Grand Rounds: Acute Respiratory Failure Ashley Hazelwood Ashley Hazelwood.
51
Grand Rounds: Grand Rounds: Acute Respiratory Failure Acute Respiratory Failure Ashley Hazelwood Ashley Hazelwood
-
Upload
sheila-welch -
Category
Documents
-
view
224 -
download
0
Transcript of Grand Rounds: Acute Respiratory Failure Ashley Hazelwood Ashley Hazelwood.

Grand Rounds: Grand Rounds: Acute Respiratory FailureAcute Respiratory Failure
Ashley HazelwoodAshley Hazelwood

DemographicsDemographics
78 year old African 78 year old African American FemaleAmerican Female
WidowedWidowed
Baptist Baptist
Never employedNever employed
One DaughterOne Daughter
Height: 64 inchesHeight: 64 inches
Weight: 84.9 KgWeight: 84.9 Kg
Allergy: TetanusAllergy: Tetanus
Full CodeFull Code

Events Leading to HospitalizationEvents Leading to Hospitalization
Total hysterectomy late FebruaryTotal hysterectomy late February
Sent to rehab facility after surgerySent to rehab facility after surgery
Found her unresponsiveFound her unresponsive
Experiencing agonal respirations Experiencing agonal respirations
Taken to hospital and intubated on 3/21Taken to hospital and intubated on 3/21
Risk FactorsRisk Factors
AgeAge
Ovarian Cancer stage IIIOvarian Cancer stage III
Total hysterectomy (abdominal incision)Total hysterectomy (abdominal incision)
HypertensionHypertension
DiabetesDiabetes
AnemiaAnemia

Past Medical HistoryPast Medical History
Right sided Right sided hydronephrosis hydronephrosis secondary to ovarian secondary to ovarian cancercancer
Pyelonephritis Pyelonephritis
GoutGout
HyperlipidemiaHyperlipidemia
Diabetes Diabetes
Hypertension Hypertension
AnemiaAnemia
OsteoarthritisOsteoarthritis

Medical DiagnosisMedical Diagnosis
Acute Respiratory FailureAcute Respiratory Failure
MRSAMRSA

Acute Respiratory FailureAcute Respiratory Failure
Classified as blood gas abnormalitiesClassified as blood gas abnormalities
Occurs rapidlyOccurs rapidly
Gives little time for body to compensateGives little time for body to compensate
Three types: Failure of oxygenation, failure of ventilation, Three types: Failure of oxygenation, failure of ventilation, and failure of bothand failure of both
Failure of OxygenationFailure of Oxygenation
Thoracic pressures are normal Thoracic pressures are normal
Pulmonary blood not adequately oxygenated Pulmonary blood not adequately oxygenated
4 Mechanisms 4 Mechanisms – HypoventilationHypoventilation– Intrapulmonary shuntingIntrapulmonary shunting– Ventilation/perfusion mismatchVentilation/perfusion mismatch– Diffusion defectsDiffusion defects

Failure of OxygenationFailure of Oxygenation
Hypoventilation: Hypoventilation: – Buildup of CO2 Buildup of CO2
displaces O2 displaces O2 (abdominal surgery)(abdominal surgery)
Intrapulmonary shunting:Intrapulmonary shunting:– Blood is shunted past Blood is shunted past
lungslungs– Unoxygenated blood Unoxygenated blood
sent back to left side sent back to left side of heart (atelectasis)of heart (atelectasis)
Ventilation/Perfusion Ventilation/Perfusion mismatch: mismatch: – Degree of a shuntDegree of a shunt– Degree of dead spaceDegree of dead space– Most common cause Most common cause
of hypoxemiaof hypoxemia
Diffusion:Diffusion:– Distance between Distance between
alveoli and capillaries alveoli and capillaries is increasedis increased

Failure of VentilationFailure of Ventilation
Perfusion is normalPerfusion is normal
Ventilation inadequate Ventilation inadequate
Little oxygen reaches alveoli Little oxygen reaches alveoli
Carbon dioxide is retainedCarbon dioxide is retained
Hypoxemia developsHypoxemia develops
2 mechanisms2 mechanisms– HypoventilationHypoventilation– Ventilation/Perfusion mismatch Ventilation/Perfusion mismatch
Failure of VentilationFailure of Ventilation
Hypoventilation: Hypoventilation: – CO2 accumulates in CO2 accumulates in
alveolialveoli– CO2 is not blown offCO2 is not blown off
Ventilation/Perfusion Ventilation/Perfusion mismatch:mismatch:– Increase in volume of Increase in volume of
dead spacedead space– Area no longer Area no longer
participates in gas participates in gas exchangeexchange

SymptomsSymptoms
Hallmark: DyspneaHallmark: Dyspnea
HypoxemiaHypoxemia
HypercapniaHypercapnia
Release of lactic acidRelease of lactic acid
Decreased level of Decreased level of consciousness consciousness
TachycardiaTachycardia
Increased blood pressureIncreased blood pressure
Peripheral Peripheral vasoconstrictionvasoconstriction

ComplicationsComplications
ImmobilityImmobility
Medication side effectsMedication side effects
Fluid and electrolyte Fluid and electrolyte imbalanceimbalance
Hazards of mechanical Hazards of mechanical ventilationventilation
Hazards of mechanical Hazards of mechanical ventilation:ventilation:– AspirationAspiration– VolutraumaVolutrauma– Oxygen toxicityOxygen toxicity– Ventilator associated Ventilator associated
pneumonia pneumonia

MRSA-Methicillin Resistant MRSA-Methicillin Resistant Staphylococcus AureusStaphylococcus Aureus
Bacteria resistant to certain antibiotics. Bacteria resistant to certain antibiotics.
Frequently found in:Frequently found in:– Immunocompromised patients patients– Hospitalized patientsHospitalized patients

Collaboration of CareCollaboration of Care
Nurses Nurses
Nursing StudentsNursing Students
Nursing InstructorNursing Instructor
PhysiciansPhysicians
Respiratory TherapistsRespiratory Therapists
Family Family

Respiratory AlkalosisRespiratory AlkalosisABGs 3/22/08ABGs 3/22/08 ResultResult High/LowHigh/Low RationaleRationale
pH pH 7.547.54 HighHigh
Normal:7.35-Normal:7.35-7.457.45
Mechanical Mechanical ventilationventilation
PCO2 PCO2 34.0 mmHg34.0 mmHg LowLow
Normal: 35-45Normal: 35-45
Increased Increased respiratory raterespiratory rate
PO2 PO2 109 mmHg109 mmHg HighHigh
Normal 80-100Normal 80-100
HyperventilationHyperventilation
HCO3HCO3 20 mmol/L20 mmol/L LowLow
Normal 22-26Normal 22-26
Compensating Compensating for alkalosisfor alkalosis

Laboratory ResultsLaboratory ResultsLabLab Result Result High/LowHigh/Low RationaleRationale
Serum Protein: Serum Protein: PrealbuminPrealbumin
3/25/20083/25/2008
<5.0 mg/dL<5.0 mg/dL LowLow
Normal: 18-25Normal: 18-25
Inflammation r/t Inflammation r/t acute acute respiratory respiratory failurefailure
Coagulation:Coagulation:
PTTPTT
3/25/20083/25/2008
70.9 Sec.70.9 Sec. HighHigh
Normal: 22-35Normal: 22-35
Prolonged Prolonged clotting time r/t clotting time r/t Lovenox Lovenox therapytherapy
MRSA swabMRSA swab
3/27/20083/27/2008
Positive for Positive for MRSA MRSA
AbnormalAbnormal
Normal: Normal: negative swabnegative swab
MRSA infectionMRSA infection

Laboratory ResultsLaboratory ResultsHematologyHematology
3/27/20083/27/2008
ResultsResults High/LowHigh/Low RationaleRationale
WBCWBC 28.7x10^3/mm328.7x10^3/mm3 HighHigh
Normal:4.3-Normal:4.3-10.010.0
Infection, Infection, stress, stress, inflammationinflammation
RBC RBC 3.37x10^6/mm33.37x10^6/mm3 LowLow
Normal:4.0-Normal:4.0-5.405.40
History of History of AnemiaAnemia
HemoglobinHemoglobin 9.3g/dl9.3g/dl LowLow
Normal:12.0-Normal:12.0-16.016.0
History of History of AnemiaAnemia
HematocritHematocrit 29.6%29.6% LowLow
Normal:35-Normal:35-47%47%
History of History of AnemiaAnemia
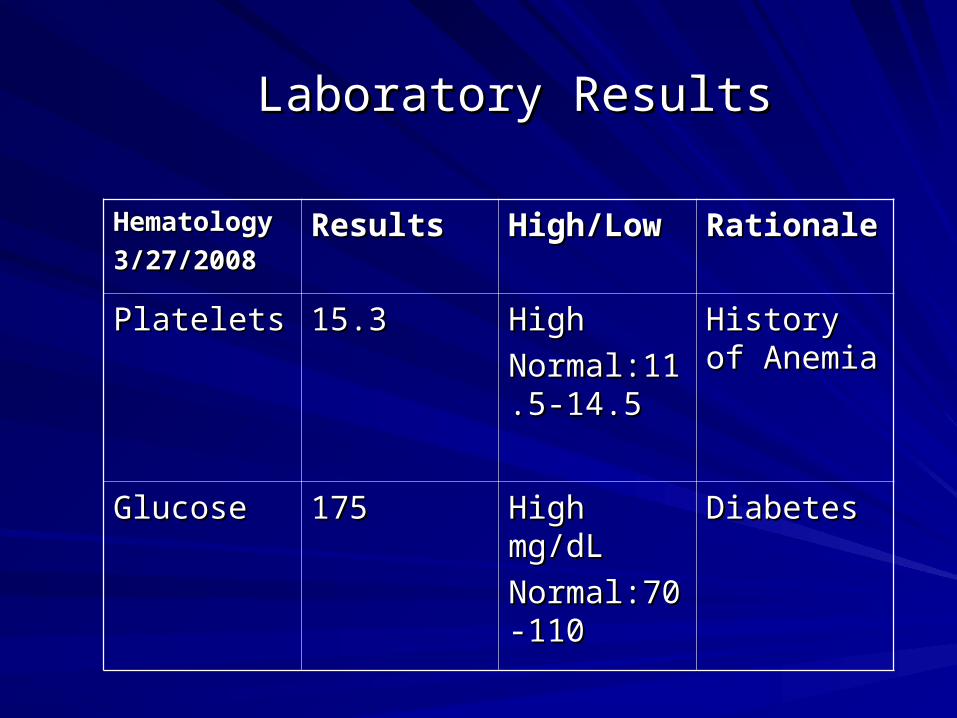
Laboratory ResultsLaboratory Results
HematologyHematology
3/27/20083/27/2008ResultsResults High/LowHigh/Low RationaleRationale
PlateletsPlatelets 15.315.3 HighHigh
Normal:11.5Normal:11.5-14.5-14.5
History of History of AnemiaAnemia
GlucoseGlucose 175175 High mg/dLHigh mg/dL
Normal:70-Normal:70-110110
DiabetesDiabetes

Diagnostics: X-RaysDiagnostics: X-RaysDiagnosticDiagnostic Date Date FindingsFindings
X-Ray: Placement of X-Ray: Placement of ET tubeET tube
3/213/21 Above Canna(1-2cm)Above Canna(1-2cm)
No infiltrates or No infiltrates or infusionsinfusions
X-Ray: Abdomen Flexi X-Ray: Abdomen Flexi flow placementflow placement
3/223/22 Tip in transport Tip in transport position in duodenal position in duodenal flapflap
X-Ray: Chest, post X-Ray: Chest, post procedure of procedure of thoracentesisthoracentesis
3/253/25 No pneumothorax, No pneumothorax, mild volume loss right mild volume loss right lung, no pulmonary lung, no pulmonary edemaedema
X-Ray: portable chestX-Ray: portable chest
PICC placementPICC placement
3/263/26 Right Upper Extremity, Right Upper Extremity, tip in mid-SVCtip in mid-SVC
X-Ray: ChestX-Ray: Chest 3/273/27 Atelectasis in lower left Atelectasis in lower left basebase
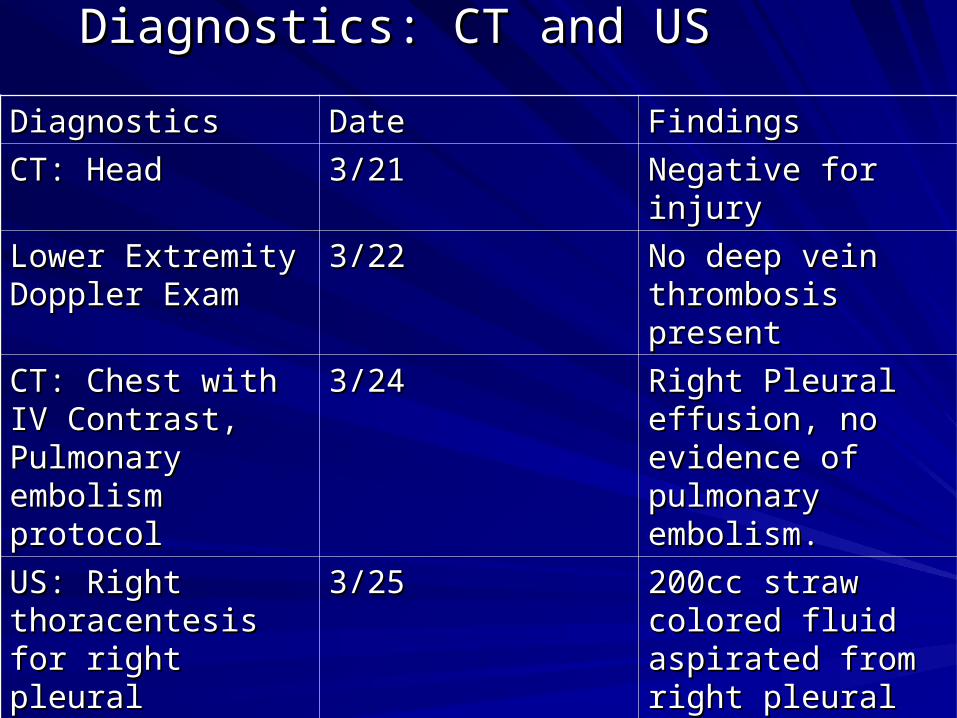
Diagnostics: CT and USDiagnostics: CT and US
DiagnosticsDiagnostics DateDate FindingsFindings
CT: HeadCT: Head 3/213/21 Negative for injuryNegative for injury
Lower Extremity Lower Extremity Doppler ExamDoppler Exam
3/223/22 No deep vein No deep vein thrombosis presentthrombosis present
CT: Chest with IV CT: Chest with IV Contrast, Pulmonary Contrast, Pulmonary embolism protocolembolism protocol
3/243/24 Right Pleural Right Pleural effusion, no effusion, no evidence of evidence of pulmonary pulmonary embolism.embolism.
US: Right US: Right thoracentesis for thoracentesis for right pleural effusionright pleural effusion
3/253/25 200cc straw colored 200cc straw colored fluid aspirated from fluid aspirated from right pleural space right pleural space

MedicationsMedicationsMedicationMedication ClassClass DoseDose RouteRoute FrequencyFrequency RationaleRationale
Insulin Insulin RegularRegular
Short acting Short acting insulininsulin
BG-BG-100/20=# U100/20=# U
SubQ SubQ QID,AC,QID,AC,
BedtimeBedtime
DiabetesDiabetes
Insulin Insulin LantusLantus
Long acting Long acting insulininsulin
15 Units15 Units SubQSubQ QdayQday DiabetesDiabetes
PulmocarePulmocare
Tube Tube FeedingFeeding
Nutrition Nutrition
supplementsupplement
40mL/h40mL/h Per TubePer Tube Continuous Continuous Feeding Q24 Feeding Q24 hourshours
Respiratory Respiratory failurefailure
BenazeprilBenazepril
(Lotensin)(Lotensin)
ACE ACE inhibitorinhibitor
10mg10mg Per TubePer Tube BIDBID HTN Hold if HTN Hold if SBP<100SBP<100
DiltiazemDiltiazem
(Cardizem)(Cardizem)
Ca channel Ca channel blocker blocker
60mg60mg Per TubePer Tube Q6hQ6h tachycardia,tachycardia,
HTNHTN
AmlodipineAmlodipine
(Norvasc)(Norvasc)
Ca channel Ca channel blockerblocker
10mg10mg Per TubePer Tube QdayQday HTN, HTN, TachycardiaTachycardia

MedicationsMedicationsMedicationMedication ClassClass DoseDose RouteRoute FrequencyFrequency RationaleRationale
EsomaprazoleEsomaprazole (nexium)(nexium)
Proton Proton pump pump
inhibitorinhibitor
40mg40mg Per Tube Per Tube add 15 mL add 15 mL of waterof water
QdayQday Prevent Prevent stress stress ulcersulcers
AlbuterolAlbuterol Broncho-Broncho-dilatordilator
4 puffs4 puffs InhalationInhalation
By RTBy RT
Q4hQ4h Respiratory Respiratory FailureFailure
Potassium Potassium ChlorideChloride
ElectrolyteElectrolyte 40 mEq 40 mEq Per Tube Per Tube TIDTID Prevent Prevent hypokalemiahypokalemia
EnoxaparinEnoxaparin
(Lovenox)(Lovenox)
AnticoagulantAnticoagulant, , low low molecular molecular weight weight heparinheparin
40mg40mg SubQ
abdomen
Q24hQ24h Prevent Prevent Deep vein Deep vein
thrombosisthrombosis

MedicationsMedicationsMedicationMedication ClassClass DoseDose RouteRoute FrequencyFrequency RationaleRationale
Piperacillin-Piperacillin-TazobactumTazobactum
(Zosyn)(Zosyn)
Extended Extended
Spectrum Spectrum
penicillinpenicillin
3.375 gm3.375 gm IV solutionIV solution
100mL/h100mL/h
Q6HQ6H MRSA, MRSA, Respiratory Respiratory FailureFailure
LinezolidLinezolid
(Zyvox)(Zyvox)
OxazolidinoneOxazolidinone 600mg600mg IV solutionIV solution
300mL/h300mL/h
BIDBID MRSAMRSA
FurosemideFurosemide
(Lasix)(Lasix)
Loop DiureticLoop Diuretic 40mg40mg Per Tube Per Tube BIDBID Peripheral Peripheral EdemaEdema
LoperamideLoperamide
(Immodium)(Immodium)
PiperidinePiperidine
DerivativeDerivative
2-4mg2-4mg Per Tube Per Tube PRN for PRN for diarrheadiarrhea
DiarrheaDiarrhea
Several soft Several soft stools a daystools a day

AssessmentAssessment
Vital Signs: Vital Signs: – BP:158/62BP:158/62– HR: 101HR: 101– RR: 29RR: 29– O2 sat: 99O2 sat: 99– Temp: 98.4Temp: 98.4– Pain: 0Pain: 0
Intake: Intake: – D5W with 40 D5W with 40
Potassium at 30mL/hPotassium at 30mL/h
Output: Output: – 3 to 4 stools a day3 to 4 stools a day– Zossi PlacedZossi Placed– Urine average of 40-Urine average of 40-
60 mL/h60 mL/h

Assessment: NeurologicalAssessment: Neurological
LOC: LOC: – easily arousedeasily aroused– alert responds to alert responds to
verbal stimuliverbal stimuli– calm, nods to calm, nods to
questionsquestions
Pupils are PERRLA Pupils are PERRLA
Coma Score: Coma Score: – Eyes Open: Spont. 4Eyes Open: Spont. 4
– Best Verbal Best Verbal Response: T (Trach)Response: T (Trach)
– Best Motor Response: Best Motor Response: Obeys Commands 6Obeys Commands 6
– Total: 10TTotal: 10T
Assessment: HEENTAssessment: HEENT
Head: Head: – No lumps, lesions or No lumps, lesions or
tendernesstenderness– SymmetricalSymmetrical
Face: Face: – Symmetrical Symmetrical – No weaknessNo weakness– No involuntary No involuntary
movementsmovements
Eyes: Eyes: – Brows and lashes Brows and lashes
presentpresent– No ptosisNo ptosis– Conjunctiva clearConjunctiva clear– Sclera whiteSclera white– No lesionsNo lesions
Ears: Ears: – No masses, or lesionsNo masses, or lesions– No tenderness or No tenderness or
dischargedischarge

Assessment: HEENTAssessment: HEENT
Nose: Nose: – SymmetricalSymmetrical– No drainageNo drainage– Flexi Flow in left Flexi Flow in left
nostril nostril – No skin breakdownNo skin breakdown
Throat: Throat: – Endotracheal tube in Endotracheal tube in
placeplace– Trachea midlineTrachea midline– No painNo pain– Teeth missingTeeth missing– Mucosa pink and dryMucosa pink and dry

Assessment: MusculoskeletalAssessment: Musculoskeletal
NonambulatoryNonambulatory
Limited range of motionLimited range of motion
Assist with all activities of Assist with all activities of daily livingdaily living
Minimal equal weakness: Minimal equal weakness: upper extremitiesupper extremities
General weakness: left General weakness: left lower extremitylower extremity
Greater weakness: right Greater weakness: right lower extremitylower extremity

Assessment: CardiovascularAssessment: Cardiovascular
Normal heart sounds, S1 Normal heart sounds, S1 and S2 notedand S2 noted
Telemetry: Normal sinus Telemetry: Normal sinus rhythm with premature rhythm with premature atrial beatsatrial beats
No jugular vein distentionNo jugular vein distention
Capillary Refill <3 Capillary Refill <3 secondsseconds
Right and left dorsalis Right and left dorsalis pedis weakpedis weak
Right and left radial 2+Right and left radial 2+
2+ edema in lower 2+ edema in lower extremitiesextremities
1+ edema in hands1+ edema in hands

Assessment: RespiratoryAssessment: Respiratory
Clear lung soundsClear lung sounds
Diminished lung sounds Diminished lung sounds in bases bilaterallyin bases bilaterally
Sputum thick and whiteSputum thick and white
Mechanical Mechanical Ventilation Settings:Ventilation Settings:– CPAPCPAP– PEEP: 5PEEP: 5– FiO2: 30%FiO2: 30%– Pressure Support: 20Pressure Support: 20– Vt: 600Vt: 600

Assessment: GastrointestinalAssessment: Gastrointestinal
Bowel sounds in all four Bowel sounds in all four quadrants quadrants
Abdomen Soft and Abdomen Soft and distendeddistended
Healed abdominal Healed abdominal incision from incision from hysterectomy (midline)hysterectomy (midline)
Impaired swallowing: Impaired swallowing: mechanical ventilationmechanical ventilation
NPO NPO
Flexi Flow NGTFlexi Flow NGT– Continuous feeding: Continuous feeding:
Pulmacore at 40mL/hPulmacore at 40mL/h
Several loose, yellow Several loose, yellow stools a daystools a day
Zossi PlacedZossi Placed

Assessment: GenitourinaryAssessment: Genitourinary
Urine clearUrine clear
Color: pale yellowColor: pale yellow
Urine output > 30mL/hUrine output > 30mL/h
Foley catheter in place and patentFoley catheter in place and patent

Assessment: IntegumentaryAssessment: Integumentary
Excoriated skin on Excoriated skin on buttocks and perineumbuttocks and perineum
Stage 2 breakdownStage 2 breakdown
Braden Score:Braden Score:– Sensory Perception: Sensory Perception:
no impairment 4no impairment 4– Moisture: very moist Moisture: very moist
22– Activity: bedfast 1Activity: bedfast 1– Mobility: very limited Mobility: very limited
22– Nutrition: adequate Nutrition: adequate
33– Friction & Shear: Friction & Shear:
problem 1 problem 1 – Total: 13 Total: 13
interventions in interventions in placeplace

Assessment: IntegumentaryAssessment: Integumentary
Other areas of skin dry, Other areas of skin dry, warm, and intactwarm, and intact
No clubbing No clubbing
PICC on right upper PICC on right upper forearm:forearm:– No infiltration or No infiltration or
inflammationinflammation– Dressing dry and Dressing dry and
intactintact– Patent Patent

Assessment: PsychosocialAssessment: Psychosocial
Patient cried a few times Patient cried a few times from impaired from impaired communication and communication and several accidentsseveral accidents
Most of the time was Most of the time was calm and restingcalm and resting
Had family support at Had family support at bedsidebedside
Daughter visited Daughter visited everydayeveryday
Was there by 0800 every Was there by 0800 every morning morning

Impaired Gas ExchangeImpaired Gas Exchange
Related toRelated to altered oxygen altered oxygen supply secondary to supply secondary to acute respiratory failure.acute respiratory failure.
As Evidenced By:As Evidenced By:– abnormal ABGs abnormal ABGs
(pH:7.54, (pH:7.54, CO2:34.0mmHg, CO2:34.0mmHg, O2:109mmHg, O2:109mmHg, HCO3:29.2mmol/L)HCO3:29.2mmol/L)
– tachypnea (varying tachypnea (varying from 29-33)from 29-33)
– tachycardia (101)tachycardia (101)– anxietyanxiety– dyspneadyspnea– mechanical ventilationmechanical ventilation– decreased RBCs decreased RBCs
(3.37x10^6/mm3), Hgb (3.37x10^6/mm3), Hgb (9.3g/dl), Hct (29.6%)(9.3g/dl), Hct (29.6%)

Goals and InterventionsGoals and Interventions
Goal: Patient will not Goal: Patient will not experience discomfort in experience discomfort in maintaining air exchange maintaining air exchange
Interventions:Interventions:– Monitor VS and I&O Monitor VS and I&O
every hourevery hour– Position every 2 Position every 2
hourshours– Suction as neededSuction as needed– Elevate HOB Elevate HOB – Assess lung sounds Assess lung sounds
every assessmentevery assessment– Assess for Assess for
restlessness and restlessness and change in LOC change in LOC
– Provide ADLs, restProvide ADLs, rest

EvaluationEvaluation
Vital signs and I&O Vital signs and I&O recorded every hourrecorded every hour
Positioned every two Positioned every two hours to promote gas hours to promote gas exchangeexchange
No further ABGs were No further ABGs were drawndrawn
Suctioned twice a daySuctioned twice a day
Lung sounds remained Lung sounds remained clear clear Remained alert and Remained alert and orientedorientedMouth care and bathing Mouth care and bathing was performed was performed Head of bed elevatedHead of bed elevatedO2 oximetry stayed O2 oximetry stayed above 90above 90No signs of respiratory No signs of respiratory distressdistress

Impaired Skin Integrity Impaired Skin Integrity
Related to immobility Related to immobility secondary to mechanical secondary to mechanical ventilationventilation
As Evidenced By:As Evidenced By:– Excoriated buttocks Excoriated buttocks
and perineum, stage 2and perineum, stage 2– Braden score of 13Braden score of 13– InflammationInflammation– DiarrheaDiarrhea– Increased WBC Increased WBC
(28.7x10^3/mm3)(28.7x10^3/mm3)– Low pre albumin Low pre albumin
(<5.0mg/dL) (<5.0mg/dL) – Decreased RBCs Decreased RBCs
(3.37x10^6/mm3), Hgb (3.37x10^6/mm3), Hgb (9.3g/dl), Hct (29.6%)(9.3g/dl), Hct (29.6%)

Goals and InterventionsGoals and InterventionsGoal: Patient will not Goal: Patient will not exhibit any further exhibit any further breakdown.breakdown.
Interventions: Interventions: – Assess skin every Assess skin every
shift assessment shift assessment – Keep skin dry and Keep skin dry and
cleanclean– Turn and position Turn and position
every two hoursevery two hours– Clean accidents Clean accidents
promptly, make sure promptly, make sure zossi is draining zossi is draining with no leaks.with no leaks.
– Apply skin creamApply skin cream– Consult with wound Consult with wound
care nursecare nurse

EvaluationEvaluation
Skin assessed and Skin assessed and documented every eight documented every eight hours.hours.
Patient cleaned promptly Patient cleaned promptly when had accidentwhen had accident
Patient was bathed and Patient was bathed and skin driedskin dried
Turned and positioned Turned and positioned every two hoursevery two hours
No further breakdown No further breakdown occurredoccurred

Impaired Verbal CommunicationImpaired Verbal Communication
Related to artificial airway Related to artificial airway and mechanical and mechanical ventilation secondary to ventilation secondary to respiratory failurerespiratory failure
As Evidenced By: As Evidenced By: – ET tubeET tube– AnxietyAnxiety– Few episodes of Few episodes of
cryingcrying– FrustrationFrustration

Goals and InterventionsGoals and Interventions
Goal: Patient will be able Goal: Patient will be able to communicate her to communicate her needs to the best of her needs to the best of her abilityability
InterventionsInterventions– Establish method that Establish method that
is appropriate for heris appropriate for her– Attempt reading Attempt reading
gesturesgestures– Speak slowly and Speak slowly and
clearlyclearly– Explain proceduresExplain procedures– Expect frustrationExpect frustration– Involve familyInvolve family
EvaluationEvaluation
I used yes/no questions I used yes/no questions to communicate with N.M.to communicate with N.M.
Able to nod to answer my Able to nod to answer my questionsquestions
Every procedure was Every procedure was explained in a clear slow explained in a clear slow mannermanner
Frustration and anxiety Frustration and anxiety were decreased when were decreased when she used the yes/no she used the yes/no responsesresponses
Family was involved in Family was involved in trying to communicate trying to communicate with N.M.with N.M.

Research ArticleResearch Article
A Prospective, Randomized Study of A Prospective, Randomized Study of Ventilator-Associated Pneumonia in Ventilator-Associated Pneumonia in Patients Using a Closed vs. Open Patients Using a Closed vs. Open
Suction System Suction System

PurposePurpose
Verify incidence of nosocomial pneumonia in Verify incidence of nosocomial pneumonia in mechanically ventilated patients having suctioning by mechanically ventilated patients having suctioning by open vs. closed suction method open vs. closed suction method

Methods and Sample SizeMethods and Sample Size
Methods: Methods: – Randomized assay Randomized assay – Parallel groups Parallel groups – Approval was givenApproval was given
Sample:Sample:– Forty seven patientsForty seven patients– Twenty-four received Twenty-four received
open suctionopen suction– Twenty-three received Twenty-three received
closed suctionclosed suction– All older than thirteenAll older than thirteen– Mechanical ventilation Mechanical ventilation
greater than forty eight greater than forty eight hours hours

ResultsResults
Of 24 receiving open Of 24 receiving open suctioningsuctioning– 11 developed 11 developed
ventilator-associated ventilator-associated pneumoniapneumonia
Of 23 receiving closed Of 23 receiving closed suctioning suctioning – 7 developed ventilator-7 developed ventilator-
associated pneumoniaassociated pneumonia
Use of a closed suction Use of a closed suction system did not decrease system did not decrease the incidence compared the incidence compared with the open systemwith the open system

Relation to patient Relation to patient
On mechanical ventilationOn mechanical ventilation
At risk for developing ventilator-associated pneumoniaAt risk for developing ventilator-associated pneumonia
Receiving closed system suctioning Receiving closed system suctioning
Did not acquire pneumonia during my careDid not acquire pneumonia during my care

ReferencesReferences
Ignatavicius, D., and Workman, JL (2006). Medical-surgical nursing: Critical Ignatavicius, D., and Workman, JL (2006). Medical-surgical nursing: Critical thinking for collaborative care. 5th ed. Philadelphia: WB Saunders.thinking for collaborative care. 5th ed. Philadelphia: WB Saunders.
MRSA Infection (2008). MayoClinic.com MRSA Infection (2008). MayoClinic.com http://www.mayoclinic.com/print/mrsa/DS00735/METHOD=print&DSECTION=all
Zeitoun, S., Barros, A., Diccini, S. (2003). A prospective, randomized study of Zeitoun, S., Barros, A., Diccini, S. (2003). A prospective, randomized study of ventilator-associated pneumonia in patients using a closed vs. open suction ventilator-associated pneumonia in patients using a closed vs. open suction system. system. Journal of Clinical Nursing, Journal of Clinical Nursing, 12, 484-489. 12, 484-489.
Pagan, K. and Pagana T. Pagan, K. and Pagana T. Mosby’s Diagnostic and Laboratory Test Reference. Mosby’s Diagnostic and Laboratory Test Reference. 77thth edition. edition. Elsvier Mosby Inc. Philadelphia, PA, 2005. Elsvier Mosby Inc. Philadelphia, PA, 2005.
Skidmore-Roth, L. (2007). Mosby’s drug guide for nurses, 7Skidmore-Roth, L. (2007). Mosby’s drug guide for nurses, 7 thth edition. St. Louis: edition. St. Louis: Mosby Elsevier. Mosby Elsevier.
Sole, ML, Klein, D, and Moseley, M (2004). Introduction to critical care nursing. Sole, ML, Klein, D, and Moseley, M (2004). Introduction to critical care nursing. 4th edition. Philadelphia: WB Saunders.4th edition. Philadelphia: WB Saunders.