Grand Rounds
26
Grand Rounds Eddie Apenbrinck M.D. University of Louisville School of Medicine Department of Ophthalmology & Visual Sciences 3/7/2014
-
Upload
trevor-camacho -
Category
Documents
-
view
71 -
download
2
description
Grand Rounds. Eddie Apenbrinck M.D . University of Louisville School of Medicine Department of Ophthalmology & Visual Sciences 3/7/2014. Subjective. CC: Left inferotemporal periorbital tenderness and swelling - PowerPoint PPT Presentation
Transcript of Grand Rounds

Grand Rounds
Eddie Apenbrinck M.D.University of Louisville School of
MedicineDepartment of Ophthalmology & Visual
Sciences3/7/2014

SubjectiveCC: Left inferotemporal periorbital
tenderness and swelling
HPI: 17 year old white female with a 2 ½ month history of chronic sinus congestion presents to Kosair ED with 1 day of tenderness and swelling of the left inferotemporal orbital rim

Treatment prior to ED Diagnosed with pansinusitis 2 week prior
to ED visit Started on clindamycin and prednisone PO
Minimal improvement on antibiotics and steroids CT sinuses: erosion of nasal septum Nasal Mucosa Biopsy:
Initially read as likely granulomatosis with polyangiitis (GPA)
Second opinion read biopsy as possible Epstein Bar Virus (EBV) lymphoma
Treated with pulse steroids and scheduled for pediatric rheumatology appointment

POH: Myopic
PMHx: saddle nose deformity
FHx: seasonal allergies
ROS: intermittent headaches, epistaxis, myalgia and fatigue (~2½ months)
Allergies: cefprozil (hives)
Meds: none

Exam OD OS
VA(sc,n): 20/20 OU
Pupils: 3 2 OU No RAPD
IOP: 12 OU EOM: Full OU
slight inferior periorbital tenderness on upgaze
Orbits: No proptosis, No lid retraction, No ecchymosis

Exam OD OSAnterior Segment
L/L: WNL slight swelling of left inferotemporal periorbital areaC/S: WNL OU K: WNL OU AC: No cell or flare OU
I/L: WNL OUVitreous: WNL OU
Dilated Fundus Exam: WNL OU


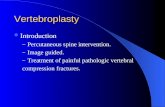
MRI
T2 Coronal MRI of orbits shows enhancement of ethmoid sinus with erosion into left medial orbit

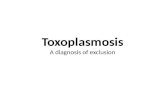
MRI
T1 Axial with gadolinium shows enhancement of ethmoid sinus with erosion into left medial orbit

Assessment
Assessment: 17yo white female with chronic sinus congestion found to have an ethmoid sinus lesion with extension into the left orbit.
DDx Granulomatosis with polyangiitis (GPA) EBV lymphoma Chronic Sinusitis

Plan Plan
Admission for further workup and treatment
Started on IV ampicillin-sulbactam (Unasyn) 3,000mg q6h
Repeat biopsy of nasal mucosa Biopsy of left inferior nasal septum and left
inferior turbinate obtained and sent to pathology
Ophthalmology follow-up as outpatient following discharge

Hospital CourseLabs
ESR: 65 (0-25)CRP: 166.7 (1.0-9.0)Proteinase-3 Auto
Antibodies: positivec-ANCA: negativep-ANCA: negativeMyeloperoxidase Auto
antibodies: negativeTSH: wnlFree T4: wnl
Immunoglobulin Panel: (all WNL)C3 149C4 25IgA 165IgG 949IgM 67
CBC, CMP and UA: wnl
Gram Stain: positive for gram negative bacillus
Nasal Mucosa Culture: Klebsella Pneumonia

Hospital Course
Imaging CXR, MRI/MRA brain: WNL
Flow Cytometry normal percentages and absolute numbers of T-
cell, B-cell and natural killer cell populations. No evidence of B-cell monoclonality or increased blast population
Anatomic Pathology Both biopsy samples showed necrotizing
granulomatous inflammation consist with GPA

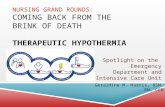
Pathology
Necrotizing granulomatous inflammation
10x magnification
20x magnification
eosinophiles
Multinucleated giant cell
granuloma
Granuloma with necrotic center

Hospital Course
Started on Solumedrol 1g once followed by oral taper as outpatient
Started on rituximab (15mg/kg) and cyclophosphamide (15mg/kg) once
Patient discharged with plan for readmission in 2 weeks for second dose of rituximab and cyclophosphamide

Ophthalmology 1 week follow up OD OS
VA(cc): 20/20 OUPupils: 4 3 OU; No RAPDIOP: 13 14EOM Full OU without painAnt Segment: WNL OUDFE: WNL OU
Assessment: Patient with GPA currently asymptomatic
Plan: Observe with follow-up in 6 months

Clinical Course Second dose of rituximab and cyclophosphamide
2 weeks after discharge Patient with increased energy, no epistaxis and
improved nasal congestion CBC & CMP: WNL CRP = 15.8 (<10.0)
Patient was started on maintenance therapy of Azathioprine, Bactrim, and continued prednisone taper

Granulomatosis with Polyangiitis GPA is a multisystem autoimmune disorder
characterized by the classic triad of necrotizing granulomatous vasculitis of the upper and lower respiratory tract, focal segmental glomerulonephritis, and necrotizing vasculitis of small vessels
Incidence: 3 per 100,000 reported in United States
Differential Diagnosis: Clinical: Orbital pseudotumor, Sarcoidosis, fungal
infections, Histiocytosis X, IGG4-related disease, , Rosai-Dorfman disease (sinus histiocytosis with massive lymphadenopathy),
Pathology: polyarteritis nodosa, microscopic polyangiitis, Churg-Strauss syndrome

Anti-cytoplasmic Nuclear Antibodies (ANCA): staining occurs in two patterns Cytoplasmic staining pattern (C-ANCA), which is
specific for Proteinase-3 (PR3) also called myeloblastin Perinuclear staining pattern (P-ANCA), which is specific
for myeloperoxidase
32% to >95% of patients with GPA are positive C-ANCA depending on disease activity 7
91% sensitivity and 99% specificity in active disease 8
Less than 5% of patient with GPA are positive for P-ANCA
Granulomatosis with Polyangiitis

Clinical Features Patient typically have flu-like symptoms lasting
several days or weeks including fever, polymyalgia, polyarthralgia, headache, malaise, anorexia, unintended weight loss
90% of patients report ear, nose, or throat problems
75% of patients seek care because of upper and lower respiratory complaints
Ocular or orbital involvement is seen in 15% of patients at presentation and up to 50% during the course of the disease.

Clinical Features
Chronic Complications: Orbital socket contracture, enophthalmos, restrictive ophthalmopathy, chronic orbital pain
Foster CS, Yang J. Wegener’s Granulomatosis. Albert & Jakobiec's Principles and Practice of Ophthalmology. Pages 4447- 4460. 2008.

Treatment There is no standardized treatment regimen for
granulomatosis with polyangiitis
Treatment is aimed at inducing remission General approach includes high-dose steroids and
cyclophosphamide Rituximab-based regimen plus steroids may be
considered as alternative in patients with relapsing or refractory disease
Remission maintained with cyclophosphamide, methotrexate or azathioprine
Plasma exchange may be beneficial in patients with severe renal disease

Randomized double blind clinical trial included 197 patients, compared rituximab (once a week for 4 weeks) followed by placebo to cyclophosphamide administered for 3 to 6 months followed by azathioprine for 12 to 15 months.
Both groups showed comparable rates of remission at 6, 12 and 18 months
Conclusion: a single course of rituximab was as effective as continuous conventional immunosuppressive therapy for the induction and maintenance of remission over the course of 18 months.
Literature Search
Aug 2013

Literature Search
Retrospective noninterventional comparative case series including 247 patients with orbital inflammation, compared GPA with other causes of orbital inflammation to identify the presenting clinical and radiographic features most likely to predict GPA
Features highly suggestive of GPA: sinonasal symptoms, sinonasal changes, or paranasal bone erosion on imaging.
22% of patients (8/37) with GPA had evidence of systemic involvement at presentation, and no patient presenting with only orbital GPA developed later systemic disease over a median follow-up of 2.7 years.
Ophthalmology. 2014 Feb

Thank You

References1. BCSC: Intraocular Inflammation and Uveitis. Pgs :145-1462. BCSC: Update on General Medicine. Optic Neuritis. Pgs 177-1793. Pakrou N, Selva D, Leibovitch I. Wegener;s Granulomatosis:
ophthalmic manifestations and management. Semin Arthritis Rheum. 2006;35(5):284-292
4. Berden A, Göçeroglu A, Jayne D, et al. Diagnosis and management of ANCA associated vasculitis. BMJ. 2012 Jan 16;344:e26.
5. Schilder AM. Wegener's Granulomatosis vasculitis and granuloma. Autoimmun Rev. 2010 May;9(7):483-7.
6. Tan LT, Davagnanam I, et.al. Clinical and Imaging Features Predictive of Orbital Granulomatosis with Polyangiitis and the Risk of Systemic Involvement. Ophthalmology. 2014 Feb 20. pii: S0161-6420(13)01175-5. doi: 10.1016/j.ophtha.2013.12.003. [Epub ahead of print]
7. Foster CS, Yang J. Wegener’s Granulomatosis. Albert & Jakobiec's Principles and Practice of Ophthalmology. Pages 4447- 4460. 2008.
8. Schonermarck U, Lamprecht P, Csernok E, Gross WL. Prevalence and spectrum of rheumatic diseases associated with proteinase 3-antineutrophil cytoplasmic antibodies (ANCA) and myeloperoxidases- ANCA. Rheumatology 2001; 40; 178-84
9. Specks U, Merkel PA, Seo P, Spiera R et al. RAVE-ITN Research Group. Efficacy of remission-induction regimens for ANCA-associated vasculitis. N Engl J Med. 2013 Aug 1;369(5):417-27.