Gestational Diabetes: An Update
67
GESTATIONAL DIABETES: AN UPDATE Iris Thiele Isip Tan MD, MSc, FPCP, FPSEM Clinical Associate Professor, UP College of Medicine Section of Endocrinology, Diabetes & Metabolism Department of Medicine, Philippine General Hospital Friday, November 18, 11
-
Upload
iris-thiele-isip-tan -
Category
Health & Medicine
-
view
4.716 -
download
0
description
Presentation delivered at the 16th ASEAN Federation of Endocrine Societies congress in Ho Chi Minh City, Vietnam
Transcript of Gestational Diabetes: An Update

GESTATIONAL DIABETES:AN UPDATE
Iris Thiele Isip Tan MD, MSc, FPCP, FPSEMClinical Associate Professor, UP College of Medicine
Section of Endocrinology, Diabetes & MetabolismDepartment of Medicine, Philippine General Hospital
Friday, November 18, 11

http://www.flickr.com/photos/yogma/3961135108/
1st birthday
MD
Here I am!http://www.sxc.hu/photo/533027
Son #1 Son #2
19641972
19821996 2003 2006
2008 2010 2011
Friday, November 18, 11

http://www.flickr.com/photos/yogma/3961135108/
1st birthday
MD
Here I am!http://www.sxc.hu/photo/533027
Son #1 Son #2
19641972
19821996 2003 2006
2008 2010 2011
“For at least a generation there has been a divergence of opinions about GDM.”
Robert G. Moses, MDNew Consensus Criteria for GDM: Problem Solved or a Pandora’s Box
Diabetes Care 2010;33(3):690-1
Friday, November 18, 11

http://www.flickr.com/photos/yogma/3961135108/
1st birthday
MD
Here I am!http://www.sxc.hu/photo/533027
Son #1 Son #2
19641972
19821996 2003 2006
2008 2010 2011
O’Sullivan & Mahan criteria
Carpenter & Coustan
HAPO
IADPSGConsensus
“For at least a generation there has been a divergence of opinions about GDM.”
Robert G. Moses, MDNew Consensus Criteria for GDM: Problem Solved or a Pandora’s Box
Diabetes Care 2010;33(3):690-1
Friday, November 18, 11

Hyperglycemia Adverse Pregnancy Outcomes (HAPO)
International Association of Diabetes
in Pregnancy Study Groups (IADPSG)
Implications on screening and
diagnosis of GDM
Friday, November 18, 11

Hyperglycemia Adverse Pregnancy Outcomes
HAPO25,505 pregnant
15 centers9 countries
Thailand, Hong Kong, Singapore
NEJM 2008; 358:1991-2002
largediverse
populationsingle protocol
Friday, November 18, 11

75-g OGTT24-32 weeks
Results unblinded ifFPG >105 mg/dL2h PG >200 mg/dLRPG >160 mg/dLany PG <45 mg/dL
HAPO NEJM 2008; 358:1991-2002
Friday, November 18, 11

HAPO
http://www.flickr.com/photos/mikewade/3267336862/
BW>90th %ile
Primary CS
Cord blood serum C-peptide >90 %ile
Neonatal hypoglycemia
http://www.flickr.com/photos/tessawatson/379265818/
PrimaryOUTCOMES
http://www.flickr.com/photos/clairity/1385780317/http://www.flickr.com/photos/j2dread/4501366303/
NEJM 2008; 358:1991-2002
Friday, November 18, 11

OR for adverse pregnancy outcomes
1 level SD increase
FPG 6.9 mg/dL (0.4 mmol/L)
HAPO NEJM 2008; 358:1991-2002
1 h PG 30.9 mg/dL (1.7 mmol/L)2 h PG 23.5 mg/dL (1.3 mmol/L)
Friday, November 18, 11

HAPO
http://www.flickr.com/photos/mikewade/3267336862/
BW>90th %ile Fasting 1.38 (95%CI
1.32,1.44) OR
NEJM 2008; 358:1991-2002 1h PG 1.46 (95%CI
1.39,1.53)2h PG 1.38 (95%CI
1.32,1.44)
Fasting 1.55(95%CI
1.47,1.64)1h PG 1.46 (95%CI
1.38,1.54) 2h PG 1.37(95%CI
1.30,1.44)Cord blood serum
C-peptide >90 %ilehttp://www.flickr.com/photos/clairity/1385780317/
Friday, November 18, 11

HAPO
OR
NEJM 2008; 358:1991-2002
Primary CS Fasting 1.11 (95%CI
1.06,1.15)
1h PG 1.10 (95%CI
1.06,1.15) 2h PG 1.08 (95%CI
1.03,1.12)
http://www.flickr.com/photos/j2dread/4501366303/
Fasting 1.08(95%CI
0.98,1.19)1h PG 1.13 (95%CI
1.03,1.26) 2h PG 1.10(95%CI
1.00,1.12)
Neonatal hypoglycemia
http://www.flickr.com/photos/tessawatson/379265818/
Friday, November 18, 11

HAPO NEJM 2008; 358:1991-2002
No obvious threshold at which risks increased
Friday, November 18, 11

HAPO NEJM 2008; 358:1991-2002
FPG mg/dLCategory 1 <752 75-793 80-844 85-89 5 90-946 95-997 >100
FPG mg/dLCategory 1 <752 75-793 80-844 85-89 5 90-946 95-997 >100
No obvious threshold at which risks increased
Friday, November 18, 11

HAPO NEJM 2008; 358:1991-2002
1h PG mg/dLCategory 1 <1052 106-1323 133-1554 156-171 5 172-1936 194-2117 >212
1h PG mg/dLCategory 1 <1052 106-1323 133-1554 156-171 5 172-1936 194-2117 >212
No obvious threshold at which risks increased
Friday, November 18, 11

HAPO NEJM 2008; 358:1991-2002
2h PG mg/dLCategory1 <902 91-1083 109-1254 126-1395 140-1576 158-1777 >178
2h PG mg/dLCategory1 <902 91-1083 109-1254 126-1395 140-1576 158-1777 >178
No obvious threshold at which risks increased
Friday, November 18, 11

HAPO NEJM 2008; 358:1991-2002
LGA
Hypoglycemia
C-section
C-peptide
Friday, November 18, 11

HAPO NEJM 2008; 358:1991-2002
“Lack of clear thresholds and the fact that the four primary outcomes are not necessarily of equal clinical importance make direct translation of our results into clinical practice challenging.”
Friday, November 18, 11

Coustan et al. AJOG 2010; 202(6):654.e1-654.e6
“... the relationship between maternal glucose levels and fetal growth and outcome appear to be a basic biologic phenomenon, and not a clearly demarcated disease state ...”
Friday, November 18, 11

“What is a challenge is to decide how much increase in risk is the point at which treatment should be initiated and what is the hope and expectation for the treatment to reduce those risks ...”
Metzger B. Endocrine Today 2008
Friday, November 18, 11

“Secondly, should the associations of glucose be weighted equally with the primary outcomes or are some more important than others?
The third issue is whether all of the glucose measures are needed to identify increased risk.”
Metzger B. Endocrine Today 2008
Friday, November 18, 11

Hyperglycemia Adverse Pregnancy Outcomes (HAPO)
International Association of Diabetes
in Pregnancy Study Groups (IADPSG)
Friday, November 18, 11

http://www.sxc.hu/photo/358002
IADPSGencourage and facilitate research and advance education
facilitate an international approach to enhancing the quality of care for women with diabetes in pregnancy
Coustan et al. AJOG 2010; 202(6):654.e1-654.e6
Friday, November 18, 11

Coustan et al. AJOG 2010; 202(6):654.e1-654.e6
workshop/conference June 2008 (220 delegates approx 40 countries)
consensus development session (50 delegates)
IADPSG
Friday, November 18, 11

OR for increased neonatal body fat, LGA and cord serum C-peptide
Mean glucose as reference
Coustan et al. AJOG 2010; 202(6):654.e1-654.e6
OR%
Subjects > Threshold
Positive Predictive Valuefor >90th %ile
Positive Predictive Valuefor >90th %ile
Positive Predictive Valuefor >90th %ileOR
% Subjects > Threshold Birth
weight C-peptide % Body fat
1.75 16.1 16.2 17.5 16.62.0 8.8 17.6 19.7 18.8
Friday, November 18, 11

Coustan et al. AJOG 2010; 202(6):654.e1-654.e6
IADPSG recommendation for diagnosis of GDM
FBS 92 mg/dL
1h 180 mg/dL
2h 153 mg/dL
Diagnosis requires only one threshold value exceeded
Friday, November 18, 11

Coustan et al. AJOG 2010; 202(6):654.e1-654.e6
IADPSG recommendation for diagnosis of GDM
FBS 92 mg/dL
1h 180 mg/dL
2h 153 mg/dL
ADA FBS 95 mg/dL1h 180 mg/dL2h 155 mg/dL
Diagnosis requires only one threshold value exceeded
Friday, November 18, 11

First prenatal visit Measure FPG, A1c or random plasma glucose in all or only in high-risk
IADPSG Consensus Panel. Diabetes Care Mar 2010;33(3):676-82
Overt Diabetes in Pregnancy
FPG > 7 mmol/L A1c > 6.5%Random PG > 11.1 mmol/L
Gestational Diabetes
FPG 5.1-6.9 mmol/L (92-125 mg/dL)
Order a 75-g OGTT at 24-28 wks AOG
FPG <5.1 mmol/L
Friday, November 18, 11

Coustan et al. AJOG 2010; 202(6):654.e1-654.e6
IADPSG recommendation for diagnosis of GDM
FBS 92 mg/dL
1h 180 mg/dL
2h 153 mg/dLDiagnosis requires only one
threshold value exceeded
Overt diabetesFPG >7.0 mmol/L (126 mg/dL)
24-28 wks AOG
Friday, November 18, 11

Implications on screening and diagnosis of GDM
Friday, November 18, 11

http://www.flickr.com/photos/kkoshy/4334413228/
More women will be diagnosed with GDM17.8% of pregnant women in HAPO
Use of IADPSG criteria
Ryan EA. Diabetologia 2011; 54:480-6
+ 1,702 women with GDMfrom 2,448 to 4,150 of 23,316 pregnancies in HAPO
Friday, November 18, 11

n = 1038
50-g GCT
Morikawa M. Diab Res Clin Pract 2010; 90:339-42.
Friday, November 18, 11

n = 1038
50-g GCT
>7.8 mmol/L+ GCT
n = 228
Morikawa M. Diab Res Clin Pract 2010; 90:339-42.
Friday, November 18, 11

n = 1038
50-g GCT
>7.8 mmol/L+ GCT
n = 228
<7.8 mmol/L- GCT
n = 810
Morikawa M. Diab Res Clin Pract 2010; 90:339-42.
Friday, November 18, 11

n = 1038
50-g GCT
>7.8 mmol/L+ GCT
n = 228
<7.8 mmol/L- GCT
n = 810
75-g OGTTJapan SOG criteriaFPG>100 mg/dL1h PG >180 mg/dL2h PG >150 mg/dL
Morikawa M. Diab Res Clin Pract 2010; 90:339-42.
Friday, November 18, 11

n = 1038
50-g GCT
>7.8 mmol/L+ GCT
n = 228
<7.8 mmol/L- GCT
n = 810
75-g OGTTJapan SOG criteriaFPG>100 mg/dL1h PG >180 mg/dL2h PG >150 mg/dL
Morikawa M. Diab Res Clin Pract 2010; 90:339-42.
>7.8 mmol/L+
n = 25
OGTT
Friday, November 18, 11

n = 1038
50-g GCT
>7.8 mmol/L+ GCT
n = 228
<7.8 mmol/L- GCT
n = 810
75-g OGTTJapan SOG criteriaFPG>100 mg/dL1h PG >180 mg/dL2h PG >150 mg/dL
Morikawa M. Diab Res Clin Pract 2010; 90:339-42.
>7.8 mmol/L+
n = 25
OGTT
n = 203
>7.8 mmol/L- OGTT
Friday, November 18, 11

n = 1038
50-g GCT
>7.8 mmol/L+ GCT
n = 228
<7.8 mmol/L- GCT
n = 810
75-g OGTTJapan SOG criteriaFPG>100 mg/dL1h PG >180 mg/dL2h PG >150 mg/dL
+IADPSG criteria
5 overt DM20 GDM
43 GDM
Morikawa M. Diab Res Clin Pract 2010; 90:339-42.
>7.8 mmol/L+
n = 25
OGTT
n = 203
>7.8 mmol/L- OGTT
Friday, November 18, 11

n = 1038
50-g GCT
>7.8 mmol/L+ GCT
n = 228
<7.8 mmol/L- GCT
n = 810
75-g OGTTJapan SOG criteriaFPG>100 mg/dL1h PG >180 mg/dL2h PG >150 mg/dL
+IADPSG criteria
5 overt DM20 GDM
43 GDM
Total 68 GDM172% increase
Morikawa M. Diab Res Clin Pract 2010; 90:339-42.
>7.8 mmol/L+
n = 25
OGTT
n = 203
>7.8 mmol/L- OGTT
Friday, November 18, 11

Flack JR et al. Aus NZ J Obstet Gynecol 2010; 50:439-43.
29% increase in workload
extra 366 women diagnosed
Impact on workload of changing GDM diagnostic criteria by lowering fBGL alone and with increasing 2h BGL (IADPSG)
ADIPS criteriafBGL >5.5 mmol/L2h BGL >8.0 mmol/L
Friday, November 18, 11

Flack JR et al. Aus NZ J Obstet Gynecol 2010; 50:439-43.
“One approach will be to argue that we cannot cope with the change in numbers and that these new criteria should be ignored.”
will leave a significant number at risk untreated...
Friday, November 18, 11

Flack JR et al. Aus NZ J Obstet Gynecol 2010; 50:439-43.
Adjust thresholds for fasting, 1h & 2h BG levels “to keep the number of women diagnosed with GDM stable ... an example of explicit rationing of medical care.”
Friday, November 18, 11

Stratify risk.
“Those women diagnosed at the lower end of the ‘new’ diagnostic range may be expected to be at ‘lower risk’ and if so, their management ‘may’ be ...‘less stringent’.”
Flack JR et al. Aus NZ J Obstet Gynecol 2010; 50:439-43.
Friday, November 18, 11

75-g OGTTJapan SOG criteriaFPG>100 mg/dL1h PG >180 mg/dL2h PG >150 mg/dL
IADPSG criteria43 GDM
of which 5 needed insulin
20 GDM 5 overt DM
needed insulin
Morikawa M. Diab Res Clin Pract 2010; 90:339-42.
>7.8 mmol/L+ n = 25OGTT
n = 203
>7.8 mmol/L- OGTT
n = 228
IADPSG “overt diabetes” diagnosis may help differentiate women who need insulin from women who do not need insulin.
Friday, November 18, 11

http://www.sxc.hu/photo/249796
X 140 cases of LGAX 21 cases of shoulder dystocia
X 16 cases of birth injury
Ryan EA. Diabetologia 2011; 54:480-6
IADPSG criteria
of 23,316 pregnancies in HAPO cohort
Friday, November 18, 11

http://www.sxc.hu/photo/249796
X 140 cases of LGAX 21 cases of shoulder dystocia
X 16 cases of birth injury
Ryan EA. Diabetologia 2011; 54:480-6
Modest outcomes?
IADPSG criteria
of 23,316 pregnancies in HAPO cohort
Friday, November 18, 11

n = 1038
50-g GCT
>7.8 mmol/L+ GCT
n = 228
<7.8 mmol/L- GCT
n = 810
75-g OGTTJapan SOG criteriaFPG>100 mg/dL1h PG >180 mg/dL2h PG >150 mg/dL
+IADPSG criteria
5 overt DM20 GDM
43 GDM
Total 68 GDM172% increase
Morikawa M. Diab Res Clin Pract 2010;90: 339-42.
>7.8 mmol/L+
n = 25
OGTT
n = 203
>7.8 mmol/L- OGTT
Friday, November 18, 11

75-g OGTTJapan SOG criteriaFPG>100 mg/dL1h PG >180 mg/dL2h PG >150 mg/dL
IADPSG criteria43 GDM
5 overt DM20 GDM
Morikawa M. Diab Res Clin Pract 2010;90 339-42.
>7.8 mmol/L+ n = 25OGTT
n = 203
>7.8 mmol/L- OGTT
n = 228
no specific treatment for GDM
+ GCT
Friday, November 18, 11

75-g OGTTJapan SOG criteriaFPG>100 mg/dL1h PG >180 mg/dL2h PG >150 mg/dL
IADPSG criteria43 GDM
5 overt DM20 GDM
Morikawa M. Diab Res Clin Pract 2010;90 339-42.
>7.8 mmol/L+ n = 25OGTT
n = 203
>7.8 mmol/L- OGTT
n = 228
no specific treatment for GDM
6 infants >3600 g (14%)p=0.021 vs non-GDM 3.8% (n=160)
Number Needed to Treat (NNT)1/(0.14-0.038) = 9.8
+ GCT
Friday, November 18, 11

Nurses, dietitians & physicians
Glucose monitoringTherapy of diabetes
Ryan EA. Diabetologia 2011; 54:480-6
Friday, November 18, 11

Nurses, dietitians & physicians
Glucose monitoringTherapy of diabetes
Ryan EA. Diabetologia 2011; 54:480-6
Cost-effective strategy based on riskGDM risk <1%: no screening/treatment strategy1-4.2%: FPG followed by OGTT>4.2%: OGTT alone
Round JA et al. Diabetologia 2011; 54:256-63
Friday, November 18, 11

RR for developing gestational diabetes by ethnicity (adjusted for age, BMI and parity; white as reference)
UK Data (1992) RR (95%CI)Black 3.1 (1.8 to 5.5)
South East Asian 7.6 (4.1 to 14.1)
Indian 11.3 (6.8 to 18.8)
Dornhorst A, Paterson CM, Nicholls JSD, et al. High prevalence of gestational diabetes in women from ethnic minority groups. Diabetic Medicine 1992; 9:820–5.
Friday, November 18, 11

Prevalence (%)Indonesia 16Malaysia 13Philippines 14Singapore 10Thailand 13ASEAN 13
AFES Study Group on Diabetes in Pregnancy (ASGODIP)
Litonjua AD et al. AFES Study Group on Diabetes in Pregnancy: Preliminary Data on Prevalence. PJIM 1996:34:67-68.
Philippines n/NLow risk 35/853High risk 136/350
Overall 171/120314.2%
ASGODIP protocol 1-step (high-risk)75-g OGTT2h cut-off 140 mg/dL
Friday, November 18, 11

Holt RIG et al. Diabete Med 2011; 28:382-5.
Increased prevalence of GDM using the IADPSG criteria “can only be justified if it is shown convincingly that pregnancy outcomes are improved.”
Friday, November 18, 11

Landon et al NEJM 2009; 361:1339-48.
PI
MO
Intervention (n=485)
diet CBG insulin vs
routine care (n=473)
Composite of stillbirth/perinatal
death and neonatal
complications
Randomized controlled
trial
“mild” GDM24-31 wks AOG
Landon MB et al. A multicenter, randomized trial of treatment for mild gestational diabetes. NEJM 2009; 361:1339-48.
hyperbilirubinemia hypoglycemia
hyperinsulinemia birth trauma
Friday, November 18, 11

Landon et al NEJM 2009; 361:1339-48.
PI
MO
Intervention (n=485)
diet CBG insulin vs
routine care (n=473)
Composite of stillbirth/perinatal
death and neonatal
complications
Randomized controlled
trial
“mild” GDM24-31 wks AOG
Landon MB et al. A multicenter, randomized trial of treatment for mild gestational diabetes. NEJM 2009; 361:1339-48.
hyperbilirubinemia hypoglycemia
hyperinsulinemia birth trauma
Composite endpoint RR 0.87 (95% CI 0.72-1.07), p=0.14
Friday, November 18, 11

Landon et al NEJM 2009; 361:1339-48.
PI
MO
Intervention (n=485)
diet CBG insulin vs
routine care (n=473)
Randomized controlled
trial
“mild” GDM24-31 wks AOG
Landon MB et al. A multicenter, randomized trial of treatment for mild gestational diabetes. NEJM 2009; 361:1339-48.
Composite endpoint RR 0.87 (95% CI 0.72-1.07), p=0.14
Friday, November 18, 11

Landon et al NEJM 2009; 361:1339-48.
PI
MO
Intervention (n=485)
diet CBG insulin vs
routine care (n=473)
Randomized controlled
trial
“mild” GDM24-31 wks AOG
Landon MB et al. A multicenter, randomized trial of treatment for mild gestational diabetes. NEJM 2009; 361:1339-48.
Composite endpoint RR 0.87 (95% CI 0.72-1.07), p=0.14
LGA infants RR 0.49
(95%CI 0.32-0.76) p<0.001
BW >4000 g RR 0.41
(95%CI 0.26-0.66) p<0.001
Friday, November 18, 11

ACHOISCrowther et al. NEJM 2005; 352:2477-86.
Crowther CA et al. Effect of Treatment of Gestational Diabetes Mellitus on Pregnancy Outcomes. NEJM 2005; 352:2477-86.
PI
MO
GDM24-28 wks AOG
Intervention (n=490)
diet CBG insulin vs
routine care (n=510)
Serious perinatal
complications death
shoulder dystociabone fracturenerve palsy
Randomized controlled
trial
Friday, November 18, 11

ACHOISCrowther et al. NEJM 2005; 352:2477-86.
Crowther CA et al. Effect of Treatment of Gestational Diabetes Mellitus on Pregnancy Outcomes. NEJM 2005; 352:2477-86.
PI
MO
GDM24-28 wks AOG
Intervention (n=490)
diet CBG insulin vs
routine care (n=510)
Serious perinatal
complications death
shoulder dystociabone fracturenerve palsy
Randomized controlled
trial
Any serious perinatal complication Adj RR 0.33 (95% CI 0.14-0.75), p=0.01
Friday, November 18, 11

http://www.flickr.com/photos/craigoneal/4084388198/
OGTT is poorly reproducibleDiagnosis based on a single test, on a single abnormal value
Ryan EA. Diabetologia 2011; 54:480-6
Friday, November 18, 11

Gestational diabetes would be diagnosed if one or morevalues met or exceeded the following levels of glucose:fasting 5.1 mmol/l, 1 h post glucose 10.0 mmol/l and 2 hpost glucose 8.5 mmol/l. Use of these criteria will result in17.8% of the pregnant population being diagnosed withgestational diabetes. A detailed analysis of the same HAPOstudy information and other recent related publicationsraises issues that are worthy of further debate in the widerdiabetes community.
Observational data
HAPO was an international prospective observational studyof 23,316 pregnant women directed to answer the question:‘Is hyperglycaemia during pregnancy, at a level below thatfor overt diabetes, associated with increased risk ofmaternal or fetal complications?’ [2]. The participatingwomen had an OGTT and were divided into seven glucosecategories. The category 3 group encompassed the meanglucose values, i.e. fasting 4.5 mmol/l, 1 h post OGTT7.4 mmol/l and 2 h post OGTT 6.2 mmol/l, while the newproposed cut-offs from IADPSG fall in category 5. Theprimary endpoints were large-for-gestational age infants(LGA), primary Caesarean section rate, neonatal hypogly-caemia and cord C-peptide. The study demonstrated acontinuous relationship between glycaemia (fasting, and 1or 2 h post glucose load) and each of the primary outcomes,having adjusted for field centre and ethnicity. Whilesupporting the Pedersen hypothesis [3], the results did notshow any inflection point indicating clearly increased riskof any of these outcomes with a particular glucose category;rather, risk increased gradually over the glucose range.
A further publication from the group examined the roleof maternal BMI with the same primary outcomes [4]. Thisreport used an adjustment (Model 1) for many of theexpected confounders (age, alcohol, smoking, sex etc.), andalso a model (Model 2) that adjusted for fasting plasma
glucose and mean arterial pressure. The OR for LGA,primary Caesarean section and cord C-peptide increasedsignificantly for increasing categories of BMI, this differ-ence being maintained when adjusted for glucose and meanarterial pressure (reference group BMI <22.6 kg/m2;Fig. 1a). When the plot for LGA vs glucose is added(reference group category 1 glucose as used in the HAPOreport; Fig. 1a), it is apparent that maternal BMI has agreater impact on OR than maternal glucose in all exceptthe highest glucose category. This is also true for theprimary Caesarean section rate (Electronic supplementarymaterial [ESM] Fig. 1a), whereas the glucose level hadmore influence on the OR for cord C-peptide in glucosecategories 5–7 (ESM Fig. 1b). Thus, maternal BMI andglucose both contribute to risk of LGA, but the role of BMIwas more pronounced than that of glucose in determiningLGA incidence, until the highest glucose category wasreached. Using the category BMI 22.6–28.4 kg/m2 (whichincludes overweight women) and category 3 for glucose asthe reference groups (i.e. using reference groups thatinclude the means) shows that BMI and glucose have asimilar impact on the OR (ESM Fig. 2a–c).
The majority of women from the HAPO data hadglucose levels !category 3, i.e. the category encompassingthe mean glucose level (Fig. 1b). Moreover, the number ofLGA increased proportionately with higher glucose levels(Fig. 1b), but when the numbers of mothers with LGA ingiven glucose categories are classed separately (Fig. 1c),the majority (63%) of women with LGA are seen to haveglucose levels from the OGTT at or lower than category 3,the category incorporating the mean glucose level. This isalso true for the 1 and 2 h post-load challenge (ESMFig. 3). It is also noteworthy that at category 5 (equivalentto the IADPSG cut-off criteria, accepting that some cases incategory 5 will lie above these cut-offs within category 5)women below these cut-offs who had LGA represented78% of all women giving birth to LGA.
BMI category (Kg/m2)
Glucose category
Wom
en (
n)
Wom
en (
n)
8,000 700
600
500
400
300
200
100
0
6,000
4,000
2,000
0
<22.6 22.6!28.4
28.5!32.9
33.0!37.4
37.5! 42.041.9
1 2 3 4 5 6 7
Glucose category1 2 3 4 5 6 7
a b c
OR
0
1
2
3
4
5
1 3 52 4 6 7Glucose category
Fig. 1 a Relationship of the OR for an infant of birthweight >90thpercentile vs the BMI in categories (reference group BMI <22.6 kg/m2
[4]) or maternal fasting glucose in categories from HAPO (diamonds;reference group category 1 lowest glucose [2]). a The BMIrelationship is adjusted for model 1 (circles) or model 2 (triangles)
(see text for details). The relationship for maternal fasting glucosecategories is also shown (black diamonds). b Number of participantsin each category of glucose in HAPO (white bars), with number ofmothers with LGA infants (black bars). c Number of participants ineach category of glucose who had LGA infants
Diabetologia (2011) 54:480–486 481
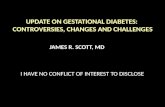
Ryan EA. Diabetologia 2011; 54:480-6
Greater impact of maternal BMI on OR for LGA than maternal glucose except highest glucose category
HAPO
● BMI Model 1▲ BMI Model 2
◆ Maternal FG
Model 1: Adjusted for age, alcohol, smoking, sex, etc.Model 2: Adjusted for mean FG and MAP
Friday, November 18, 11

Gestational diabetes would be diagnosed if one or morevalues met or exceeded the following levels of glucose:fasting 5.1 mmol/l, 1 h post glucose 10.0 mmol/l and 2 hpost glucose 8.5 mmol/l. Use of these criteria will result in17.8% of the pregnant population being diagnosed withgestational diabetes. A detailed analysis of the same HAPOstudy information and other recent related publicationsraises issues that are worthy of further debate in the widerdiabetes community.
Observational data
HAPO was an international prospective observational studyof 23,316 pregnant women directed to answer the question:‘Is hyperglycaemia during pregnancy, at a level below thatfor overt diabetes, associated with increased risk ofmaternal or fetal complications?’ [2]. The participatingwomen had an OGTT and were divided into seven glucosecategories. The category 3 group encompassed the meanglucose values, i.e. fasting 4.5 mmol/l, 1 h post OGTT7.4 mmol/l and 2 h post OGTT 6.2 mmol/l, while the newproposed cut-offs from IADPSG fall in category 5. Theprimary endpoints were large-for-gestational age infants(LGA), primary Caesarean section rate, neonatal hypogly-caemia and cord C-peptide. The study demonstrated acontinuous relationship between glycaemia (fasting, and 1or 2 h post glucose load) and each of the primary outcomes,having adjusted for field centre and ethnicity. Whilesupporting the Pedersen hypothesis [3], the results did notshow any inflection point indicating clearly increased riskof any of these outcomes with a particular glucose category;rather, risk increased gradually over the glucose range.
A further publication from the group examined the roleof maternal BMI with the same primary outcomes [4]. Thisreport used an adjustment (Model 1) for many of theexpected confounders (age, alcohol, smoking, sex etc.), andalso a model (Model 2) that adjusted for fasting plasma
glucose and mean arterial pressure. The OR for LGA,primary Caesarean section and cord C-peptide increasedsignificantly for increasing categories of BMI, this differ-ence being maintained when adjusted for glucose and meanarterial pressure (reference group BMI <22.6 kg/m2;Fig. 1a). When the plot for LGA vs glucose is added(reference group category 1 glucose as used in the HAPOreport; Fig. 1a), it is apparent that maternal BMI has agreater impact on OR than maternal glucose in all exceptthe highest glucose category. This is also true for theprimary Caesarean section rate (Electronic supplementarymaterial [ESM] Fig. 1a), whereas the glucose level hadmore influence on the OR for cord C-peptide in glucosecategories 5–7 (ESM Fig. 1b). Thus, maternal BMI andglucose both contribute to risk of LGA, but the role of BMIwas more pronounced than that of glucose in determiningLGA incidence, until the highest glucose category wasreached. Using the category BMI 22.6–28.4 kg/m2 (whichincludes overweight women) and category 3 for glucose asthe reference groups (i.e. using reference groups thatinclude the means) shows that BMI and glucose have asimilar impact on the OR (ESM Fig. 2a–c).
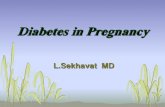
The majority of women from the HAPO data hadglucose levels !category 3, i.e. the category encompassingthe mean glucose level (Fig. 1b). Moreover, the number ofLGA increased proportionately with higher glucose levels(Fig. 1b), but when the numbers of mothers with LGA ingiven glucose categories are classed separately (Fig. 1c),the majority (63%) of women with LGA are seen to haveglucose levels from the OGTT at or lower than category 3,the category incorporating the mean glucose level. This isalso true for the 1 and 2 h post-load challenge (ESMFig. 3). It is also noteworthy that at category 5 (equivalentto the IADPSG cut-off criteria, accepting that some cases incategory 5 will lie above these cut-offs within category 5)women below these cut-offs who had LGA represented78% of all women giving birth to LGA.
BMI category (Kg/m2)
Glucose category
Wom
en (
n)
Wom
en (
n)
8,000 700
600
500
400
300
200
100
0
6,000
4,000
2,000
0
<22.6 22.6!28.4
28.5!32.9
33.0!37.4
37.5! 42.041.9
1 2 3 4 5 6 7
Glucose category1 2 3 4 5 6 7
a b c
OR
0
1
2
3
4
5
1 3 52 4 6 7Glucose category
Fig. 1 a Relationship of the OR for an infant of birthweight >90thpercentile vs the BMI in categories (reference group BMI <22.6 kg/m2
[4]) or maternal fasting glucose in categories from HAPO (diamonds;reference group category 1 lowest glucose [2]). a The BMIrelationship is adjusted for model 1 (circles) or model 2 (triangles)
(see text for details). The relationship for maternal fasting glucosecategories is also shown (black diamonds). b Number of participantsin each category of glucose in HAPO (white bars), with number ofmothers with LGA infants (black bars). c Number of participants ineach category of glucose who had LGA infants
Diabetologia (2011) 54:480–486 481
Ryan EA. Diabetologia 2011; 54:480-6
HAPO☐ Participants■ Participants with LGA infants
Majority of women had glucose levels < Cat. 3 (mean glucose level)
Most cases of LGA occur in normal maternal glycemia
78% of LGA born to women not fulfilling IADPSG criteria
Friday, November 18, 11

Diagnosis of GDM identifies women at risk of type 2 diabetes
GDM independent risk
factor for diabetes in Filipino-Americans
RR 21.65 (95%CI 6.73-69.67)
Cuasay et al. Diabetes Care 2001;24(12):2054-8
IADPSG criteria may overestimate
risk of diabetes
Friday, November 18, 11

Approved by ADAACOG did not approve
IADPSG Consensus
ACOG Committee on Obstetric Practice. Screening & Diagnosis of Gestational Diabetes Mellitus. Obstetrics & Gynecology 2011; 118(3):751-3
Friday, November 18, 11

Philippine Diabetes CPG has partially adopted the IADPSG consensus by endorsing the HAPO-derived thresholds for the 75-g OGTT.
Friday, November 18, 11

Hyperglycemia Adverse Pregnancy Outcomes (HAPO)
International Association of Diabetes
in Pregnancy Study Groups (IADPSG)
Implications on screening and
diagnosis of GDM
Friday, November 18, 11

THANK YOUhttp://www.endocrine-witch.net
Friday, November 18, 11