GIT j club gastropariesis16.
40
Kurdistan Board GEH/GIT Surgery J Club Supervised by: Professor Dr.Mohamed Alshekhani. MBChB-CABM-FRCP-EBGH.
-
Upload
shaikhani -
Category
Health & Medicine
-
view
99 -
download
0
Transcript of GIT j club gastropariesis16.

Kurdistan Board GEH/GIT Surgery J ClubSupervised by:
Professor Dr.Mohamed Alshekhani.MBChB-CABM-FRCP-EBGH.

MAIN FUNCTIONS OF STOMACH
I. PROXIMALFunctions: Accommodation
Storage of ingested food Regulation of intragastric
pressure Tonic movement of chyme
Motor Pattern: Tonic activity
II. DISTALFunctions: Grinding of food
Emptying to duodenumMotor Pattern: Phasic activity

B3
Pacemaker region
Corpus
Fundus
Antrum
Pylorus
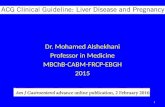
Pacemaker potentials determine contractile parametersContractile parameters
Max frequency (3/min)
Propagation velocityPropagation direction
Motility of the Antral Pump Is Initiated by a Dominant Pacemaker in the Mid-corpus
The antral pump is formed by the mid and distal corpus, antrum, and pylorus
Pacemakerpotential
B87

B4
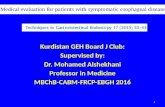
% Meal remaining in stomach
Lag phaseEmptying
phase
Onset and Rate of Gastric Emptying Varies With the Composition of the Meal
Time after meal (min)
Solid meal
Liquid meal
100
75
50
25
0200 6040 10080
Semisolid meal




Gastric emptying – evolving concepts
• Relationship with symptoms unclear
– NOT nausea, vomiting or pain– Accelerating gastric emptying does not
necessarily improve symptoms– Symptomatic improvement including weight gain
is possible without improving gastric emptying
Gastroparesis is frequently overdiagnosed on the basis of outdated emptying tests

Causes of Gastroparesis
• Idiopathic 36%
• Diabetic 29%
• Upper GI surgery 13%• Parkinson’s 8%
• Collagen tissue disorder 5%
• Intestinal pseudo-obstruction 4%
• Miscellaneous (Incl eating disorders) 6%
Soykan et al, DDS 1998; 43:2398-2404

Drugs that delay gastric emptying(Partial listing)
β AgonistsAnticholinergicsTricyclic agentsPhenothiazinesDopamine agonistsOpiatesProton pump inhibitorsMiscellaneous
Dexfenfluramine AntihistaminesLithium
TetrahydrocannabinolTobacco

Workup for suspected gastroparesis
UGI Series: Excludes mechanical obstruction Retention of barium w/o
obstruction is diagnostic
Endoscopy: Bezoar without obstruction highly suggestive
Gastric Emptying: Solids more sensitive than liquids

Normal values for low fat, egg white GES
Lower normal limit Upper normal limitTime for gastric retention* for gastric retention**
0.5 hr. 70%1.0 hr. 30% 90%2.0 hr. 60%4.0 hr. 10%
* Lower value suggests rapid emptying** Higher values suggest delayed emptying
Am J Gastroenterol 2008

2. A 30 y.o. woman with a one year history of type II diabetes mellitus presents with nausea and early satiety. Her blood sugars have been erratic and her last HBAIC was 9.2. Endoscopy was normal and a gastric emptying test showed 20% retention of the meal at 4 hours (normal < 10%).
Which of the following would you recommend:
• a) Metoclopramide
• b) Rigorous control of blood sugars
• c) Erythromycin
• d) Botulinum toxin injection of the pylorus

Slow gastric emptying was frequent in women with type 2 diabetes with hyperglycemia and normalized after diabetic control
J Diabetes & Complications, 2013

2. A 23 y.o. woman developed a viral illness associated with fever, myalgias, nausea, vomiting and diarrhea. Although most of her symptoms resolved over 2 weeks, she continued to have nausea, occasional retentive vomiting, early satiety and a 10 lb. weight loss. Endoscopy showed a modest amount of retained food in the stomach and a gastric retention of a test meal consisting of egg whites, toast and jam at 4 hours was 35% (normal <10%).
Which of the following would you recommend first?
a) Metoclopramide
b) Botulinum toxin injection (pylorus)
c) Erythromycin
d) Gastric stimulator

Management of Gastroparesis
Dietary ModificationsSmall frequent (6/day) mealsReduced fat (<40 gm/day)Soup, crackers, noodles, pasta,
potatoes, rice, cheeseReduced fiber helps avoid bezoarLiquid caloric supplementation

Prokinetic Agents
• ACh-esterase inhibitors: pyridostigmine
• Motilides: erythromycin
• Antidopamine agents: domperidone*
• Antidopamine/serotonin agents:• metoclopramide• Serotonin agents: tegaserod*, prucalopride*
*Not available in USA

ERYTHROMYCIN
• Motilin agonist• No antiemetic effect• Stimulates antral contractions
(IV >> PO)• Stimulates MMC• Dose: 125-250 mg bid/tid (PO) 3 mg/kg q 8 hours (IV)

Metoclopramide
• Central/peripheral D2 antagonist and 5 HT agonist• Increases antral contractions• Decreases fundal relaxation• Improves antroduodenal
coordination• Dose: 5-20 mg qid (PO, IV, SQ, SL)

Metoclopramide• 30% of patients experience side
effects• 10% have neurologic side effects
Parkinson-type syndromeTardive dyskinesia
• Hyperprolactinemia
* Boxed Warning for chronic use issued by FDA*

Domperidone
• Peripheral D2 antagonist• Increases antral contractions• Decreases fundal relaxation• Improves antroduodenal
coordination• Dose: 10-30 mg qid (PO)
Limited availability in USA

Efficacy of Domperidone in Diabetic Gastroparesis
□ Improved symptoms in 64%
□ Improved gastric emptying in 60%
□ Reduced hospital admission in 67%
□ 28 trials (19 double arm); 1016 patients
Sugumar A et al, CGH 2008

Effects of Botulinum Toxin on GE and GI Symptoms
Within Group Between Group P
Botox P Placebo P
Improved % 37.5 56.3 0.29
GCSI score -6.8 + 9.2 0.01 -10.1 + 12.7 0.01 0.42
GVAS score -190 + 228 0.01 -176 + 256 0.02 0.88
% Gastric retention 2 hr
-16.3 + 22.9 0.02 -10.8 + 20.6 0.08 0.52
% Gastric retention 4 hr
-13.3 + 18.0 0.01 -3.6 + 25.5 0.62 0.27
Friedenberg FK, et al. Am J Gastro 2008

3. A 28 y.o. man with IDDM is referred for chronic and recurrent nausea and vomiting. He reports 3-4 episodes yearly for the past 5 years with frequent ED visits or hospitalizations lasting 3-4 days. Between episodes, he feels well and has lost no weight. During these episodes, he finds great relief when taking hot showers.
The most appropriate intervention for this patient is:
• a) Domperidone 20 mg AC meals
• b) Nortriptyline in doses up to 100mg hs
• c) Discontinue smoking marijuana
• d) Strict control of blood sugars; metoclopramide 10 mg SQ during episodes

DD:Cyclic Vomiting Syndrome
Recurrent and stereotypical episodes of severe nausea and vomiting separated by symptom free intervals
- Gastric emptying rapid or normal- Maintenance of weight

DD:Cannabinoid Hyperemesis
- Cyclic vomiting syndrome
- Compulsive hot water bathing
- Poor response to TCAs

Cyclic Vomiting in Adults(Non-Cannabinoid)DD”
• Association with migraine headaches• Psychological disorders
(anxiety/depression)• Absence of compulsive hot water bathing• Often responds to TCAs

Physiology of gastric emptying:• Different meals are emptied at different rates, based on physical
consistency, fat content& total caloric load. • Liquids of low caloric density empty under the pressure gradient
between fundic tone & pylorus with little motor action of the distal stomach& liquids empty exponentially from the stomach.
• Higher caloric liquids or homogenized solids empty almost linearly under the pressure gradient from the fundus& coordinated antropyloroduodenal motility.
• Digestible food of more solid consistency requires antral trituration until the particle size is reduced to < 2 mm; after which , food empties linearly from the stomach at a rate similar to that of a homogenized solid meal.
• Trituration involves establishing liquid shearing forces where solids & liquids are repeatedly propelled against a closed pylorus at the maximum frequency of 3 / minute in humans.

Definition of gastric emptying:• Gastroparesis is a syndrome of significantly delayed gastric
emptying in the absence of mechanical obstruction&cardinal symptoms of early satiety, postprandial fullness, nausea, vomiting, bloating&upper abdominal pain.
• Diabetes, postsurgical, post-viral or idiopathic are the most common associated conditions
• Extrinsic neurologic disorders as parkinsonism, paraneoplastic. • Scleroderma

Deranged mechanisms:• In gastroparesis, there is an abnormal function of smooth muscle,
enteric & extrinsic autonomic nerves, or the interstitial cells of Cajal (pacemakers in the stomach wall).
• The pathophysiological disturbances from diverse pathologic mechanisms seem to be uniform.
• Myopathic disorders are typically infiltrative diseases, such as scleroderma or amyloidosis; degenerative disorders, such as hollow visceral myopathy; or mitochondrial cytopathy.
• When these disorders cause gastroparesis, they invariably present as a more generalized motility disorder affecting other regions, such as the small bowel, esophagus, LES.
• Gastric emptying delay in gastroparesis is associated with distal antral hypomotility, pylorospasm, or intestinal dysmotility.

Deranged mechanisms:• Measurement of gastric emptying does not differentiate
neuropathic from myopathic disorders but requires appraisal for systemic, serologic, or biopsy of the underlying diseases (eg, scleroderma or mitochondrial cytopathy, Urine or SPE, fat or duodenal biopsy for amyloidosis) or, rarely, documentation of low-amplitude eso (typically < 30 mm Hg), LES resting pressure (typically < 20 mm Hg),15,16 antral (typically < 40 mm Hg), or duodenal (typically < 10 mm Hg) contr amplitude by manometry.
• Antral hypomoility is usually present when there is pylorospasm • Decreased PP antral motility index prolongs gastric emptying for
solids by prolonging the lag time & lowering post-lag emptying.• Intestinal dysmotility retards the gastric emptying, typically
without prolonging lag phase of gastric emptying. • Finding residual food in the stomach at the time of endoscopy
after a period of fasting may occur in patients with gastroparesis.

Diagnosis:• Gastric emptying by scintigraphy is still widely used.• Measurement Gastric emptying of low 2% fat Egg Beaters
(chicken egg white) or 30% fat, 320-kcal meal is gold standard.• Significant delay is documented by at least 10% retention at 4
hours with the EggBeaters meal&> 25% retention at 4 hours with the 320-kcal, 30% fat meal.
• FDA approved:• A.Wireless motility capsule, which detects gastric emptying time
at the point of care by identifying the sudden change in pH from entry into the duodenum.
• B. C13 isotope with solid meal &after emptied from stomach, digested & absorbed in the proximal SI, liver metabolized & excreted by lungs, resulting in rise in expired 13 CO2 over baseline, inaccurate in malabsorption, liver, or lung diseases; 80% specificity, 89% sensitivity compared with simultaneous scintigraphy&agreed with it 73%– 97% of the time.

Dietary recommendations:• Foods provoking symptoms;orange juice,fried chicken, cabbage,
oranges, sausage, pizza, peppers,onions, tomato juice, lettuce, coffee, salsa, broccoli, bacon, roast beef, were generally fatty, acidic, spicy,roughage-based.
• A high-fat solid meal significantly increased overall symptoms • Saltine crackers, Jell-O,graham crackers moderately improved
symptoms, and 12• Additional foods were tolerated without provoking symptoms;
ginger ale, gluten-free foods, tea,sweet potatoes, pretzels, white fi sh, clear soup, salmon,potatoes, white rice, popsicles, applesauce.
• A small particle size diet reduces upper gastrointestinal symptoms (nausea, vomiting, bloating, postprandial fullness, regurgitation, heartburn) in patients with diabetic gastroparesis

Standard medications:• The only approved drugs for treatment of gastroparesis target
dopamine D2 receptors; metoclopramide (a D2 -receptor antagonist with some 5-HT4 receptor agonism) & Domperidone.
• Tardive dyskinesia risk is overstimated.• Metochlopromide nasal spray, reduced symptoms of gastroparesis
in women, but not in men.• Domperidone risk of SCD from prolonged QT.• Motilin agonists; erythro,azithro & clarithro also prolong QT &
should not be combined with prokinetics.• Tachyphylaxis is a problem.• All should not be given for > 3 months.

Novel medications:• Novel Motilin Agonist : GSK962040 (or camicinal) is a small
molecule, selective motilin receptor agonist.• Ghrelin agonist; Relamorelin accelerated gastric half-emptying
time of solids in patients with type 2 or type 1 diabetes with delayed gastric emptying.
• New 5-HT4 Receptor Agonists: prucalopride; Velusetrag is a selective 5-HT4 receptor agonist, YKP10811 is a novel benzamide derivative, selective 5-HT4 receptor agonist.
• In nonobese diabetic mice phosphodiesterase 5 inhibitor, sildenafil reversed gastric emptying.

Intrapyloric Botox inj:• It directly inhibits smooth muscle contractility, as evidenced by a
decreased contractile response to acetylcholine.• Not approved yet.• It can improve gastric emptying & symptoms,> with 200-
unit,second inj, female,< 50 years& idiopathic cause.

Transpyloric FCMS:• Improvements in gastric emptying & clinical outcomes in 75% ,
with greater efficacy in predominant nausea/or vomiting (79%) rather than those with predominant pain (21%).

Gastric Per-Oral or lap Endo Myotomy:• Extended to include patients with gastroparesis secondary to
vagal injury.

Gastric Electrical Stimulation:• Approved for diabetic & idiopathic gastroparesis, for persistence
of symptoms despite antiemetic/prokinetics for at least 1 year. • NICE in 2014: current evidence is adequate to support its use.

Endoscopic GES implantation:• Temporary gastric stimulators placed endoscopically to
determine response to GES before permanent implantation• A novel, wirelessly powered miniature GES implanted into the pig
stomach through an overtube & attached to the gastric mucosa with endoclips needs validation in humans.