
Geriatric Assessment and Interventions · MrsA–Geriatric Assessment • Functional status:...
58
Geriatric Assessment and Interventions Siri Rostoft, MD, PhD Department of Geriatric Medicine Oslo University Hospital Norway
Transcript of Geriatric Assessment and Interventions · MrsA–Geriatric Assessment • Functional status:...

Geriatric Assessment and
Interventions
Siri Rostoft, MD, PhD
Department of Geriatric Medicine
Oslo University Hospital
Norway

Disclosure
No conflicts of interest to declare

Mrs A, aged 94
• Admitted to the acute geriatric ward
because of fatigue and dizziness
• Work up revealed severe iron-deficiency
anemia (she was bleeding)
• Colonoscopy revealed right sided large
colon cancer, narrow passage
• Surgery?

Decrease in capacity - heterogeneity
Muravchik, Anesthesia 5th ed, 2000

What factors to consider?
• Discuss for 2-3 minutes with the person next
to you

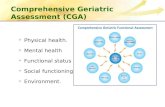
Geriatric assessment (GA)1
- Functional status
- Comorbidity
- Polypharmacy
- Cognitive function/
dementia
- Nutritional status
- Depression
- Social support
Remaining life expectancy
Detection of unidentified problems
Optimization before treatment
Prediction of adverse outcomes
Treatment planning
Baseline information
Shared decision-making
FRAILTY
1Wildiers et al, JCO, 2014

Siri Rostoft 2017

Studies included in review
• CGA and ability to detect health problems: n=29
• CGA and prediction of outcomes: n=17
• CGA and tailored interventions: n=3

Results
• All CGA types identified
- large numbers of geriatric problems
- multiple comorbidities likely to interfere with
cancer treatment and to compete with cancer as a
cause of death
• Some CGA domains may influence treatment decisions
– functional status and nutritional status may have the strongest effect

Results cont.
• Each CGA domain was associated with chemotoxicity and survival in at least one study
• The domains most often predicting mortality and chemotoxicity:
– functional impairment
– malnutrition
– comorbidities

Siri Rostoft 2017

Methods and results
• 10 studies included in the review
• Change in oncologic treatment:
– the initial treatment plan modified in 39% of patients
after geriatric evaluation
– two thirds resulted in less intensive treatment
• Implementation of non-oncologic interventions
– interventions were suggested for more than 70% of patients
– most frequently social interventions and pharmacological interventions

Conclusion
• A geriatric evaluation has significant impact on
oncologic and non-oncologic treatment
decisions in older cancer patients

Journal of Surgical Research 193 (2015) 265-272
Siri Rostoft 2017

Results
• Elective surgery only
• 10 publications from 6 studies
• GA domains predicting overall and major complications
– dependency in ADLs and IADLs (functional status)
– higher ASA score
– decreased mini-mental state examination score
– worse geriatric depression score
– worse frailty scores
– fatigue
Journal of Surgical Research 193 (2015) 265-272

Results cont.
• Age was not an independent predictor of morbidity
in any studies
• No GA domains predicted postoperative mortality
(low mortality rates in elective surgery)
• Frailty predicted readmissions
• Functional status and frailty predicted discharge to
a nursing home
Journal of Surgical Research 193 (2015) 265-272

Categorization
Geriatric assessment
Geriatric assessment
FitFit IntermediateIntermediate FrailFrail

Geriatric assessment
• Overall assessment
• Multidisciplinary
• Areas where older patients often have
problems
• CGA – assessment with interventions
• Implementing GA in older hospitalized adults
increases likelihood of being alive and living in
their own home1
1Ellis Cochrane Rev 2011

GA in oncology
• Delphi study1:
• All cancer patients > 70 years
• Younger with age-related issues
• Most important domains:
– Functional status
– Comorbidities
– Cognitive function
1O´Donovan et al 2015

Mrs A – Geriatric Assessment
• Functional status: Dependence in IADL. Needed help shopping. Problems walking, uses a cane. TUG > 20 sec
• Comorbidity: Heart failure – but is the diagnosis correct? She can walk one flight of stairs without being out of breath. Stroke in 2008, no apparent sequela. Reduced vision and reduced hearing.
• Polypharmacy: beta blocker and diuretics

• Nutritional status: No appetite last month (due to tumour), weight loss, at risk of malnutrition
• Cognitive function: MMSE 27/30, she appeared adequate in conversation, she could discuss treatment options
• Emotional status: No symptoms of depression

Recommendation
• She had some frailty indicators, risk of post-
operative complications high
• Complications from tumour at present
(anemia, weight loss)
• Risk in emergency surgery much higher than
elective surgery
• Operated electively, had some complications,
survived, discharged home

A FEW WORDS ABOUT FUNCTIONAL
STATUS

Case – man with rectal cancer
• 69 years old, home dwelling
• Locally advanced rectal cancer
• Admitted for preoperative chemoradiotherapyaccording to guidelines
• After a week non-cooperative, pulled out i.v.lines, completely bed-ridden, aggressive
• What do we call this? Any risk factors?

“She Was Probably Able to Ambulate,
but I’m Not Sure”
• Failure to assess functional status in hospitalized patients is the norm
• Basic: ADL-function, mobility, and cognition
• 1/3 of patients 70+ encounter hospitalization-associated disability (even when acute illness is effectively treated)
Covinsky JAMA 2011

How to measure functional status
ADL = activities of daily living
- survive (eat, go to the toilet)
IADL = instrumental ADL
- live independently (manage money, shop,
medication use)
Performance measures: Gait speed, TUG (timed
up and og test), grip strength
Ask about falls

Walter et al, JAMA, 2001Siri Rostoft 2017

Stanaway, BMJ, 2011
Grim reaper´s maximum speed: 1.36 m/s

“HAVE YOU FALLEN?”
Jones et al, JAMA Surgery, 2013

COMORBIDITY
Siri Rostoft 2017

Why is comorbidity relevant?
• Discuss with the person next to you for a few
minutes
• How do you assess comorbidity in your clinical
practice?
Siri Rostoft 2017

Barnett et al, Lancet 2012
Chronic disorders by age-group
Siri Rostoft 2017

Comorbidity scales
• Charlson´s comorbidity index
• Weighted comorbidity index
• Predicted survival in cancer patients
• 19 selected conditions

Siri Rostoft 2017

CIRS – cumulative illness rating scale
• Developed in 1968
• Revised in 1992
• Revised scoring manual in 2008
• Scores 14 organ systems – disease severity
possible to score
• Too cumbersome for clinical practice
Siri Rostoft 2017

Optimization of comorbidities
• Geriatrician?
• Internal medicine specialist?
• Subspecialist, i.e. cardiologist?
• Core activity in the acute geriatric ward
• Competing risks
Siri Rostoft 2017

Polypharmacy
• Definitions vary
– More than 5 drugs in daily use
– The use of inappropriate medications
• Interactions
• Adverse events
• Polypharmacy is a risk factor for
undertreatment
Siri Rostoft 2017

Polypharmacy
• Goal: Dynamic approach
• What about drugs with a preventive effect?
• Discontinuation trials
Siri Rostoft 2017

Siri Rostoft 2017

Patients and methods• Multicenter, parallel-group, unblinded, pragmatic
clinical trial
• Estimated life expectancy 1 month - 1 year
• Statin therapy for 3 months or more for primary or sec. prevention of cardiovascular disease
• Recent deterioration in functional status
• No recent active cardiovascular disease
• Participants were randomized to either discontinue or continue statin therapy and were monitored monthly for up to 1 year

Conclusions
• Stopping statin medication therapy is
- safe
- may be associated with benefits including
improved quality of life
- use of fewer non-statin medications

Cognitive function
• Mild cognitive impairment
• Dementia
• Screening instruments, MMSE, MOCA, Mini-Cog
• Why improtant?
Siri Rostoft 2017


Why important?
• Consent
• Prognosis
• Treatment planning
• Baseline - chemobrain
Siri Rostoft 2017

Siri Rostoft 2017

Siri Rostoft 2017

NUTRITIONAL STATUS

Malnutrition
• Differs between countries – in Norway
malnutrition is the dominant problem
• Home dwelling: 6%, hospitals 40%, nursing
homes 14%
• Tool: mini nutritional assessment (MNA)
• Definite risk factor – but do interventions
help?
• How to intervene?
Siri Rostoft 2017

EMOTIONAL STATUS
Siri Rostoft 2017

Emotional function
• Depression, anxiety and distress
• Common among older people
• Common among cancer patients
• Risk factors are pain and physical distress
• Fear of impeding mortality
• Protective: Attachment security, self-esteem, sense of meaning and purpose
• Treatment options?
Siri Rostoft 2017

Study (depression)1
• Older cancer patients (>70) receiving
chemotherapy (n=344)
• 45% depressed
• Risk factor: malnutrition at baseline
1Duc et al. Psychooncology, 2016Siri Rostoft 2017

SOCIAL SUPPORT
Siri Rostoft 2017

Social support
• Fundamental for treatment planning
• Population level – sociodemographic factors
strong predictors for receiving treatment and
survival
Siri Rostoft 2017

GA COMPLETED – WHAT NOW?
Siri Rostoft 2017

Geriatric assessment (GA)1
Remaining life expectancy
Detection of unidentified problems
Optimization before treatment
Prediction of adverse outcomes
Treatment planning
Baseline information
Shared decision-making
1Wildiers et al, JCO, 2014

TOO TIME-CONSUMING???
Siri Rostoft 2017

SUMMARY
• The heterogeneity increases with increasing
age
• We need to assess frailty rather than looking
at chronological age alone when deciding
treatment
• Geriatric assessment provides a practical
approach to older patients
• GA is necessary in many older cancer patients
for a number of reasons

THANK YOU FOR YOUR ATTENTION
QUESTIONS?












![geriatric assessment [EDocFind.com].ppt](https://static.fdocuments.net/doc/165x107/56d6c0791a28ab30169a87ff/geriatric-assessment-edocfindcomppt.jpg)




