GI bleeding - cch.org.t lecture/medical/GIB.pdf · GI bleeding GI bleeding ... R’t side colon...
12
1 GI bleeding GI bleeding Term: Hematemesis : bloody vomitus Melena: tarry stool passage Maroon : tarry- bloody stool passage Hematochezia: bloody stool passage
Transcript of GI bleeding - cch.org.t lecture/medical/GIB.pdf · GI bleeding GI bleeding ... R’t side colon...

1
GI bleeding
GI bleedingTerm:Hematemesis : bloody vomitusMelena: tarry stool passageMaroon : tarry- bloody stool
passageHematochezia: bloody stool
passage

2
GI bleeding Bleeding > 5~10ml OB (+)Bleeding > 50~100ml tarry stool
Bleeding above Treitz lig. hematemesisBleeding above ileocecal valve tarry
stoolBleeding below ileocecal valve fresh
bloody stool1. R’t side colon blood mixed inside
the stool2. L’t side colon blood coated outside
the stool 3.rectosigmoid fresh bloody discharge
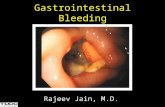
Common cause of acute UGI bleeding
Erosive, hemorrhagic gastropathy ( aspirin, other NSAIDs) (3~11%)Ulcer: Gastric or duodenal ulcer (35~62%)Mallory-Weiss tear (4~13%)Varices – portal hypertensive gastropathy(4~31%)Arteriovenous malformationMaligancy (1~4%)No source identified ( 7~25%)

3
Common cause of acute LGI bleeding
< 55 y/o1. Anorectal disease
( hemorrhoid, fissures)
2. Colitis (IBD, infection)
3. Diverticulosis4. Polys, cancer5. Angiodysplasia
> 55 y/o1. Anorectal disease
(hemorrhoid, fissures)2. Diverticulosis3. Angiodysplasia4. Polys, cancer5. Enterocolitic
(ischemic, infection, IBD, radiation)
Evaluated blood loss
>35%
20~35%
10~20%
0~10%
%
+ shock<60bpmSBP<90>1750
+oliguria>120bpm90<SBP<1201000~1750
Peripheral cool
<120bpmPosturehypotension
500~1000
NoneNo changeNo change0~500
S/SHRBPBlood loss (ml)

4
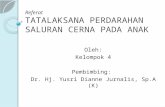
Peptic ulcerPhase of GU, DU
Active stage:A1: well-defined, deep ulceration;
marked bleeding from the ulcer base marginal welling
A2: stop bleedingHealing stage (H): H1,H2,H3Scarred stage (S): S1( red scar), S2(white scar)
Forrest Grade I

5
Forrest Grade IIA IIB
Forrest GradeIIC III

6
Peptic ulcerRisk of recurrent bleeding
SRH: stigmata of recent hemorrhageexposure vesselsadherent clotsarterial spurting or oozingEndoscopic therapyHSE (hypertonic saline and epinephrine),bipolar electrocoagulation, heat probe, hematoclip, APC
Risk factors > 60 y/o ageMore than one comorbid illnessBlood loss > 5 unitsShock on admissionBright-red hematemesis with hypotensionCoagulopathyLarge ( > 2cm) ulcerRecurrent hemorrrhage ( within 72 hrs)Requirement for emergency surgery

7
GI bleeding – goals of management
Hemodynamic stableActive bleeding stoppedRecurrent bleeding prevented
Hemodynamic stablePulse pressure > 30 mmHgSBP > 110 mmHgDBP > 70 mmHgHR < 100 bpmGood skin turgor

8
UGI bleeding -- managementRestoration of intravascular volumeHct: > 25% Hct: > 30% in cardiac or pulmonary dz
Vasopressors indicated ?Vol resuscitation end-pointCVP=15 mmHgWedge pressure = 10 to 12 mmHgBlood lactate < 4 mmol/ LBase deficit –3 to +3 mmol/LC.I. > 3L/min/m2
UGI bleeding -- managementO2 consumption ( V O2) = Q * Hb *
(SaO2-SvO2) Volume deficit = % loss * normal blood volumeMales – 70 ml / kg or 3.2 L/ M2
Females – 60 ml / kg or 2.9 L/ M2

9
UGI bleeding -- managementCorrection of coagulopathyInitial infusion: FFP 2~4 uProtamine infusion ( 1mg antagonizes
=100 u of heparin)Vit-K (10 mg,IM): warfarin, hepatobiliary
diseasePLT transfusion: > 50000/cummAirway protection
PUD-- treatmentAntacidsdrug interaction – Tetracyclines, Quinolone, ketoconazole,Peptic ulcer ( with evidence)
H2-blocker: Ranitidine (Zantac, Quicran)side effect: headache, lethargy, confusion,
depressiondrug interaction: Cimetidineβ-blockers, Metformin, Phenytoin, Procainamide,
Theophylline, TCA and Warfarin.

10
PUD -- treatmentPeptic ulcer ( with evidence)
PPIs: Omeprazole ( Losec)-- elder-- intractable bleeding-- combine with theophylline
Raise intragastric pH to 6~7Enhance clot stablity decreased further bleeding (but not mortality)
UGI bleeding -- treatmentVariceal hemorrhage 1. Stabilize hemodynamic ( crystal with colloid
supply) 2. Airway patent3. NG decompression of early detect of re-
bleeding4. Octreotide: Somatostatine (Somatosan)
2Amp add N/S to 50ml loading 2ml and maintain 2ml/ hr

11
UGI bleeding -- treatmentVariceal hemorrhage
5. Endoscopic therapy with ligation6. Sclerotherapy7. Balloon tamponade Sengstaken-Blakemore
tube8. Avoid hepatic encephalopathy9. Prophylaxis: reduce portal hypertensoion
-- Inderal, nitrates10. Surgery
Recurrent bleeding prevented
Eradication of H.P rebleeding rate < 5%Avoid NSAIDs

12
if no hemodynamic change andno dropping Hb:
routine endoscopy
ICU for 1 dayward for 1 to 2 days
Endoscopic therapy
active bleedingor visible vessel
ward for 3 days
no Endoscopic therapy
adherent clot or flat,pigmented spot
discharge
no Endoscopic therapy
clear base
ulcer
ICU for 1~2 dayward for 2 to 3 days
ligation orsclerotherapy
EV
ward for 1~2 days
Endoscopic therapy
active bleeding
discharge
no Endoscopic therapy
no active bleeding
Mallory-Weiss tear
hemodynamic change anddropping Hb:
urgent endoscopy
acute UGI bleeding