Geno Derma

of 24
-
Upload
nicky-adi-saputra -
Category
Documents
-
view
33 -
download
0
description
kdfkdskfjrl
Transcript of Geno Derma
Genodermatoses are inherited genetic skin conditions often grouped into three categories: chromosomal, single gene, and polygenetic.[1]:547A few genodermatoses Epidermolysis Bullosa Ichthyosis Palmoplantar keratoderma Neurofibromatosis Xeroderma pigmentosum Incontinentia pigmenti Restrictive dermopathyEpidermolysis bullosaFrom Wikipedia, the free encyclopedia(Redirected from Epidermolysis Bullosa)Epidermolysis bullosa
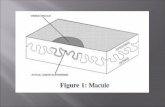
A five-year-old boy with congenital epidermolysis bullosa
Classification and external resources
SpecialtyDermatology
ICD-10Q81
ICD-9-CM757.39
DiseasesDB31928 33248
MedlinePlus001457
eMedicinederm/124
Patient UKEpidermolysis bullosa
MeSHD004820
[edit on Wikidata]
Epidermolysis bullosa (EB) is a group of inherited connective tissue diseases that cause blisters in the skin and mucosal membranes, with an incidence of 20 per million newborns in the United States.[1] It is a result of a defect in anchoring between the epidermis and dermis, resulting in friction and skin fragility. Its severity ranges from mild to lethal.The condition was brought to public attention in 2004 in the UK through the Channel 4 documentary The Boy Whose Skin Fell Off, chronicling the life and death of Jonny Kennedy, an Englishman with EB.[2] In the United States, the same could be said of the HBO documentary My Flesh and Blood from 2003.[citation needed]"Butterfly Children" is a term often used to describe younger patients (because the skin is said to be as fragile as a butterflys wings),[3] "Cotton Wool Babies",[4][5] or (in South America) as "Crystal Skin Children".[6]Contents 1 Classification 1.1 Epidermolysis bullosa simplex 1.2 Junctional epidermolysis bullosa 1.3 Dystrophic epidermolysis bullosa 1.4 Other genetic 1.5 Other 2 Pathophysiology 3 Treatment 4 Epidemiology 5 Monitoring 6 See also 7 References 8 External linksClassificationEpidermolysis bullosa refers to a group of inherited disorders that involve the formation of blisters following trivial trauma. Over 300 mutations have been identified in this condition.[7] They have been classified into the following types:[8][9]:596Epidermolysis bullosa simplexMain article: Epidermolysis bullosa simplexEpidermolysis bullosa simplex is a form of epidermolysis bullosa that causes blisters at the site of rubbing. It typically affects the hands and feet, and is typically inherited in an autosomal dominant manner, affecting the keratin genes KRT5 and KRT14.Junctional epidermolysis bullosaMain article: Junctional epidermolysis bullosa (medicine)Junctional epidermolysis bullosa is an inherited disease affecting laminin and collagen. This disease is characterised by blister formation within the lamina lucida of the basement membrane zone[9]:599 and is inherited in an autosomal recessive manner. It also presents with blisters at the site of friction, especially on the hands and feet, and has variants that can occur in children and adults. Less than one per million people are estimated to have this form of epidemolysis bullosa.[10]Dystrophic epidermolysis bullosaMain article: Dystrophic epidermolysis bullosaDystrophic epidermolysis bullosa is an inherited variant affecting the skin and other organs. "Butterfly children" is the term given to those born with the disease, as their skin is seen to be as delicate and fragile as a butterfly's wings. Dystrophic epidermolysis bullosa is caused by genetic defects (or mutations) within the human COL7A1 gene encoding the protein type VII collagen (collagen VII).[11] DEB-causing mutations can be either autosomal dominant or autosomal recessive.Other geneticOMIMNameLocusGene
609638epidermolysis bullosa, lethal acantholytic6p24DSP
Other Epidermolysis bullosa acquisita Epidermolysis bullosa pruriginosaPathophysiologyThe human skin consists of two layers: an outermost layer called the epidermis and a layer underneath called the dermis. In individuals with healthy skin, there are protein anchors between these two layers that prevent them from moving independently from one another (shearing). In people born with EB, the two skin layers lack the protein anchors that hold them together, resulting in extremely fragile skineven minor mechanical friction (like rubbing or pressure) or trauma will separate the layers of the skin and form blisters and painful sores. Sufferers of EB have compared the sores with third-degree burns.[12] Furthermore, as a complication of the chronic skin damage, people suffering from EB have an increased risk of malignancies (cancers) of the skin.Treatment
Treatment of the epidermolysis bullosa by transplantation of laminin5 modified stem cellsRecent research has focused on changing the mixture of keratins produced in the skin. There are 54 known keratin genesof which 28 belong to the type I intermediate filament genes and 26 to type IIwhich work as heterodimers. Many of these genes share substantial structural and functional similarity, but they are specialized to cell type and/or conditions under which they are normally produced. If the balance of production could be shifted away from the mutated, dysfunctional keratin gene toward an intact keratin gene, symptoms could be reduced. For example, sulforaphane, a compound found in broccoli, was found to reduce blistering in a mouse model to the point where affected pups could not be identified visually, when injected into pregnant mice (5 mol/day = 0.9mg) and applied topically to newborns (1 mol/day = 0.2mg in jojoba oil).[13]As of 2008 clinical research at the University of Minnesota has included a bone marrow transplant to a 2-year-old child who is one of 2 brothers with EB. The procedure was successful, strongly suggesting that a cure may have been found. A second transplant has also been performed on the child's older brother, and a third transplant is scheduled for a California baby. The clinical trial will ultimately include transplants to 30 subjects.[14] However, the severe immunosuppression that bone marrow transplantation requires causes a significant risk of serious infections in patients with large scale blisters and skin erosions. Indeed, at least four patients have died in the course of either preparation for or institution of bone marrow transplantation for epidermolysis bullosa, out of only a small group of patients treated so far.A pilot study performed in 2015 suggests that systemic granulocyte-colony stimulating factor (G-CSF) may promote increased wound healing in patients with dystrophic epidermolysis bullosa. In this study seven patients with dystrophic epidermolysis bullosa were treated daily with subcutaneous G-CSF for six days and then re-evaluated on the seventh day. After six days of treatment with G-CSF, the size of the open lesions were reduced by a median of 75.5% and the number of blisters and erosions on the patients were reduced by a median of 36.6%. There will need to be many more studies using G-CSF as a treatment in epidermolysis bullosa, with a larger and more diverse patient population and a longer time frame, but this pilot study is encouraging for this new potential treatment.[15]EpidemiologyAn estimated 50 per million live births are diagnosed with EB, and 9 per million people in the general population have the condition. Of these cases, approximately 92% are epidermolysis bullosa simplex (EBS), 5% are dystrophic epidermolysis bullosa (DEB), 1% are junctional epidermolysis bullosa (JEB), and 2% are unclassified. Carrier frequency ranges from 1 in 333 for JEB, to 1 in 450 for DEB; the carrier frequency for EBS is presumed to be much higher than JEB or DEB.[citation needed]The disorder occurs in every racial and ethnic group and affects both sexes.[16][17]MonitoringThe Epidermolysis Bullosa Activity and Scarring index (EBDASI) is a scoring system that objectively quantifies the severity of epidermolysis bullosa. The EBDASI is a tool for clinicians and patients to monitor the severity of the disease. It has also been designed to evaluate the response to new therapies for the treatment of EB. The EBDASI was developed and validated by Professor Dedee Murrell and her team of students and fellows at the St George Hospital, University of New South Wales, in Sydney, Australia. It was presented at the International Investigative Dermatology congress in Edinburgh in 2013 and a paper-based version was published in the Journal of American Academy of Dermatology in 2014.[18]
IchthyosisFrom Wikipedia, the free encyclopediaIchthyosis
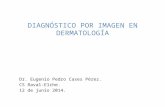
Ichthyosis is characterized by rough, scaly skin.
Classification and external resources
SpecialtyDermatology
ICD-10Q80
ICD-9-CM757.1
DiseasesDB6646
MeSHD007057
[edit on Wikidata]
Ichthyosis (plural ichthyoses) is a heterogeneous family of at least 28,[1] generalized, mostly genetic skin disorders.All types of ichthyosis have dry, thickened, scaly or flaky skin.[1] In many types there is cracked skin,[2] which is said to resemble the scales on a fish; the word ichthyosis comes from the Ancient Greek (ichthys), meaning "fish."[3]The severity of symptoms can vary enormously, from the mildest, most common, type such as ichthyosis vulgaris which may be mistaken for normal dry skin up to life-threatening conditions such as harlequin type ichthyosis. Ichtyosis vulgaris accounts for more than 95% of cases.[4]Contents 1 Types 1.1 Genetic simple ichthyoses 1.2 Genetic disease with ichthyosis 1.3 Non-genetic ichthyosis 2 Diagnosis 3 Treatments 4 Other animals 5 See also 6 References 7 External linksTypesThere are many types of ichthyoses and an exact diagnosis may be difficult. Types of ichthyoses are classified by their appearance and their genetic cause. Ichthyosis caused by the same gene can vary considerably in severity and symptoms. Some ichthyoses do not appear to fit exactly into any one type. Also different genes can produce ichthyoses with similar symptoms. Of note, X-linked ichthyosis is associated with Kallmann syndrome (close to KAL1 gene). The most common or well-known types are as follows:[5]Genetic simple ichthyosesNameOMIMGeneProtein
Ichthyosis vulgaris146700FLGFilaggrin
X-linked ichthyosis308100STSSteroid sulfatase
Congenital ichthyosiform erythroderma, Nonbullous (nbCIE)242100TGM1, ALOXE3/ALOX12BTransglutaminase 1Arachidonate lipoxygenase 3Arachidonate 12-lipoxygenase, 12R type
Epidermolytic hyperkeratosis (bullous ichthyosis, bCIE)113800KRT1, KRT10Keratins
Harlequin-type ichthyosis242500ABCA12ATP-binding cassette transporter 12
Ichthyosis bullosa of Siemens146800KRT2Keratin 2A
Ichthyosis hystrix, Curth-Macklin type146590KRT1Keratin 1
Hystrix-like ichthyosis with deafness602540GJB2Connexin-26 (Gap junction beta-2)
Lamellar ichthyosis, type 1242300TGM1Transglutaminase 1
Lamellar ichthyosis, type 2601277ABCA12ATP-binding cassette transporter 12
Lamellar ichthyosis, type 3604777CYP4F22Cytochrome P450, subfamily 4F, polypeptide 22
Lamellar ichthyosis, type 4613943LIPNLipase family, member N
Lamellar ichthyosis, type 5606545ALOXE3Arachidonate lipoxygenase 3
Autosomal Recessive Congenital Ichthyosis[6]615023CERS3ceramide synthase 3
Genetic disease with ichthyosisNameOMIMGeneProtein
CHILD Syndrome308050NSHDLNAD(P) dependent steroid dehydrogenase-like
Conradi-Hnermann syndrome302960EBPEmopamil binding protein
Ichthyosis follicularis with alopecia and photophobia syndrome308205MBTPS2Membrane-bound transcription factor peptidase, site 2
Keratitis-ichthyosis-deafness syndrome148210GJB2Connexin-26
Netherton syndrome256500SPINK5Serine peptidase inhibitor, Kazal type 5
Neutral lipid storage disease with ichthyosis275630ABHD51-acylglycerol-3-phosphate O-acyltransferase
Adult Refsum disease266500PHYHPEX7Phytanoyl-CoA hydroxylasePeroxin 7
Ichthyosis and male hypogonadism308200?
Sjgren-Larsson syndrome270200ALDH3A2Fatty acid dehydrogenase
Photosensitive trichothiodystrophy (IBIDS syndrome)601675ERCC2, ERCC3, GTF2H5Transcription factor IIH components
Gaucher Disease, type 2230900GBAGlucocerebrosidase
Non-genetic ichthyosis Ichthyosis acquisitaDiagnosisA physician often can diagnose ichthyosis by looking at the skin. A family history is very useful. In some cases, a skin biopsy is done to help to confirm the diagnosis. In some instances, genetic testing may be helpful in making a diagnosis. Diabetes has not been definitively linked to acquired ichthyosis or ichthyosis vulgaris; however, there are case reports associating new onset ichthyosis with diabetes.[7]Ichthyosis has been found to be more common in any Native American, Asian, Mongolian group. As of now, there is no way to prevent ichthyosis.TreatmentsTreatments for ichthyosis often take the form of topical application of creams and emollient oils, in an attempt to hydrate the skin. Creams containing lactic acid have been shown to work exceptionally well in some cases.[citation needed] Application of Propylene Glycol has been used as another treatment method. Retinoids are also used for some conditions.Exposure to sunlight may improve[citation needed] or worsen the condition. In some cases, excess dead skin sloughs off much better from wet tanned skin after bathing or a swim, although the dry skin might be preferable to the damaging effects of sun exposure.There can be ocular manifestations of ichthyosis, such as corneal and ocular surface diseases. Vascularizing keratitis, which is more commonly found in congenital keratitis-ichythosis-deafness (KID), may worsen with isotretinoin therapy.
Palmoplantar keratodermaFrom Wikipedia, the free encyclopediaPalmoplantar keratoderma
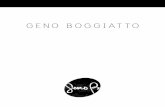
A picture of a 40 y/o Caucasian female with only the soles of the feet affected. The amputation was prior to this admission
Classification and external resources
Specialtydermatology
ICD-10L85.1-L85.2, Q82.8
ICD-9-CM701.1, 757.39
OMIM144200 600962
DiseasesDB32042
eMedicinederm/589
MeSHD007645
[edit on Wikidata]
Palmoplantar keratodermas are a heterogeneous group of disorders characterized by abnormal thickening of the palms and soles.Autosomal recessive and dominant, X-linked, and acquired forms have all been described.[1]:505[2]:211[3]Contents 1 Clinical patterns 1.1 Diffuse 1.2 Focal 1.3 Punctate 1.4 Ungrouped 2 Genetics 3 See also 4 ReferencesClinical patternsClinically, three distinct patterns of palmoplantar keratoderma may be identified: diffuse, focal, and punctate.[1]:505DiffuseDiffuse palmoplantar keratoderma is a type of palmoplantar keratoderma that is characterized by an even, thick, symmetric hyperkeratosis over the whole of the palm and sole, usually evident at birth or in the first few months of life.[1]:505 Restated, diffuse palmoplantar keratoderma is an autosomal dominant disorder in which hyperkeratosis is confined to the palms and soles.[4] The two major types can have a similar clinical appearance:[4] Diffuse epidermolytic palmoplantar keratoderma (also known as "Palmoplantar keratoderma cum degeneratione granulosa Vrner," "Vrner's epidermolytic palmoplantar keratoderma", and "Vrner keratoderma"[4]) is one of the most common patterns of palmoplantar keratoderma, an autosomal dominant condition that presents within the first few months of life, characterized by a well-demarcated, symmetric thickening of palms and soles, often with a "dirty" snakeskin appearance due to underlying epidermolysis.[1]:506 Diffuse nonepidermolytic palmoplantar keratoderma (also known as "Diffuse orthohyperkeratotic keratoderma," "Hereditary palmoplantar keratoderma," "Keratosis extremitatum progrediens," "Keratosis palmoplantaris diffusa circumscripta," "Tylosis," "UnnaThost disease", and "UnnaThost keratoderma"[4]) is inherited as an autosomal dominant condition and is present from infancy, characterized by a well-demarcated, symmetric, often "waxy" keratoderma involving the whole of the palms and soles.[1]:5068[2]:213FocalFocal palmoplantar keratoderma, a type of palmoplantar keratoderma in which large, compact masses of keratin develop at sites of recurrent friction, principally on the feet, although also on the palms and other sites, a pattern of calluses that may be discoid (nummular) or linear. Focal palmoplantar keratoderma with oral mucosal hyperkeratosis (also known as "Focal epidermolytic palmoplantar keratoderma,"[4] "Hereditary painful callosities,"[4][5] "Hereditary painful callosity syndrome,"[1] "Keratosis follicularis,"[1] "Keratosis palmoplantaris nummularis",[1] and "Nummular epidermolytic palmoplantar keratoderma"[4]) is an autosomal dominant keratoderma that represents a clinical overlap syndrome with pachyonychia congenita type I but without the classic nail involvement.[1]:510PunctatePunctate palmoplantar keratoderma is a form of palmoplantar keratoderma in which many tiny "raindrop" keratoses involve the palmoplantar surface, skin lesions which may involve the whole of the palmoplantar surface, or may be more restricted in their distribution.[1]:505[4] Type 1: Keratosis punctata palmaris et plantaris (also known as "Autosomal-dominant hereditary punctate keratoderma associated with malignancy," "BuschkeFischerBrauer disease," "Davis Colley disease," "Keratoderma disseminatum palmaris et plantaris," "Keratosis papulosa," "Keratoderma punctatum," "Keratodermia punctata," "Keratoma hereditarium dissipatum palmare et plantare," "Palmar and plantar seed dermatoses," "Palmar keratoses," "Papulotranslucent acrokeratoderma," "Punctate keratoderma," "Punctate keratoses of the palms and soles," and "Maculosa disseminata") is a skin condition, an autosomal dominant palmoplantar keratoderma with variable penetrance, characterized clinically by multiple, tiny, punctate keratoses over the entire palmoplantar surfaces, beginning over the lateral edge of the digits.[1]:509[2]:212213 It has been linked to 15q22-q24.[6] Type 2: Spiny keratoderma (also known as "Porokeratosis punctata palmaris et plantaris," "Punctate keratoderma," and "Punctate porokeratosis of the palms and soles") is an autosomal dominant keratoderma of late onset that develops in patients aged 12 to 50, characterized by multiple tiny keratotic plugs, mimicking the spines on a music box, involving the entire palmoplantar surfaces.[1]:509[4] Type 3: Focal acral hyperkeratosis (also known as "Acrokeratoelastoidosis lichenoides," and "Degenerative collagenous plaques of the hand") is a late-onset keratoderma, inherited as an autosomal dominant condition, characterized by oval or polygonal crateriform papules developing along the border of the hands, feet, and wrists.[1]:509 It is considered similar to Costa acrokeratoelastoidosis.[7]Ungrouped Palmoplantar keratoderma and spastic paraplegia (also known as "CharcotMarieTooth disease with palmoplantar keratoderma and nail dystrophy"[1]) is an autosomal dominant or x-linked dominant condition that begins in early childhood with thick focal keratoderma over the soles and, to a lesser extent, the palms.[1]:513 Palmoplantar keratoderma of Sybert (also known as "Greither palmoplantar keratoderma,"[1] "Greither syndrome,"[4] "Keratosis extremitatum hereditaria progrediens,"[1] "Keratosis palmoplantaris transgrediens et progrediens"[1] "Sybert keratoderma,"[4] and "Transgrediens and progrediens palmoplantar keratoderma"[4]) is an extremely rare autosomal dominant[8] keratoderma (a skin condition involving horn-like growths) with symmetric severe involvement of the whole palmoplantar surface in a glove-and-stocking distribution.[1]:509 It was characterized by Aloys Greither in 1952.[9][10][11] It was characterized by Virginia Sybert in 1988.[12] Striate palmoplantar keratoderma (also known as "Acral keratoderma,"[1] "Brnauer-Fuhs-Siemens type of palmoplantar keratoderma,"[1] "Focal non-epidermolytic palmoplantar keratoderma,"[4] "Keratosis palmoplantaris varians,"[1] "Palmoplantar keratoderma areata,"[4] "Palmoplantar keratoderma striata,"[4] "Wachter keratoderma,"[4]:778,785 and "Wachters palmoplantar keratoderma"[1]) is a cutaneous condition, an autosomal dominant keratoderma principally involving the soles with onset in infancy or the first few years of life.[1]:509 Type 1: 148700: DSG1 Type 2: 612908: DSP Type 3: 607654: KRT1 Carvajal syndrome (also known as "Striate palmoplantar keratoderma with woolly hair and cardiomyopathy"[4] and "Striate palmoplantar keratoderma with woolly hair and left ventricular dilated cardiomyopathy,"[1]) is a cutaneous condition inherited in an autosomal recessive fashion, and due to a defect in desmoplakin.[4]:811 Striate palmoplantar keratoderma, woolly hair, and left ventricular dilated cardiomyopathy has been described in both autosomal dominant and autosomal recessive forms, but only the recessive forms have a clear association with dilated cardiomyopathy.[1]:513 The skin disease presents as a striate palmoplantar keratoderma with some nonvolar involvement, particularly at sites of pressure or abrasion.[1]:513 Scleroatrophic syndrome of Huriez (also known as "Huriez syndrome," "Palmoplantar keratoderma with scleroatrophy,"[4] "Palmoplantar keratoderma with sclerodactyly," "Scleroatrophic and keratotic dermatosis of the limbs," and "Sclerotylosis") is an autosomal dominant keratoderma with sclerodactyly present at birth with a diffuse symmetric keratoderma of the palms and soles.[1]:513[2]:576 An association with 4q23 has been described.[13] It was characterized in 1968.[14] Vohwinkel syndrome (also known as "Keratoderma hereditaria mutilans,"[4] "Keratoma hereditaria mutilans,"[4] "Mutilating keratoderma of Vohwinkel",[2]:213 "Mutilating palmoplantar keratoderma"[4]) is a diffuse autosomal dominant keratoderma with onset in early infancy characterized by a honeycombed keratoderma involving the palmoplantar surfaces.[1]:512 Mild to moderate sensorineural hearing loss is often associated.[1] It has been associated with GJB2.[15] It was characterized in 1929.[16] Olmsted syndrome (also known as "Mutilating palmoplantar keratoderma with periorificial keratotic plaques," "Mutilating palmoplantar keratoderma with periorificial plaques"[4] and "Polykeratosis of Touraine") is a keratoderma of the palms and soles, with flexion deformity of the digits, that begins in infancy.[1]:510[2]:214[4] Treatment with retinoids has been described.[17] It has been associated with mutations in TRPV3.[18] Aquagenic keratoderma, also known as acquired aquagenic palmoplantar keratoderma,[4]:788transient reactive papulotranslucent acrokeratoderma,[4] aquagenic syringeal acrokeratoderma,[4] and aquagenic wrinkling of the palms,[2] is a skin condition characterized by the development of white papules on the palms after water exposure.[2]:215 The condition causes irritation of the palms when touching certain materials after being wet, e.g., paper, cloth. An association with cystic fibrosis has been suggested.[19]
NeurofibromatosisFrom Wikipedia, the free encyclopediaNeurofibromatosis
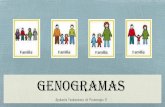
Back of an elderly woman with neurofibromatosis
Classification and external resources
SpecialtyNeurosurgery
ICD-10Q85.0
ICD-9-CM237.7
ICD-OM9540/0
OMIM162200 101000,162091
eMedicinederm/287
Patient UKNeurofibromatosis
MeSHD017253
[edit on Wikidata]
Neurofibromatosis (NF) refers to several genetically inherited conditions that are clinically and genetically different and carry a high possibility of tumor formation.[1] This disorder is divided into Neurofibromatosis type 1, Neurofibromatosis type 2 and Schwannomatosis.[2]Contents 1 Signs 2 Cause 3 Pathophysiology 4 Diagnosis 5 Treatment 6 Prognosis 7 Epidemiology 8 See also 9 References 10 Further reading 11 External linksSignsNeurofibromatosis (NF1) in early life may cause learning and behavior problems, about 60% of children who have NF1 have a mild form of difficulty in school.[3] In terms of signs the individual might have are the following:[4][5] Six or more light brown dermatological spots (caf-au-lait spots") At least two neurofibromas At least two growths on the eye's iris Abnormal growth of the spine (scoliosis)CauseNeurofibromatosis is an autosomal dominant disorder, which means only one copy of the affected gene is needed for the disorder to develop. Therefore, if only one parent has neurofibromatosis, his or her children have a 50% chance of developing the condition as well.The affected child could have mild NF1 even though inherited from a parent with a severe form of the disorder.[6] The types of neurofibromatosis are: Neurofibromatosis type I, in which the nerve tissue grows tumors (neurofibromas) that may be benign and may cause serious damage by compressing nerves and other tissues.[7] Neurofibromatosis type II, in which bilateral acoustic neuromas (tumors of the vestibulocochlear nerve or cranial nerve 8 (CN VIII) also known as schwannoma) develop, often leading to hearing loss.[8] Schwannomatosis, in which painful schwannomas develop on spinal and peripheral nerves.[9]PathophysiologyThe pathophysiology of neurofibromatosis (type 1) consists of the NF1 gene protein.[10] This protein is a tumor suppressor and therefore serves as a signal regulator of cell proliferation and differentiation. A dysfunction of neurofibromin can affect regulation, and cause uncontrolled cell proliferation. Schwann cells in neurofibromas have a mutation in the NF1 alleles.[11]Diagnosis
CT scanThe neurofibromatoses are considered as RASopathies and as members of the neurocutaneous syndromes (phakomatoses).[12] Conditions which may be confused with NF-1 but which are not considered NF include, LEOPARD syndrome,[13] and Legius syndrome[14] The diagnosis of neurofibromatosis is done via the following means:[15] Radiograph MRI or CT scan EEG Slit-lamp examination Genetic testing HistologyTreatmentSurgical removal of tumors is an option, however the risks involved should be assessed first[16] With regard to OPG (optic pathway gliomas) the preferred treatment is chemotherapy, However radiotherapy isn't recommended in children who present with this disorder.[17] It is recommended that at an early age children diagnosed with NF1 have an examination each year, this is a form of monitoring any potential growths or changes related to the disorder.[18]PrognosisIn most cases, symptoms of NF1 are mild, and individuals live normal and productive lives. In some cases, however, NF1 can be severely debilitating and may cause cosmetic and psychological issues.[medical citation needed] The course of NF2 varies greatly among individuals. In some cases of NF2, the damage to nearby vital structures, such as other cranial nerves and the brain stem, can be life-threatening. Most individuals with schwannomatosis have significant pain. In some extreme cases the pain will be severe and disabling.[5]EpidemiologyNF1 occurs 1 in 3000 individuals, and is equal among men and women. Furthermore, it is among the most common inherited nervous system disorders.[19] Such individuals have a 10 to 15 year reduction in life expectancy compared to the average person.[20]See alsoIncontinentia pigmentiFrom Wikipedia, the free encyclopediaThe lead section of this article may need to be rewritten. Please discuss this issue on the article's talk page. Use the lead layout guide to ensure the section will be inclusive of all essential details. (August 2010)
Incontinentia pigmenti
Classification and external resources
Specialtymedical genetics
ICD-10Q82.3
ICD-9-CM757.33
OMIM308300
DiseasesDB29600
MedlinePlus001583
eMedicinearticle/1114205 article/1176285
MeSHD007184
GeneReviews Incontinentia pigmenti
[edit on Wikidata]
Incontinentia pigmenti (IP, also known as "BlochSiemens syndrome,"[1] "BlochSulzberger disease,"[2] "BlochSulzberger syndrome"[1] "melanoblastosis cutis," and "nevus pigmentosus systematicus") is a genetic disorder that affects the skin, hair, teeth, nails, and central nervous system. It is named due to its microscopic appearance.Contents 1 Presentation 2 Diagnosis 3 Genetics 4 History 5 See also 6 References 7 External linksPresentation
Incontinentia pigmenti forming along Blaschko's lines in a 3-year-old girl.The skin lesions evolve through characteristic stages:1. blistering (from birth to about four months of age),2. a wart-like rash (for several months),3. swirling macular hyperpigmentation (from about six months of age into adulthood), followed by4. linear hypopigmentation.Alopecia, hypodontia, abnormal tooth shape, and dystrophic nails are observed. Some patients have retinal vascular abnormalities predisposing to retinal detachment in early childhood. Cognitive delays/mental retardation are occasionally seen.Discolored skin is caused by excessive deposits of melanin (normal skin pigment). Most newborns with IP will develop discolored skin within the first two weeks. The pigmentation involves the trunk and extremities, is slate-grey, blue or brown, and is distributed in irregular marbled or wavy lines. The discoloration sometimes fades with age.Neurological problems can include: cerebral atrophy, the formation of small cavities in the central white matter of the brain, and the loss of neurons in the cerebellar cortex. About 20% of children with IP will have slow motor development, muscle weakness in one or both sides of the body, mental retardation, and seizures. They are also likely to have visual problems, which can include: crossed eyes, cataracts, and severe visual loss. Dental problems are common, and include missing or peg-shaped teeth - patients with IP often keep milk teeth into adult life.Breast anomalies can occur in 1% of patients; anomalies can include hypoplasia and supernumerary nipples.Skeletal and structural anomalies can occur in approximately 14% of patients, including: Somatic asymmetry, Hemivertebrae, Scoliosis, Spina bifida, Syndactyly, Acheiria (congenital absence of the hands - note: other limbs may be affected), Ear anomalies, Extra ribs, Skull deformities, Primary pulmonary hypertension, Cardiopulmonary failureDiagnosisThe diagnosis of IP is established by clinical findings and occasionally by corroborative skin biopsy. Molecular genetic testing of the NEMO IKBKG gene (chromosomal locus Xq28) reveals disease-causing mutations in about 80% of probands. Such testing is available clinically.In addition, females with IP have skewed X-chromosome inactivation; testing for this can be used to support the diagnosis.Many people in the past were misdiagnosed with a second type of IP, formerly known as IP1. This has now been given its own name - 'Hypomelanosis of Ito' (incontinentia pigmenti achromians). This has a slightly different presentation: swirls or streaks of hypopigmentation and depigmentation. It is not inherited and does not involve skin stages 1 or 2. Some 3350% of patients have multisystem involvement eye, skeletal, and neurological abnormalities. Its chromosomal locus is at Xp11, rather than Xq28.GeneticsIP is inherited in an X-linked dominant manner.[3][4] IP is lethal in most, but not all, males. A female with IP may have inherited the IKBKG mutation from either parent or have a new gene mutation. Parents may either be clinically affected or have germline mosaicism. Affected women have a 50% risk of transmitting the mutant IKBKG allele at conception; however, most affected male conceptuses miscarry. Thus, the expected ratio for liveborn children is 33% unaffected females, 33% affected females, and 33% unaffected males. Genetic counseling, prenatal testing, and preimplantation genetic diagnosis is available.In females, the cells expressing the mutated IKBKG gene due to lyonization selectively die around the time of birth so the X-inactivation is extremely skewed.[5]IP is caused by mutations in a gene called NEMO (NF-kappaB essential modulator).
Restrictive dermopathyFrom Wikipedia, the free encyclopediaRestrictive dermopathy
Classification and external resources
Specialtymedical genetics
ICD-10Q82.8
OMIM275210
DiseasesDB32974
[edit on Wikidata]
Restrictive dermopathy is a rare, lethal autosomal recessive skin condition characterized by abnormal facies, tight skin, sparse or absent eyelashes, and secondary joint changes.[1]:563MechanismRestrictive dermopathy (RD) is caused either by the loss of the gene ZMPSTE24, which encodes a protein responsible for the cleavage of farnesylated prelamin A (progerin) into mature non-farnesylated lamin, or by a mutation in the LMNA gene. This results in the accumulation of farnesyl-prelamin A at the nuclear membrane.[2] Mechanistically, restrictive dermopathy is somewhat similar to Hutchinson-Gilford progeria syndrome (HGPS), a disease where the last step in lamin processing is hindered by a mutation that causes the loss of the ZMPSTE24 cleavage site in the lamin A gene.See also Relapsing linear acantholytic dermatosis List of cutaneous conditions Lamellar ichthyosis - Possible differential diagnosisReferences1. James, William; Berger, Timothy; Elston, Dirk (2005). Andrews' Diseases of the Skin: Clinical Dermatology. (10th ed.). Saunders. ISBN 0-7216-2921-0.2. Young SG, Meta M, Yang SH, Fong LG (December 2006). "Prelamin A farnesylation and progeroid syndromes". J. Biol. Chem. 281 (52): 3974139745. doi:10.1074/jbc.R600033200. PMID17090536.