotherapy ResponseGranzyme B PET Imaging as a Predictive Biomarker of
Updated version
http://cancerres.aacrjournals.org/content/77/9/2318
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2017/07/22/77.9.2318.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerres.aacrjournals.org/content/77/9/2318.full#ref-list-1
This article cites 31 articles, 10 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/77/9/2318.full#related-urls
This article has been cited by 13 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/77/9/2318To request permission to re-use all or part of this article, use this link
on June 9, 2020. © 2017 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from