

Granulomatosis with polyangiitis
72
Granulomatosis with polyangiitis Yoavanit Srivaro M.D.
-
Upload
chulalongkorn-allergy-and-clinical-immunology-research-group -
Category
Health & Medicine
-
view
108 -
download
3
Transcript of Granulomatosis with polyangiitis

Granulomatosis with polyangiitis
Yoavanit Srivaro M.D.

Outline
• Historical Perspective• Epidemiology• Pathogenesis• Clinical manifestation• Different GPA phenotypes• Differential Diagnosis• Diagnosis• Treatment

Historical Perspective
1931 : Klinger described The first case of GPA was by Klinger as a variant of polyarteritis nodosa.
1936 : Wegener recognized the syndrome as a separate clinical entity.
2011 :An international panel of experts in vasculitis recommended changing the name of the syndrome to granulomatosis with polyangiitis (GPA)
Sneller MC. et al.Middleton's Allergy ; 8th edition. 2014. p. 1014-31

Historical Perspective
Friedrich Wegener (April 7, 1907 – July 9,1990)
German pathologist
Available at: http://en.wikipedia.org/w/index.php?title=Friedrich_Wegener&oldid=659562046. Accessed April 30, 2015.

Epidemiology
• Mean age at onset at 40 years• M:F = 1:1• Caucasians are overrepresented
Hoffman GS, Kerr GS, Leavitt RY, et al. Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med 1992;116: 488-94.
Reinhold-Keller E, Beuge N, Latza U, et al. An interdisciplinary approach to the care

Epidemiology
• Incidence varies 4 per million in Olmsted County, United States. 15 per million in northern Norway.
Gonzalez-Gay MA, Garcia-Porrua C. Epidemiology of the vasculitides. Rheum Dis Clin North Am 2001;27:729-49.
Koldingsnes W, Nossent H. Epidemiology of Wegener’s granulomatosis in northern Norway. Arthritis Rheum 2000;43:2481-7.

Gradual twofold to fourfold increase in the incidence of GPA over the past 2 decades.
Gibelin A, Maldini C, Mahr A. Epidemiology and etiology of Wegener granulomatosis, microscopic polyangiitis, Churg-Strauss syndrome and Goodpasture syndrome: vasculitides with frequent lung involvement. Semin Respir Crit Care Med
2011;32:264-73.


Pathogenesis
G
Genetics
Aberrant Cell mediated
immune response ANCA
Sneller MC. et al.Middleton's Allergy ; 8th edition. 2014. p. 1014-31

Genetics
•GWAS of 1683 cases of GPA & 489 of MPA •Cases of vasculitis with anti-PR3 ANCA were associated with 1. HLA-DP gene 2. SERPINA1 (gene encoding forα1 antitrypsin) gene 3. PRTN3 (gene encoding for proteinase 3) gene
Lyons PA, Rayner TF, Trivedi S, Holle JU, Watts RA, Jayne DRW, et al. Genetically distinct subsets within ANCA-associated vasculitis. N Engl J Med 2012;367:214–23.

Aberrant Cell mediated immune response
Immunoregulatory defect response to environmental insults (e.g. infection) or autoantigens.
Excessive production of Th1/Th17 cytokines (IL-17, TNF & IFN-γ)
Granulomatous inflammatory vascular lesion
Sneller MC. et al.Middleton's Allergy ; 8th edition. 2014. p. 1014-31

ANCA
Kallenberg CG, Heeringa P, Stegeman CA. Mechanisms of Disease: pathogenesis and treatment of ANCA-associated vasculitides. Nat Clin Pract Rheumatol 2006; 2 : 661– 70.

ANCA
Kallenberg CG, Heeringa P, Stegeman CA. Mechanisms of Disease: pathogenesis and treatment of ANCA-associated vasculitides. Nat Clin Pract Rheumatol 2006; 2 : 661– 70.

ANCA
Kallenberg CG, Heeringa P, Stegeman CA. Mechanisms of Disease: pathogenesis and treatment of ANCA-associated vasculitides. Nat Clin Pract Rheumatol 2006; 2 : 661– 70.

ANCA
Kallenberg CG, Heeringa P, Stegeman CA. Mechanisms of Disease: pathogenesis and treatment of ANCA-associated vasculitides. Nat Clin Pract Rheumatol 2006; 2 : 661– 70.

ANCA
Kallenberg CG, Heeringa P, Stegeman CA. Mechanisms of Disease: pathogenesis and treatment of ANCA-associated vasculitides. Nat Clin Pract Rheumatol 2006; 2 : 661– 70.

Organ Frequency at onset (%)
Total frequency(%)
Upper respiratory tract
73-93 92-99Lower respiratory tract
48-55 66-85Musculoskeletal system
18-54 70-75Kidney 32-61 67-77Eye 15-40 52-61Skin 13-23 30-46Nervous system 1-21 20-40
Hoffman GS, Kerr GS, Leavitt RY, Hallahan CW, Lebovics RS, Travis WD, et al. Wegener granulomatosis: an analysis of 158 patients. Annals of internal medicine. 1992;116(6):488-98.
Clinical manifestation

Clinical manifestation

Constitutional signs
• Fever, asthenia,weight loss are frequent (50%)• Non-specific
Comarmond C, Cacoub P. Granulomatosis with polyangiitis (Wegener): clinical aspects and treatment. Autoimmunity reviews. 2014;13(11):1121-5.

Ear Nose and Throat involvement
• Crusting rhinorrhea• Sinusitis• Chronic otitis media• Damage of the facial cartilage with deformities
causing saddle nose• Perforation of the nasal septum, the palate or the
pinna of the ear.
Trimarchi M, Sinico RA, Teggi R, Bussi M, Specks U, Meroni PL. Otorhinolaryngological manifestations in granulomatosis with polyangiitis (Wegener's). Autoimmunity reviews. 2013;12(4):501-5.

Ear Nose and Throat involvement
• Crusting rhinorrhea• Sinusitis• Chronic otitis media• Damage of the facial cartilage with deformities
causing saddle nose• Perforation of the nasal septum, the palate or the
pinna of the ear.
Present in 70 to 100% of cases at diagnosis.
Trimarchi M, Sinico RA, Teggi R, Bussi M, Specks U, Meroni PL. Otorhinolaryngological manifestations in granulomatosis with polyangiitis (Wegener's). Autoimmunity reviews. 2013;12(4):501-5.

Ear Nose and Throat involvement
• Crusting rhinorrhea• Sinusitis• Chronic otitis media• Damage of the facial cartilage with deformities
causing saddle nose• Perforation of the nasal septum, the palate or the
pinna of the ear.
• Nasal-sinus involvement is the hallmark of the disease• Nasal obstruction with hyposmia or anosmia is often the first symptom.
Present in 70 to 100% of cases at diagnosis.
Trimarchi M, Sinico RA, Teggi R, Bussi M, Specks U, Meroni PL. Otorhinolaryngological manifestations in granulomatosis with polyangiitis (Wegener's). Autoimmunity reviews. 2013;12(4):501-5.

Fig 1. Endoscopic features in GPA patients: a) left nasal cavity with an ulcer (u) on the nasal septum (NS) and the middle turbinate (MT). b) Left nasal cavity with septal perforationand diffuse crusting with ulcers (CU). c) Right nasal cavity showing diffuse crusting with infection. d) Right nasal cavity with crusting in a patient with remission.
Trimarchi M, Sinico RA, Teggi R, Bussi M, Specks U, Meroni PL. Otorhinolaryngological manifestations in granulomatosis with polyangiitis (Wegener's). Autoimmunity reviews. 2013;12(4):501-5.

Comarmond C, Cacoub P. Granulomatosis with polyangiitis (Wegener): clinical aspects and treatment. Autoimmunity reviews. 2014;13(11):1121-5.
Saddle-nose appearance

Clinical manifestation

Lung involvement
• Alveolar hemorrhage • Parenchymatous nodules• Tracheal and subglottic stenosis sometimes associated with endobronchial locations
Comarmond C, Cacoub P. Granulomatosis with polyangiitis (Wegener): clinical aspects and treatment. Autoimmunity reviews. 2014;13(11):1121-5.

Lung involvement
• Alveolar hemorrhage • Parenchymatous nodules• Tracheal and subglottic stenosis sometimes associated with endobronchial locations
Present in 50 to 90% of cases
Comarmond C, Cacoub P. Granulomatosis with polyangiitis (Wegener): clinical aspects and treatment. Autoimmunity reviews. 2014;13(11):1121-5.

Sneller MC. et al.Middleton's Allergy ; 8th edition. 2014. p. 1014-131
Figure 62-1 A, Chest computed tomographic scan of a patient with GPA shows typical nodular lung infiltrate with cavitation.


Sneller MC. et al.Middleton's Allergy ; 8th edition. 2014. p. 1014-131
Subglottic stenosis

Clinical manifestation

Renal involvement
• Focal segmental necrotizing glomerulonephritis associated with extracapillary proliferation with pauci-immune crescent formation
• Urogenital manifestations
Comarmond C, Cacoub P. Granulomatosis with polyangiitis (Wegener): clinical aspects and treatment. Autoimmunity reviews. 2014;13(11):1121-5.

Clinical manifestation

Nervous system involvement
• PNS Mononeuritis multiplex Sensorimotor neuropathy.• CNS Pachymeningitis ( Granulomatous deposits, intracerebral vascular
lesions, or an extension of sinus lesions )
Seror R, Mahr A, Ramanoelina J, Pagnoux C, Cohen P,Guillevin L. Central nervous system involvement in Wegener granulomatosis. Medicine (Baltimore) 2006;85:54–65.

Skin involvement
• Vascular purpura to the lower limbs• Subcutaneous nodules• Pyoderma gangrenosum• Raspberry-red gingivitis• Intraoral and/or genital ulcerations.
Comarmond C, Cacoub P. Granulomatosis with polyangiitis (Wegener): clinical aspects and treatment. Autoimmunity reviews. 2014;13(11):1121-5.

Comarmond C, Cacoub P. Granulomatosis with polyangiitis (Wegener): clinical aspects and treatment. Autoimmunity reviews. 2014;13(11):1121-5.
Necrotic vascular purpura

Different GPA phenotypes
Comarmond C, Cacoub P. Granulomatosis with polyangiitis (Wegener): clinical aspects and treatment. Autoimmunity reviews. 2014;13(11):1121-5.

Differential Diagnosis
• Microscopic Polyangiitis • Churg-Strauss Syndrome • Goodpasture Disease
Sneller MC. et al.Middleton's Allergy ; 8th edition. 2014. p. 1014-131

Sneller MC. et al.Middleton's Allergy ; 8th edition. 2014. p. 1014-131

Sneller MC. et al.Middleton's Allergy ; 8th edition. 2014. p. 1014-131

Sneller MC. et al.Middleton's Allergy ; 8th edition. 2014. p. 1014-131

Criteria of the American College of Rheumatology(ACR 1990)
Criterior Definition1.Nasal or oral inflammation 1.Development of painful or painless oral ulcers; or purulent or bloody nasal discharge2.Abnormal chest radiograph 2.Presence of nodules fixed infiltrates or cavities3.Urinary sediment 3.Microhematuria ( > 5 RBCs per high power field) or red cell casts4.Granulomatous inflammation 4.Granulomatous inflammation on biopsy within the wall of an artery or in the perivascular orextravascular area (artery or arteriole)
• GPA is defined by the presence of at least 2 of the 4 criteria• Sensitivity 88.2% • Specificity 92.0 %
Leavitt RY, Fauci AS, Bloch DA,Michel BA, Hunder GG, ArendWP, et al. The American College of Rheumatology 1990 criteria for the classification of Wegener's granulomatosis. Arthritis Rheum 1990;33:1101–7

2012 revised Chapel Hill criteria
• GPA is defined as Necrotizing granulomatous inflammation of the
upper and lower respiratory tracts. with
Necrotizing vasculitis of small- and medium size vessels, i.e. the capillaries, veins, arterioles and
arteries.
Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum 2013;65:1–11.

Diagnosis
• Necrotizing granulomatous inflammation with vasculitis on tissue biopsy
Devaney KO, Travis WD, Hoffman G, et al. Interpretation of head and neck biopsies in Wegener’s granulomatosis: a pathologic study of 126 biopsies in 70 patients. Am J Surg Pathol 1990;14:555-64. Langford
CA. The diagnostic utility of c-ANCA in Wegener’s granulomatosis. Cleve Clin J Med 1998;65:135-40.
Diagnosis
• Necrotizing granulomatous inflammation with vasculitis on tissue biopsy
• Kidney biopsy :glomerulonephritis
Devaney KO, Travis WD, Hoffman G, et al. Interpretation of head and neck biopsies in Wegener’s granulomatosis: a pathologic study of 126 biopsies in 70 patients. Am J Surg Pathol 1990;14:555-64. Langford
CA. The diagnostic utility of c-ANCA in Wegener’s granulomatosis. Cleve Clin J Med 1998;65:135-40.

Diagnosis
• Necrotizing granulomatous inflammation with vasculitis on tissue biopsy
• Kidney biopsy :glomerulonephritis• Positive antiproteinase-3 ANCA :very high specificity
Devaney KO, Travis WD, Hoffman G, et al. Interpretation of head and neck biopsies in Wegener’s granulomatosis: a pathologic study of 126 biopsies in 70 patients. Am J Surg Pathol 1990;14:555-64. Langford
CA. The diagnostic utility of c-ANCA in Wegener’s granulomatosis. Cleve Clin J Med 1998;65:135-40.

Granulomatous vasculitis involving a small pulmonary artery in the lung of a patient with GPA. The vessel wall is markedly thickened with an inflammatory infiltrate that includes multinucleated giant cells.
Sneller MC. et al.Middleton's Allergy ; 8th edition. 2014. p. 1014-131

Multinucleated Giant Cell


Glomeruli showing segmental necrosis with early crescent formation (arrows). Sneller MC. et al.Middleton's Allergy ; 8th
edition. 2014. p. 1014-131

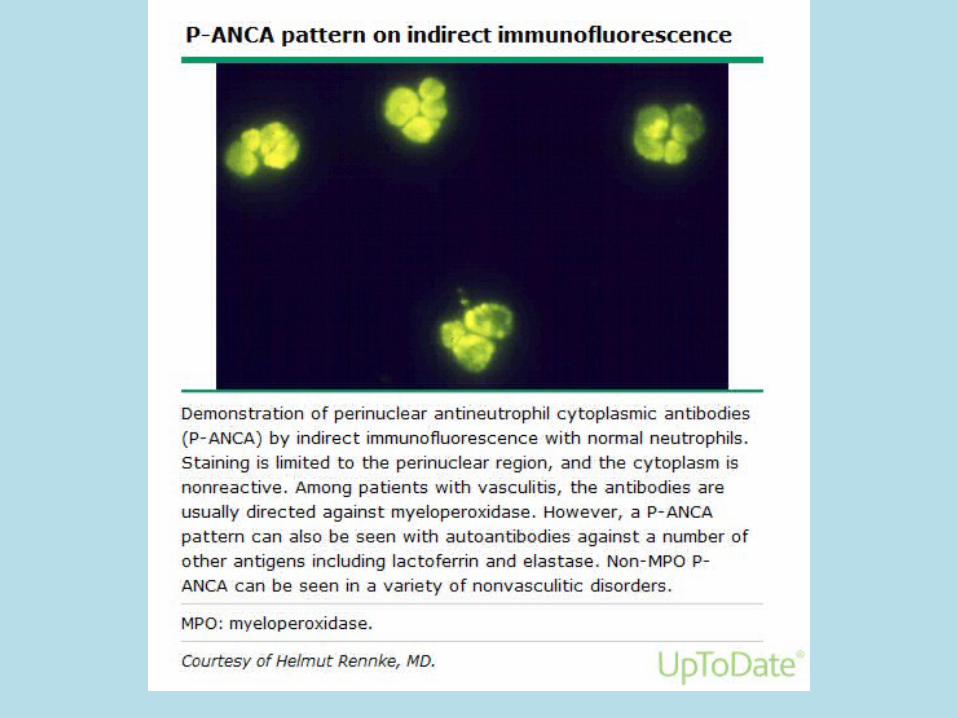

ANCA
Kallenberg CG. Pathogenesis of ANCA-associated vasculitides. Annals of the rheumatic diseases. 2011;70 Suppl 1:i59-63.

Treatment
• Intensive immunosuppressive regimens • Plasma exchange • Anti-TNF agents • Rituximab:A chimeric monoclonal antibody against
CD20
Sneller MC. et al.Middleton's Allergy ; 8th edition. 2014. p. 1014-31

Intensive immunosuppressive regimens
de Groot K, Harper L, Jayne DR, et al. Pulse versus daily oral cyclophosphamide for induction of remission in antineutrophil cytoplasmic antibody-associated vasculitis: a randomized trial. Ann Intern Med 2009;150:670-
80.
High-dose glucocorticoids Prednisone:1 mg/kg/day initially (for the first month of
therapy) as a daily regimen and
Cyclophosphamide given a daily oral dose (2 mg/kg/day) or
monthly intravenous pulses (15 mg/kg)
Gradual conversion to an alternate-day schedule followed by tapering & discontinuation after 6 to
8 months

Intensive immunosuppressive regimens
de Groot K, Harper L, Jayne DR, et al. Pulse versus daily oral cyclophosphamide for induction of remission in antineutrophil cytoplasmic antibody-associated vasculitis: a randomized trial. Ann Intern Med 2009;150:670-
80.
After remission, cyclophosphamide is discontinued
Maintenance therapy with
Methotrexate or AzathioprineAt least 1 year
Complete disease remission within 3-6 months

Plasma exchange
• Adjuvant treatment for severe manifestations• Removing potentially pathogenic ANCA• Severe renal vasculitis• Severe diffuse alveolar hemorrhage
Walsh M, Catapano F, Szpirt W, et al. Plasma exchange for renal vasculitis and idiopathic rapidly progressive glomerulonephritis: a meta-analysis. Am J Kidney Dis 2011;57: 566-74.
Klemmer PJ, Chalermskulrat W, Reif MS, et al. Plasmapheresis therapy for diffuse alveolar hemorrhage in patients with small-vessel vasculitis. Am J Kidney Dis 2003;42:1149-53.

Anti-TNF agents
• Etanercept was used in combination with standard therapy in patients with active GPA.
• The addition of etanercept to standard therapy did not prove beneficial in reducing the frequency of early disease relapses.
Etanercept plus standard therapy for Wegener’s granulomatosis. N Engl J Med 2005; 352:351-61.

Rituximab
• Chimeric monoclonal antibody against CD20• Induce death of both malignant and normal CD20+
B cells• Inhibit production of these autoantibodies (ANCA)
. Comarmond C, Cacoub P. Granulomatosis with polyangiitis (Wegener): clinical aspects and treatment.
Autoimmunity reviews. 2014;13(11):1121-5.

Making treatment decisionsThe site of disease is an important consideration
Major organ involvement
Glucocorticoidsand
Cytotoxic agent or Rituximab
Minor organ involvement
Joint,Skin Nasal and Sinus S/S
Sneller MC. et al.Middleton's Allergy ; 8th edition. 2014. p. 1014-131
Lung,Kidney
Tx with Glucocorticoidsand
Cytotoxic agent should be weight risk&benefit

Making treatment decisionsThe site of disease is an important consideration
Nasal and Sinus S/S
Sneller MC. et al.Middleton's Allergy ; 8th edition. 2014. p. 1014-131
Stepwise approach should be considered•Beginning with a program of local care including nasal irrigation and nasal glucocorticoids, combined with a course of antibiotics to treat superimposed infections.• If these measures are ineffective, use of low-dose glucocorticoids followed by methotrexate could be considered

Thaiwat S, Aunhachoke K. A case report of limited Wegener's granulomatosis presenting with a chronic scalp ulcer. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2010;93 Suppl 6:S208-11.

Thaiwat S, Aunhachoke K. A case report of limited Wegener's granulomatosis presenting with a chronic scalp ulcer. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2010;93 Suppl 6:S208-11.

Investigation
• Absolute eosinophil count = 672/μL• Blood chemistry :normal• Thyroid function test:normal• Urine and stool examinations:normal• ANA tests:negative• c-ANCA and p-ANCA were negative
Thaiwat S, Aunhachoke K. A case report of limited Wegener's granulomatosis presenting with a chronic scalp ulcer. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2010;93 Suppl 6:S208-11.

Investigation
• CXR:normal• EKG:normal• Abdominal USG:normal
Thaiwat S, Aunhachoke K. A case report of limited Wegener's granulomatosis presenting with a chronic scalp ulcer. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2010;93 Suppl 6:S208-11.

Investigation
• Paranasal sinus X-ray :showed a prominent right nasal turbinate. • Fiberoptic laryngoscopy :mild generalized swelling of nasopharynx,
turbinate and arytenoids but biopsies were all negative.
Thaiwat S, Aunhachoke K. A case report of limited Wegener's granulomatosis presenting with a chronic scalp ulcer. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2010;93 Suppl 6:S208-11.

Diagnosis
• He was diagnosed as limited form of Wegener’s granulomatosis. fulfilled two of the four criteria1. Skin lesions that showed eosinophilic
granuloma & vasculitis on skin biopsy 2. Swelling of nasopharynx, turbinate &
arytenoids
Thaiwat S, Aunhachoke K. A case report of limited Wegener's granulomatosis presenting with a chronic scalp ulcer. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2010;93 Suppl 6:S208-11.

Treatment
• Treated with combination of prednisolone and methotrexate.
Thaiwat S, Aunhachoke K. A case report of limited Wegener's granulomatosis presenting with a chronic scalp ulcer. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2010;93 Suppl 6:S208-11.

Take-Home Messages
• GPA is a multifocal vasculitis characterized by frequent involvement of the upper & lower respiratory tract & kidneys.
• The presence of c-ANCA with anti-proteinase 3 specificity is observed in more than 90% of pts with GPA.
• Two phenotypes of GPA are recognized: 1.Systemic forms with potentially life-threatening 2.Limited form

Take-Home Messages
• Effective induction therapy with corticosteroids combined with cyclophosphamide or rituximab transformed the survival of patients with GPA, with 5-year survival rates> 80%.

Take-Home Messages
• GPA is now a chronic relapsing disorder with >50% rate of relapse within 5 years of initial remission.
• Maintenance therapy to prevent relapses and the occurrence of late complications remains the main
therapeutic challenge in this vasculitis.


















