"Global Aging: The Challenge of Success" · PDF fileSocial Theories of Aging ... Aging’s...
44
CELEBRATING 75 YEARS • 1929-2004 Vol. 60, No. 1 A publication of the Population Reference Bureau B ULLETIN ULLETIN Population March 2005 Global Aging: The Challenge of Success By Kevin Kinsella and David R. Phillips Population aging is a human success story. Widespread fertility decline is accelerating population aging. Policies on aging need to address the entire society.
Transcript of "Global Aging: The Challenge of Success" · PDF fileSocial Theories of Aging ... Aging’s...

C E L E B R A T I N G 7 5 Y E A R S • 1 9 2 9 - 2 0 0 4POPULATION REFERENCE BUREAU
Vol. 60, No. 1 A publication of the Population Reference Bureau
BBULLETINULLETINPopulation March 2005
Global Aging: The Challenge of SuccessBy Kevin Kinsella and David R. Phillips
Population aging is a human success story.
Widespread fertility decline is accelerating population aging.
Policies on aging need toaddress the entire society.

Population Reference Bureau (PRB)Founded in 1929, the Population Reference Bureau is the leader in providing timely andobjective information on U.S. and international population trends and their implications.PRB informs policymakers, educators, the media, and concerned citizens working in the public interest around the world through a broad range of activities, including publications,information services, seminars and workshops, and technical support. Our efforts are sup-ported by government contracts, foundation grants, individual and corporate contributions,and the sale of publications. PRB is governed by a Board of Trustees representing diversecommunity and professional interests.
OfficersDouglas Richardson, Chair of the Board,
Executive Director, Association of American Geographers, Washington, D.C.Terry D. Peigh, Vice Chair of the Board
Executive Vice President and Director of Corporate Operations, Foote, Cone & Belding, Chicago, IllinoisWilliam P. Butz, President and Chief Executive Officer,
Population Reference Bureau, Washington, D.C.Michael P. Bentzen, Secretary of the Board,
Partner, Hughes and Bentzen, PLLC, Washington, D.C.Richard F. Hokenson, Treasurer of the Board,
Director, Hokenson and Company, Lawrenceville, New Jersey
TrusteesPatty Perkins Andringa, Consultant and Facilitator, Bethesda, MarylandJoel E. Cohen, Abby Rockefeller Mauzé Professor of Populations, Rockefeller University and Head,
Laboratory of Populations, Rockefeller and Columbia Universities, New YorkBert T. Edwards, Executive Director, Office of Historical Trust Accounting, Office of the Secretary,
U.S. Department of the Interior, Washington, D.C.Wray Herbert, Assistant Managing Editor, U.S. News & World Report, Washington, D.C.James H. Johnson Jr., William Rand Kenan Jr. Distinguished Professor and Director,
Urban Investment Strategies Center, University of North Carolina, Chapel HillWolfgang Lutz, Leader, World Population Project, International Institute for Applied Systems Analysis
and Director, Vienna Institute of Demography of the Austrian Academy of Sciences, Vienna, Austria. Elizabeth Maguire, President and Chief Executive Officer, Ipas, Chapel Hill, North CarolinaFaith Mitchell, Deputy Director, Division of Behavioral and Social Sciences and Education,
National Research Council/National Academy of Sciences, Washington D.C.Gary B. Schermerhorn, Managing Director of Technology, Goldman, Sachs & Company, New YorkBarbara Boyle Torrey, Independent Writer and Consultant, Washington, D.C.Leela Visaria, Professor, Gujarat Institute of Development Research, Ahmedabad, IndiaMontague Yudelman, Senior Fellow, World Wildlife Fund, Washington, D.C.
Editor: Mary Mederios KentProduction/Design: Michelle Nigh, Jon Howard
The Population Bulletin is published four times a year and distributed to members of the Population Reference Bureau. Population Bulletins are also available for $7 (discounts for bulkorders). To become a Friend of PRB or to order PRB materials, contact PRB, 1875 ConnecticutAve., NW, Suite 520, Washington, DC 20009-5728; Tel.: 800-877-9881; Fax: 202-328-3937; E-mail: [email protected]; Website: www.prb.org.
The suggested citation, if you quote from this publication, is: Kevin Kinsella and David R.Phillips, “Global Aging: The Challenge of Success,” Population Bulletin 60, no. 1 (Washington, DC:Population Reference Bureau, 2005). For permission to reproduce portions from the PopulationBulletin, write to PRB, Attn: Permissions, or [email protected].
© 2005 by the Population Reference BureauISSN 0032-468X
Printed on recycled paper

3
Vol. 60, No. 1 A publication of the Population Reference Bureau
BBULLETINULLETINPopulation March 2005
Global Aging:The Challenge of SuccessIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
Who Is Old? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
The Global Process of Aging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Figure 1. The World’s 20 ‘Oldest’ Countries and the United States, 2004 . . . 5Table 1. Percent of Population in Older Ages by Region,
2000, 2015, and 2030 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Box 1. How Useful Are Elderly Support Ratios? . . . . . . . . . . . . . . . . . . . . . . . . 7
The Demographic Drivers of Aging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Table 2. Life Expectancy at Birth in Years, Selected Countries,
1900, 1950, and 2003 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Figure 2. Population Age-Sex Structure in Less Developed and
More Developed Countries, 1950, 1990, and 2030 . . . . . . . . . . . . . . . . . . 12
Emergent Diversity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Figure 3. Speed of Population Aging in Selected Countries . . . . . . . . . . . . . 13Box 2. Aging and Depopulation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Health Transitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16Figure 4. Stylized Wild and Modern Survival Curves . . . . . . . . . . . . . . . . . . . 17Figure 5. Progression of Disability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Box 3. The Challenge of Alzheimer’s Disease and Other Dementias . . . . . . 19Table 3. Ten Leading Sources of the Global Burden of Disease,
1990 and 2020 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20Box 4. The Impact of HIV/AIDS on Older People in the Less
Developed World: African and Asian Examples . . . . . . . . . . . . . . . . . . . . 21
Gender and Aging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Table 4. Sex Ratio for People Age 65 or Older in 20 Countries, 2004 . . . . . 22Figure 6. Percent Widowed Among Older Australians, Malaysians,
and Croatians, Circa 2000 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Intergenerational Relationships . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Figure 7. Older Canadians Living Alone, 1961 to 2001 . . . . . . . . . . . . . . . . . . 27Figure 8. Living Arrangements of Older Japanese, 1960 to 2010 . . . . . . . . . . 27
Work, Retirement, and Well-Being . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28Box 5. The Transition to Retirement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30Box 6. Social Theories of Aging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33Figure 9. Model of Successful Aging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
Continued on page 2Population Bulletin Vol. 60, No. 1 2005www.prb.org

4
About the Authors
Kevin Kinsella is a special assistant with the U.S. Census Bureau’s International ProgramsCenter (IPC). In addition, he is assisting the Behavioral and Social Research Program,National Institute on Aging, with a report on the U.S. Health and Retirement Study. In 2001,he completed a two-year assignment with the Committee on Population of the National Academyof Sciences, where he directed two studies resulting in two 2001 publications, Preparing for AnAging World: The Case for Cross-National Research and Cells and Surveys: ShouldBiological Measures Be Included in Social Science Research?
David R. Phillips is chair and professor of social policy and academic dean for humanitiesand social sciences at Lingnan University, Hong Kong. He founded the Asia-Pacific Instituteof Ageing Studies at Lingnan in 1998, and was its director until 2001. He researches andteaches gerontology and social epidemiology. His current research interests include health trends,social care, and quality of life among older people in Hong Kong and the Asia Pacific, with aspecial interest in the importance of urbanization and the environment for older people. Herecently co-edited Ageing and Place (2005), Ageing and Long-Term Care: NationalPolicies in the Asia-Pacific (2002), and Environment and Ageing (1999); he also editedAgeing in the Asia-Pacific Region (2000).
This Population Bulletin benefited from suggestions and comments from several reviewers,in particular Huw Jones and Paolo Saad.
The authors wish to acknowledge the ongoing efforts of the U.S. National Institute onAging’s Behavioral and Social Research Program and the United Nations Population Divisionin supporting data development and analyses that enhance our understanding of the globalaging process. The opinions expressed herein are solely those of the authors and do not necessari-ly reflect the views of the U.S. Census Bureau or Lingnan University.
© 2005 by the Population Reference Bureau
Longer-Term View . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Suggested Resources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
Population Bulletin Vol. 60, No. 1 2005 www.prb.org

5
Populations are growing older incountries throughout the world.While the populations of more
developed countries have been agingfor well over a century, this processbegan recently in most less developedcountries, and it is being compressedinto a few decades. By 2050, nearly1.2 billion of the expected 1.5 billionpeople age 65 or older will reside intoday’s less developed regions.1 Just22 percent of the world’s older peo-ple will live in what we today callmore developed countries. Thisdemographic transformation will pro-foundly affect the health and socioe-conomic development of all nations.
Population aging may be seen as ahuman success story—the triumph ofpublic health, medical advancements,and economic development over dis-eases and injuries that had limitedhuman life expectancy for millennia.But the worldwide phenomenon ofaging also brought an acknowledge-ment by the United Nations (UN) ofthe many challenges regarding agingand national development, issues con-cerning the sustainability of familiesand the ability of states and communi-ties to provide for aging populations.2
In April 2002, representatives from159 nations met in Madrid to convenethe Second UN World Assembly onAging, two decades after the first suchassembly. During the 20-year interimbetween these major conferences, thefocus had shifted from basic demo-graphic and economic issues of agingto the inclusion of older people at alllevels of society, a movement to
expand roles for older people, andactive aging policies. Policymakersincreasingly recognize that policies onaging must address the entire societyand people of all ages and that globalaging needs to be integrated into thebroader process of development. Thecentral themes running throughoutthe Madrid International Plan ofAction on Ageing 2002 fall underthree priorities:■ Older people and economic devel-
opment,■ Advancing health and well-being
into old age, and■ Ensuring enabling and supportive
environments.
©Ir
ina G
ush
in/C
CP,
Court
esy
of
Photo
share
Global Aging: TheChallenge of SuccessBy Kevin Kinsella and David R. Phillips
Russia, like many industrialized countries, has seen itspopulation age because of decades of low birth rates.
Population Bulletin Vol. 60, No. 1 2005www.prb.org
Picture removed.

6
This Population Bulletin addressesmany issues that fall under theseoverarching priorities. It examinesthe causes of global population agingand considers related dimensionssuch as the importance of healthimprovements and extended lifeexpectancy for the individual well-being of older people and for socialcosts related to health care.
This Bulletin also considerswhether mounting evidence ofdeclining disability at older agesanswers the question: Are longer lifeexpectancies accompanied by betterhealth or simply more years of poorhealth? Related to this are questionssurrounding intergenerational rela-tionships affected by demographicand social changes, all central to thethree priorities outlined at theMadrid conference. How will smallerfamilies and new forms of familialorganization, for example, affectsocial and personal support systems?How will the labor market, pensionplans, and services adapt to longerlife expectancies, as retirees require25 or more years of income as wellas social and other services?
Who Is Old? When does someone become “old”or “elderly”? A number of terms areused to describe people consideredold, but there is an increasing aware-ness that the terms used shouldacknowledge the tremendous diversi-ty inherent in a group of peoplewhose ages can span a range of 40 ormore years.
Some gerontologists object to theterms “elderly” and “senior citizen”as inadequate generalizations thatconnote negative stereotypes, includ-ing social isolation, frailty, and physi-cal and financial dependence. At thesame time, a general term is usefulfor crossnational comparisons. Inthis Bulletin, “older people” and“older population” refer to peopleage 65 or older; the “oldest old”refers to people age 80 or older,unless otherwise noted.
The Global Processof AgingThe world’s older population has beengrowing more numerous for centuries,but the pace of growth has accelerated.The global population age 65 or olderwas estimated at 461 million in 2004,an increase of 10.3 million just since2003.3 Projections suggest that theannual net gain will continue toexceed 10 million over the nextdecade—more than 850,000 eachmonth. In 1990, 26 nations had olderpopulations of at least 2 million, and by2000, older populations in 31 countrieshad reached the 2 million mark.Projections to 2030 indicate that morethan 60 countries will have at least 2 million people age 65 or older.
People usually associate the growthof older populations with the industri-alized countries of Europe and NorthAmerica. Indeed, industrializednations have the highest percentagesof older people in the world today;before the middle of the 21st century,some of these countries may havemore grandparents than childrenunder age 18. But less developednations also have large numbers ofolder citizens—and the numbers ofolder people are increasing rapidly.Sixty percent of the world’s olderpopulation now live in less developedcountries—an estimated 279 millionpeople. By 2030, this proportion isprojected to increase to 71 percent(690 million). Many less developedcountries have had or are now experi-encing a significant downturn in nat-ural population increase (birthsminus deaths) similar to the declinethat previously occurred in industrial-ized nations. As the rate of naturalincrease slows further, age structureswill change, and the older populationwill be an ever-larger proportion ofeach nation’s total population.
Measures of Aging Population aging is usually defined asthe percentage of a given populationage 65 or older (and sometimes the
Population Bulletin Vol. 60, No. 1 2005 www.prb.org

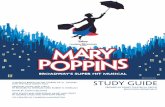
percentage ages 60 and older). Morethan 19 percent of Italy’s populationis age 65 or older, making it theworld’s “oldest” major country. Exceptfor Japan, the world’s 20 oldest coun-tries are all in Europe (see Figure 1).The U.S. population is relatively“young” by European standards, withless than 13 percent age 65 or older.The United States ranks as the 38tholdest country. The U.S. proportionwill rise only slightly during the firstdecade of the 21st century as theearly large birth cohorts of the babyboom (born between 1946 and 1964)approach 65. Beginning in 2011, theaging of the baby-boom generationwill push the proportion of olderAmericans to 20 percent by 2030. Itwill still be lower than in mostWestern European countries.
Europe should remain the world’soldest region well into the 21st centu-ry. The older share of population isexpected to more than doublebetween 2000 and 2030 in Asia andLatin America and the Caribbean.Aging is occurring more slowly in sub-Saharan Africa, where relatively highbirth rates are keeping the popula-tion “young” (see Table 1, page 6).
But these regional averages oftenmask great diversity among and withincountries. India and Thailand may beclose geographically, but Thailand isaging much more rapidly. Likewise,many Caribbean nations have highproportions of older people (theCaribbean is the oldest of all less devel-oped regions) compared with theirCentral American neighbors. Moreimportant, simple percentages cannotdepict the momentum of older-popu-lation growth. Although the percent ofolder population in sub-Saharan Africawill change little between 2000 and2015, the size of this population isexpected to jump by nearly 50 per-cent—from 18.9 million to 28.1 mil-lion people—as the region’s total pop-ulation surges from 651 million to aprojected 899 million. In less devel-oped countries as diverse as Malaysiaand Colombia, older populations areexpected to more than triple in sizebetween 2000 and 2030.
There are several demographicindices of aging—the aging index,median age, and support ratios—thatcompare different portions of a givenpopulation. One straightforward indi-cator of age structure is the agingindex, defined here as the number ofpeople age 65 or older per 100 chil-dren under age 15. At the turn of thecentury, only a few countries (such asItaly, Germany, Bulgaria, and Japan)had more older people than youthages 0 to 14. By 2030, however, nearlyall more developed countries will havea projected aging index of at least100, and several European countriesand Japan will be in excess of 200.Today’s aging index usually is muchlower in less developed countries thanin the more developed world, and thepattern of future change is likely tovary among countries. Absolutechange in the aging index will besmall if future fertility rates remain
7
ItalyJapan
GreeceGermany
SpainSwedenBelgiumBulgariaPortugalEstoniaFranceCroatiaAustriaLatvia
United KingdomFinland
GeorgiaUkraine
SwitzerlandSlovenia
United States
Percent age 65 or older
19.1 19.0 18.6 18.3 17.6 17.3 17.3 17.1 16.9 16.5 16.4 16.4 16.0 15.8 15.7 15.7 15.5 15.4 15.3 15.112.4
Note: The United States ranks 38th.
Source: U.S. Census Bureau, International Data Base (www.census.gov/ipc/www/idbnew.html, accessed Dec. 12, 2004).
Figure 1The World’s 20 ‘Oldest’ Countries and the UnitedStates, 2004
Population Bulletin Vol. 60, No. 1 2005www.prb.org

8
relatively high. Generally, however, theproportional rise in the aging index inless developed countries is expectedto be greater than in more developedcountries.
The median age of country popula-tions will increase everywhere. Themedian age in most developed coun-tries is at least 32, while the medianage in most developing nations isbelow 25. By 2030, Italy and Japan areprojected to have the world’s highestmedian age, with half their popula-tions age 52 or older, largely reflect-ing their extremely low fertility. At theother end of the spectrum, persistent-ly high birth rates are likely to pre-clude a large rise in median age insuch less developed countries asPakistan, Liberia, and Malawi.
Finally, social support ratios areanother widely used indicator ofbroad changes in a nation’s age struc-
ture. These ratios typically indicatethe number of youths and/or olderpeople per 100 people ages 20 to 64,the primary working ages. One com-monly used term is the elderly supportratio, also called the elderly depen-dency ratio, and is defined here asthe number of people age 65 or olderper 100 people ages 20 to 64 in agiven population (see Box 1). Infuture decades, elderly support ratioswill rise in more developed countriesbecause of declining fertility andincreasing longevity among their resi-dents. The rise has been and will con-tinue to be modest in most countriesbecause the large post-World War IIbirth cohorts will still be of workingage through at least 2010. In theUnited Kingdom, the United States,Russia, and several other industrial-ized countries, the elderly supportratio will not change significantly inthe first decade of the 21st century.Other industrialized nations, however,are aging much faster. Between 2000and 2015, the elderly support ratio islikely to increase 33 percent inDenmark (from 24 to 32) and 36 per-cent in the Czech Republic (from 22to 30). Nearly all European countrieswill have elderly support ratiosgreater than 40 by 2030. Japan’selderly support ratio is expected tojump from 27 to 45 between 2000 and2015, and to 53 by 2030.
In countries where fertility remainshigh or has just recently begun todecline significantly—as in much ofAfrica and South Asia—elderly supportratios should change little between2000 and 2030. Eastern and southeast-ern Asia and parts of Latin America,on the other hand, should experiencesignificant change in elderly supportratios during that time. The elderlysupport ratio is projected to at leastdouble between 2000 and 2030 inmany Asian and Latin American coun-tries, and to triple in South Korea.
The Oldest OldThe older population within coun-tries is also aging. Over time, anation’s older population often
Population Bulletin Vol. 60, No. 1 2005 www.prb.org
Table 1Percent of Population in Older Ages by Region, 2000,2015, and 2030
65 years 80 yearsRegion Year or older or older
Asia 2000 5.9 0.92015 7.8 1.42030 12.0 2.3
Europe 2000 14.7 3.02015 17.6 4.72030 23.5 6.4
Latin America/Caribbean 2000 5.6 1.02015 7.6 1.52030 11.5 2.5
Middle East/North Africa 2000 4.4 0.62015 5.5 0.92030 8.4 1.4
North America 2000 12.4 3.32015 14.7 3.92030 20.0 5.4
Oceania 2000 10.1 2.32015 12.4 3.12030 16.3 4.4
Sub-Saharan Africa 2000 2.9 0.32015 3.1 0.42030 3.6 0.5
Source: U.S. Census Bureau, International Data Base (www.census.gov/ipc/www/idbnew.html, accessed Dec. 12, 2004).

grows older on average as a largerproportion survive to advancedages. The “oldest old” (people age80 or older) constituted 18 percentof the world’s older people in 2004:24 percent in more developed coun-tries and 15 percent in less devel-oped countries. More than half ofthe world’s oldest old in 2004 livedin just six countries: China, theUnited States, India, Japan,Germany, and Russia.
In many countries, the oldest oldare the fastest growing segment of thepopulation. In the mid-1990s, theglobal growth rate of the oldest oldwas somewhat lower than that of theworld’s older population, a result of asharp dip in birth rates that prevailedin many countries around the time ofWorld War I. People reaching age 80in 1996, for example, were part of arelatively small birth cohort. Thegrowth rate of the world’s oldest-oldpopulation from 1996 to 1997 wasonly 1.3 percent. Just a few years later,however, the larger post-World War Icohort entered advanced ages, andthe oldest age group began to swell.Between 1999 and 2000, the growthrate of the world’s 80-and-older popu-lation had jumped to 3.5 percent,considerably higher than that of theworld’s elderly as a whole (2.3 per-cent). Demographers expect to seethis high growth of the oldest oldcontinue. The number of people age80 or older is projected to jump near-ly 50 percent between 2000 and 2010,and another 37 percent between 2010and 2020. In contrast, the 65-and-older population is projected toincrease 24 percent between 2000and 2010.
Age profiles of elderly populationsvary considerably among countries. Inthe United States, the oldest old were26 percent of all older people in2000. This share will rise graduallyduring the current decade, thendecline by 2020, and return slowly tothe 2000 level as we near 2030. SomeEuropean nations will experience asustained rise in the ratio of peopleage 80 or older, while others will seean increase during the next two
decades and then a subsequentdecline. The most striking nationalincrease is likely to occur in Japan; by2030, 40 percent of all older Japaneseare expected to be at least 80 yearsold. Most less developed countriesshould experience modest long-termincreases in this ratio.
Even when the proportion of old-est old within an elderly populationremains stable, the absolute numbersof this oldest group can increase sub-stantially. In the United States, theoldest old increased from 374,000 in1900 to more than 10 million today.
9
The standard definition of an elderly support ratio implies thatall people over age 64 are in some sense dependent on the pop-ulation of working age (20 to 64). People ages 20 to 64 supportolder people indirectly through payroll taxes and contributionsto social welfare programs. We know, however, that elderly popu-lations have extremely diverse resources, needs, and abilities,and that many older people are financially and physically inde-pendent. Through their taxes, income, and wealth, older peoplealso fuel economic growth and provide support to younger gen-erations. Likewise, substantial portions of the working-age popu-lation may not earn incomes because they are unemployed,unable to work, in school, or have opted out of the labor force.
Although it is difficult to include factors such as intrafamilyfinancial assistance and child-care activities in an overall mea-sure of social support, it is feasible to consider employmentcharacteristics in both the working-age and elderly populations.An alternative to the standard support ratio might, for example,include only the economically active population in the denomi-nator, thereby excluding people who choose not to work,unpaid household workers, nonworking students, and individu-als whose poor health keeps them out of the labor force. A relat-ed alternative is to also remove economically active people age65 or older from the numerator on the assumption that they arenot economically dependent. Economically active older peoplecould be added to younger economically active adults who alsocontribute tax revenue.
The alternative ratios in each country are higher than thestandard elderly support ratio in most industrialized nations.Japan is an exception—older Japanese have a relatively high rateof participation in part-time work. Whether labor force partici-pation is excluded or included can make a considerable differ-ence for planning agencies that use support ratio calculations.When data are available, these ratios also can be adjusted forsuch factors as workers under age 20; the effects of unemploy-ment; average retirement ages; levels of pension receipt andinstitutionalization among older people; and the prevalence ofhigh-cost disabilities.
Box 1How Useful Are Elderly Support Ratios?
Population Bulletin Vol. 60, No. 1 2005www.prb.org

10
The number is projected to rise bymore than 9 million between 2004and 2030, even though the share ofAmericans age 80 or older will remainabout the same. Four-generation fam-ilies are becoming increasingly com-mon, and the aging of the baby boommay produce a great-grandparentboom in many countries.
Prior population projections oftenhave underestimated the slowdown inmortality among the oldest old, andthe number of tomorrow’s oldest oldcould be much higher than nowanticipated. The actual numbers inthe highest age groups are importantfor planners and policymakersbecause the oldest old consume dis-proportionate amounts of health andlong-term care services.4 In the past,population projections for the world’scountries often grouped everyone age80 or older into a single, open-endedcomponent. Recently and for the firsttime, the UN Population Division, theU.S. Census Bureau’s InternationalPrograms Center, and other institu-tions are adding more age detail totheir international population projec-tions—often up to ages 100 andolder—a reflection of the expectedgrowth at these oldest ages.
As longevity increases, the conceptof “oldest old” will change. Whilepeople of extreme old age constitutea tiny portion of total population inmost of the world, their numbers areof growing importance, especially inmore developed nations. Thanks toimprovements in nutrition, health,and health care, we now have theopportunity to consider significantgrowth of the population age 100 orolder. According to Europeanresearchers, the number of centenari-ans has doubled each decade since1950 in industrialized countries.Using reliable statistics from 10Western European countries andJapan, demographers James Vaupeland Bernard Jeune estimated thatsome 8,800 centenarians lived inthese countries as of 1990, and thatthe number of centenarians grew atan average annual rate of approxi-mately 7 percent between the early
1950s and the late 1980s.5 Vaupel andJeune also estimated that the odds ofliving from birth to age 100 may haverisen from 1 in 20 million to 1 in 50for females in low-mortality nationssuch as Japan and Sweden.
The DemographicDrivers of Aging When asked “Why do populationsage?,” most people intuitively think ofchanges in longevity. We know thatlife expectancy has been rising inmost countries throughout the world,so it seems reasonable that popula-tion aging is an outcome of peopleliving longer. Yet, the most prominenthistorical factor in population aginghas been declining fertility. If wethink of population aging as anincrease in the percent of people age 65 or older, we realize that, overtime, a decline in the number ofbabies will mean fewer young peopleand proportionally more people atolder ages.
Fertility—The PrimaryDriverThe decrease in fertility in industrial-ized nations during the last centuryhas pushed the average number ofchildren per woman in almost allmore developed countries below thepopulation replacement level of 2.1children. Sustained low fertility sincethe late 1970s has reduced the size ofsuccessive birth cohorts and increasedthe proportion of older people inthese countries’ populations. Fertilitydecline in the less developed worldhas been more recent and morerapid; most regions have seen largereductions in fertility rates during thelast 30 years. Although the aggregatetotal fertility rate (TFR, the averagenumber of children per woman givencurrent birth rates) remains in excessof 4.5 children per woman in Africaand many countries of the MiddleEast, overall levels in Asia and LatinAmerica decreased by about 50 per-
Population Bulletin Vol. 60, No. 1 2005 www.prb.org
At very oldages, the rate of increase inmortality tendsto slow.

cent (from 6 to 3 children perwoman) between 1965 and 1995. TheTFR in many less developed countriesis now at or below replacementlevel—notably in the world’s mostpopulous country, China. By 2000, amajority of the world’s populationlived in countries with near- or below-replacement fertility.6 The UN pro-jects that, by 2050, three of every fourof today’s less developed countrieswill have below-replacement fertility.
Populations with high fertility tendto have low proportions of older peo-ple and vice versa. The term “demo-graphic transition” is used to describea gradual process of change fromhigh rates of fertility and mortality tolow rates of fertility and mortality.The process is characterized first bydeclines in infant and childhood mor-tality, as infectious and parasitic dis-eases are controlled through expan-sion of public health services andfacilities and disease eradication pro-grams. This improvement in mortalityoccurs while fertility is still high,resulting in large birth cohorts andan expanding proportion of childrenrelative to adults. Other things beingequal, the initial decline in mortalitygenerates a younger population agestructure.7
Increasing Importance ofMortalityIn countries where infant mortalityrates are relatively high but declining,most of the improvement in lifeexpectancy at birth results from help-ing infants survive the high-risk earlyyears of life. Reductions in maternalmortality also contribute to increasedlife expectancy at birth. As a nation’sinfant, childhood, and maternal mor-tality reach low levels, longevity gainsat older ages become more promi-nent contributors to increased lifeexpectancy.8 Most countries today areexperiencing a rise in life expectancyat older ages, which contributes to ris-ing life expectancy at birth. For exam-ple, the average Japanese womanreaching age 65 in 2000 could expectto live more than 22 additional years,
and the average man more than 17years. Japanese life expectancy at age65 for both sexes combined increased44 percent from 1970 to 2000, whilelife expectancy at birth increased only9 percent. Comparative figures forthe United States are 19 percent and9 percent, respectively.
The speed at which death rates atadvanced ages decline will play amajor role in determining futurenumbers of older, and especially ofvery old, populations. The remaininglife expectancy of 80-year-old womenin England and Wales is about 50 per-cent higher today than it was in 1950.Hence, the number of female octoge-narians is about 50 percent higherthan it would have been had oldest-old mortality remained at 1950 levels.In absolute terms, there are morethan 500,000 British women age 80 orolder alive today who otherwise wouldhave died if death rates for the oldest-old had not improved.9
Until the mid-1990s, conventionaldemographic wisdom held that thehuman death rate increases with agein an exponential manner. Newerresearch has documented that, at veryold ages, the rate of increase in themortality rate tends to slow down. Astudy of 28 countries with reliable datafor 1950 to 1990 found not only adecline in mortality rates at ages 80and older, but also a tendency towardgreater decline in more recent years.10
Other work has confirmed this tenden-cy, and one study in the United Statessuggests that the age at which mortali-ty deceleration occurs is rising.11
There are at least two potentialexplanations of this deceleration ofmortality at the oldest ages. The “het-erogeneity” hypothesis, an extensionof the notion of “survival of thefittest,” posits that the deceleration inold-age mortality is a result of frailerolder people dying at younger ages,thus creating a very old populationwith exceptionally healthy attributesresulting from genetic endowmentand/or lifestyle. A second, “individual-risk” hypothesis, suggests that the rateof aging may slow down at very oldages, and/or that certain genes that
11Population Bulletin Vol. 60, No. 1 2005www.prb.org

12
are detrimental to survival may be sup-pressed.12 The observed decelerationin mortality, combined with the factthat human mortality at older ages hasdeclined substantially, has led to thequestioning of many of the theoreticaltenets of aging. Important insights arebeing garnered from “biodemograph-ic” research that attempts to crossfer-tilize the biologic and demographicperspectives of aging and senescence.A clearer picture of the causes of mor-tality deceleration at very old ages mayemerge from the study of evolutionarybiology and aging in nonhumanspecies. But recognition of this slow-down in old-age mortality—at a timewhen numbers of the very old aregrowing rapidly—has important policyimplications.13
Changes in LifeExpectancyThe dramatic increases in lifeexpectancy that began in the mid-1800s often are thought to be theresult of medical breakthroughs. Infact, the major impact of improve-ments in medicine and sanitation didnot occur until the late 19th century.Prior innovations in industrial andagricultural production and distribu-tion, which improved nutrition forlarge numbers of people, were morepowerful forces in mortality reduc-tions. A growing multidisciplinaryresearch consensus attributes the gainin human longevity since the 1800s tothe interplay of advancements inmedicine and sanitation against abackdrop of new modes of familial,social, economic, and political organi-zation.14 Life expectancy at birth inJapan approached 82 years in 2003,the highest level among the world’smajor countries. Life expectancy is atleast 79 years in several other devel-oped nations, including Australia,Canada, Italy, Iceland, Sweden, andSwitzerland. Average life expectancyin the United States and most otherdeveloped countries ranged between76 and 78 years.
Throughout the less developedworld, there are extreme variations in
life expectancy at birth. Some nationshave levels equal to or higher thanthose in many European nations,whereas life expectancy at birth innumerous African countries is lessthan 45 years. The average personborn in a more developed countrycan now expect to outlive his or hercounterpart in the less developedworld by 14 years.
In some nations, life expectancymore than doubled during the 20thcentury (see Table 2). Increases in lifeexpectancy were more rapid in thefirst half than in the second half ofthe century. Between 1900 and 1950,many Western nations added 20 ormore years to their average lifeexpectancy. Reliable estimates of lifeexpectancy for less developed coun-tries prior to 1950 are scarce, butchanges in life expectancy in thesecountries have been fairly uniformsince then. Practically all nations haveshown continued improvement, withsome exceptions in Latin Americaand more recently in Africa, the latterdue to the impact of the HIV/AIDSepidemic. The most dramatic gainshave occurred in East Asia, whereaverage life expectancy at birth forthe region increased from less than45 years in 1950 to more than 72years today.
An increasing gender differentialin life expectancy was a hallmark ofmortality patterns in more developedcountries in the 20th century, reflect-ing the generally lower mortality offemales than males in every agegroup and for most causes of death.In Europe in 1900, women typicallyoutlived men by two or three years.Today, the average gap between thesexes is approximately seven years,and may be as high as 12 years inparts of the former Soviet Union.Gender differentials tend to be small-er (between three and six years) inless developed countries, and arereversed in a few South Asian andMiddle Eastern societies in whichsuch cultural factors as low femalesocial status and a preference formale rather than female offspringaffect female life expectancy.
Population Bulletin Vol. 60, No. 1 2005 www.prb.org

Changing Age Structure Populations begin to age when fertil-ity declines and adult mortality ratesimprove. Successive birth cohortseventually become smaller, althoughthe trend may be interrupted by“baby-boom echoes” as women ofprior large birth cohorts reach child-bearing age. International migrationusually does not play a major role inthe aging process, but can be impor-tant in smaller populations. SomeCaribbean nations, for example,have experienced a combination ofemigration of working-age adults,immigration of retirees from othercountries, and return migration ofolder former emigrants; all threefactors contribute to populationaging. Many observers expect inter-national migration to assume a moreprominent role in the aging process,particularly in “older” countrieswhere persistently low fertility hasled to stable or even declining popu-lation size.15
Most if not all countries once hada youthful age structure similar tothat of less developed countries as awhole in 1950, with a large percent-age of the entire population underage 15. Given the comparatively highrates of fertility that prevailed in mostless developed countries from 1950through the early 1970s, the pyrami-dal shape of the age and sex profileof less developed countries had notchanged greatly by 1990 (see Figure2, page 12). However, the effects offertility and mortality decline can beseen in the projected age-sex pyramidfor 2030, which loses its strictly trian-gular shape as the size of youngerfive-year cohorts stabilizes and theolder portion of the total populationincreases.
The picture in more developedcountries has been and will be quitedifferent. In 1950, there was relative-ly little variation in the size of five-year groups between the ages of 5and 24. The beginning of the post-World War II baby boom can beseen in the 0-to-4 age group. By1990, the baby-boom cohorts wereages 25 to 44, and younger cohorts
were successively smaller. If project-ed fertility rates are reasonably accu-rate through 2030, the aggregatepyramid will start to invert, withmore weight on the top than on thebottom, and the size of the oldest-old population (especially women)will increase substantially.
13
Table 2Life Expectancy at Birth in Years, Selected Countries, 1900, 1950, and 2003
Circa 1900 Circa 1950 Circa 2003Region/country Male Female Male Female Male Female
More developed countries
Western EuropeAustria 38 40 63 68 75 81 France 45 49 64 70 75 83Sweden 53 55 70 73 78 83United Kingdom 46 50 67 72 76 81
Southern and eastern EuropeHungary 37 38 62 66 68 76Italy 43 43 64 68 76 82Spain 34 36 62 66 76 83
OtherAustralia 53 57 67 72 76 82Japan 43 44 60 63 78 85United States 48 51 66 72 74 80
Less developed countries
AfricaEgypt — — 41 44 67 71Ghana — — 40 44 57 59Mali — — 31 34 48 49South Africa — — 44 46 45 51Uganda — — 39 42 45 47
AsiaChina — — 39 42 69 73India — — 39 38 63 65Kazakhstan — — 52 62 61 72South Korea — — 46 49 72 79Syria — — 45 47 71 73
Latin AmericaArgentina — — 60 65 71 78Bolivia — — 39 43 62 66Brazil — — 49 53 64 73Costa Rica — — 56 59 76 81Mexico — — 49 52 70 76
— Not available.Note: Average number of years a person born in those years could expect to live.
Source: UN Population Division, World Population Prospects: The 2002 Revision (2003);and G. Siampos, Statistical Journal of the United Nations Economic Commission for Europe 7,no. 1 (1990): 13-25.
Population Bulletin Vol. 60, No. 1 2005www.prb.org

14
Emergent DiversityDemographers have long known thatthe world was aging because ofdeclines in birth rates and increasesin adult life expectancy. On the tradi-tional path toward population aging,however, a number of unexpectedboulders have surfaced. Scientists
have been surprised by the speed ofaging in some parts of the world, byunforeseen developments in mortalitychange, and by the emergence orreemergence of diseases. While differ-ences in the levels of populationaging between more developed andless developed countries have beenobvious for some time, several devel-
Population Bulletin Vol. 60, No. 1 2005 www.prb.org
More developed countries
Figure 2Population Age-Sex Structure in Less Developed and More Developed Countries, 1950, 1990, and 2030
Less developed countries
Source: UN Population Division, World Population Prospects: The 2002 Revision (http://esa.un.org/unpp, accessed Dec. 9, 2004).

opments have added new wrinkles towhat was once expected to be amonotonic march toward aging.
Compression of AgingOne of the most surprising demo-graphic developments in the last twodecades has been the pace of fertilitydecline in many less developed coun-tries. The common perception is thatbelow-replacement fertility levels areseen only in the industrialized nationsof the Northern Hemisphere. As of2002, however, the TFR was belowreplacement level in 33 less developedcountries—mostly in Latin Americaand the Caribbean and parts of Asia—and is declining steeply in many oth-ers. The demographic effects of fertili-ty decline have been most dramatic insome highly populous Asian countriesbecause of the rapidity of the declinein these countries.
Aging has proceeded more gradu-ally in Western nations. It took 115years for the proportion of France’spopulation age 65 or older toincrease from 7 percent to 14 percent(see Figure 3). Most other moredeveloped nations have had manydecades to adjust to this structuralchange. Japan is the major exception,where this same increase occurred injust 26 years. A similarly rapid trajec-
tory is underway elsewhere in Eastand Southeast Asia (especially China,South Korea, Taiwan, and Thailand),fueled by dramatic and relativelyrecent drops in fertility. Such rapidlyaging non-Western societies arebeginning to engage in the samedebates about public pension andhealth care costs that have becomecommon in Europe and NorthAmerica.
The People’s Republic of Chinaillustrates how rapidly declining fertil-ity affects population aging. China’sTFR plummeted from about 6.0 in1965 to near-replacement level by1990 and to 1.7 by 2002. The declinewas reinforced by strict birth planningpolicies enacted in the late 1970s.Consequently, China will age soonerand more quickly than most lessdeveloped countries. China’s age pro-file in 2002 contained a large “bulge”consisting of people ages 28 to 39.The oldest people in this age bulgewill be entering their 60s just prior to2025, signaling a rapid aging of theChinese population in the third andfourth decades of the 21st century.The number of Chinese ages 65 andolder is projected to swell from 88million in 2000 to 199 million in2025—and to 349 million in 2050,barring a catastrophic rise in adultmortality or massive emigration.
15
Note: Dates show the span of years when percent of population age 65 or older rose (or is projected to rise) from 7 percent to 14 percent.
Source: K. Kinsella and Y.J. Gist, Older Workers, Retirement, and Pensions: A Comparative International Chartbook (1995); and authors’ calculations.
Figure 3Speed of Population Aging in Selected Countries
Number of years required or expected for percent of population age 65 or older to rise from 7% to 14%
Population Bulletin Vol. 60, No. 1 2005www.prb.org

16
Recognizing this near-certain surge,the central Chinese government andvarious local governments are strug-gling to establish alternative forms ofpensions to provide for what is still apredominantly rural nation. Someanalysts and policymakers are callingfor an easing of birth restrictions toslow the pace of aging.
Slow Structural AgingIn stark contrast to the rapidity ofaging in other parts of the less devel-oped world, most of sub-SaharanAfrica remains in an intermediatestage of demographic transition.Fertility and mortality rates are quitehigh by global standards, and theregional age structure is changingonly gradually. Women in sub-Saharan Africa still bear nearly 5.5children on average, compared with2.8 in North Africa and 2.4 in Asia.Although infant and maternal mortal-ity are also comparatively high, thelarge numbers of babies born eachyear ensure that the base of sub-Saharan Africa’s population pyramidwill remain quite broad. At the sametime, life expectancy at birth for theregion is approximately 50 years, 13years below the average for all lessdeveloped countries. The scourge ofHIV/AIDS has pushed average lifeexpectancy below 40 years in somesub-Saharan nations. “Old age” inZimbabwe or Mali has a very differentchronological interpretation than inSwitzerland or Japan.
The proportion of older people inAfrica is expected to increase onlymodestly in the coming decades,although the absolute number ofolder people will rise steeply. Whileaging as a sociopolitical issue is not ahigh priority for most African govern-ments, there are unique features ofmany African societies that beardirectly on older people. One is theimpact of HIV/AIDS (discussedlater), which thrusts older adults backinto the role of primary childproviders. Another is the rapidlygrowing number of widows and therole that polygyny may play in their
well-being or lack thereof. Also, sub-Saharan Africa is the most rapidlyurbanizing world region, and theimplications of migration patterns forthe well-being of older Africans arenot well understood.
Aging and Depopulation The world is witnessing a new andunprecedented demographic phenom-enon: simultaneous population agingand an overall decline in the total sizeof some national populations (see Box2). European demographers havesounded warning bells for at least 30years about the possibility of decliningpopulation size in industrializednations. But this idea had not resonat-ed in public discourse until recently.Many in these societies were aware thattheir populations were aging, but theyoften did not equate aging with popu-lation decline. In the last several years,the awareness of potential populationdecline has increased considerably, inlarge part because of reports suggest-ing that populations in much ofEurope and Japan will decrease in sizeover the next 50 years, and because ofpublicity generated by recent actualpopulation declines in Spain, Italy,Russia, and other nations.
Projections to 2030 suggest that 11countries are expected to lose at least1 million people within 30 years.Russia tops the list with a projecteddecline of 12 million, followed byJapan with 11 million. Not all popula-tion declines will result from persis-tently low fertility. South Africa is pro-jected to have 10 million fewer citizensin 2030 than it does today because ofHIV/AIDS mortality. By and large,however, aging and depopulation willbe a European phenomenon.
Divergence in LifeExpectancyIn the 1950s, female life expectancycontinued its rise everywhere, butgains among males slowed significant-ly and in some cases leveled off. Fromthe early 1950s to the early 1970s, forexample, male life expectancy
Population Bulletin Vol. 60, No. 1 2005 www.prb.org
There areunique featuresof Africansocieties thataffect olderpeople.

changed little in Australia, theNetherlands, Norway, and the UnitedStates, before resuming a modestincrease.
In eastern Europe and the formerSoviet Union, advances in living condi-tions and public health policies pro-duced large declines in mortality inthe 1950s and early 1960s. Some majorcauses of death, such as tuberculosis,were reduced to minimal levels. Gainsin life expectancy in excess of fiveyears per decade were common. Therate of increase in life expectancy fellsharply in the mid-1960s, however.Changes in female life expectancy atbirth were erratic during the next twodecades, while male life expectancyfell throughout the region. The politi-cal and economic collapse of the for-mer Soviet Union undermined publichealth and led to severe declines inlife expectancy, especially for Russianmen. Between 1987 and 1994, lifeexpectancy at birth for Russian males
plunged 7.3 years to 57.6 years and hasnot fully recovered. The large increas-es in adult male mortality usually areattributed to a combination of factors,including increased homicide andaccident rates, excessive alcohol con-sumption, poor diet, and environmen-tal/workplace degradation.16 Researchon indicators of social capital inHungary suggests that gender differ-ences in social support systems alsoplay a role; support systems for menappear strained by changes inHungarian society, while traditionallyclose-knit networks among womenremain relatively unchanged.17
In parts of Africa, the HIV/AIDSepidemic has devastated life expectan-cy at birth, reflecting the concentra-tion of AIDS deaths there in child-hood and the middle adult ages. U.S.Census Bureau projections to the year2010 imply that AIDS will reduce lifeexpectancy at birth by more than 30years from otherwise-expected levels in
17
Is persistent below-replacement fertility a threat toEuropean and other societies, and if so, how might itbe altered? Should so-called “replacement migra-tion” be encouraged to offset population aging?
There are no straightforward answers to thesequestions. A number of theories attempt to explainmodern-day levels of low fertility, focusing on con-cepts such as risk aversion, materialist values, andgender equity.1 One study that examined a diverseset of countries that have made the transition to lowfertility found very few countries in which fertility sta-bilized above two children per woman.2 Such anoccurrence would require substantial proportions ofthird or higher-order births, but higher-order birthsare largely anachronistic in industrial-country set-tings. The tentative conclusion was that fertility isunlikely to rebound significantly, though we shouldremember that few demographers anticipated thepost-World War II baby boom that will soon acceler-ate population aging.
Governments in low-fertility countries haveemployed various means to increase fertility, includ-ing direct financial incentives for additional births;tax reductions; indirect pension (early retirement)or in-kind benefits such as preferential access to sub-sidized housing; more liberal maternity and paternityleave and childcare arrangements; and legislationpromoting gender equity in employment. These
policies have had modest impacts in authoritarianstates, but only minimal impacts in liberal democra-cies such as France and Sweden.3
In 2000, a United Nations study concluded thatimmigration was not a realistic counterbalance toaging for avoiding population decline.4 UN expertsfound that immigration could buffer the impact ofaging if used by governments in conjunction withother policies, such as measures to encourage higherfertility or to increase labor force participation, espe-cially among women.
References1. Peter McDonald, “Sustaining Fertility Through Public
Policy: The Range of Options,” Population 57, no. 3(2002): 417-46.
2. National Research Council, Beyond Six Billion: Forecastingthe World’s Population, ed. John Bongaarts and Rodolfo A.Bulatao (Washington, DC: National Academies Press,2000).
3. Michael S. Teitelbaum, “Long-Range DemographicProjections and Their Implications for the UnitedStates,” in United Nations Expert Group Meeting on PolicyResponses to Population Ageing and Population Decline, ed.United Nations (UN) Population Division,ESA/P/WP.163 (New York: UN, 2000): 17/1-11.
4. UN Population Division, United Nations Expert GroupMeeting on Policy Responses to Population Ageing andPopulation Decline.
Box 2Aging and Depopulation
Population Bulletin Vol. 60, No. 1 2005www.prb.org

18
Botswana, Namibia, South Africa, andZimbabwe. The epidemic also canhave a significant impact on older pop-ulations. In the United States in 2000,the HIV-death rate among people ages65 to 74 was more than four times ashigh as among youth ages 15 to 24.18
Intranational DifferencesIn addition to global and regional dif-ferences in aging, important differ-ences may play out within nations aswell. Census data for Brazil show that,while the overall national aging indexwas 14 in 1991, the index rangedfrom less than 6 in several northernstates to 21 in the state of Rio deJaneiro. In the United States, morethan one-third of the population insome counties is age 65 or older. In2003, 17 percent of Florida’s residentswere at least 65 years old.
In many countries, older peopleare becoming concentrated in ruralareas as young adults leave rural areasfor the cities and some older urbanmigrants return to rural communitiesas they reach old age. Older womenare more likely than older men to livein rural areas, causing an imbalancedage-sex distribution. In the Russianregion of Kursk, for example, nearly31 percent of rural females are age 65or older, compared with just 15 per-cent of rural males.
Skewed age structures complicatethe provision of services for olderpeople in some localities. Based onthe experiences of Japan and Korea,demographer Ronald Skeldon hasnoted that overall population agingcoincides with rural depopulationand population stagnation in small-and medium-sized towns, and sug-gests that this pattern will increasinglybe seen throughout Asia in the firsthalf of this century.19 A similar phe-nomenon has been identified inItaly.20 While few if any negativenational economic consequences areassociated with the concentration ofolder people in rural communities,social conditions in relatively isolatedrural areas are likely to requireincreasing attention by policymakers.
Health TransitionsThe global phenomenon of popula-tion aging is directly related to a fun-damental health transition that has beenoccurring throughout the world at dif-ferent rates and along different paths.The health transition—also called theepidemiological transition—is defined bya broad set of changes that include ashift from high to low fertility, steadyexpansion of life expectancy at birthand at older ages, and a transitionfrom the predominance of infectiousand parasitic diseases to the growingimportance of noncommunicable dis-eases and chronic conditions. Thehealth transition has been linked tomodernization and urbanization, espe-cially improvements in standards of liv-ing and education. As Russia’s recenterosion in life expectancy illustrates,health transition gains can be lost asnational economies and public ser-vices stagnate and even regressbecause of social, political, or econom-ic upheavals.
The health transition is allied withthe demographic transition that beganin more developed countries duringthe 18th and 19th centuries as popu-lations shifted from high to low mor-tality, thanks to better health andnutrition. As death rates fell, popula-tion growth surged until birth ratesdropped, eventually falling close to—or even below—the level of deathrates. This transition took at least 100years in most of Europe and theUnited States. While many less devel-oped countries have not completedthe transition to low birth and deathrates and slow population growth,many have passed through some ofthe same stages of falling mortality,rapid population growth driven byhigh fertility, and then falling fertilityand slower population growth.
The epidemiological transition wasoriginally conceptualized as a three-stage process that paralleled the laterstages of demographic transition. AnAge of Pestilence and Famine was suc-ceeded by an Age of RecedingPandemics and then an Age ofDegenerative and Man-Made
Population Bulletin Vol. 60, No. 1 2005 www.prb.org

Diseases. A fourth stage has been rec-ognized in recent decades—a hybridstage in which some social and geo-graphic factors affect the health ofspecific population groups. Behaviorsand lifestyle obviously influencehealth status, and health practitionersare increasingly concerned about ris-ing ill health and mortality from whatare sometimes called social patholo-gies: cirrhosis, substance abuse, obesi-ty, suicide, homicide, HIV/AIDS, andresurgent diseases such as drug-resis-tant tuberculosis and other strains ofinfectious diseases. New emerginginfectious disease variants can beespecially risky for older people, whoare more vulnerable than youngerpeople to acute respiratory diseases.For example, the outbreak in manycountries in 2003 of SARS (severeacute respiratory syndrome) affectedolder people disproportionately. InHong Kong, people ages 65 and olderaccounted for 19 percent of thereported 1,755 SARS cases in 2003.More important, the older populationwas hit much harder with fatalities inthe epidemic; nearly two-thirds of the300 SARS deaths in Hong Kong wereamong older people.21
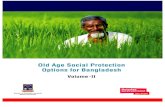
While communicable diseases stillexact a toll—especially among olderpeople—the broad decline in mortali-ty from infectious diseases and the ris-ing importance of chronic diseaseshas delayed deaths until older andolder ages. The epidemiological tran-sition shifts the human survival curvethat depicts people’s chance of surviv-ing another year as they age. In a so-called “wild” survival curve that likelycharacterized nonindustrial, pre-demographic transition societies, therisk of death remains relatively con-stant throughout life, and only a smallproportion of those born reach oldage. Modern survival curves, particu-larly in highly industrialized societies,are much more rectangular, as mostpeople live past middle age anddeaths are highly concentrated atolder ages (see Figure 4). The UN cal-culates that, for more developed coun-tries, 86 percent of people born todaywill survive to age 60 (91 percent for
females, 81 percent for males); almostone-half of people born today canexpect to reach age 80.
How healthy can these older peo-ple be? This question underlies oneof gerontology’s great debates andhas generated varied attempts toquantify the health of older people.The answers have important policyimplications because they influencethe health and social care needs andresidential options for older people.
The health profile of older peoplespans a wide spectrum: Some peoplelive long and healthy lives, while othersexperience the “creaking door” syn-drome of longer life but graduallydeteriorating health. Most analyststhink that some combination of genet-ic factors and lifestyle explains muchof the variation in health at older ages.While some people operate at fullcapacity into very old age, many olderpeople begin to have difficulty with atleast some common daily activities.When do such difficulties become solimiting that an individual is consid-ered disabled or handicapped? Thedefinition is not always clear-cut, but itis important on a variety of levels.
Measuring DisabilityDisability is often visualized as aprocess, as depicted in Figure 5, page18. Many analysts claim this model
19
Figure 4Stylized Wild and Modern Survival Curves
Population Bulletin Vol. 60, No. 1 2005www.prb.org

20
oversimplifies the complexity of dis-ability and function. In itsInternational Classification ofImpairments, Disabilities andHandicaps (ICIDH), the World HealthOrganization (WHO) takes the modela step further, proposing three possi-ble outcomes of disease: impairment,disability, and handicap. Impairmentrefers to the performance of an organor part of the body, whereas disabilityrefers to the performance of an activityby a person. Not all impairments willlead to disability, such that a function-ally limited person may still be able tocarry out all normal activities indepen-dently. The distinction between disabil-ity and handicap is determined byseverity and situation. WHO considersa handicap to be a disadvantage due toan impairment or disability that limitsor prevents a person from fulfilling anormal role. There is wide internation-al variation in the definition and appli-cation of the ICIDH concepts.22
However, the framework is useful forassessing how assistance (either per-sonal or mechanical) can prevent adisability from becoming a handicapthat, for example, prevents a personfrom fulfilling the role of a spouse orgrandparent.
More specific measures of therange of disability a person mightexperience are used to assess needsfor medical care and general assis-tance. Two widely used (but imper-fect) means of measuring a person’sdifficulty in performing personal careand home management tasks areADLs (Activities of Daily Living) andIADLs (Instrumental ADLs). ADLsgauge the extent to which a personcan manage personal care activitiessuch as eating, moving from a bed orchair, bathing, dressing, toileting, andwalking. IADLs refer to home man-
agement activities such as using thephone, shopping, dealing with per-sonal finances, and light housework.These measures assess the ability ofpeople (older people in particular) tolive independently; they are also usedto indicate the need for health andsocial services. Results from the sever-al types of ADL and IADL scales usedto estimate disability prevalence—including Katz, Barthel, and Pulses—can differ by as much as 60 percent.23
By any measure, however, ADL andIADL problems increase with age.Data from the Berlin Aging Studyshowed that, among people ages 70 to84, 9 percent needed help withbathing, 6 percent needed helpclimbing stairs and going for walks,and 4 percent needed help withdressing. In the 85-and-older agegroup, 46 percent needed help withbathing, 33 percent with climbingstairs, 34 percent with going for walks,and 18 percent with dressing.Roughly 20 percent of the younger-old needed assistance with shoppingand transportation, while more than70 percent of people age 85 or oldereither needed help with or wereunable to do these activities.24
There is no simple correlationbetween disability-free life expectancyand life expectancy. International dis-ability figures often are not compara-ble because of differences in defini-tions, concepts of disability, and com-putational methods. Even withinEurope, countries show wide variationsin self-reported levels of severe or anydisability. For example, against a stan-dardized relative risk of severe disabili-ty of 100 for the older populations ineight countries, the United Kingdomand Denmark had a risk of around 70while the level in France exceeded140. Life expectancy at age 65 in the
Population Bulletin Vol. 60, No. 1 2005 www.prb.org
Disease Physiological impairment
Performancelimitations Disability
Figure 5Progression of Disability
Severalmeasures ofdisability forolder Americanshave shownimprovement.

United States and the United Kingdomis similar, but rates of disability appearmuch lower in the United Kingdom;consistent with this disparity, the per-centage of the population 65 or olderreceiving formal home care is almostthree times higher in the UnitedStates. However, the percentage ofoverall expenditure on home care as aproportion of gross domestic product(GDP) is similar in the two countries.25
One international effort to harmonizedisability measures indicates that, inmost countries, the expectation of lifewithout severe disability for older peo-ple is gradually increasing and some-times at a similar rate to increases inlife expectancy.26 A rigorous review ofeight surveys in the United States con-cluded that several measures of disabil-ity for older Americans have shown
improvement in the past decade.27 Lessdeveloped countries eye disability datafrom the more developed world withinterest, as many countries are rapidlycatching up in life expectancy but havelittle insight into the health of theirolder populations. Even if rates of dis-ability can be reduced or the onsetpostponed, demographic trends willalmost inevitably increase the numbersof disabled older people in less devel-oped countries, especially when thenumbers with dementia are included(see Box 3).
Compression of Morbidity Related to the discussion of changingincidence and prevalence of disabilityis the debate on “compression of mor-bidity,” which was articulated by James
21
Dementia is a growing concern around the world aspopulations age. Dementia is an acquired syndromethat eventually destroys memory, reasoning, speech,and other cognitive functions. A crossnational studyconducted by the Organisation for EconomicCooperation and Development (OECD) found thatdementia affected about 10 million people in OECDmember countries, just under 7 percent of people age65 or older. But the prevalence increases sharply withage and threatens to transform dementia into ahealth care crisis in the world’s aging populations.1
Dementia prevalence estimates vary considerablyinternationally, in part because of variations in diag-noses and reporting systems. The syndrome is noteasy to diagnose, especially in its initial stages. Thememory problems, misunderstandings, and inappro-priate behavior common in the early and intermedi-ate stages are often attributed to normal effects ofaging, accepted as personality traits, or simplyignored. Many cases remain undiagnosed even inthe intermediate, more serious stages.
Alzheimer’s disease (AD) is the most commonform of dementia. AD accounted for between two-fifths and four-fifths of all dementia cases in theOECD study. The prevalence of AD and other demen-tias is very low at younger ages but increases with age;the prevalence nearly doubles with every five years ofage. In the OECD study, for example, dementia affect-ed fewer than 3 percent of those ages 65 to 69, butalmost 30 percent of those ages 85 to 89. Amongwomen age 90 or older, more than 50 percent had
dementia in France and Germany; corresponding lev-els were around 40 percent in the United States andjust under 30 percent in Spain.
There are no effective treatments for dementia.Family members often play a key part in the care,especially in the initial stages of what is often a rela-tively slow and distressing decline in a loved one. Thecomplexity of the disease and the wide range of fami-ly and housing settings can make helping people andfamilies with dementia very difficult. However, it is achallenge that must be faced in health and social careworldwide, especially with increasing numbers of peo-ple surviving past age 85. While industrialized coun-tries have struggled to cope with the mounting finan-cial and social burdens of AD, the challenge is evengreater in the less developed world, where at leasttwo-thirds of dementia sufferers are thought to livebut where far fewer coping resources are available.2
References1. Antonio Lobo et al., “Prevalence of Dementia and Major
Subtypes in Europe: A Collaborative Study ofPopulation-Based Cohorts,” Neurology 54, no. 11 (2000):S4-9; and Pierre Moise et al., “Dementia Care in 9 OECDCountries: A Comparative Analysis,” OECD HealthWorking Papers 13 (Paris: Organisation for EconomicCooperation and Development (OECD), 2004).
2. Martin Prince, “Dementia in Developing Countries: AConsensus Statement From the 10/66 DementiaResearch Group,” International Journal of GeriatricPsychiatry 15, no. 1 (2000): 14-20.
Box 3The Challenge of Alzheimer’s Disease and Other Dementias
Population Bulletin Vol. 60, No. 1 2005www.prb.org

22
Fries and others in the 1980s.28
Projections of future burdens of ill-ness depend on which of two contrast-ing scenarios may hold true. In thefirst, average life expectancy at birthincreases, but the average age atwhich a person becomes chronicallyill does not. In the second scenario,life expectancy increases, and theaverage age of the onset of chronic ill-ness also rises.
In the extreme, chronic illnessoccurs only in the final years or evenmonths of life. This extreme scenariois known as the compression of morbidi-ty. Data from the United States lendsome support to the compression ofmorbidity hypothesis: The rate ofchronic disability among olderAmericans declined between 1982and 1999, and there were 25 percentfewer chronically disabled olderAmericans than there would havebeen if the U.S. disability rate hadnot changed since 1982.29 If healthimproves alongside mortality (that is,if there is a compression of morbidi-ty), health and social welfare costswill be very different than they wouldbe if disability rates do not fall. Inmost countries, however, the shortageof data on disability across time, onsocial groups, and by generation andage greatly hamper attempts to
understand the causal factors thatunderlie these changes.
The Global Burden ofDisease In a landmark study in the 1990s, theWHO, World Bank, and HarvardUniversity attempted to estimate thecurrent and future global burden ofmajor diseases. This Global Burden ofDisease project has been extended tolook at the burden of disease andaging.30 Earlier results from the studyindicate that, between 1990 and 2020,the leading causes of disease burdenin the world as a whole will shift fromlower respiratory conditions, diar-rhoeal diseases, and perinatal condi-tions to ischemic heart disease, unipo-lar major depression, and road trafficaccidents (see Table 3). The study alsoprojects that cerebrovascular diseasewill make its way up the list, and thatHIV will reach the top 10 leading caus-es of disease burden by 2020. Thesetrends—especially the increasedimpact of mortality and morbidityfrom HIV/AIDS—will have importantimplications for older people and theirfamilies (see Box 4).
While the Global Burden of Diseasestudy has attracted criticism, it hasclearly prompted a valuable analysis of
Population Bulletin Vol. 60, No. 1 2005 www.prb.org
Table 3Ten Leading Sources of the Global Burden of Disease, 1990 and 2020
Rank 1990 Disease or injury 2020 Disease or injury
1 Lower respiratory infections Ischemic heart disease2 Diarrhoeal diseases Unipolar major depression3 Conditions arising during the perinatal period Road traffic accidents4 Unipolar major depression Cerebrovascular disease5 Ischemic heart disease Chronic obstructive pulmonary disease6 Cerebrovascular disease Lower respiratory infections7 Tuberculosis Tuberculosis8 Measles War9 Road traffic accidents Diarrhoeal diseases10 Congenital anomalies HIV/AIDS
Note: These estimates of disease burden as measured by disability-adjusted life years are from the Global Burden of DiseaseStudy conducted by the World Health Organization, the World Bank, and Harvard University in the 1990s. Many countries andagencies have modified the study methodology; further refinements are being tested in a project spearheaded by the HarvardUniversity Burden of Disease Unit. More information is available at www.hsph.harvard.edu/organizations/bdu/About.html.
Source: C.J.L. Murray and A.D. Lopez, eds., The Global Burden of Disease (1996).

disease factors and health systemresponses. One important componentof older people’ living standards ishealth care and its costs. As costs haveescalated in the past decade, a growingbody of research has focused on iden-tifying the costs of specific illnessesand on projecting health expendi-tures.31 The WHO’s World Health Report2002 was devoted to identifying, quan-tifying, and reducing disease risk fac-tors. Data from the EuropeanCommunity Household Panel Surveyin the 1990s began to shed light onthe interplay between health statusand the retirement decisions of olderEuropean couples. Several ongoingnational longitudinal studies, includ-
ing the Health and Retirement Studyin the United States and the EnglishLongitudinal Study of Ageing in theUnited Kingdom, also attempt to cap-ture the complexity of such transitionsand understand their significance forpolicy planning. Several other nationshave mounted similar longitudinalstudies to track these issues.
Gender and AgingWomen constitute a majority of theolder population in almost everycountry, and their majority increaseswith age. The gender imbalance atolder ages has many implications for
23
The World Health Organization (WHO) and the JointUnited Nations Programme on HIV/AIDS (UNAIDS)estimated that 18.8 million people had died of AIDSby 2001. Of these, 14.8 million were in sub-SaharanAfrica. An estimated 37 million people were livingwith HIV, and 95 percent of new infections wereoccurring in less developed countries.1 The risingAIDS toll and the consequent increasing numbers ofAIDS orphans worldwide are having far-reachinghealth, economic, and psychosocial impacts, particu-larly in Africa and increasingly in parts of Asia. Of the14 million children under age 15 who had lost theirmother or both parents to AIDS, about 90 percentlived in sub-Saharan Africa. The care and support ofHIV/AIDS patients often fall on older parents andgrandparents.
A study in Zimbabwe found that older people werethe main caregivers, either of the terminally ill or ofthe orphans whose parents had died of AIDS.2Caregivers faced a range of problems, including loss offinancial support; lack of food and clothing; limitedaccess to affordable health services; inability to payschool fees; diminished livelihood opportunities; andstigmatization of the disease (even from health person-nel). Similar findings have been reported in Uganda.3The Zimbabwean study found that the health of oldercaregivers had often suffered, with many under seriousphysical and emotional stress and suffering from physi-cal violence and abuse resulting from accusations ofwitchcraft. Respondents had many serious concerns, asvoiced by a 62-year-old woman, guardian of threegrandchildren: “I am so afraid of what the future hasin store for these orphans. If I were to die and leavethem, who would look after them?”
A 59-year-old woman in Mbare, Zimbabwe, whocared for her children before they died and now caresfor seven orphaned grandchildren, explained: “Theperson with AIDS is very sick and at times loses his/hermind. When this happens, it becomes impossible toprovide effective care, as the sick person may be abu-sive and violent.”
While HIV/AIDS now affects sub-Saharan Africadisproportionately, the epidemic is expected to placea heavy burden on older caregivers in a number ofAsian countries, including Thailand, India,Cambodia, China, and the Philippines. A Thai studyfound that two-thirds of adults who died fromHIV/AIDS lived with or had moved near their par-ents by the terminal stage of illness.4 Seventy percentof these adults received at least some care from aparent or other older-generation relative. Suchextensive involvement of older caregivers may serveas a model for planning public health programs inother less developed nations—targeting older peoplewith caretaker education and socioeconomic supportof people living with HIV.
References1. Peter Lamptey et al., “Facing the HIV/AIDS Pandemic,”
Population Bulletin 57, no. 3 (2002). 2. World Health Organization (WHO), Impact of AIDS on
Older People in Africa: Zimbabwe Case Study (Geneva: WHO,2002).
3. Alun Williams and Grace Tumwekwase, “MultipleImpacts of the HIV/AIDS Epidemic on the Aged inRural Uganda,” Journal of Cross-Cultural Gerontology 16, no.3 (2001): 221-36.
4. John Knodel et al., “Older People and AIDS:Quantitative Evidence of the Impact in Thailand,” SocialScience and Medicine 52, no. 9 (2001): 1313-27.
Box 4The Impact of HIV/AIDS on Older People in the Less Developed World: African andAsian Examples
Population Bulletin Vol. 60, No. 1 2005www.prb.org

24
population and individual aging, per-haps most important with regard tomarital status and living arrange-ments. Family members are the mainsource of emotional and economicsupport for older people in less devel-oped countries, although some gov-ernments have assumed a larger shareof the economic responsibilities.
The primary reason there are manymore women than men at older ages isthat men have higher death rates thanwomen at all ages. Although about 105boys are born per 100 girls in mostpopulations, women usually begin tooutnumber men between ages 30 and40. The female numerical advantageincreases with age. A precise explana-tion of why women live longer thanmen still eludes scientists because itinvolves the complex interplay of bio-logical, social, and behavioral condi-tions. Greater exposure of males torisk factors such as tobacco and alco-hol use and occupational hazards iscited as one source of higher malemortality rates. If this is true, the gapin life expectancy should have nar-rowed as women increased their use oftobacco and alcohol and their partici-pation in the labor force. Data fromindustrialized countries still show noclear pattern of change. The gendergap is widening in much of easternEurope and the former Soviet Union,while it is narrowing in most othercountries. In the United States, for
example, life expectancy at birthincreased 4.4 years for males and 2.3years for females between 1980 and2002, narrowing the gender gap from7.5 to 5.4 years. But in some nationswith high overall life expectancy (forexample Japan, Greece, and Iceland),gains in female longevity continue tooutpace those of males.
Sex Ratios In most countries of the world, theratio of men to women at older agesis well below 100. Ukraine’s sex ratioof 50 men per 100 women ages 65and older is an extreme example,partly attributable to the lingeringeffects of high male mortality duringWorld War II. More developed coun-tries tend to have lower sex ratiosamong their older populations thando less developed countries, reflect-ing the wider gender differentials inlife expectancies at birth in moredeveloped countries (see Table 4).
In the future, sex ratios at olderages are projected to move in oppo-site directions in the more developedand less developed regions. Theseratios are expected to increase in thenext few decades in many industrial-ized countries as their life expectancygender gap narrows. The oppositetrend is anticipated in less developedcountries. Given the small averagegender gap in life expectancy in lessdeveloped countries relative to moredeveloped nations, most demogra-phers expect to see a widening of thefemale/male difference in upcomingdecades, along the lines of the histori-cal trend in industrialized nations.Many less developed countries areexperiencing increases in alcohol andtobacco consumption and vehicularand industrial accidents—all of whichtend, at least initially, to adverselyaffect men more than women.
Education is also related to thegender gap. As women “catch up” tomen in terms of educational attain-ment, female survival and health sta-tus may improve.32 Regardless of theprojected trends, women are expect-ed to make up the majority of the
Population Bulletin Vol. 60, No. 1 2005 www.prb.org
Table 4Sex Ratio for People Age 65 or Older in 20 Countries, 2004
More developed countries Less developed countries
Australia 79 Bangladesh 117Bulgaria 72 Brazil 70France 69 Ethiopia 84Germany 68 Fiji 85Italy 71 Ghana 89Poland 62 Honduras 90Russia 46 India 103Ukraine 51 Iran 98United Kingdom 74 Mexico 84United States 71 Zambia 79
Note: The sex ratio reflects the number of men per 100 women in the 65-and-older age group.
Source: U.S. Census Bureau, International Data Base (www.census.gov/ipc/www/idbnew.html, accessed Dec. 12, 2004).

world’s older population throughoutthe 21st century. Continuing or grow-ing disparities in sex ratios mean thatmany of the challenges and problemsfaced by older people of today andtomorrow are, in essence, challengesand problems faced by older women.
Marital StatusMarried people, particularly marriedmen, enjoy healthier and longer livesthan their unmarried counterparts. Arecent study of the U.S. noninstitution-alized population found that marriedadults were healthier than unmarriedadults within every population group(including age, sex, race, or ethnicgroups) and within groups with similarhealth indicators (whether they weresmokers, disabled, or physically inac-tive, for example). The only negativehealth indicator for which marriedadults had a higher prevalence wasbeing overweight or obese.33
Older married couples also tend tobe more financially secure thanunmarried people. Married older peo-ple are less likely to enter a nursinghome because their spouses are oftenavailable to care for them in case of ill-ness or disability. Changes in maritalstatus at older ages can affect pensionpotential, retirement income, and an
individual’s social support network;older widowed men, in particular, maylose contact with much of their sup-port network after their wives die. Bycontrast, widowed women tend tomaintain their support network afterthe death of a spouse. In almost everysociety, older men are likely to be mar-ried and older women are likely to bewidowed. For both men and women,the proportion married decreases witholder age and the proportion widowedincreases (see Figure 6).
Gender differences in marital sta-tus reflect the interplay of several fac-tors. First and most obvious is the sexdifference in longevity: Women livelonger than men. Second, womentend to marry men older than them-selves which, combined with the sexdifference in life expectancy, increas-es the chance that a woman’s hus-band will die before she does.Furthermore, older widowed menhave higher remarriage rates thanolder widowed women in many coun-tries, often as a function of culturalnorms.34 Thus, women are more like-ly than men to lose their spouse andless likely to remarry if they are wid-owed. This preponderance of singlewomen in older ages has importanteconomic consequences for individu-als and societies. Longitudinal data
25
Source: Compiled by the U.S. Census Bureau from national sources.
Figure 6Percent Widowed Among Older Australians, Malaysians, and Croatians, Circa 2000
Population Bulletin Vol. 60, No. 1 2005www.prb.org

26
from Germany and the United Stateshave revealed that, although thepoverty rate is lower in Germany thanin the United States, women in bothnations tend to experience a declinein living standards when they becomewidows, and many fall into povertybecause they lose their husband’spension support.35
Changes in Marriage andChildbearingGlobally, the share of older men andwomen who are married hasincreased slightly and the proportionwho are widowed has decreased dur-ing the past 30 years. Much of thischange is attributable to improvedjoint survival of husbands and wives.In most countries relatively few olderpeople have never married: 5 percentor fewer older men and 10 percent orfewer women. The percentages aresomewhat higher in parts of Europe,where World War II deaths shrank thepool of potential husbands whentoday’s older women were of primemarriage age. Above-average propor-tions of older people in several LatinAmerican and Caribbean nations alsoare never married, but this largelyreflects the prevalence of consensualunions in those societies. While thecategory “consensual union” is widelyused in census tabulations in thesecountries, some people who are living(or who have lived) in a consensualunion are likely to report themselvesas never married.
In most countries, a relatively smallproportion of older people aredivorced, because divorce was lesssocially acceptable for this earlier gen-eration. The number and percentageof older divorcees will increase asyounger cohorts with higher divorcerates reach older age.36 In the UnitedStates, for example, 9 percent of peo-ple ages 65 and older were divorcedor separated in 2003, compared with17 percent of people 55 to 64 and 19percent people 45 to 54. The chang-ing marital composition of the olderpopulation as these younger cohortsreach age 65 will affect the nature
and types of support services thatboth families and governments mayneed to provide.37
Increases in childlessness will alsoaffect future caregiving demands forolder people. In the United States, forexample, the likelihood of beingchildless among women ages 40 to 44nearly doubled between 1980 and2000 (from 10 percent to 19 percent).Childlessness is common in Europe,and is increasing in Latin Americaand Southeast Asia. Some childless-ness is involuntary, occurring becauseof marital disruption, birth limitationpolicies, or infecundity, loss of chil-dren to HIV/AIDS or other healthproblems. But increasingly, people arechoosing not to have any children,reflecting lower marriage rates andcultural changes that make childless-ness more socially acceptable. Becausechildren often provide support fortheir parents, trends in childlessnesswill be an important determinant offuture elder-care arrangements.
Educational DifferencesWhile literacy has increased through-out the world, many older people,particularly women and the oldestold, grew up with few educationalopportunities. In some less devel-oped countries, the vast majority ofolder residents, particularly women,are illiterate.
In some more developed coun-tries, younger cohorts are more thantwice as likely as older people to havecompleted secondary education. Inless developed countries, the differ-ence between younger and oldercohorts is even more striking. The lat-est census data for Bolivia indicate,for example, that women ages 25 to44 were more than five times as likelyas women age 65 or older to havecompleted secondary education.
Younger women in many countriesnow complete secondary education athigher rates than do men, and insome nations young women areabout as likely as young men toattend college.38 Thus, the disadvan-tages that older women face because
Population Bulletin Vol. 60, No. 1 2005 www.prb.org

they have lower levels of educationthan men should abate as today’solder populations are replaced bymore educated cohorts.
While older people in the futurewill be more educated, the highlevel of illiteracy among today’solder population perpetuates manysocial and economic disadvantages.A lack of written proof of age, forexample, often is enough to barolder people from defending theirrights to property.39
IntergenerationalRelationshipsIntergenerational relationships strictlyrefer to interactions and relationshipsbetween parents, children, grandpar-ents, and grandchildren at themicrosocial level. Within families,intergenerational relations often deter-mine the willingness and even the abil-ity of families to provide care and sup-port for their older members. Theserelations also affect intergenerationaltransfers of wealth. Intergenerationalrelations are codified in some soci-eties, especially in Asia, with reciprocalduties between generations viewed as amutual obligation. These obligationsare most readily identified as filial piety and, in a more extreme form,ancestor worship.40
The expectation that people willcare for their older relatives is notunique to Asia; almost every societyhas a similar, if less formal, under-standing of the importance of familyrelations and the value of older peo-ple. While some social analysts suggestthat vertical family bonds—tyingtogether different generations—haveweakened over recent decades, thissuggestion has been refuted byresearch findings in many countries.41
Indeed, greater longevity actuallymakes bonds among adults moreimportant than in the past and, whiledirect contact between generationsmay have lessened, indirect contactsare as strong as ever. A heated debatehas emerged in many countries about
the so-called “decline of the family.”Some sociologists argue the family hasbeen stripped down to its bare essen-tials: just two generations and twofunctions (childbearing and financialand emotional support for nuclearfamily members). Other analysts arguethat, while families have changed overthe last century, population aging hasactually extended families across gen-erations and expanded their supportfunctions over longer periods.42
Intergenerational relations can beviewed along two axes: solidarity andconflict. Most studies have focused onthe solidarity component, which isassumed to remain strong even ifsocial factors such as smaller familysize, high residential mobility, andurbanization make intergenerationalbonds more difficult to maintain.Researchers recognize various positiveaspects of social and familial cohesion,interaction, and sentiment associatedwith solidarity. Conflict in intergenera-tional relations has been less thor-oughly studied, but research suggeststhat families alternate between conflictand competition during some periodsand stability, order, and cooperationduring other periods.
Family StructureThe nature of family life and inter-generational relations stronglydepends on the structure of a family:whether one has a spouse, children,grandchildren, siblings, or survivingparents or grandparents. As seen ear-lier, many women worldwide have ahusband or partner until their 60s,when they become widows. Mostolder people have children and manyhave grandchildren. As many as 80percent also have siblings, althoughthis percentage is steadily dropping asfamily size is falling. In countries withvery low birth rates, future genera-tions of adults and older people willhave few if any siblings.
The picture of the nuclear familythat stays together through life is stillthe norm in most countries, but thisnorm is changing. Among the baby-boom generation in the West, there is
27
A majority ofolder people inmany countries
are illiterate.
Population Bulletin Vol. 60, No. 1 2005www.prb.org

28
a wide variety of family forms andlifestyles, reflecting rising rates ofdivorce and remarriage, delayed mar-riage, and increasing percentages ofnever-married and childless adults aswell as greater labor force participa-tion among women.
The global trend toward fewer chil-dren means fewer potential caregiversfor older parents. The word “poten-tial” is important, because simulationsof future support scenarios haveshown that fertility decline alone isnot likely to result in the collapse of atraditional support system.43 Addedyears of life prolong relationshipswith others: parents, grandparents,children, and grandchildren. In 2000,a 50-year-old American had an esti-mated 80 percent chance of having atleast one parent alive and a 27 per-cent chance of having both alive.44
Living ArrangementsLiving arrangements take on specialimportance with regard to older peo-ple, because living arrangementsreflect both the nature of accommo-dation required and the need forcommunity or institutional long-termcare. Living arrangements oftenreflect sociocultural preferences—forexample, a preference for living innuclear-family households versus liv-ing in an extended-family house-hold—or the propensity of society toallow, encourage, and support institu-tionalization of older people. Livingarrangements also reflect the desireand ability of many older people tolive independently.
Large proportions of older peoplelive alone in many industrialized coun-tries. Well over one-third live alone inSweden, the United Kingdom,Finland, and Denmark, and the pro-portion is higher in the oldest agegroups. Figure 7, based on Canadiancensus data, demonstrates how theincrease in the number of older peo-ple living alone has largely been fueledby women. Older-person-only house-holds (especially unmarried women)are increasingly common. In theUnited Kingdom, for example, about
15 percent of all households in the1990s were single pensioners livingalone. However, the most common“older household” in many Westerncountries consists of two older people.In a comparison of 13 European coun-tries in the 1990s, between 29 percentand 45 percent of all older peoplelived with another person age 65 orolder.45 The Berlin Aging Study, whichlooks at people in West Berlin age 70or older, found that almost 62 percentwere living alone in the 1990s, 25 per-cent lived with a spouse or partner,and 8 percent lived in nursing homesor other institutional arrangements.Among those age 85 or older, the lat-ter figure was 19 percent.46
At one time, living alone wasthought to indicate social isolation orfamily abandonment of older people.However, research in more developedcountries consistently shows thatolder people prefer to reside in theirown homes and communities, even ifthat means living alone. The growthof households consisting of one olderperson has been fueled by a combina-tion of factors: greater longevity;increases in benefits and pensions; ris-ing home ownership levels; moreelder-friendly housing; greateremphasis on care in the community;increased availability of communitysupport; and reduced public financ-ing for living in nursing homes.
Multigenerational households havebeen declining in more developedcountries, but two- and three-genera-tion households are still the norm inmany less developed countries. Moststudies in less developed countriesindicate that older people want to livewith their children or at least close tothem. A four-country review of livingarrangements and support for olderpeople in Southeast Asia found thatbetween 69 percent and 85 percent ofpeople age 60 or older in those coun-tries lived with their children in themid-1990s, although the percentagehad declined slightly since the 1980sin at least three of the countries.47
The percentages who were livingalone or with a spouse only weresmall—6 percent or less. But many
Population Bulletin Vol. 60, No. 1 2005 www.prb.org

older people who lived apart fromtheir children often lived close by andsaw them on a daily basis. The four-country study concluded that theenormous socioeconomic changes inthe region over the past few decadeshave not yet significantly affected tra-ditional living arrangements.However, changes are becoming evi-dent in East Asian countries such asHong Kong, China, Korea, and Japan,where significant numbers of olderpeople live alone and the share livingwith children is falling rapidly (seeFigure 8).
In patrilineal systems such asfound in northern Vietnam, an olderparent is much more likely to livewith a married son than with a mar-ried daughter. The reverse is true inthe Philippines and Thailand, wherethe parent would be more likely tolive with a married daughter than amarried son.
Although older people in lessdeveloped countries appear to havestrong family support, several trendsconcern social scientists. The firsttrend relates to specific groups suchas unmarried older women or widowswithout any children, who can be leftwith little support and nowhere to liveif extended family members will nottake them in. The changing house-
hold structures and living arrange-ments in high HIV/AIDS-prevalenceareas can leave many orphans depen-dent on older grandparents. Somesocial scientists are also concernedabout the effects of urbanization andmodernization on family life—withsome worried that these changes willundermine traditional family supportsystems for older people.48
29
Source: Statistics Canada, national census data.
Figure 7Older Canadians Living Alone, 1961 to 2001
*Includes small numbers living in unspecified arrangements.
Sources: M. Atoh, “Who Takes Care of Children and the Elderly in an Aging Society?” (October 1998); andJapan National Institute of Population and Social Security Research, “Housing With Seniors: 1975–-2010”(www.jinjapan.org/insight/html/focus10/page08.html, accessed March 13, 2003).
Figure 8Living Arrangements of Older Japanese, 1960 to 2010
Population Bulletin Vol. 60, No. 1 2005www.prb.org

30
Long-term care (LTC) for olderpeople has become a key issuethroughout the world. LTC involves arange of support mechanisms, includ-ing nursing and assistance in thehome, various forms of communitycare and day care, residential care, andlong-stay hospitals and similar institu-tions.49 Western societies have movedaway from institutional residential careexcept when absolutely necessary formedical or social reasons. One recentstudy of 10 European nations suggest-ed that the share of older people inresidential care ranged from justunder 4 percent in Germany to morethan 9 percent in Denmark andNorway.50 On average, about 6 percentof older people in the more developedworld live in residential care communi-ties and nursing homes at any point intime, although a much higher percent-age of older people may expect tospend some time in an institutionalsetting before they die.
Aging in place and care in the commu-nity have become watch-phrases forpolicy in many countries. These con-cepts imply that older people shouldbe able to live in their own homes orin small institutions as long as possi-ble and that, while institutional careshould be available when necessary, itshould be a last resort. Care in thecommunity and aging in place mayremain key policy levers if more olderpeople live longer and healthier lives.However, these options require thatappropriate social and medical sup-port are available in the communityfor older people and their familiesand that residential settings and localenvironments are designed to accom-modate the special needs of peoplewith limited physical functioning andmobility. Too often, these designaspects are neglected in planning andrequire considerable expense toinstall retrospectively.
CaregivingCaregiving is usually characterized aseither formal or informal, althoughthe distinction between the two can attimes be artificial. Formal care or sup-
port generally comes from paid pro-fessionals and public and private ser-vices set up specifically to provide aservice such as home nursing, homehelp, or counseling. Some services—such as meals-on-wheels programs forhouse-bound older people—are for-mally organized but often deliveredpartly by volunteers, making theseprograms a combination of formaland informal support. Informal care iscare provided by relatives, friends,and neighbors to older people andtheir families. Much informal care isprovided by other older people, andis instrumental (such as help withcooking, cleaning, and shopping);personal (help with eating or toilet-ing); and emotional (personal visitsand communication). Such care isextremely important but difficult toquantify because many activities maynot be recognized by the giver orreceiver as “support” or “care.” Familymembers are the major providers ofinformal support: daughters anddaughters-in-law are often the primarycaregivers. Today, however, increasingjoint survivorship at older ages meansthat the spouse (usually the wife)rather than an adult daughter often isthe primary informal caregiver. Whilemany older people receive financialand other support from adult chil-dren, support often is reciprocal. Incountries with well-established pen-sion programs, many older adults givesupport and care to their childrenand grandchildren. Older people inless developed countries are less likelyto provide financial help to youngerpeople, but often contribute signifi-cantly to family well-being in manyways, ranging from socialization tohousekeeping to child care.
Work, Retirement,and Well-BeingNo set of issues has galvanized publicdiscourse about aging more thanthose surrounding work, retirement,and economic security in old age. Ineastern Europe’s transitional
Population Bulletin Vol. 60, No. 1 2005 www.prb.org
Wealthiercountries tend to have muchlower labor forceparticipationamong olderresidents.

economies, and indeed in much ofthe less developed world, govern-ments increasingly seek to define abalance between public and privatesocial security systems. The precari-ousness of old-age security can beseen in stagnant and declining realpensions in transitional economies, inthe dire fate of pensioners during thecollapse of Argentina’s economy in2001, in the surprisingly high povertyrates among older Japanese, and per-haps most vividly in the lack of socialsafety nets for a majority of older peo-ple in Africa and Asia.
Labor Force ParticipationLabor force participation declineswith age, especially after age 50, butwork patterns for older people varyamong and within countries (see Box5, page 30). Older people in moredeveloped countries are generally lesslikely to work than those in less devel-oped countries. Only 2 percent ofmen age 65 or older participate inthe labor force in some more devel-oped countries, whereas more thanone-half are economically active incertain less developed countries.National differences in labor forceactivity are associated with societalwealth: Wealthier countries tend tohave much lower labor force partici-pation rates among older residentsthan do low-income countries.51
Labor force participation rates forolder men declined in more devel-oped countries in recent decades.One compilation of data for 16nations showed especially pro-nounced declines in participation formen in their early 60s. In the early1970s, well over half of men ages 60to 64 were still working in a majorityof countries. By the late 1990s, onlyfour of the 16 countries—Japan, NewZealand, Sweden, and the UnitedStates—had male participation ratesover 50 percent in this age group.52
Labor force participation rates fellbelow 10 percent among the 65-and-older age group in most of the coun-tries. Financial incentives for earlyretirement have enabled many older
workers to leave the labor force. Also,new technologies have increased thevalue of a recently trained labor forcerelative to older workers. And incountries with persistently highunemployment, older workers may bepressured to leave the labor force tomake room for younger workers.
The decline in labor force participa-tion among older workers may havehalted. A report from the Organisationfor Economic Cooperation andDevelopment (OECD) found a slightincrease in employment rates for menin their late 50s and early 60s in thelate 1990s in the United States and theNetherlands, and a cessation of thelong-term decline in several otherOECD countries. The report suggeststhat the increase was related to an eco-nomic upturn in the late 1990s.53
Older women have had differentlabor force patterns than older men.In many industrialized countries,female participation rates haveincreased for almost all adult agegroups up to age 60. The increase wassharp in some countries. In NewZealand, for example, 60 percent ofwomen ages 55 to 59 were economi-cally active in 1998, up from 28 per-cent in 1971. While female participa-tion was increasing at younger ages,nearly all more developed countriessaw a decrease among older womenbetween the early 1970s and the late1990s. Small proportions (typically 4percent or less) of older women areeconomically active in more devel-oped nations.
Older men and women in lessdeveloped countries are much morelikely to work than those in industrial-ized nations. Older people in predomi-nantly rural agrarian societies oftenwork out of necessity—retirement maybe a luxury reserved for urban elites.In nations as diverse as Bangladesh,Indonesia, Jamaica, Mexico, Pakistan,and Zimbabwe, more than 50 percentof all older men are considered eco-nomically active. The economic activityof women tends to be underreported,particularly in less developed countrieswhere much of the work that womenengage in is not captured in censuses
31Population Bulletin Vol. 60, No. 1 2005www.prb.org

Population Bulletin Vol. 60, No. 1 2005 www.prb.org32
In more developed countries, retirement from theworkforce occurred almost exclusively at a regulatedage until the 1950s; older workers had little possibilityof receiving a pension prior to the designated retire-ment age. Since then, countries have adopted a widerange of approaches to providing old age security, andpeople have a wider array of routes to retirement.
Part-time work is one option that appeals to manyolder workers because it enables them to remainactive in the labor force while pursuing leisure activi-ties. But the opportunities for part-time work varytremendously among countries. In nine more devel-oped countries, the prevalence of part-time employ-ment among working men ages 60 to 64 ranged fromless than 8 percent in Italy and Germany to more than35 percent in Sweden and the Netherlands.1
Older working women are much more likely thanolder men to be involved in part-time work. InAustralia, three-fourths of women ages 65 and olderwho were economically active in 1999 worked part-time, compared with fewer than half of economicallyactive older men. A study of 15 European Unioncountries showed that 41 percent of working womenages 55 to 64 were in part-time positions in 1998,compared with just 8 percent of working men in thatage group.2 The rate of part-time work for peoplenearing retirement generally was increasing in the1990s. However, part-time workers often represent asmall fraction of the older population.
Disability programs have provided another path toretirement for older workers. Economic recessionsand high unemployment in Europe in recent decadesled some governments (including Germany, theNetherlands, and Sweden) to enable early retirementvia relaxed disability criteria and generous long-termsickness benefits. Wide variations in national pro-grams produced enormous differences in retirement
patterns; among 16 European countries in the mid-1990s, the percentage of older retired men whoretired because of illness or disability ranged from 2percent in Portugal to 29 percent in Switzerland.
Unemployment also has been seen as a bridge toretirement. Older workers typically have low levels ofunemployment compared with younger workers, butif older workers become unemployed, they tend toremain unemployed longer than younger workers.OECD data for several wealthy countries show thatwell over half of unemployed people age 55 or olderwere unemployed for more than one year. Many enterthe ranks of “discouraged workers,” people who areno longer looking for work because they think there isno work available or because they do not know whereto look. In some countries, older workers may feelexcluded from the labor force because of changes inoccupational structure and the need for a more-edu-cated workforce that favors younger workers.
One comparison of 13 countries indicated thatpeople ages 55 to 64 accounted for a disproportionateshare of discouraged workers, especially in the UnitedKingdom, where more than two-thirds of all discour-aged male workers were ages 55 to 64. In countrieswith trend data, discouraged older workers were morenumerous in the 1990s than in the 1980s. Because ofthe difficulties older people face in obtaining a newjob, discouragement often becomes a transition fromunemployment to retirement.
References1. Organisation for Economic Cooperation and
Development (OECD), Reforms for an Ageing Society (Paris:OECD, 2000).
2. Statistical Office of the European Communities (EURO-STAT), The Social Situation in the European Union 2000(Luxembourg: EUROSTAT, 2000).
Box 5The Transition to Retirement
and labor force surveys, or is not con-sidered economic activity. Olderwomen in less developed societies, forexample, often are involved in subsis-tence agriculture or household indus-tries, neither of which is well docu-mented by conventional data collec-tion methods.
Most older workers in less devel-oped countries work in agriculture.Agriculture remains a major employ-er of older people, even in manymore-developed countries. In 1995 inJapan, one-third of all older workerswere engaged in agriculture. Data for23 OECD countries show that the
ratio of workers age 55 or older toworkers below age 55 is generallymuch higher in agriculture, hunting,and forestry than in any other goods-producing or service sector.54
Retirement SystemsPublic pension systems developedlargely because families found itincreasingly difficult to support theirolder and infirm relatives. Just 33countries had old age, disability, andsurvivors programs in 1940, comparedwith more than 165 countries in 2000.In response to general economic con-

ditions, changes in welfare philosophy,and private pension trends over thepast several decades, many industrial-ized nations lowered the age at whichpeople become fully entitled to publicpension benefits. The proliferation ofearly retirement schemes has increasedthe number and usually the propor-tion of older workers who take advan-tage of such programs.
CoverageMandatory old-age pension plans nowcover more than 90 percent of thelabor force in most industrializedcountries. Governments are responsi-ble for mandating, financing, manag-ing, and insuring public pensions.Public pension plans usually offerbenefits that are not tied to individualcontributions, but are financed bypayroll taxes. This arrangement iscommonly referred to as a “pay-as-you-go” system because taxes on work-ing adults finance the pension pay-ments of people who are retired.
Most pay-as-you-go systems in indus-trialized countries initially promisedgenerous benefits. When first estab-lished, these programs were based ona small number of pensioners relativeto a large number of contributors(workers). As systems matured, ratiosof pensioners to contributors grewand in some countries became unsus-tainable, particularly during periodsof economic stagnation. One resultwas the development of private pen-sion systems to complement public sys-tems. Other measures implementedor considered have included increas-ing worker contribution rates, restruc-turing or reducing benefits, and rais-ing the minimum age of retirement.55
In less developed countries, publicpension systems typically cover a muchsmaller fraction of workers. Even eco-nomically vibrant societies such asMalaysia and Thailand offer no pub-licly supported, comprehensive retire-ment pension scheme. Governmentsthat do offer coverage often restrict itto certain workers such as civil ser-vants, military personnel, and employ-ees in the formal economic sector.Rural, predominantly agricultural
workers have little or no pension cov-erage in much of the less developedworld, although some governmentshave taken steps to address this situa-tion.56 Each state in India, for example,has implemented an old-age pensionscheme for destitute people with nosource of income and no family sup-port. In addition to these stateschemes, the Indian government hasdeveloped a means-tested NationalSocial Assistance Programme thatseeks to provide uniformly availablesocial protection throughout the coun-try. While pension amounts are mini-mal and coverage far from universal,the system provides a foundation onwhich to expand future coverage.
Informal (usually family) systemsprovide the bulk of social support forolder individuals in many countries,particularly in Africa and South Asia.As economies expand and nationsurbanize, informal support systems,such as extended family care andmutual aid societies, have tended toweaken. Expanding the older popula-tion served by formal systems whilemaintaining the existing informalsupport mechanisms has become amajor challenge for governments inless developed nations.
Pension ReformA number of factors have convergedto make pension reform a contentiouspolitical issue. Increased longevity andearly retirement mean that demo-graphic change alone could doubleretiree–worker ratios in many coun-tries over the next 30 years.Economists have expressed concernsabout declining savings rates, whilepoliticians and the general publichave been reluctant to embraceincreased payroll taxes and higherretirement ages.57 With the cost ofpublic pensions absorbing upwards of15 percent of GDP in some countries,there is an emerging consensus thatpension systems should be revampedto rely less on traditional public-bene-fit formulas and to require more fromprivate accounts and individual-work-er savings.58 During the last decade,dozens of books and monographs
33Population Bulletin Vol. 60, No. 1 2005www.prb.org

34
have debated the often-complex fiscalpros and cons of privatization. Therealso are strong philosophical (somewould say ethical) aspects to thedebate. Proponents of privatizationseek to promote individual responsi-bility and reduce the role of govern-ment. Other analysts stress that tradi-tional public pension systems aresocial insurance programs based onthe notion of collective responsibility.Beyond the rhetoric, two facts standout: First, traditional public programsare not set in stone and are periodical-ly reformed to resolve legislatedfinancing problems. Second, there isnevertheless a clear trend toward pri-vatizing public systems. Approximately30 nations have privatized at least aportion of their public systems, andprivatization has been more commonin countries with well-developed pub-lic systems that cover a large percent-age of workers.
Privatization of pensions can takemany forms, and it can coexist withstrong public programs. One progres-sive idea, developed by the Switzer-land-based Geneva Association, pro-motes the concept of Four Pillars ofSupport. In many countries, pensionfunding rests on two or three pillars: apublic pension based on pay-as-you-gofunding; a supplemental or mandato-ry occupational pension (common insome European nations) that often isfully funded; and individual savings,which may include personal invest-ments and life insurance. The GenevaAssociation proposes a fourth pillarbased on a new design for retirementthat encourages continued economicactivity (either full-time or part-time)by older people, and incorporates theconcept of gradual retirement insteadof early retirement.59 Crossnationalresearch on labor force participationat older ages has shown that levels ofparticipation are a consequence(intended or unintended) of retire-ment provisions and/or tax policy.60
The financial structure of nationalsocial security systems may rewardearly retirement, and attempts toencourage increased labor force par-ticipation at older ages may be largely
contingent upon politically difficultchanges in these systems.
Successful AgingAging is not merely a matter of accu-mulating years but also, as a popularcatch-phrase states, a process of“adding life to years, not years to life.”People grow old in a social and eco-nomic context that affects their psy-chosocial development: their feelingsof self-esteem, value, and place infamily and society. These factors havea combined effect on the morale ofolder people, and a number of mod-els have been developed to explainwhy some people remain more activeand healthier at older ages than otherpeople. These are generalized modelsand cannot account for differences inthe genetic makeup of individuals,although the models can identify fac-tors that favor healthy lifestyles andways in which a society can assist itsmembers to grow old with dignity andcomfort. Underpinning these con-cepts or models are several decades ofstudy by gerontologists who haveoffered a number of social theories ofaging (see Box 6).
The concept of successful aging hasrecently attracted a great deal of poli-cy and research attention and is relat-ed to the broad issues of coping andadaptation in later life. Growing num-bers of older people do not exhibitthe chronic health problems anddeclining cognitive skills that wereassumed to accompany aging.Successful aging is viewed as maximiz-ing desired outcomes and minimizingundesired ones. As demonstrated inthe Berlin Aging Study, adaptation isa key component to successful aging:Older adults can compensate for loss-es and declines and retain the poten-tial for further growth. Aging expertsJohn Rowe and Robert Kahn view suc-cessful aging as the confluence ofthree functions: decreasing the risk ofdiseases and disease-related disability;maintaining physical and mentalfunctioning; and being activelyengaged with life (see Figure 9, page34).61 There is debate, however, about
Population Bulletin Vol. 60, No. 1 2005 www.prb.org

35
Theory building—the cumulative developmentof explanation and understanding of observa-tions and findings—lies at the core of scientificinquiry and knowledge. In areas such as socialgerontology, social theories are essential forproviding coherent and valid bases for policies,programs, and activities. Social theories arenot proved or disproved; rather, they representa cumulative and evolutionary understandingas parts of the explanations are better under-stood, improved, or rejected.
Role theory is one of the oldest socialgerontological theories, dating back to the1940s.1 Individuals play a variety of roles dur-ing their lives—child, adult, spouse, parent,employer, employee, grandparent, retiree.Roles are often sequential, some are concur-rent, and individuals lose and gain rolesthroughout life. Chronological age oftendetermines some changes (such as attainingvoting age or retirement age), but agenorms—assumptions that people should door cease certain activities at certain ages—underpin much of role theory. Some roleimages and changes can be challenged legally(such as formal retirement ages) or by publicperceptions (older people as athletes, astro-nauts, entertainers, and other positiveimages).
Activity theory (from the 1960s) suggeststhat older people who take on a large numberand variety of activities and roles will have amore positive older age, adjust to aging better,and be more satisfied with their lives.2 Activitytheory tends to promote old age as a socialproblem or issue that individuals can tackle. Adiffering perspective to this was disengagementtheory, which found a mutual withdrawalbetween the older person and society.3Disengagement theory sees society withdraw-ing from the aging person as much as theolder person withdrawing from society, anddisengagement is viewed as adaptive behavior.Assumptions about disengagement of olderpeople—which was seen by some as unavoid-able and universal—have prompted muchdebate, research, and modification.
Continuity theory holds that middle-agedand older adults often attempt to preserveties with their own past experiences by substi-tuting new roles that are similar to lost ones.4The theory suggests that people are most sat-isfied in their older years when their newroles and activities are consistent with previ-ous experiences. This approach tends to
emphasize individual behavior and neglectsthe societal constraints that deter older peo-ple from continuing some activities, but itnevertheless looks positively at continuationof activities such as sports, religion, reading,or teaching.
While these theories have been sometimesportrayed as challenging one another, theyalso represent an evolution of understandingof aging and the place of older people in soci-ety. A number of alternative and additionaltheories have focused on the interactionbetween an individual and the environment.5The subculture of aging theory views olderpeople as maintaining their self-concepts andidentities through membership in socialgroups. Subcultures might form within politi-cal, religious, and professional groups, or from“membership” that accrues from living in, say,a retirement home or retirement community.Within such potentially closed communities,residents may act and behave in collective waysthat perhaps they would not do if living in thewider community.
Other more general theories such as mod-ernization theory discuss negative effects onthe roles and status of older people if theirknowledge, traits, and skills are deemed lessrelevant or valuable as modernization pro-ceeds. Exchange theory helps explain whymost older people, in spite of reducedresources, seek to maintain some degree ofreciprocity while remaining independent andactive. Feminist gerontology criticizes the male-centered views inherent in much theory onaging, even though older people are predomi-nantly women.6
References 1. Leonard S. Cottrell, “The Adjustment of the
Individual to His Age and Sex Roles,” AmericanSociological Review 7 (1942): 617-20.
2. Cary S. Kart and Jennifer M. Kinney, The Realitiesof Aging: An Introduction to Gerontology (Boston:Allyn and Bacon, 2001).
3. Elaine Cumming and William E. Henry, GrowingOld (New York: Basic Books, 1961).
4. Robert C. Atchley, The Social Forces in Later Life(Belmont, CA: Wadsworth, 1972); and Robert C.Atchely, “A Continuity Theory of Normal Aging,”The Gerontologist 29, no. 2 (1989): 183-90.
5. Nancy R. Hooyman and H. Asuman Kiyak, SocialGerontology: A Multidisciplinary Perspective, 6th ed.(Boston: Allyn and Bacon, 2002).
6. Robert J. Lynott and Patricia Passuth Lynott,“Tracing the Course of Theoretical Developmentin the Sociology of Aging,” The Gerontologist 36, no.6 (1996): 749-60.
Box 6Social Theories of Aging
Population Bulletin Vol. 60, No. 1 2005www.prb.org

Population Bulletin Vol. 60, No. 1 2005 www.prb.org
how those who age successfully differfrom others and about the role ofexternal factors in the process.62
In addition to successful aging, con-cepts such as productive aging (the abil-ity to contribute directly and indirectlyin older age) and healthy aging (theability to remain physically and men-tally fit) have been identified. Theseconcepts come together in the WHO’spolicy framework of active aging devel-oped between the late 1990s and2002.63 The word “active” refers tocontinuing participation in social, eco-nomic, cultural, spiritual, and civicaffairs, not just being physically or eco-nomically active. Active aging encom-passes those who have retired as wellas people who are frail, disabled, or inneed of care; and it takes place withina broad social context of friends, fami-ly, neighbors, associates, and the work-place. Active aging recognizes theUN’s principles of independence, par-ticipation, dignity, care and self-fulfill-ment. It shifts strategic planning awayfrom a needs-based approach (whichimplies older people are passive recip-ients) to a rights-based approach ofequality and opportunity. The WHOadvocates a life-course approach toactive aging that recognizes older peo-ple not as a homogeneous group butas individuals who, collectively, are asdiverse as younger members of a soci-
ety. The strategy promotes supportiveenvironments and fosters healthy lifechoices at all stages of life. Finally, itrecognizes that a collective approachto aging and older people will ulti-mately determine how we and ourchildren and grandchildren experi-ence life in later years.
Longer-Term ViewIn most countries, but especiallythose in less developed regions, eco-nomic growth remains the priority;social considerations take a back seat.While economic development mayultimately increase the ability of coun-tries to support older people, devel-opment and population aging inter-act in numerous ways.
The UN Economic and SocialCommission for Asia and the Pacificelaborated these interactions in 1999when it sponsored the first aging anddevelopment plan for a less devel-oped region, the Macau Plan ofAction on Ageing for Asia and thePacific.64 The plan explicitly notesthat population aging tends toincrease fiscal demands on govern-ments, especially for income support,health, and social services. In addi-tion, the urbanization that almostalways accompanies developmenttends to reduce traditional supportnetworks for older people at the sametime that labor markets have decreas-ing demand for the skills and experi-ence of older workers. The agingcohorts in many less developed coun-tries are an interim generation: Theyare reaching retirement age beforegaining sufficient personal savingsand pensions and at the same time astheir traditional family support maybe withering.65 In this sense, popula-tion aging can reduce the savingsavailable for national investment.Some economists from more devel-oped regions fear that the financialburden of pensions and long-termcare for expanding retired popula-tions may reduce the ability to investoverseas and buy industrial goodsfrom less developed countries.
Avoidanceof diseaseand disability
Involvementin society
High cognitive andphysical function
Successfulaging
Source: Adapted from J.W. Rowe and R.L. Kahn,The Gerontologist 37, no. 4 (1997): 433–40.
Figure 9Model of Successful Aging
36

Demographic aging has become aglobal development issue. Economists,however, may be overly pessimistic.Family systems of care have provedvery resilient worldwide and, with amodicum of formal help, may contin-ue to support older relatives fordecades. Shoring up family systemswould entail reorienting investmenttoward training and long-term careassistance, but it could ultimately buildmore supportive societies.66 Anotherfactor that could ease the financialburden of aging is the incorporationof pension needs in the developmentstrategies of international donor orga-nizations. Less developed countriesthat provide even a minimal pensionto a significant portion of their olderpopulation have demonstrated thatpensions can ameliorate poverty.67 Therising demand for imported labor inthe richer, demographically stagnantcountries is another potential sourceof support for older people in lessdeveloped countries. While suchdemand may induce a brain drainfrom less developed nations, it wouldalso generate an increasing flow ofremittances to older individuals. Thereare other development opportunitiesthat aging populations can create, notthe least of which is in parts of Asiacalled the “silver market,” the demandfor goods and services by older peoplethemselves.
Aging and NationalSecurity The profound shifts in age structurearound the world have prompted areexamination of strategic and eco-nomic thinking about national securi-ty. Countries that are growing slowly(or not at all) are experiencingdeclines in the size of their youngerpopulations. While most of thesenations have shifted from manpower-intensive to capital-intensive armedforces, some analysts are concernedabout the future size and demographicprofile of defense forces. Countrieswith high fertility rates, in contrast,have a surplus of youth. Large armiesare a source of employment as well as
national strength, and countries at anearlier level of demographic transitionare potentially destabilizing forces notonly vis-à-vis immediate neighbors butto the world as a whole.68
The more worrisome long-termsecurity scenarios involve wideningbudget deficits in more developedcountries. There is concern that high-er spending on social programs willincrease interest rates and crowd outprivate investment. Some analystsargue that, as populations stabilize ordecline, the shrinking numbers ofworkers and consumers may reducenational GDP growth, asset values, sav-ings rates, and currency values.Consequently, tax revenues and thevalues of mortgage-backed securitieswill decline in some countries, withripple effects throughout the world.The OECD, the InternationalMonetary Fund (IMF), the EuropeanCommission, and other groups havestudied the influence of aging on theeconomy. While the studies have dif-ferent approaches and emphases, theshared conclusion is that economicgrowth will slow as populations age.69
Global Capital FlowsWhether population decline and slow-er economic growth are twin evils forsocial well-being is debatable andbeyond the scope of this report. The“doom and gloom” scenarios of agingpainted by some analysts are coun-tered by optimistic assessments fromother analysts. A sustained rise in pro-ductivity, for example, could offsetmany of the fiscal negatives men-tioned above. If, as some claim, econ-omists know very little about howtechnological change occurs, then theeffects of aging populations on tech-nological innovation are unknown.70
Considering the broader picture, ana-lysts have begun to examine theimplications of population aging forglobal capital flows. By the late 1990s,the aging Japanese society hadbecome the world’s largest exporterof capital.71 Simulations suggest thatthere will be substantial capital flowsfrom rapidly aging countries such as
37Population Bulletin Vol. 60, No. 1 2005www.prb.org

38
Italy and Germany to the rest of theworld in the near future, althoughthe long-term impact of such flowsremains unclear.72
Looking further down the road,IMF simulations foresee a turningpoint between 2010 and 2030, whenEurope and North America becomecapital importers of flows from today’sless developed regions.73 If retiredbaby boomers in wealthier countriesdecide to sell off their stocks andother assets as they age, standard eco-nomic theory predicts that the priceof such assets will fall. Someobservers, however, believe that“younger” countries will step in andabsorb any sell-off. Countries in less-advanced stages of the demographictransition have large segments oftheir populations in the prime work-ing ages, with the potential for highlevels of economic output and sav-ings. Depending on the economic cli-mate, this “demographic dividend”has the potential to fuel growth andcapital accumulation, as it did in partsof Asia during prior decades.74
Will Living StandardsImprove? Given the maturation of public pen-sions systems, increased female laborforce participation, and the expand-ed private pension schemes in indus-trialized nations, older citizens inthese countries would be expected tobe better off economically than previ-ous generations of older people.Indeed, the OECD has concludedthat the economic picture for olderpeople has been stable or improvedin recent decades, both in absoluteterms and relative to younger popula-tion groups. Poverty rates for olderpeople have declined in mostnations, as has the share of olderpeople among the poor.
In the United States, real medianhousehold income (adjusted forhousehold size) improved muchmore for older people than for thegeneral population. And povertyamong people age 65 or older hasdeclined. One-third of all older U.S.
citizens were below the poverty line in1960; by the mid-1990s, just 10 per-cent were below poverty, lower thanthe rate for children.75
There is a growing perception insome countries that the older popula-tion is faring better than other agegroups. However, the complexity ofmeasuring economic well-being oftenprecludes a definitive assessment, andthere is considerable concern aboutthe willingness and ability of house-holds to adequately save for retire-ment needs.76 The ongoingLuxembourg Income Study revealssubstantial variation among countriesin poverty rates at older ages. Onecomparison of nine countries foundthat Canada, Germany, and Hungaryprovided their older residents withbetter overall protection from povertythan the other six countries. Theseoverall figures may mask large disad-vantages for specific groups withincountries—in particular, for olderwomen living alone.77
Age WavesIn spite of inevitable changes in polit-ical regimes and economic uncertain-ty, forecasters must sometimes peerfar into the future. The U.S. SocialSecurity Administration makes popu-lation projections 75 years ahead; theInternational Institute for AppliedSystems Analysis looks to the year2100; and the UN Population Divisionnow produces population projectionsfor the next 300 years. While suchlong-range scenarios are likely to beconfounded by unforeseen events,they do provide broad planning tar-gets. Some demographers have usedlong-term projections to identify pat-terns of population aging and raisewarning flags about potential conse-quences. Demographer Ian Pool, forexample, argues that aging is not amonotonic transitional process, butrather the outcome of complex agestructural mutations that vary bycountry. By plotting the changing sizeof different age groups between 1950and 2050, Pool paints a picture ofdouble or multiple population waves
Population Bulletin Vol. 60, No. 1 2005 www.prb.org

that result not just from declining fer-tility rates, but from the timing of lowfertility (for example, during theGreat Depression, the World Wars,and the baby bust following the babyboom), from resurgences in fertilityduring baby booms and baby-boomechoes, and from the effects of trendsin migration and survival.78
The inexorable momentum ofpopulation aging around the worldwill likely become the most significantdemographic process of the 21st cen-tury. Continuing shifts in populationage structure will require new socialsensitivities and innovative policy
responses. Demographic aging hasimplications for a wide range ofhuman behavior, and researchersincreasingly recognize the need formultidisciplinary approaches to theaging process. Initiatives in NorthAmerica, Europe, and Asia that inte-grate several salient domains of peo-ple’s lives have created successfulprototypes for such interdisciplinarystudies. The next steps in understand-ing the aging phenomenon will comefrom a further integration of scientif-ic inquiry, combining ideas frombiodemography, genomics, psycholo-gy, and macroeconomics.
39
References1. Following United Nations usage, the terms “more developed,” “developed,” or “industrialized” include all
European and North American countries, along with Australia, New Zealand, and Japan. The terms “less devel-oped,” “developing,” or “nonindustrialized” refer to all other countries. While these broad categories commonlyare used for comparative purposes, they do not necessarily reflect developmental differences between nations.
2. United Nations (UN), World Population Ageing 1950-2050 (New York: UN, 2002).
3. Throughout this Population Bulletin, estimates and projections of population size and composition (unless otherwisenoted) come from the International Programs Center, Population Division, U.S. Census Bureau.
4. Zhou Yang, Edward C. Norton, and Sally C. Stearns, “Longevity and Health Care Expenditures: The Real ReasonsOlder People Spend More,” Journal of Gerontology: Social Sciences 58B, no. 1 (2003): S2-10.
5. James W. Vaupel and Bernard Jeune, “The Emergence and Proliferation of Centenarians,” in Exceptional Longevity:From Prehistory to the Present, ed. B. Jeune and J.W. Vaupel (Odense, Denmark: Odense University Press, 1995).
6. Hans-Peter Kohler, Francesco C. Billari, and Jose Antonio Ortega, “The Emergence of Lowest-Low Fertility inEurope During the 1990s,” Population and Development Review 28, no. 4 (2002): 641-80.
7. Ronald D. Lee, “The Formal Demography of Population Aging, Transfers, and the Economic Life Cycle,” inDemography of Aging, ed. Linda G. Martin and Samuel H. Preston (Washington, DC: National Academies Press,1994): 8-49.
8. Arjan Gjonka, Hilke Brockmann, and Heiner Maier, “Old-Age Mortality in Germany Prior to and AfterReunification,” Demographic Research 3, Article 1 (July 2000), accessed online at www.demographic-research.org/volumes/vol3/1/html/default.htm, on Dec. 27, 2004.
9. James W. Vaupel, “Demographic Analysis of Aging and Longevity,” American Economic Review 88, no. 2 (1998): 242-47.
10. Vaino Kannisto, Development of Oldest-Old Mortality, 1950-1990: Evidence From 28 Developed Countries (Odense,Denmark: Odense University Press, 1994).
11. John R. Wilmoth et al., “Increase in Maximum Life-Span in Sweden, 1861-1999,” Science 289 (Sept. 29, 2000): 2366-68; and Scott M. Lynch and J. Scott Brown, “Reconsidering Mortality Compression and Deceleration: AnAlternative Model of Mortality Rates,” Demography 38, no. 1 (2001): 79-95.
12. For a discussion and examination of these hypotheses, see Shiro Horiuchi and John R. Wilmoth, “Deceleration inthe Age Pattern of Mortality at Older Ages,” Demography 35, no. 4 (1998): 391-412.
13. S. Jay Olshansky, “On the Biodemography of Aging: A Review Essay,” Population and Development Review 24, no. 2(1998): 381-93; and Caleb E. Finch, James W. Vaupel, and Kevin Kinsella, eds., Cells and Surveys: Should BiologicalMeasures Be Included in Social Science Research? (Washington, DC: National Academies Press, 2001).
14. Thomas J. Moore, Lifespan (New York: Simon and Schuster, 1993); and James C. Riley, Rising Life Expectancy: A GlobalHistory (Cambridge, England: Cambridge University Press, 2001).
15. Peter G. Peterson, Gray Dawn: How the Coming Age Wave Will Transform America—and the World (New York: CrownPublishing Group, 2000).
16. A study of crosscountry and Russian household survey data found that alcohol consumption and stress (associatedwith a poor outlook for the future) were the most important determinants of life expectancy decline in Russia. SeeElizabeth Brainerd and David M. Cutler, “Autopsy on an Empire: Understanding Mortality in Russia and the
Population Bulletin Vol. 60, No. 1 2005www.prb.org

Former Soviet Union,” National Bureau of Economic Research Working Paper 10868 (October 2004), accessed online atwww.nber.org/papers/w10868, on Dec. 27, 2004.
17. Árpád Skrabski, Maria Kopp, and Ichiro Kawachi, “Social Capital in a Changing Society: Cross-SectionalAssociations With Middle-Aged Female and Male Mortality Rates,” Journal of Epidemiology and Community Health 57,no. 2 (2003): 114-19.
18. National Center for Health Statistics, Health, United States, 2002, accessed online atftp://ftp.cdc.gov/pub/Health_Statistics/NCHS/Publications/Health_US/hus02/, on March 8, 2003.
19. Ronald Skeldon, “Ageing of Rural Populations in South-East and East Asia,” in The World Ageing Situation: Exploringa Society for All Ages, ed. United Nations (UN) (New York: UN, 2001): 38-54.
20. Antonio Golini, “Possible Policy Responses to Population Ageing and Population Decline,” in UN PopulationDivision, United Nations Expert Group Meeting on Policy Responses to Population Ageing and Population Decline,ESA/P/WP.163 (New York: UN, 2000): 7/1-16.
21. Kevin McCracken and David R. Phillips, “International Demographic Transitions,” in Ageing and Place, ed. Gavin J.Andrews and David R. Phillips (London and New York: Routledge, 2005): 36-60; Hong Kong, SARS in Hong Kong:From Experience to Action: Report of the SARS Expert Committee (Hong Kong: Government of the Hong Kong SpecialAdministrative Region, 2003); and Hong Kong Hospital Authority, unpublished data, June 2003.
22. Eric Barbotte et al., “Prevalence of Impairments, Disabilities, Handicaps and Quality of Life in the GeneralPopulation: A Review of Recent Literature,” Bulletin of the World Health Organization 79, no. 11 (2001): 1047-55.
23. Gerda G. Fillenbaum, “Activities of Daily Living,” in The Encyclopedia of Aging, ed. George L. Maddox (New York:Springer, 1995): 7-9.
24. Paul B. Baltes and Karl Ulrich Mayer, eds., The Berlin Aging Study: Aging From 70-100 (Cambridge, England:Cambridge University Press, 1999).
25. Michael G. Marmot and James Y. Nazroo, “Social Inequalities in Health in an Ageing Population,” European Review9, no. 4 (2001): 445-60.
26. Jean-Marie Robine et al., Determining Health Expectancies (New York: Wiley, 2002). See also www.revesnetwork.net foradditional information.
27. Vicki A. Freedman, Linda G. Martin, and Robert F. Schoeni, “Recent Trends in Disability and Functioning AmongOlder Adults in the United States,” Journal of the American Medical Association 288, no. 24 (2002): 3137-46.
28. James F. Fries, “The Compression of Morbidity: Near or Far?” Milbank Quarterly 67, no. 2 (1989): 208-32.
29. Kenneth G. Manton and XiLaing Gu, “Changes in the Prevalence of Chronic Disability in the United States Blackand Nonblack Population Above Age 65 From 1982 to 1999,” Proceedings of the National Academy of Sciences 98, no. 11(2001): 6354-59.
30. Joshua A. Salomon and Christopher J. Murray, “The Epidemiologic Transition Revisited: Compositional Models forCauses of Death by Age and Sex,” Population and Development Review 28, no. 2 (2002): 205-28.
31. Organisation for Economic Co-Operation and Development (OECD), Study on Cross-National Differences of Ageing-Related Diseases, June 2002 workshop, accessed online at www.oecd.org, on Jan. 26, 2005; and Stephane Jacobzoneand Howard Oxley, “Aging and Health Care Costs,” International Politics and Society 2002, no. 1, accessed online atwww.fes.de/ipg/ONLINE2_2002/INDEXE.HTM, on March 6, 2003.
32. Albert I. Hermalin, “Capturing Change: Transitions at Older Ages and Cohort Succession,” in The Well-Being of theElderly in Asia: A Four-Country Comparative Study, ed. Albert I. Hermalin (Ann Arbor, MI: University of MichiganPress, 2002): 519-41.
33. Charlotte A. Schoenborn, “Marital Status and Health: United States, 1999-2002,” Advance Data From Vital and HealthStatistics 351 (Dec. 15, 2004).
34. Maria Cattell, “African Widows, Culture and Social Change: Case Studies from Kenya,” in The Cultural Context ofAging, 2d ed., ed. Jay Sokolovsky (Westport, CT: Greenwood, 1997): 71-98.
35. Thomas L. Hungerford, “The Economic Consequences of Widowhood on Elderly Women in the United States andGermany,” The Gerontologist 41, no. 1 (2001): 103-10.
36. Jenny de Jong Gierveld, “Gender and Well-Being: The Elderly in the Industrialized World,” paper prepared for theInternational Union for the Scientific Study of Population Seminar on Population Ageing in the IndustrializedCountries: Challenges and Responses, Tokyo, March 19-21, 2001.
37. Lilian E. Pezzin and Barbara Steinberg Schone, “Parental Marital Disruption and Intergenerational Transfers: AnAnalysis of Lone Elderly Parents and Their Children,” Demography 36, no. 3 (1999): 287-97.
38. UN Educational, Scientific and Cultural Organization (UNESCO), “Education Statistics,” accessed online athttp://portal.unesco.org/uis, on Feb. 22, 2003.
39. HelpAge International, State of the World’s Older People 2002 (London: HelpAge International, 2002).
40. Anita C.Y. Ng, David R. Phillips, and William K.M. Lee, “Persistence and Challenges to Filial Piety and InformalSupport of Older Persons in a Modern Chinese Society: A Case Study in Tuen Mun, Hong Kong,” Journal of AgingStudies 16, no. 1 (2002): 1-20.
40

41
41. Cary S. Kart and Jennifer M. Kinney, The Realities of Aging: An Introduction to Gerontology, 6th ed. (Boston: Allyn andBacon, 2001).
42. Vern L. Bengtson et al., “Families and Intergenerational Relationships in Aging Societies,” Hallym InternationalJournal of Aging 2, no. 1 (2000): 3-10.
43. Zachary Zimmer and Julia Kwong, “Family Size and Support of Older Adults in Urban and Rural China: CurrentEffects and Future Implications,” Demography 40, no. 1 (2003): 23-44.
44. Nancy R. Hooyman and H. Asuman Kiyak, Social Gerontology: A Multidisciplinary Perspective, 6th ed. (Boston: Allynand Bacon, 2002).
45. Statistical Office of the European Communities (EUROSTAT), Population, Households, and Dwellings in Europe, MainResults of the 1990/1991 Censuses (Luxembourg: EUROSTAT, 1996).
46. Baltes and Mayer, “The Berlin Aging Study.”
47. John Knodel and Nibhon Debavalaya, “Living Arrangements and Support Among the Elderly in South-East Asia:An Introduction,” Asia-Pacific Population Journal 12, no. 4 (1997): 5-16.
48. Chuks J. Mba, “Determinants of Living Arrangements of Lesotho’s Elderly Female Population,” Journal ofInternational Women’s Studies 3, no. 2 (2002), accessed online atwww.bridgew.edu/SoAS/jiws/June02/aginglesotho.pdf, on Jan. 29, 2005.
49. David R. Phillips, ed., Ageing in the Asia-Pacific Region (London: Routledge, 2000).
50. Estimates may vary according to national definitions of institutions. See Mary Jo Gibson, Steven R. Gregory, andSheel M. Pandya, “Long-Term Care in Developed Nations: A Brief Overview,” AARP Public Policy Institute, October2003, accessed online at http://research.aarp.org/health/2003_13_ltc_dv.html, on Jan. 28, 2005.
51. Robert L. Clark, Elizabeth Anne York, and Richard Anker, “Retirement and Economic Development: AnInternational Analysis,” in Social Policy and the Labour Market, ed. Philip R. De Jong and Theodore R. Marmor(Brookfield, VT: Ashgate, 1997): 117-46.
52. Kevin Kinsella and Victoria A. Velkoff, An Aging World: 2001 (Washington, DC: Government Printing Office, 2001).
53. Organisation for Economic Co-Operation and Development (OECD), Reforms for an Ageing Society (Paris: OECD, 2000).
54. OECD, Employment Outlook 2000 (Paris: OECD, 2000).
55. Robert Holzmann and Joseph E. Stiglitz, eds., New Ideas About Old Age Security: Towards Sustainable Pension Systems inthe 21 Century (Washington, DC: The World Bank, 2001).
56. HelpAge International, Age and Security (London: HelpAge International, 2004).
57. Barry Bosworth and Gary Burtless, eds., Aging Societies: The Global Dimension (Washington, DC: Brookings InstitutionPress, 1998).
58. Robert Palacios and Montserrat Pallares-Miralles, “International Patterns of Pension Provision,” Social ProtectionDiscussion Paper, no. 9 (Washington, DC: The World Bank, 2000).
59. The Geneva Association, “The Four Pillars Research Programme 1987-2002” (June 2002), accessed online atwww.genevaassociation.org, on Dec. 12, 2004.
60. Jonathan Gruber and David Wise, eds., Social Security and Retirement Around the World (Chicago: University ofChicago Press, 1999).
61. John W. Rowe and Robert L. Kahn, Successful Aging: The MacArthur Foundation Study (New York: Pantheon, 1998).
62. Douglas D. Friedrich, Successful Aging (Springfield, IL: Charles C. Thomas, 2001).
63. WHO, Active Ageing: A Policy Framework (2002), accessed online atwww.who.int/hpr/ageing/ActiveAgeingPolicyFrame.pdf, on Jan. 26, 2005.
64. United Nations, The Macau Plan of Action on Ageing for Asia and the Pacific, accessed online at www.unescap.org/ageing/macau.htm, on Nov. 12, 2004.
65. Phillips, Ageing in the Asia-Pacific Region.
66. David R. Phillips and Alfred C.M. Chan, eds., Ageing and Long-Term Care (Singapore: Institute of Southeast AsianStudies; and Ottawa: International Development Research Centre, 2002).
67. HelpAge International, State of the World’s Older People 2002 (London: HelpAge International, 2002).
68. Brian Nichiporuk, The Security of Demographic Factors (Santa Monica, CA: RAND, 2000).
69. Robert Stowe England, The Macroeconomic Impact of Global Aging: A New Era of Economic Frailty? (Washington, DC:CSIS Press, 2002); and Pension Research Council (PRC) of the Wharton School, University of Pennsylvania, “RiskManagement for Global Aging: Perspectives on the Challenges Facing Industrialized Countries,” PRC Working Paper2003-1 (2003).
70. Alan Greenspan, Statement to the U.S. Senate Special Committee on Aging, in Global Aging: Opportunity or Threatfor the U.S. Economy? Serial No. 108-4, Feb. 27, 2003 (Washington, DC: U.S. Government Printing Office, 2003).
71. Center for Strategic and International Studies (CSIS) and Watson Wyatt Worldwide, Global Aging: The Challenge ofthe New Millennium (Washington, DC: CSIS and Watson Wyatt Worldwide, 2000).

72. Axel Boersch-Supan, Alexander Ludwig, and Joachim Winter, “Aging and International Capital Flows,” in Aging,Financial Markets and Monetary Policy, ed. Alan Auerbach and Heinz Hermann (Heidelberg, Germany: Springer,2002): 55-83. See also Axel Boersch-Supan, “Global Aging: Issues, Answers, More Questions,” University of MichiganRetirement Research Center Working Paper WP-2004-084 (June 2004).
73. Robin Brooks, “Population Aging and Global Capital Flows in a Parallel Universe,” IMF Staff Papers 50, no. 2(2003).
74. David E. Bloom, David Canning, and Jaypee Sevilla, The Demographic Dividend: A New Perspective on the EconomicConsequences of Population Change (Santa Monica, CA: RAND, 2003).
75. Robert B. Friedland and Laura Summer, Demography Is Not Destiny (Washington, DC: National Academy on an AgingSociety, 1999).
76. F. Landis MacKellar, “The Predicament of Population Aging: A Review Essay,” Population and Development Review 26,no. 2 (2000): 365-97.
77. Peter Saunders and Timothy M. Smeeding, “How Do the Elderly in Taiwan Fare Cross-Nationally? Evidence fromthe Luxembourg Income Study Project,” SPRC Discussion Paper 81 (University of New South Wales Social PolicyResearch Centre, April 1998), accessed online at www.sprc.unsw.edu.au/dp/dp081.pdf, on Dec. 27, 2004.
78. Ian Pool, “Age-Structure in Industrialized Countries,” in Ageing and Age-Structural Transitions in IndustrializedCountries, ed. Naohiro Ogawa et al. (Oxford, England: Clarendon Press, forthcoming).
42
Suggested ResourcesBaltes, Paul B., and Karl Ulrich Mayer. The Berlin Aging Study: Aging From 70 to 100. Cambridge, England: Cambridge
University Press, 1999.
HelpAge International. State of the World’s Older People 2002. London: HelpAge International, 2002.
Hermalin, Albert I., ed. The Well-Being of the Elderly in Asia: A Four-Country Comparative Study. Ann Arbor, MI: University ofMichigan Press, 2002.
Hooyman, Nancy, and H. Asuman Kiyak. Social Gerontology: A Multidisciplinary Perspective, 6th ed. Boston: Allyn andBacon, 2002.
Lloyd-Sherlock, Peter, ed. Living Longer. London: Zed Books, 2004.
National Research Council. Preparing for an Aging World: The Case for Cross-National Research. Washington, DC: NationalAcademies Press, 2001.
Olshanksy, Stuart Jay, and Bruce A. Carnes. The Quest for Immortality: Science at the Frontiers of Aging. New York: W.W.Norton, 2001.
United Nations Population Division. World Population Ageing 1950-2050. New York: United Nations, 2002.
WebsitesAsia-Pacific Institute of Ageing Studies, Lingnan University, Hong Kong
www.ln.edu.hk/apias/
International Network on Healthy Life Expectancy (REVES)www.prw.le.ac.uk/reves/
U.S. Census Bureau, International Data Basewww.census.gov/ipc/www/idbnew.html
United Nations Second World Assembly on Ageing (and Follow-up)www.un.org/esa/socdev/ageing/waa/
World Health Organization Ageing and Life Course Programmewww.who.int/hpr/ageing/index.htm

Transitions in World Population,by Population Reference Bureau Staff, 2004This Population Bulletin chronicles changes in worldpopulation in the last century, with a particularfocus on the last 50 years. It examines the social andeconomic factors that affect population change,including wide disparities in income, education, andwomen’s status within countries. It also discusses theheightened international concern since the 1950sabout rapid population growth, widespread fertilitydeclines, and the new world consensus reached in the 1990s about howbest to respond to population trends. BUL59.1 ($7.00)
Disability in America,by Vicki A. Freedman, Linda G. Martin, and Robert F. Schoeni, 2004This Population Bulletin provides a broad overview of disability inAmerica in the 21st century. It reviews basic concepts and measures ofdisability and shows recent U.S. trends on the demography of disability.This report also defines support systems and supportive living environ-ments for disabled individuals, and it describes current federal pro-grams and policies pertaining to those with disabilities. BUL59.3 ($7.00)
Women of Our World, 2005 Datasheet,by Lori Ashford and Donna Clifton, 2005The situation of women around the world is gainingprominence in national and international policydebates. The last half-century has seen major gainsin women’s health, education, and rights, butprogress has been slow or uneven in many areas.Disparities between men and women are still pro-nounced in the poorest regions and countries of theworld. This Population Reference Bureau data sheetpresents indicators of women’s status and progress in nearly 180 coun-tries, with a focus on demography, reproductive health, education, work,and public life. IDS05WWENG ($4.50)
Improving the Health of the World’s Poorest Peopleby Dara Carr, 2004For the more than 1 billion people living on less than $1 a day—one ofevery six people worldwide—health services and modern medicines areout of reach. And many initiatives that tried to improve the health ofpeople in extreme poverty have failed. This report discusses the rich-poor health divide and the cultural and political barriers to betterhealth for all. IMPROHEA ($7.00)
Recent Population Bulletins
Volume 60 (2005)No. 1 Global Aging: The Challenge of Success, by Kevin Kinsella and David R. Phillips
Volume 59 (2004)No. 4 America’s Military Population, by David R. Segal and Mady WechslerSegal
No. 3 Disability in America, by Vicki A. Freedman, Linda G. Martin, and Robert F. Schoeni
No. 2 China’s Population: New Trends and Challenges, by Nancy E. Riley
No. 1 Transitions in World Population, by Population ReferenceBureau Staff
Volume 58 (2003)No. 4 Population: A Lively Introduction, 4th ed., by Joseph A. McFalls Jr.
No. 3 Critical Links: Population,Health, and the Environment, by Roger-Mark De Souza, John S.Williams, and Frederick A.B. Meyerson
No. 2 Immigration: Shaping andReshaping America, by Philip Martin and Elizabeth Midgley
No. 1 Population Dynamics in Latin America, by Jorge A. Brea
Volume 57 (2002)No. 4 What Drives U.S. PopulationGrowth? by Mary M. Kent and Mark Mather
No. 3 Facing the HIV/AIDS Pandemic, by Peter Lamptey, MerywenWigley, Dara Carr, and Yvette Collymore
No. 2 Poverty in America: BeyondWelfare Reform, by Daniel T. Lichterand Martha L. Crowley
No. 1 International Migration: Facing the Challenge, by Philip Martinand Jonas Widgren
Visit www.prb.org for more information on population trends.
To order PRB publications (discounts available):Population Reference Bureau1875 Connecticut Ave., NW, Suite 520Washington, DC 20009Phone: 800-877-9881Fax: 202-328-3937E-mail: [email protected]: www.prb.org
Related PRB Publications

Population Reference Bureau1875 Connecticut Avenue, NW, Suite 520Washington, DC 20009-5728202-483-1100www.prb.org
Global Aging: The Challenge of SuccessPopulations are growing older in countries throughout the world. While populationaging can be celebrated as a human success story, rapid and widespread aging ispart of a demographic transformation that will affect the health and developmentof all nations. This report looks at the health, labor force participation, family status, and other characteristics of older people, as well as recent demographictrends and the projected growth of the older population in major world regions.
C E L E B R A T I N G 7 5 Y E A R S • 1 9 2 9 - 2 0 0 4POPULATION REFERENCE BUREAU