RITCHEY Manual de instrucciones Introducción Antes del primer ...

Canine Haemangiosarcoma
Lauren Ritchey
Megan 13yo Female Border Collie
Presentation: worsening lethargy. With a history of intermittent anemia over the last few weeks.
Clinical Findings:
QAR
Slightly pale MM, Normal CRT
Fluid thrill noted on abdominal palpation
HR 120 bpm, Temperature and RR wnl.

Investigations
Abdominal Ultrasound: revealed large volume of free fluid. Small cavitated mass adjacent to the spleen, and a larger mass arising in cd abdomen.
Abdomenocentesis: Blood (PCV 32%)
Orthogonal thoracic radiographs: unremarkable
Cardiac scan: No obvious masses
Hematology: Moderate Anemia (HCT 28%) (ref 37-55%) Neutrophilia (15x10^9/L) (ref 6-12x10^9/L) Thrombocytopenia (60x10^9/L) (ref 200-500x10^9/L)
Mildly prolonged APTT (37 seconds) (ref 17-24sec)

Diagnosis
Haemoabdomen, likely secondary to abdominal neoplasia.
Non Traumatic/Spontaneous Causes of Haemoabdomen
• Neoplasia***• Splenic hematoma • Splenic torsion• Coagulopathies • Vena caval syndrome secondary to Dirofilariasis

Plan
Referred to Soft Tissue service for an emergency exploratory laparotomy.
Findings of Exlap: Small mass on falciform fat Larger caudal abdominal mass 800ml of free blood Grossly abnormal liver
Both masses, and a liver biopsy were sent for histopathology.

Histopathology
The histological appearance of the two masses was consistent with an haemangiosarcoma.
No normal tissue is present in the examined sections to suggest a site of origin.

Haemangiosarcoma (HSA) Highly malignant tumor of endothelial cells.
Occurs more frequently in dogs than in any other species and is characterized by a high fatality rate (1)
The overall prevalence is reported to be 0.3% to 2.0% of all tumors in dogs; German shepherds, golden retrievers, and Labrador retrievers are overrepresented (2).
The etiology of HSA is still unknown, although the strong breed association suggests an inherited or familial predisposition.

Haemangiosarcoma (HSA) cont.
The 3 most common primary sites of HSA are the spleen (28% to 50%), right atrium/auricle (up to 50%), and skin or subcutaneous tissue (13%) (1,3).
Most common sites of metastasis of HSA: Lungs (65%) Spleen (36-60%) Kidneys (55%) Liver (41-55%)
which can occur via haematogenous spread or by local seeding after tumor rupture (1).

Common Laboratory Findings
Hematology: Anemia morphological changes to red blood cells:
nucleated erythrocytes Polychromasia poikilocytes, anisocytes, shistocytes, and
reticulocytes Neutrophilia
due to either stress or tumor rupture and necrosis thrombocytopenia

Common Diagnostic Imaging Findings
Thoracic Radiographs
Metastatic patterns in dogs with HSA: widely disseminated nodular pattern (common) diffuse interstitial pattern (uncommon)
Abdominal US
primary HSA: mixed pattern of anechoic and hyperechoic regions
metastatic HSA: diffusely anechoic or hypoechoic appearance
Echocardiography
Helps detect structural abnormalities, presence of tumours, clots or fluid.
Electrocardiography
ventricular arrhythmias are commonly associated with HSA due to hypoxia, anemia, or hypovolemia

Treatment of HSA
Usually a combination of:
Chemotherapy: Doxorubicin
+/- Cyclophosphamide (AC) +/-Vincristine (VAC)
Metronomic Chemotherapy Continuous low dose oral cyclophosphamide.
Surgical: Try to remove the primary tumour. Ex: SPLENECTOMY:
Historically the treatment of SPLENIC HSA.
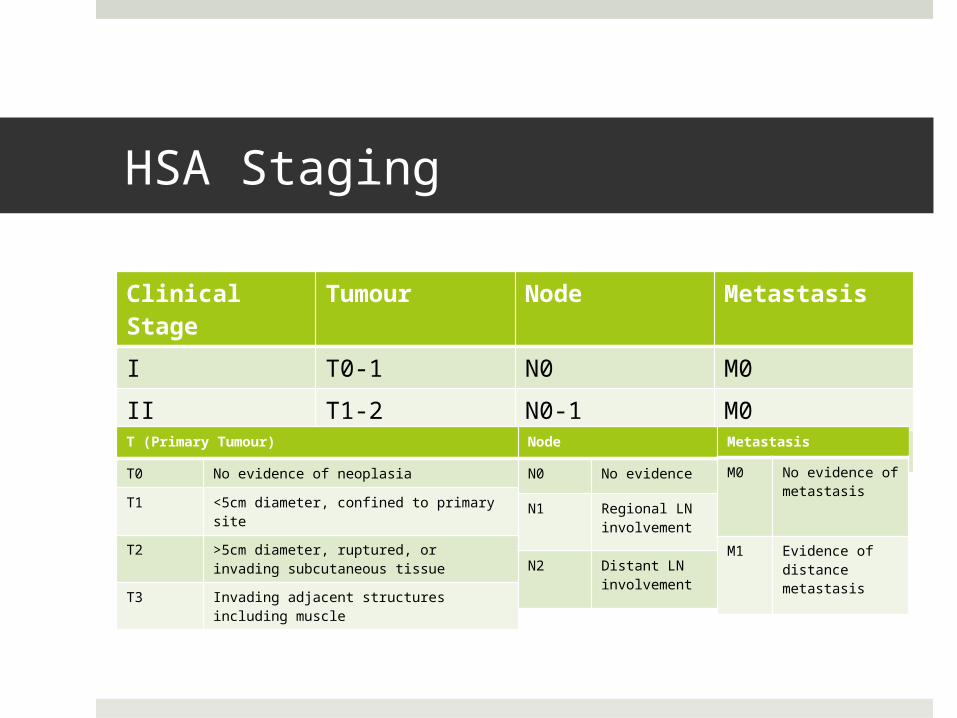
HSA Staging
Clinical Stage
Tumour Node Metastasis
I T0-1 N0 M0
II T1-2 N0-1 M0
III T2-3 N0-2 M1T (Primary Tumour)
T0 No evidence of neoplasia
T1 <5cm diameter, confined to primary site
T2 >5cm diameter, ruptured, or invading subcutaneous tissue
T3 Invading adjacent structures including muscle
Node
N0 No evidence
N1 Regional LN involvement
N2 Distant LN involvement
Metastasis
M0 No evidence of metastasis
M1 Evidence of distance metastasis

Prognosis
Relatively Poor
MST (Mean survival times)
Surgery alone: 2-3 months
Surgery followed by Chemotherapy: 4-6 months
Back to Megan…
Post Operatively:
Due to her loss of blood and thrombocytopenia she required fresh frozen plasma and Packed red cell transfusion
(post operative PCV 6%, Hg 2 g/dl) with good response over the following 24h.
She was sent home on strict cage rest, pain medications, antibiotics, and antiemetics. With a recheck in 10 days to remove the sutures and talk about chemotherapy treatment options.

Megan’s Treatment Plan
Pre Chemotherapy: Heart Scan
Showed adequate contractility Abdominal scan
Revealed a nodule on the left kidney that should be monitored
Start Doxorubicin therapy. One dose every 3 weeks, for 4-6 doses. She received her first dose this week. If protocol not tolerated, discussed switching to metronomic
chemotherapy.

Questions?

References
Canine hemangiosarcoma: retrospective analysis of 104 cases.Brown NO, Patnaik AK, MacEwen EG J Am Vet Med Assoc. 1985 Jan 1; 186(1):56-8.
Kahn, S. Anthony, et al. "Doxorubicin and deracoxib adjuvant therapy for canine splenic hemangiosarcoma: A pilot study." The Canadian Veterinary Journal 54.3 (2013): 237.
Sorenmo, K. U., Baez, J. L., Clifford, C. A., Mauldin, E., Overley, B., Skorupski, K., Bachman, R., Samluk, M. and Shofer, F. (2004), Efficacy and Toxicity of a Dose-Intensified Doxorubicin Protocol in Canine Hemangiosarcoma. Journal of Veterinary Internal Medicine, 18: 209–213. doi: 10.1111/j.1939-1676.2004.tb00162.x
Thamm DH. Hemangiosarcoma. In: Withrow SW, Vail DM, editors. Small Animal Clinical Oncology. 4th ed. St Louis, Missouri: Saunders/Elsevier; 2007. pp. 785–795.