Global Trachoma Mapping Project EMR Alliance Meeting Alliance Meeting 26th April... · Global...
38
Global Trachoma Mapping Project EMR Alliance Meeting 26th April 2014
Transcript of Global Trachoma Mapping Project EMR Alliance Meeting Alliance Meeting 26th April... · Global...

Global Trachoma
Mapping Project
EMR Alliance Meeting 26th April 2014

•© Sightsavers
Agenda
• Background on the grant
• Progress to date
• How it works (design, methodologies, systems, training etc.)
• Links to drug applications and Trachoma Action Plans
• Process for engagement and getting started
• How do you plan for country based mapping?

Background on the grant
Global Trachoma Mapping Project – the beginning of the end for trachoma
• There is an international commitment to eliminate trachoma by 2020 in line with
the target set by the World Health Assembly. Determining where trachoma is
prevalent by mapping the disease is a critical first stage.
• Historically trachoma mapping has been under-resourced and in the 12 years
before GTMP started, 1,115 districts were mapped with 559 confirmed as
endemic.
• GTMP has set out to map trachoma (as well as other NTD & WaSH data where
possible) in the estimated remaining 1,238 endemic districts, in over 30 countries
by March 2015, in only 2.5 years.
• Mapping must be completed to enable country programmes to undertake
development of action plans, request and distribute donated antibiotics, and
implement the full SAFE strategy over a period of between 3 to 5 years.
•© Sightsavers
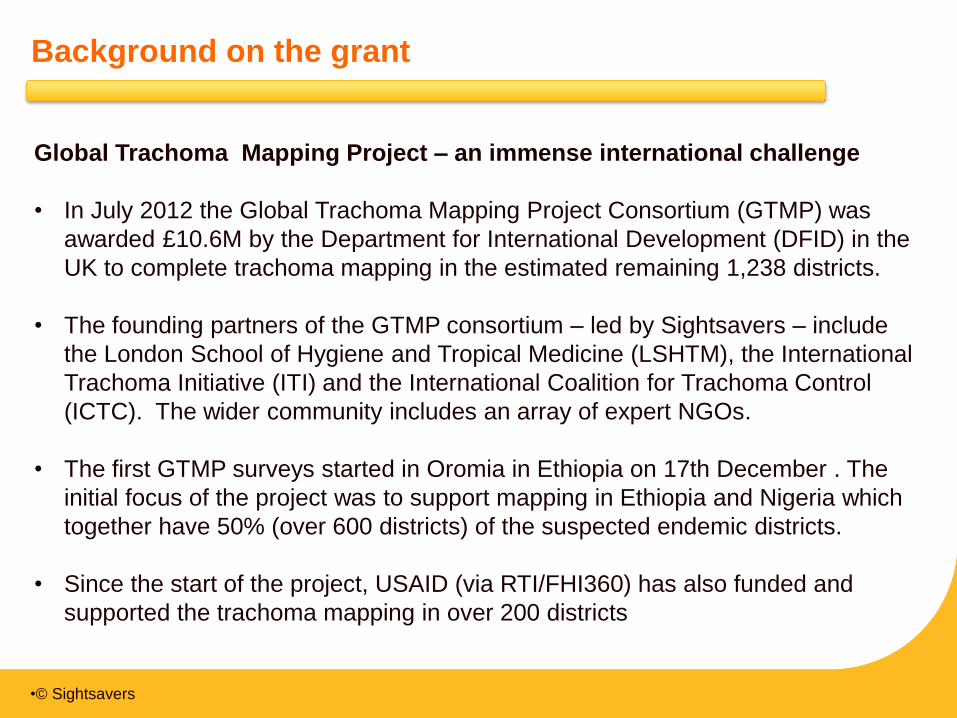
Background on the grant
Global Trachoma Mapping Project – an immense international challenge
• In July 2012 the Global Trachoma Mapping Project Consortium (GTMP) was
awarded £10.6M by the Department for International Development (DFID) in the
UK to complete trachoma mapping in the estimated remaining 1,238 districts.
• The founding partners of the GTMP consortium – led by Sightsavers – include
the London School of Hygiene and Tropical Medicine (LSHTM), the International
Trachoma Initiative (ITI) and the International Coalition for Trachoma Control
(ICTC). The wider community includes an array of expert NGOs.
• The first GTMP surveys started in Oromia in Ethiopia on 17th December . The
initial focus of the project was to support mapping in Ethiopia and Nigeria which
together have 50% (over 600 districts) of the suspected endemic districts.
• Since the start of the project, USAID (via RTI/FHI360) has also funded and
supported the trachoma mapping in over 200 districts

•© Sightsavers
• By developing standard methodologies,
protocols and materials and providing expert
assistance to Ministries of Health, this
collaboration enables the GTMP to meet its
key objective:
• supporting countries to quickly
scale-up their trachoma mapping
plans while maintaining quality in
delivery to support this step towards
global elimination.
• Since the start of the project, the scope has
increased and the estimated number of
districts to be mapped is currently in excess
of 1,800 districts (50% increase)
Background on the grant
• All mapping data collected is owned by the national governments and is uploaded to
the Trachoma Atlas - http://http://www.trachomaatlas.org/.
Global Trachoma Mapping Project – an immense international challenge
•© Sightsavers
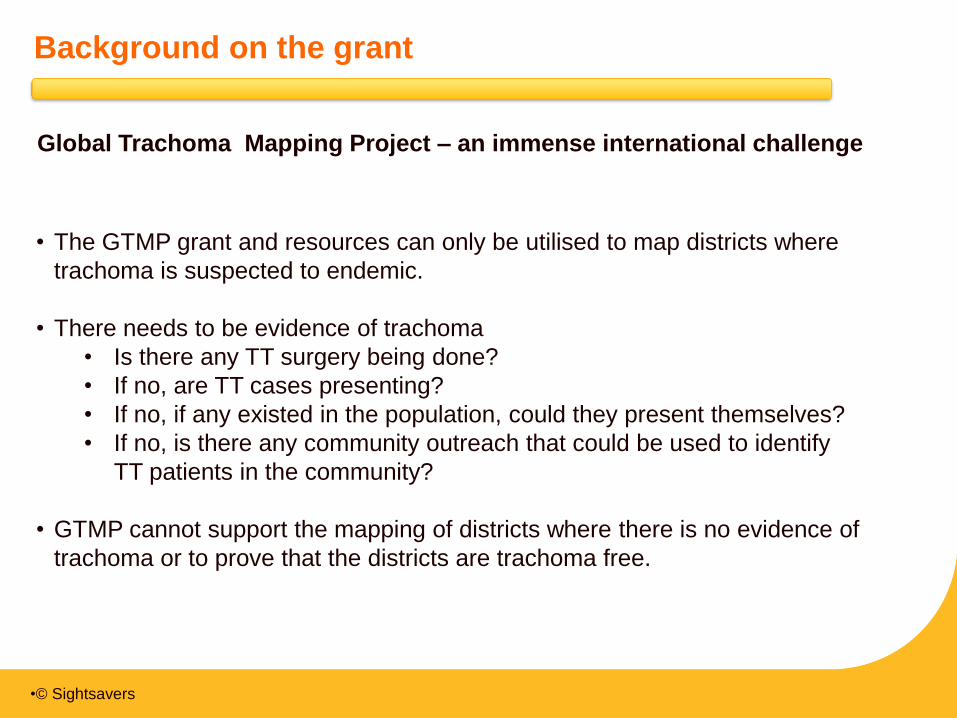
• The GTMP grant and resources can only be utilised to map districts where
trachoma is suspected to endemic.
• There needs to be evidence of trachoma
• Is there any TT surgery being done?
• If no, are TT cases presenting?
• If no, if any existed in the population, could they present themselves?
• If no, is there any community outreach that could be used to identify
TT patients in the community?
• GTMP cannot support the mapping of districts where there is no evidence of
trachoma or to prove that the districts are trachoma free.
Background on the grant
Global Trachoma Mapping Project – an immense international challenge

•© Sightsavers
Background on the grant
Trachoma Atlas – Africa & Middle East

•© Sightsavers
Agenda
• Background on the grant
• Progress to date
• How it works (design, methodologies, systems, training etc.)
• Links to drug applications and Trachoma Action Plans
• Process for engagement and getting started
• How do you plan for country based mapping?

•© Sightsavers
Progress to date
• 1,033 districts have completed mapping
(83% of original target: 1,238)
• 96% of districts have been mapped using
GTMP methodology (987 districts)
• 16 countries have now completed mapping
or are currently conducting mapping
• The total population in all districts mapped is
1.3 million people
• Over 26 million data items have been
processed
• GTMP is currently working with 19 different
implementing organisations
• GTMP has delivered nearly half of all the
trachoma surveys that have ever been
conducted (48%)
Total number of districts mapped for trachoma:
23rd July 2012 to 23rd April 2014 inclusive
763 Districts Mapped with DFID Funding
and GTMP Methods
74%
5 Districts Mapped with DFID Funding
and Other Methods
0%
224 Districts Mapped with Other Funding
and GTMP Methods
22%
41 Districts Mapped with Other Funding
and Other Methods
4%

•© Sightsavers
Progress to date – GTMP progress as of April 2014

•© Sightsavers
Progress to date
Progress in EMR Region
Countries which
are trained and
mapping
Countries in
planning stages
Discussions /
on-going
Mapping on
hold due to
security
concerns
• Sudan (45
districts: $600k)
• Yemen (phase 1,
83 districts :
$150K, phase 2,
128 districts
$280K)
• Egypt (phase 1,
12 districts: $36K
estimated total
districts 60-80)
• Afghanistan (estimated
36 districts: $540K)
• Pakistan (estimated 72
districts: $360K)
• Somalia (estimated 12
districts: $60K)
• Djibouti (estimated 2
districts: $10K)
• Sudan (19 districts
on hold)
• Yemen (1 EU on
hold)

•© Sightsavers
Progress to date
Status
• Sudan: Training held on the 6th April 2014. Planning completed. Ethics and data
management agreed. Contract formalisation and agreements in final stages.
Mapping to commence in a few weeks time. (20 clusters per EU, 28 EUs,12 teams:
x1 Recorder x1 Grader)
• With thanks to: Dr. Awad, Dr. Balgesa Elkheir Elshafie, Dr Kamal Hashim
• Egypt: Training to be held on the 11th May 2014. Planning completed for phase 1.
Ethics and data management agreed. Contract formalisation and agreements in
final stages. Mapping to commence in a few weeks. (22 clusters per EU, 4
Governorates: 3 districts each (12 EUs),12 teams: x1 Recorder x1 Grader)
• With thanks to: Dr. Khaled, Dr. Gamal, Dr. Islam el Beih, Dr. Ahmed Khairy
• Yemen: Mapping for phase 1 completed (one EU on hold because of security
concerns). Phase 2 budgets in review. Mapping to commence once budgets for
phase 2 are finalised.
• With thanks to: Tawfik Al-Khatib, Ahmed Al-Soofi, Fouad Al-Bahm

•© Sightsavers
Agenda
• Background on the grant
• Progress to date
• How it works (design, methodologies, systems, training etc.)
• Links to drug applications and Trachoma Action Plans
• Process for engagement and getting started
• How do you plan for country based mapping?

•© Sightsavers
How it works
Approach to mapping:
Collaboration
Programme engages with, and is supported by, the expert trachoma community
(currently working with 19 different organisations)
Standardisation
Standard methodologies and training materials are used, based on WHO protocols
Training
Extensive in-country training workshops – including training of trainers, training and
testing of Supervisors, Graders and Recorders
New technology
Smartphones are used to capture data, all data/results are approved by MoHs
electronically. Web-enabled financial claims and reporting systems support robust
reviews of budgets, claims and reporting.
Implementation
MoH manage and deliver mapping supported by NGOs, NGOs sign agreements and
submit financial claims on a quarterly basis
•© Sightsavers
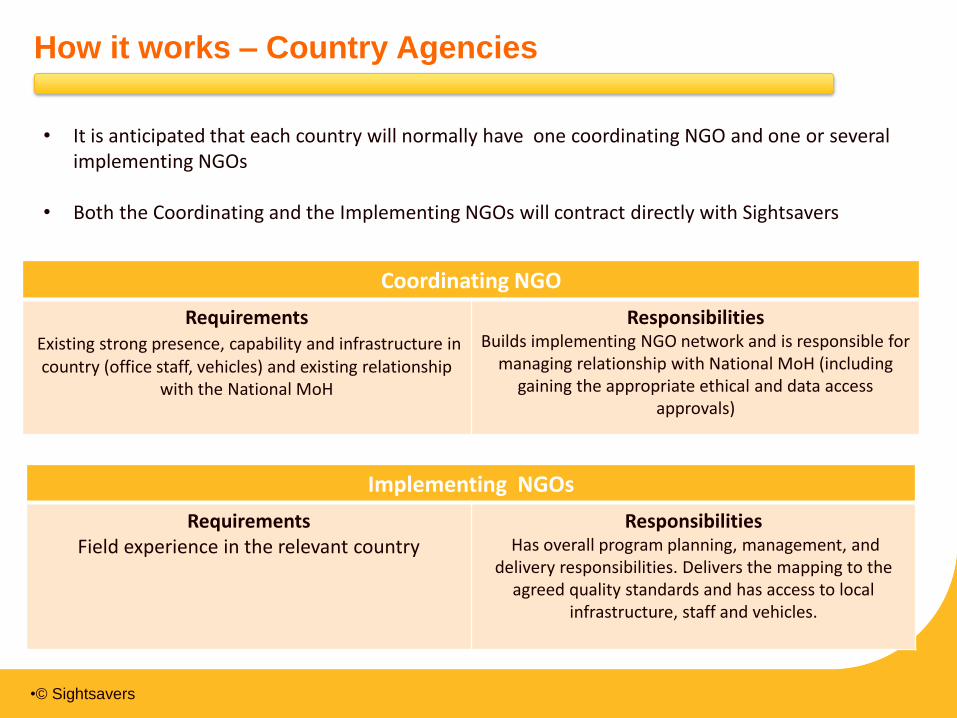
How it works – Country Agencies
• It is anticipated that each country will normally have one coordinating NGO and one or several implementing NGOs
• Both the Coordinating and the Implementing NGOs will contract directly with Sightsavers
Implementing NGOs
Requirements Field experience in the relevant country
Responsibilities Has overall program planning, management, and
delivery responsibilities. Delivers the mapping to the agreed quality standards and has access to local
infrastructure, staff and vehicles.
Coordinating NGO
Requirements Existing strong presence, capability and infrastructure in
country (office staff, vehicles) and existing relationship with the National MoH
Responsibilities Builds implementing NGO network and is responsible for
managing relationship with National MoH (including gaining the appropriate ethical and data access
approvals)

•© Sightsavers
How it works - Training & methodology
• The number of graders/recorders you train
depends on the number of EUs to be
mapped and your timescale for completion.
• One GTMP mapping team will normally be
composed of: 1 grader, 1 recorder and 1
community guide (as well as one driver).
• It normally takes 1 day to map 1 cluster.
• There are generally 20-30 clusters in an EU.
Therefore 1 GTMP mapping team will
normally map 1 EU in a month.
• There is usually a MoH Supervisor who will
supervise and support between 7 and 10
GTMP mapping teams.

•© Sightsavers
How it works – Utilising new technology: Data
“Ensure that each country’s data sovereignty and security rights are upheld”
• Data are owned by the government
• Data are stored securely and must be accessible
• Access to data is determined by each the national government
• Both the raw data and results are approved and released by the national government
• The MoH will publish the results in a peer-reviewed journal
“DFID grant requirements”
• The national government will grant DFID and the Project Partners a royalty-free and
global licence to use the data for non-commercial use, for the purposes of research
and teaching into, and prevention, treatment and eradication of, trachoma and other
neglected tropical diseases.
• The summary data is made publically available on the Trachoma Atlas that is managed
by the International Trachoma Initiative (ITI)
• In line with academic best practise, the detailed, anonymised dataset should be made
available for the purpose of research and teaching, at least 12 months after initial
government approval and only after primary publication

•© Sightsavers
How it works – Utilising new technology: Ownership
“Data are owned by the government”
To avoid a situation in which multiple data storage and processing solutions have
to be quickly created in each country and then, as required by the grant
agreement, uploaded into the Trachoma Atlas; the GTMP has developed an
innovative system to support data processing and storage and protect the rights
of national governments.
• Data are owned by the government
The government is protected by legal agreements with all the project partners
• The MoH will publish the results in a peer-reviewed journal
The government is protected by legal agreements with all the project partners
and the GTMP will support a first MoH author(s) to prepare a manuscript for
publication in a peer-reviewed journal.

•© Sightsavers
How it works – Utilising new technology: Process
The system has the capability to process and manage large volumes of data
approx. 26 million items in the first 15 months
• Data are stored securely and must be accessible
The data is encrypted and securely uploaded to the database
Data can be stored in-country but will also be stored in a “world-class” data management services
provider, maximising uptime, data-security and accessibility
• Access to data is determined by each the national government
ITI (not NGOs, donors or academic institutions) will support the national governments by providing
stewardship of the data and systems. Access to data will be determined by explicit written agreements
between the national governments and ITI
• Both the raw data and results are approved and released by the national government
There is a fully transparent cleaning process undertaken in communication with field supervisors.
The raw data and the analyses of the data are approved and released by the national government
The MoH can access, run reports, download and transfer the data at any stage
• Capacity building
The MoH data collectors (recorders), MOH Data Managers, MOH Epidemiologist and MOH Permanent
Secretary (or designate) will be supported with training to collect, access, analyse, approve and
download / transfer the data.

•© Sightsavers
How it works - New technology
Mapping data is available on the Trachoma Atlas as early as two weeks after the survey
Collection by smartphone
Standard surveys (incl WASH)
GPS coordinates
Dynamic/regular uploads
Ownership & access
Data sovereignty and security is key
Data available to be viewed online
Data can be downloaded
Data cleansing & Approval
Data reviewed daily by data manager
& by Chief Scientist
Both data and results are electronically
reviewed and approved by MoH
Reports available for implementation
planning and drug applications

•© Sightsavers
How it works
Online CLAIMS system facilitates reporting and provides an
easy to use template

•© Sightsavers
Agenda
• Background on the grant
• Progress to date
• How it works (design, methodologies, systems, training etc.)
• Links to drug applications and Trachoma Action Plans
• Process for engagement and getting started
• How do you plan for country based mapping?

•© Sightsavers
Drug Applications & Trachoma Action Plans
• ITI manage the relationship with the drug company Pfizer Inc.
• Pfizer donate the drug Zithromax to support trachoma elimination in line with the WHOs
SAFE strategy.
• ITI has instituted an annual application process for new country applications as well as
countries applying for additional rounds of Zithromax treatments. This process is
designed to assess a country’s Zithromax need over a five year horizon.
• The application requests information on up-to-date treatment distribution data, in-country
inventory and an update on prevalence data. The data collected in this process allows ITI
to determine the long term Zithromax needs in a particular Country, as well as evaluate
the progress towards the elimination of blinding trachoma.
• Zithromax donations are only approved when given in the context of the full SAFE
strategy.
• Trachoma Action Plans are created once survey data is finalised. (More on this later)
The ITI Trachoma Expert Committee (TEC) endorses the systems of the GTMP
as the gold standard method for applying WHO methodologies to produce
baseline trachoma data.

•© Sightsavers
Agenda
• Background on the grant
• Progress to date
• How it works (design, methodologies, systems, training etc.)
• Links to drug applications and Trachoma Action Plans
• Process for engagement and getting started
• How do you plan for country based mapping

•© Sightsavers
Process for engagement and getting started
Process for engagement
Building relationships and agreement • Identify the key partners who will be involved in the trachoma baseline surveys: MoH, ophthalmic
advisors, national and regional INGOs
• Make contact with GTMP to request technical and planning assistance to establish the evidence
base and proposed scope (districts) of work for the trachoma baseline surveys
• Hold a co-ordinating meeting with all stakeholders to further refine and agree the proposed scope of
work and to propose the mapping methodology, plan of action and high level budget – capture
decisions in the protocol (a word document) (GTMP are able to facilitate or advise the co-ordination
meeting if helpful)
• Submit the proposal in the form of a protocol to GTMP’s Chief Scientist Dr. Solomon and request a
formal review and agreement of the mapping methodology
Formalising mapping activities and gaining approvals • Once the protocol has been agreed by both the Ministry of Health and GTMP detailed budgets can
be submitted to GTMP for review and agreement
• After which a contract will be established between the Co-ordinating Agency and GTMP to continue
engagement and co-ordination between all stakeholders during the mapping project
• A contract will also be established between each Implementation Agency and GTMP to oversee the
delivery of the baseline mapping (this will document the number of districts and the total budget)
• The Ministry of Health are asked to provide a formal letter which stipulates that GTMP and
associated stakeholder partners are granted ethical agreement to conduct the surveys and data
access approval to upload the prevalence data onto the Trachoma Atlas website.
1
2

•© Sightsavers
Process for engagement and getting started
Getting started and running the project
Training • The Implementation Agency and the Ministry of Health identify potential trainers, and share the listing
with GTMP
• The Implementation Agency and the Ministry of Health hold the training workshop in collaboration with
GTMP training methods (classroom and field)
• GTMP provide certified grader and recorder trainers, loupes, androids and manuals (as required)
• Implementation agencies will be asked to provide EU names and the name of a Ministry of Health data
manager and Ministry of Health data approver to GTMP to enable data processing
Mapping • Smartphones can be tested during training to ensure they are operational for the mapping
• Also whilst training there is time to refine plans and to ensure all resources, vehicles and equipment
are in place for the mapping
• Conduct trachoma baseline surveys, record and send data on a regular basis
• ITI are available to answer any queries or questions that may occur regarding data capture and review
• Once the Ministry of Health has approved the data it is validated by GTMP and uploaded onto
trachoma atlas
• On conclusion of all baseline mapping activities a meeting can be held to discuss the outputs of the
survey and to update the Trachoma Action Plan
Reporting • A quarterly progress report and expenditure claim is submitted to GTMP within 10 working days of the
quarter end. Funds will be reimbursed within 30 days after submission of the claim
3
4
5

•© Sightsavers
Process for engagement and getting started
Check list
• Protocol and methodology ………………
• Ethical agreement and data access agreement letter ……………...
• Time line and plan ………………
• Budgets agreed ………………
• Trainers identified and support materials requested ………………
• What do you need to do next?
Date for completion/
people to contact
•© Sightsavers
Agenda
• Background on the grant
• Progress to date
• How it works (design, methodologies, systems, training etc.)
• Links to drug applications and Trachoma Action Plans
• Process for engagement and getting started
• How do you plan for country based mapping?
•© Sightsavers
How do you plan for country based mapping?
• After lunch we will be holding a workshop to talk you through the first steps to establish
a plan and proposal for country based mapping
• We will provide:
• A sample protocol
• A planning tool
• A draft ethics and data management agreement letter
• An implementer agreement template
• Budget templates
• Considerations to include:
• Methodology – number of clusters etc
• Cultural and religious sensitivities
• Timeframe
• Stakeholders
• Security
• People to own the process and champion the work
• End date for grant
• Copies of the training manual and surveys on the android telephones are available to
view
•© Sightsavers
Benefits of using GTMP processes and systems
• Funding and expert resources and systems to support countries to quickly
scale-up trachoma mapping plans while maintaining high quality
• Data is owned by the national government
• Use of, and access to, data is controlled by MoH
• GTMP systems and processes are proven and cost efficient
• GTMP methodologies and systems are endorsed as gold standard by the ITI
Expert Committee and will help ensure that the quality standard of the
mapping is acceptable for drug applications to Pfizer.
• The extensive training and use of new technologies will provide an opportunity
for countries to adapt these new processes to support the mapping and
intervention activities of all NTDs.
•© Sightsavers
Contacts
Dr Anthony Solomon (Chief Scientist GTMP): Contact if you have questions over project
methodology and protocol. [email protected]
Dr Paul Courtright (GTMP Technical Advisor): Advice on country set up and training support
Eleanor Challenger (Project Administrator, GTMP, LSHTM): Contact for training and general
requirements. Please copy in to all training correspondence. [email protected]
0044 (0) 207 927 2847
Tom Millar (Operations Director, NTDs, Sightsavers): Contact if you have any general
questions regarding the project or getting started. [email protected]
Siobhain McCullagh (GTMP Operations Director at Sightsavers) Overall project management
for the GTMP. [email protected] +44 (0) 1444 446771
Sarah Bovill (Risk and Finance Manager at Sightsavers) Contact for budgeting, finance &
CLAIMS. [email protected] +44 (0) 1444 446665
Cristina Jimenez (NTD co-ordinator at Sightsavers) Contact for travel and visa arrangements.
Please copy in to all travel/visa correspondence.
[email protected] +44 (0) 1444 446715

•© Sightsavers
Thank you!
Any questions?

•© Sightsavers
Workshop 1: Trachoma Mapping
• Over the next 3 hours we will help you to develop a protocol which will form the
basis of your Trachoma mapping proposal.
• We will explain the different stages, and ask you to work in your groups to
review:
• Choice of mapping areas
• Mapping methodology
• Timeline for activities
- If you already have completed your protocol please start to work on your
budgets with assistance from Siobhain McCullagh and Tom Millar (GTMP)
Please form groups to work through the
Trachoma mapping proposal activities

•© Sightsavers
Workshop 1: Trachoma Mapping
How do you choose the mapping areas?
• Is there any TT surgery being done?
• If no, are TT cases presenting?
• If no, if any existed in the population, could they present themselves?
• If no, is there any community outreach that could be used to identify TT patients in
the community?
• For the actual prioritising of countries local stakeholders (MoH, INGOs) should be
consulted
• An area will only be mapped if there is some evidence that there is trachoma
• The status of countries with regards to trachoma is listed on the WHO webpage under
http://apps.who.int/neglected_diseases/ntddata/trachoma/trachoma.html. However, this can be taken as
a first indication only, as even countries that are not listed to be endemic might have some pocket areas
of trachoma within their country.

•© Sightsavers
Workshop 1: Trachoma Mapping
How do you establish the mapping methodology ?
• One area to be mapped at a given time consists of 150.000 to 250.000 persons, the
“mapping population”. For TF 1019 children aged between none and nine are examined,
while the number of TT patients can be estimated from the TF figure.
• The number of 1-9 year old children expected to be seen in one area are based on the
census data, which then indicates the number of clusters needed to get sufficient data. The
selection of villages to include in a cluster depends very much of the population of a village,
which has to be representative for the total population in the area. However, refugees are to
be treated as a different part of the population. As a general rule at least 20 clusters should
be included in one survey. Due to the GPS technique the number and location of
households included in the survey can easily be monitored. In countries with a very high
percentage of children attending schools (> 95%) it could also be considered to screen
schools, however this in not likely to be the case in most countries.
• In areas where the security situation doesn’t allow the filed team to go from house to house,
any mapping procedure isn’t possible as the welfare of the team has absolute priority.
Moreover, any implementation might then be even more risky.
Statistical figure as stated by Anthony Solomon during the ERM Trachoma Alliance Inaugural
Meeting, 15-16 December 2013, Dubai

•© Sightsavers
Workshop 1: Trachoma Mapping
1. Acronyms
2. Introduction
• Background
• Country Profile
• Justification
3. Aim and Objectives
• Aim
• General objective
• Specific objectives
4. Methodology
• Study design
• Target population
• Sample Size
• Sample size
determination
• Sampling plan
• Survey Teams
• Data Management
Collection
• Data Ownership
• Data
collection/Questionn
aire administration
• Examination
methods
• Trachoma surgery
• Materials
5. Work plan
6. Distribution of GTMP Survey
sample size
7. Budget
8. Planning Outline
9. References
10. Annexes
How is a protocol structured?
•© Sightsavers
Workshop 1: Trachoma Mapping
Guidelines for breakout work
Activity 1: In your group, please consider and record the information which build the content of your protocol
against the headings provided.
• Considerations to include:
• Methodology – number of clusters etc
• Cultural and religious sensitivities
• Timeframe
• Stakeholders
• Security
• People to own the process and champion the work
• End date for grant
Activity 2: Please also record your timeline to:
• finalise the protocol,
• agree the ethical and data management with the MoH,
• arrange and hold training, and
• conduct the baseline survey mapping
• GTMP team members will rotate through the groups to help
• We will take 20 minutes to wrap up at the end of the working session
• Are there any questions before we begin?
• Note – tea and coffee will be served between 15.30 and 15.45

•© Sightsavers
Workshop 1: Trachoma Mapping
• What challenges did you face?
• Do you have any additional questions?
• What dependencies or outstanding activities remain?
Review