GRAND ROUNDS 22 nd February, 2006 22 nd February, 2006 Dr. N. Singh Dr. N. Singh Dr. O. Ingaramo Dr....
55
GRAND ROUNDS GRAND ROUNDS 22 22 nd nd February, 2006 February, 2006 Dr. N. Singh Dr. N. Singh Dr. O. Ingaramo Dr. O. Ingaramo Dr. S. Manuel Dr. S. Manuel
-
Upload
robyn-burke -
Category
Documents
-
view
219 -
download
1
Transcript of GRAND ROUNDS 22 nd February, 2006 22 nd February, 2006 Dr. N. Singh Dr. N. Singh Dr. O. Ingaramo Dr....

GRAND ROUNDSGRAND ROUNDS
2222ndnd February, 2006 February, 2006
Dr. N. SinghDr. N. Singh
Dr. O. IngaramoDr. O. Ingaramo
Dr. S. ManuelDr. S. Manuel

HISTORY OF PRESENT HISTORY OF PRESENT ILLNESSILLNESS
An An 8 m8 m old boy was brought to the ER with a old boy was brought to the ER with a history of several episodes of history of several episodes of epistaxisepistaxis over over the last 12 hrs. the last 12 hrs.
The mother was also concerned about some The mother was also concerned about some scattered scattered bruisingbruising on her son’s forehead, on her son’s forehead, occiput, elbows and flanks over the last 10 occiput, elbows and flanks over the last 10 days.days.

DEVELOPMENT HISTORYDEVELOPMENT HISTORY
Sitting by himself, crawling, in walker.Sitting by himself, crawling, in walker.Imm HX: Delayed – needs 6 mo vaccinations.Imm HX: Delayed – needs 6 mo vaccinations.PM Hx: 1. PM Hx: 1. Enterococcal Meningitis @ Enterococcal Meningitis @ birthbirth
2. 2. ALTE at 1 mo of ageALTE at 1 mo of age – cyanotic – cyanotic episode at home, episode at home, apneas noticed during apneas noticed during hospitalization.hospitalization.

FAMILY AND SOCIAL HISTORYFAMILY AND SOCIAL HISTORYNo h/o bleeding disorders.No h/o bleeding disorders.Single mother, lives with boyfriend in a trailer Single mother, lives with boyfriend in a trailer park.park. No h/o substance abuse.No h/o substance abuse. Primary caretaker is mother.Primary caretaker is mother. Infant also spends time in a daycare and with Infant also spends time in a daycare and with father of boyfriend (esophageal cancer).father of boyfriend (esophageal cancer).

PHYSICAL EXAMPHYSICAL EXAM
Afebrile, normal vital signs.Afebrile, normal vital signs.Wt: 5Wt: 5thth percentile percentile; Length: 10; Length: 10thth percentile; HC: 25 percentile; HC: 25thth percentile. Alert, interactive and in no distresspercentile. Alert, interactive and in no distressHEENT: With some dried blood in nares.HEENT: With some dried blood in nares. Neck: No Lymph nodes palpable. Neck: No Lymph nodes palpable. Chest: CTA B/L Chest: CTA B/L CVS-No murmur CVS-No murmur

PHYSICAL EXAMPHYSICAL EXAM
Abd - No HSM (hepatosplenomegaly), No Abd - No HSM (hepatosplenomegaly), No masses. masses.
Ext: FROM, No swelling in joints.Ext: FROM, No swelling in joints.
Skin: Several areas of green-yellow areas of Skin: Several areas of green-yellow areas of bruising on the forehead, occiput, elbows and bruising on the forehead, occiput, elbows and flanks.flanks.

SUMMARYSUMMARY
An An 8 m8 m old boy with old boy with epistaxisepistaxis over the last over the last 12 hrs. 12 hrs. BruisingBruising on forehead, occiput, elbows and on forehead, occiput, elbows and flanks over the last 10 days.flanks over the last 10 days.Enterococcal Meningitis @ birthEnterococcal Meningitis @ birth ALTE at 1 mo of ageALTE at 1 mo of age – cyanotic – cyanotic episode at home, episode at home, apneas noticed during apneas noticed during hospitalizationhospitalization

SUMMARYSUMMARY
No h/o bleeding disordersNo h/o bleeding disordersSingle mother, lives with boyfriend in a trailer Single mother, lives with boyfriend in a trailer park.park.Father of boyfriend (esophageal cancer).Father of boyfriend (esophageal cancer).Afebrile, normal vital signsAfebrile, normal vital signsWt: 5Wt: 5thth percentile percentile ; Length: 10; Length: 10thth percentile; percentile; HC: 25HC: 25thth percentile. Alert, interactive and in percentile. Alert, interactive and in no distress.no distress.

SUMMARYSUMMARY
HEENT: With some dried blood in nares.HEENT: With some dried blood in nares. Neck: No Lymph nodes palpable.Neck: No Lymph nodes palpable.Abd - No HSM (hepatosplenomegaly), No Abd - No HSM (hepatosplenomegaly), No masses masses Ext: FROM, No swelling in jointsExt: FROM, No swelling in jointsSkin: Several areas of green-yellow areas of Skin: Several areas of green-yellow areas of bruising on the forehead, occiput, elbows and bruising on the forehead, occiput, elbows and flanksflanks

HEMOSTASIS REQUIRES HEMOSTASIS REQUIRES NORMAL:NORMAL:
VesselsVessels
Platelets Platelets
Coagulation pathway components.Coagulation pathway components.


DIFFERENTIAL DIAGNOSIS OF DIFFERENTIAL DIAGNOSIS OF BLEEDING DISORDERSBLEEDING DISORDERS
Platelets Platelets – petechiae, mucosal bleeding petechiae, mucosal bleeding – CNS bleeding in severe casesCNS bleeding in severe cases
VascularVascular– contusion, ecchymosis, hemorrhagecontusion, ecchymosis, hemorrhage– palpable purpurapalpable purpura
Coagulation disorders Coagulation disorders – Usually cause larger ecchymoses, deep tissue Usually cause larger ecchymoses, deep tissue
hemorrhage, and mucosal bleedinghemorrhage, and mucosal bleeding

PLATELETS DISORDERSPLATELETS DISORDERS
Thrombocytopenias:Thrombocytopenias:
Decreased production.Decreased production.
Platelet pooling and splenic sequestration .Platelet pooling and splenic sequestration .
Increased destruction.Increased destruction.
– Plt <100 000Plt <100 000
– Spontaneous bleeding uncommmon with plt > 20,000.Spontaneous bleeding uncommmon with plt > 20,000.
– Bleeding time prolonged, PT/PTT normal.Bleeding time prolonged, PT/PTT normal.

PLATELETS DISORDERS (cont.)PLATELETS DISORDERS (cont.)
Decreased Production:Decreased Production:
Malignancies (leukemia, lymphoma, neuroblastoma).Malignancies (leukemia, lymphoma, neuroblastoma).
Bone marrow suppressionBone marrow suppression– Drug-related (aplastic anemia)Drug-related (aplastic anemia)
– Infection Infection
Congenital Congenital – Fanconi anemiaFanconi anemia
– TAR syndromeTAR syndrome
– Wiscott-AldrichWiscott-Aldrich
– Glycogen storage diseasesGlycogen storage diseases

PLATELETS DISORDERS (cont.)PLATELETS DISORDERS (cont.)
Platelet Dysfunction:Platelet Dysfunction: CongenitalCongenital– Glanzmanns thrombasthenia (GPGlanzmanns thrombasthenia (GP11b/IIIa11b/IIIa
deficiency)deficiency)– Bernard Soulier (vWF receptor deficiency)Bernard Soulier (vWF receptor deficiency)
AcquiredAcquired– Drugs Drugs (ASA/NSAIDs, lasix, nitrofurantoin)(ASA/NSAIDs, lasix, nitrofurantoin)
– Renal diseaseRenal disease– Liver diseaseLiver disease

PLATELETS DISORDERS (cont.)PLATELETS DISORDERS (cont.)
Increased Platelet Destruction:Increased Platelet Destruction: Immunologic Immunologic – ITPITP– SLESLE– Isoimmunization Isoimmunization (post-transfusion, neonatal)(post-transfusion, neonatal)– Drug related Drug related (heparin, quinine, digoxin, sulphonamides, phenytoin)(heparin, quinine, digoxin, sulphonamides, phenytoin)
Infection – SepsisSepsis
Mechanical Mechanical – DIC DIC – HUS-TTPHUS-TTP– Giant hemangioma (Kasabach-Merritt)Giant hemangioma (Kasabach-Merritt)– BurnsBurns– TraumaTrauma

PLATELETS DISORDERS (cont.) PLATELETS DISORDERS (cont.)
Thrombocytopenia:Thrombocytopenia:
SequestrationSequestration– HypersplenismHypersplenism– Sickle cell anemiaSickle cell anemia
DilutionalDilutional– Massive transfusionMassive transfusion

VASCULAR DISORDERSVASCULAR DISORDERS
Loss of Vascular IntegrityLoss of Vascular Integrity:: Acquired: Acquired:
- Trauma/NAI, Scurvy, Steroid induced, Increased - Trauma/NAI, Scurvy, Steroid induced, Increased intravascular pressure (coughing, vomiting, straining). intravascular pressure (coughing, vomiting, straining). Congenital:Congenital:
- Disorders of connective tissue: Ehlers-Danlos - Disorders of connective tissue: Ehlers-Danlos syndrome, Osteogenesis imperfecta, Marfan’s.syndrome, Osteogenesis imperfecta, Marfan’s. - Disorders of blood vessels: Hemorrhagic telangiectasia- Disorders of blood vessels: Hemorrhagic telangiectasia

VASCULAR DISORDERS: VASCULAR DISORDERS: VasculitisVasculitisDrug-relatedDrug-relatedInfectionInfection– ViralViral
Coxsackie A9, B3Coxsackie A9, B3Echoviruses 4,9Echoviruses 4,9Atypical measlesAtypical measles
– BacterialBacterialMeningococcemiaMeningococcemiaStreptococcal pharyngitisStreptococcal pharyngitisSeptic emboliSeptic emboliSBESBEGonococcusGonococcus
– RickettsialRickettsialRocky Mountain spotted feverRocky Mountain spotted fever
Immune-mediatedImmune-mediated– HSPHSP– SLESLE– Serum sicknessSerum sickness– DysgammaglobulinemiaDysgammaglobulinemia

COAGULATION FACTOR COAGULATION FACTOR DISORDERSDISORDERS
Clotting factor deficienciesClotting factor deficienciesCongenitalCongenital
Von Willebrand’s diseaseVon Willebrand’s diseaseHemophiliasHemophilias
II, V, X or Fibrinogen deficiency.II, V, X or Fibrinogen deficiency.AcquiredAcquired
Vitamin K deficiencyVitamin K deficiencyLiver diseaseLiver diseaseMalabsorption Malabsorption Warfarin/superwarfarinWarfarin/superwarfarin
Toxin mediated: Coumadin containing rodenticides.Toxin mediated: Coumadin containing rodenticides.

LABSLABS
LFTs – Bilirubin 0.3 mg/dLLFTs – Bilirubin 0.3 mg/dL
Alk POAlk PO44 283 u/L (150-420 u/L) 283 u/L (150-420 u/L)
Aspartate aminotransferase 83 u/LAspartate aminotransferase 83 u/L (20-65 (20-65 u/L)u/L)
Protein 5.9 gm/dL (5.6 – 7.2 gm/dL)Protein 5.9 gm/dL (5.6 – 7.2 gm/dL)
Albumin 3.5 gm/dL (3.5 – 5.5 gm/dL)Albumin 3.5 gm/dL (3.5 – 5.5 gm/dL)

LABSLABS
WBC 9.0. Hb 13, Hct 48.2 Platelets 212. WBC 9.0. Hb 13, Hct 48.2 Platelets 212.
S 56, B 0, L 38, M 5, E 1S 56, B 0, L 38, M 5, E 1
UA UA Normal Normal
PT PT 59.1 (10-13 secs) 59.1 (10-13 secs)PTT PTT 120 secs (26 – 37 secs) 120 secs (26 – 37 secs)

GRAND ROUNDSGRAND ROUNDS
Februay, 2006Februay, 2006
Dr. Singh, N.Dr. Singh, N.
Dr. Manuel, S.Dr. Manuel, S.
Dr. Ingaramo, O.Dr. Ingaramo, O.

EVALUATIONS OF BLEEDING EVALUATIONS OF BLEEDING DISORDERSDISORDERS
Require a thorough history and physical Require a thorough history and physical exam. exam. Important questions include prolonged Important questions include prolonged bleeding following minor trauma, bleeding following minor trauma, spontaneous bruising, or hematoma spontaneous bruising, or hematoma formation. formation. Drug history is important since many drugs Drug history is important since many drugs cause bleeding. ie Aspirin. cause bleeding. ie Aspirin. Family history and any possible pattern of Family history and any possible pattern of inheritance. inheritance.

PHYSICAL EXAMPHYSICAL EXAM
Petechiae and purpura are signs of Petechiae and purpura are signs of platelet dysfunction. platelet dysfunction. Large firm bruises with nodular centers Large firm bruises with nodular centers are commonly seen in congenital factor are commonly seen in congenital factor deficiencies. deficiencies. Icterus and hepatosplenomegaly are Icterus and hepatosplenomegaly are indicative of liver disease, which may be indicative of liver disease, which may be associated with bleeding disordersassociated with bleeding disorders

CLASIFICATION OF BLEEDING CLASIFICATION OF BLEEDING DISORDERSDISORDERS
Defects of primary hemostasis (platelets, Defects of primary hemostasis (platelets, vessels, etc.).vessels, etc.).
Defects of secondary hemostasis Defects of secondary hemostasis (coagulation cascade and its regulation)(coagulation cascade and its regulation)

DEFECTS OF PRIMARY DEFECTS OF PRIMARY HEMOSTASISHEMOSTASIS
Vascular disorders:Vascular disorders: -Laboratory tests are characterized by a -Laboratory tests are characterized by a
prolonged bleeding time. prolonged bleeding time. Platelets Disorders:Platelets Disorders:
-Quantitative (thrombocytopenia).-Quantitative (thrombocytopenia). -Qualitative-Qualitative (poor platelet function): (poor platelet function):
Inherited aggregation defect, Drug effect. Inherited aggregation defect, Drug effect.

COAGULATION FACTORS COAGULATION FACTORS DISORDERSDISORDERS
Congenital factor deficiencyCongenital factor deficiency -Hemophilia A and B -Hemophilia A and B -Von Willebrand disease -Von Willebrand disease -Other factor deficiencies (rare) -Other factor deficiencies (rare) Acquired factor deficiencyAcquired factor deficiency -Vitamin K deficiency -Vitamin K deficiency -Liver failure-Liver failure -DIC-DIC -Drugs: Anticoagulants. -Drugs: Anticoagulants. Antiphospholipid antibodyAntiphospholipid antibody

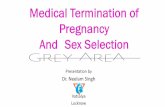
COAGULATION CASCADECOAGULATION CASCADE

LABORATORY OF BLEEDING LABORATORY OF BLEEDING DISORDERSDISORDERS
Most common ordered labs: Most common ordered labs:
Platelet count. Platelet count.
Bleeding time. Bleeding time.
PT: Extrinsic and common coagulation pathway.PT: Extrinsic and common coagulation pathway.
PTT: Intrinsec and common coagulation pathway. PTT: Intrinsec and common coagulation pathway.

LABORATORY OF BLEEDING LABORATORY OF BLEEDING DISORDERS (cont.)DISORDERS (cont.)
PTT mixing study: PTT corrects with factor PTT mixing study: PTT corrects with factor deficiency, but it does not normalize with circulating deficiency, but it does not normalize with circulating ab/anticoagulants. ab/anticoagulants. If positive, determine whether the inhibitor is a true If positive, determine whether the inhibitor is a true antibody to a coagulation protein or an antibody to a coagulation protein or an antiphospholipid ab.antiphospholipid ab.Thrombin time (TT) and reptilase time measure Thrombin time (TT) and reptilase time measure conversion of fibrinogen to fibrine and the formation conversion of fibrinogen to fibrine and the formation of the initial clot by thrombine. of the initial clot by thrombine. Ristocetin, vWF antigen, WF quantity, vWD Ristocetin, vWF antigen, WF quantity, vWD multimeric assay. multimeric assay.

LABORATORY OF BLEEDING LABORATORY OF BLEEDING DISORDERS (cont).DISORDERS (cont).
Assays for fibrinogen, platelet aggregation or Assays for fibrinogen, platelet aggregation or platelet function assay (e.g. PFA-100), factor platelet function assay (e.g. PFA-100), factor XIII, dysfibrinogenemia (thrombin time or XIII, dysfibrinogenemia (thrombin time or reptilase time)reptilase time)Also assays for factors VIII, IX or XI, even with Also assays for factors VIII, IX or XI, even with normal PTTnormal PTTMore esoteric assays include PAI-1 activity and More esoteric assays include PAI-1 activity and antiplasminantiplasmin

LABORATORY OF BLEEDING LABORATORY OF BLEEDING DISORDERS (cont).DISORDERS (cont).
PT is increased in factor deficiency (I, II, V, VII, PT is increased in factor deficiency (I, II, V, VII, X), liver failure, vitamin K deficiency, coumadin, X), liver failure, vitamin K deficiency, coumadin, warfarins. warfarins. aPTT is increased in factor deficiency (XII, XI, IX aPTT is increased in factor deficiency (XII, XI, IX and VIII), vWD, lupus anticoagulant and heparin and VIII), vWD, lupus anticoagulant and heparin tx. It is less sensitive than the PT to deficiencies tx. It is less sensitive than the PT to deficiencies within the common pathway (X, V, II and I). Not within the common pathway (X, V, II and I). Not affected by VII and XIII. affected by VII and XIII. TT is increased in fibrinogen problems and TT is increased in fibrinogen problems and heparin tx. Not affected by XIII. heparin tx. Not affected by XIII.

LABORATORY OF BLEEDING LABORATORY OF BLEEDING DISORDERS (cont).DISORDERS (cont).
Routine screening testing with the platelet count, PT, TT, Routine screening testing with the platelet count, PT, TT, aPTT should allow the clinician to more narrowly define aPTT should allow the clinician to more narrowly define the diagnostic possibilities.the diagnostic possibilities. Prolonged PT and aPTT:Prolonged PT and aPTT: In a bleeding child who is otherwise In a bleeding child who is otherwise wellwell indicates an indicates an inherited disorder within the common pathway (I, II, V, X) inherited disorder within the common pathway (I, II, V, X) or an acquired disorder involving multiple pathways or or an acquired disorder involving multiple pathways or anticoagulant factor. Other: Amyloidosis, coumadin. anticoagulant factor. Other: Amyloidosis, coumadin. In a In a sicksick child consider DIC, hepatocellular dysfunction, child consider DIC, hepatocellular dysfunction, severe vit K deficiency, thrombosis, hemangioma.severe vit K deficiency, thrombosis, hemangioma.Normal TT with normal fibrinogen level will exclude Normal TT with normal fibrinogen level will exclude abnormal fibrinogen.abnormal fibrinogen.

COAGULATION CASCADECOAGULATION CASCADE

DIFFERENTIAL DX IN DIFFERENTIAL DX IN PROLONGED PT AND PTTPROLONGED PT AND PTT
Factor X deficiency:Factor X deficiency: rare (1 per 1 million) rare (1 per 1 million) AR deficiency characterized by asymptomatic AR deficiency characterized by asymptomatic heterozygotes and by homozygotes with bleeding heterozygotes and by homozygotes with bleeding symptoms that correlate with factor activity. symptoms that correlate with factor activity. May be associated with bruising, epistaxis, May be associated with bruising, epistaxis, menorrhagia, GI/GU or umbilical stump bleeding or menorrhagia, GI/GU or umbilical stump bleeding or bleeding after surgery, trauma, dental procedures, bleeding after surgery, trauma, dental procedures, pregnancy or circumcisionpregnancy or circumcisionSevere deficiencies may resemble hemophilia and Severe deficiencies may resemble hemophilia and may be associated with intracranial hemorrhage.may be associated with intracranial hemorrhage.Treatment:Treatment: fresh frozen plasma; Prothrombin fresh frozen plasma; Prothrombin complex concentrates for serious bleedingcomplex concentrates for serious bleeding ..

COAGULATION CASCADECOAGULATION CASCADE

DIFFERENTIAL DX IN DIFFERENTIAL DX IN PROLONGED PT AND PTTPROLONGED PT AND PTT
Factor V deficiencyFactor V deficiency: rare (1 per 1 million) : rare (1 per 1 million) AR deficiency in which asymptomatic AR deficiency in which asymptomatic heterozygotes and homozygotes manifesting heterozygotes and homozygotes manifesting platelet-type bleeding (easy bruising, epistaxis). platelet-type bleeding (easy bruising, epistaxis). Severe deficiencies associated with intracranial Severe deficiencies associated with intracranial hemorrhage, although levels do not always hemorrhage, although levels do not always correlate with severity of symptomscorrelate with severity of symptomsTreatment:Treatment: 10-20 ml fresh frozen plasma/kg; 10-20 ml fresh frozen plasma/kg; commercial concentrates of factor V are not commercial concentrates of factor V are not availableavailable

COAGULATION CASCADECOAGULATION CASCADE

DIFFERENTIAL DX IN DIFFERENTIAL DX IN PROLONGED PT AND PTTPROLONGED PT AND PTT
Factor II deficiencyFactor II deficiency: rare (1 per 2 million) : rare (1 per 2 million) AR disorder associated with mucosal and deep AR disorder associated with mucosal and deep tissue bleeding. tissue bleeding. Treatment: 10-20 ml fresh frozen plasma/kg; Treatment: 10-20 ml fresh frozen plasma/kg; prothrombin complex concentrates may be prothrombin complex concentrates may be used for serious bleedingused for serious bleeding..

COAGULATION CASCADECOAGULATION CASCADE

DIFFERENTIAL DX IN DIFFERENTIAL DX IN PROLONGED PT AND PTTPROLONGED PT AND PTT
Factor I / fibrinogen deficiency or disordersFactor I / fibrinogen deficiency or disordersRareRare. . Autosomal inheritance; most mutations are Autosomal inheritance; most mutations are in alpha-fibrinogen chain gene, sparing beta and in alpha-fibrinogen chain gene, sparing beta and gamma chainsgamma chainsAfibrinogenemia:Afibrinogenemia: homozygous form; causes homozygous form; causes severe quantitative deficiency of fibrinogen and severe quantitative deficiency of fibrinogen and increased risk of bleeding; associated with increased risk of bleeding; associated with intracranial hemorrhages.intracranial hemorrhages.Hypofibrinogenemia: Hypofibrinogenemia: heterozygous form; heterozygous form; mild/moderate reductions in fibrinogen; little/no mild/moderate reductions in fibrinogen; little/no bleeding.bleeding.

DIFFERENTIAL DX IN DIFFERENTIAL DX IN PROLONGED PT AND PTTPROLONGED PT AND PTT
Dysfibrinogenemia:Dysfibrinogenemia: qualitative fibrinogen. qualitative fibrinogen.
Bleeding due to defective fibrin clot formation Bleeding due to defective fibrin clot formation (impaired release of fibrinopeptides A or B)(impaired release of fibrinopeptides A or B)Thrombosis due to (a) defective thrombin binding to Thrombosis due to (a) defective thrombin binding to fibrin, causing increased thrombin in circulation; (b) fibrin, causing increased thrombin in circulation; (b) defective binding of tPA or plasminogen to fibrin.defective binding of tPA or plasminogen to fibrin.Labs: cLabs: concentration determined by ELISA. Often oncentration determined by ELISA. Often prolonged TT and reptilase time, PT and PTTprolonged TT and reptilase time, PT and PTTTreatment:Treatment: cryoprecipitate; fresh frozen plasma cryoprecipitate; fresh frozen plasma contains more fibrinogen, but in a much larger volume.contains more fibrinogen, but in a much larger volume.

DIFFERENTIAL DX IN DIFFERENTIAL DX IN PROLONGED PT AND PTTPROLONGED PT AND PTT
Combined factor deficiencies are very rareCombined factor deficiencies are very rareCombined factor V and VIII:Combined factor V and VIII: autosomal autosomal recessive.recessive.Combined factors II, VII, IX and X deficiency:Combined factors II, VII, IX and X deficiency: due to mutation in gamma-glutamyl carboxylase due to mutation in gamma-glutamyl carboxylase gene, whose protein carboxylates glutamate gene, whose protein carboxylates glutamate residues in vitamin K-dependent coagulation residues in vitamin K-dependent coagulation factorsfactorsVery rare to have bleeding disorders due to Very rare to have bleeding disorders due to deficiency in PAI-1 or antiplasmindeficiency in PAI-1 or antiplasmin

DIFFERENTIAL DX IN PROLONGED DIFFERENTIAL DX IN PROLONGED PT AND PTTPT AND PTT
ACQUIRED DEFECTS OF SECONDARY ACQUIRED DEFECTS OF SECONDARY HEMOSTASIS: HEMOSTASIS:
Vitamin KVitamin K is needed for the synthesis of factors II, VII, is needed for the synthesis of factors II, VII, IX and X. IX and X.
Vitamin K is vital to the carboxylation of glutamic acid Vitamin K is vital to the carboxylation of glutamic acid residues which is needed for the activation of these residues which is needed for the activation of these factors. factors.
The most common circumstance in which vitamin K The most common circumstance in which vitamin K deficiency leads to bleeding is hemorrhagic disease of deficiency leads to bleeding is hemorrhagic disease of the newborn. the newborn.

ACQUIRED DEFECTS OF ACQUIRED DEFECTS OF SECONDARY HEMOSTASIS: SECONDARY HEMOSTASIS:
Vitamin KVitamin K (cont.) (cont.) Without vitamin K supplementation, significant Without vitamin K supplementation, significant GI and cutaneous hemorrhage may develop GI and cutaneous hemorrhage may develop within a few days. within a few days. After the newborn period, vitamin K is absorbed After the newborn period, vitamin K is absorbed from the GI tract. Deficiency may then result from the GI tract. Deficiency may then result from nutritional deficits, malabsorption, or from nutritional deficits, malabsorption, or alteration in intestinal flora. alteration in intestinal flora. Treatment must be directed at the underlying Treatment must be directed at the underlying disorder and vitamin K supplementation.disorder and vitamin K supplementation.

DIFFERENTIAL DX IN DIFFERENTIAL DX IN PROLONGED PT AND PTTPROLONGED PT AND PTT
ACQUIRED DEFECTS OF SECONDARY ACQUIRED DEFECTS OF SECONDARY
HEMOSTASIS (cont.)HEMOSTASIS (cont.)
Decreased synthesis of coagulation proteinsDecreased synthesis of coagulation proteins occurs in severe liver disease. occurs in severe liver disease.
Abnormalities in the liver's capacity to Abnormalities in the liver's capacity to synthesize one or more clotting factors may synthesize one or more clotting factors may result in problems with hemostasis. result in problems with hemostasis.
Treatment involves replacement of the Treatment involves replacement of the decreased factor(s) with fresh frozen plasma. decreased factor(s) with fresh frozen plasma.

DIFFERENTIAL DX IN PROLONGED DIFFERENTIAL DX IN PROLONGED PT AND PTTPT AND PTT
ACQUIRED DEFECTS OF SECONDARY ACQUIRED DEFECTS OF SECONDARY HEMOSTASISHEMOSTASIS (cont.): (cont.):
Acquired factor deficienciesAcquired factor deficiencies (due to liver (due to liver disease, DIC, lupus anticoagulants, disease, DIC, lupus anticoagulants, heparin, warfarin or other anticoagulants) heparin, warfarin or other anticoagulants) are more common than hereditary factor are more common than hereditary factor deficiencies, and should be ruled out first deficiencies, and should be ruled out first

ACQUIRED DEFECTS OF SECONDARY ACQUIRED DEFECTS OF SECONDARY HEMOSTASISHEMOSTASIS (cont.): (cont.):
Acquired inhibitorsAcquired inhibitors are antibodies that neutralize a are antibodies that neutralize a specific clotting factor's functionspecific clotting factor's functionThe most commonly inhibited factor in clinical The most commonly inhibited factor in clinical practice is factor VIII. practice is factor VIII. Autoantibodies to VIII:C are characteristically Autoantibodies to VIII:C are characteristically oligoclonal non-complement-fixing IgG. oligoclonal non-complement-fixing IgG. The incidence is 0.2 to 1 per million person-years The incidence is 0.2 to 1 per million person-years with a higher incidence in older age groups. with a higher incidence in older age groups. These cause a prolonged PTT which is not corrected These cause a prolonged PTT which is not corrected with 1:1 dilution with normal plasma. with 1:1 dilution with normal plasma.

Acquired inhibitors (cont.)Acquired inhibitors (cont.)
Lupus anticoagulant:Lupus anticoagulant:Antibodies against protein-phospholipid complexes. Antibodies against protein-phospholipid complexes. May interfere with assays for factors VIII, IX, XI and May interfere with assays for factors VIII, IX, XI and XII without causing a true decrease in factor levelsXII without causing a true decrease in factor levelsIn adults, it may be associated with spontaneous In adults, it may be associated with spontaneous abortion, and thromboembolism. In the pediatric abortion, and thromboembolism. In the pediatric population is transient with rare clinical sequelae. population is transient with rare clinical sequelae. Soft-tissue bleeding, gross hematuria, and Soft-tissue bleeding, gross hematuria, and postsurgical hemorrhage can occur; fatal bleeds may postsurgical hemorrhage can occur; fatal bleeds may occur in 15% of patients. occur in 15% of patients. The treatment is aimed at reducing the antibody titer The treatment is aimed at reducing the antibody titer using immunosuppression, IVIG, or Plasmapheresis.using immunosuppression, IVIG, or Plasmapheresis.

Acquired Defects of Secondary Acquired Defects of Secondary Hemostasis (cont.)Hemostasis (cont.)
Disseminated intravascular coagulation (DICDisseminated intravascular coagulation (DIC) ) Occurs in patients who are critically ill. Occurs in patients who are critically ill. Fever, hypotension, acidosis, oliguria, or Fever, hypotension, acidosis, oliguria, or hypoxia may be present. In addition, petechiae, hypoxia may be present. In addition, petechiae, purpura, and oozing from wounds and purpura, and oozing from wounds and venipuncture sites may develop. venipuncture sites may develop. Microvascular and large vessel thrombosis may Microvascular and large vessel thrombosis may occur. occur. The platelet count is typically decreased due to The platelet count is typically decreased due to consumption and platelet destruction.consumption and platelet destruction.

DIC (cont.)DIC (cont.)
The PT and PTT are prolonged from depletion of The PT and PTT are prolonged from depletion of factors V, VIII, IX, and XI. factors V, VIII, IX, and XI. Fibrinogen is decreased. Fibrin degradation Fibrinogen is decreased. Fibrin degradation products and the D-dimer assay are increased. products and the D-dimer assay are increased. The mainstay of therapy is to treat the The mainstay of therapy is to treat the underlying disease. underlying disease. Additional therapy consists of replacing clotting Additional therapy consists of replacing clotting factors and platelets and possibly the use of factors and platelets and possibly the use of heparin and antifibrinolytic agents. heparin and antifibrinolytic agents.

Other Acquired Defects of Other Acquired Defects of Secondary HemostasisSecondary Hemostasis
Amyloidosis:Amyloidosis:
Primary amyloidosis may cause Primary amyloidosis may cause acquired factor X deficiency due to the acquired factor X deficiency due to the binding of amyloid to factor X.binding of amyloid to factor X.
Also inhibits fibrinogen conversion to Also inhibits fibrinogen conversion to fibrin, causing prolongation of thrombin fibrin, causing prolongation of thrombin time and reptilase time.time and reptilase time.

SUMMARYSUMMARY
Possible diagnosis in this patient with Possible diagnosis in this patient with prolonged PT and PTT:prolonged PT and PTT:
Hereditary factor deficiency: I, II, V, X, Hereditary factor deficiency: I, II, V, X, antiplasmin and dysfibrinogenemia.antiplasmin and dysfibrinogenemia.
Acquired defects of hemostasis: Vit K Acquired defects of hemostasis: Vit K deficiency, liver disease, lupus anticoagulant, deficiency, liver disease, lupus anticoagulant, anticoagulant drugs, DIC, amyloidosis.anticoagulant drugs, DIC, amyloidosis.
Child abuse can be a concomitant dx.Child abuse can be a concomitant dx.

Thank you.Thank you.