Genitourinary Injuries in the Newborn - Pediatric Surgical ... · highlight the iatrogenic nature...
5
Genitourinary Injuries in the Newborn By Haroon I. Patel, Kevin P. Moriarty, Paul A. Brisson, and Neil R. Feins Boston, Massachusetts; Springfield, Massachusetts; and Schenectady, New York Background: Circumcisions and cesarian sections are com- mon procedures. Although complications to the newborn child fortunately are rare, it is important to emphasize the potential significance of this problem and its frequent iatro- genic etiology. The authors present 7 cases of genitourinary trauma in newborns, including surgical management and follow-up. Methods: The authors relate 7 recent cases of genitourinary trauma in newborns from a children's hospital in a major metropolitan area. Results: Case 1 and 2: Two infants suffered degloving inju- ries to both the prepuce and penile shaft from a Gomco clamp. Successful full-thickness skin grafting using the pre- viously excised foreskin was used in 1 child. Case 3, 4, and 5: A Mogen clamp caused glans injuries in 3 infants. In 2, hemorrhage from the severed glans was controlled with topical epinephrine; the glans healed with a flattened appear- ance. Another infant sustained a laceration ventrally, requir- ing a delayed modified meatal advancement glanoplasty to correct the injury. Case 6: A male infant suffered a ventral slit and division of the ventral urethra before placement of a Gomco clamp. Formal hypospadias repair was required. Case 7: An emergent cesarean section resulted in a grade 4-perineal laceration in a female infant. The vaginal tear caused by the surgeon's finger, extended up to the posterior insertion of the cervix and into the rectum. The infant successfully underwent an emergent multilayered repair. Conclusions: Genitourinary trauma in the newborn is rare but often necessitates significant surgical intervention. Cir- cumcision often is the causative event. There has been only 1 prior report of a perineal injury similar to case 7, with a fatal outcome. J Pediatr Surg 36:235-239. Copyright © 2001 by W.B. Saunders Company. INDEX WORDS: Newborn genitourinary trauma, circumci- sion injuries, birth trauma. T RAUMATIC INJURIES to the external genitalia in the newborn period are relatively infrequent. The medical literature is replete with reports of traumatic genital injury in older children 1-4 mainly as a result of varying forms of accidental, self-inflicted, or abuse- related trauma. However, it is evident from the published literature that the newborn child belongs to a distinct group of patients who are victims of iatrogenic injuries more often than older children. 5-8 Circumcisions and cesarean sections are among the most common procedures performed in the United States. The controversy surrounding nonritual circumcisions con- tinues to rage. 942 Complications from circumcisions, the most frequently performed operation in the United States, and the treatment thereof, are elegantly covered else- where, t3 Also, despite the reduction in morbidity and mor- tality from birth trauma, probably related to improved perinatal care, the actual incidence of external birth trauma has not always shown a proportionate decrease. 6,s,14 The purpose of this report is not to discuss the pros and cons of circumcision and cesarean section, but rather to highlight the iatrogenic nature of genitourinary injuries in the newborn. By themselves, these injuries usually are not life threatening but are a significant cause of anxiety for obstetricians, pediatricians, and the parents of the injured newborn child. The possibility of serious morbidity, permanent dis- ability, as well as litigation are all issues that compound the problem that the pediatric surgeon has to deal with. This report, which includes 7 cases referred to our center as well as 1 additional case submitted by another pedi- atric surgeon in response to a prior report of our seventh case, serves 3 purposes: (1) it highlights the iatrogenic nature of these injuries; (2) it provides management options, some of which have not been described previ- ously; (3) it emphasizes the importance of reporting these injuries to gain broader experience so that practi- tioners who perform the majority of circumcisions and cesarean sections hopefully will institute appropriate preventive measures. MATERIALS AND METHODS All patients referred to the pediatric surgical service between July 1995 and June 1998 for genitourinary injuries were included. These patients were all newborn children (6 boys and 1 girl), and all sustained From the Division of Pediatric Surgery, The Floating Hospital for Children, Boston, MA. Presented at the 31st Annual Meeting of the American Pediatric Surgical Association, Orlando, Florida, May 25-29, 2000. Address reprint requests to Haroon L Patel, MBBCh, One BMC Place, Dowling 2, Suite 2414, Boston, MA 02118. Copyright © 2001 by W.B. Saunders Company 0022-3468/01/3601-0044503. 00/0 doi: l O.l O53/jpsu.2001.20062 Journal of Pediatric Surgery, Vol 36, No 1 (January), 2001: pp 235-239 235
Transcript of Genitourinary Injuries in the Newborn - Pediatric Surgical ... · highlight the iatrogenic nature...

Genitourinary Injuries in the Newborn By Haroon I. Patel, Kevin P. Mor ia r ty , Paul A. Brisson, and Neil R. Feins
Boston, Massachusetts; Springfield, Massachusetts; and Schenectady, New York
Background: Circumcisions and cesarian sections are com- mon procedures. Although complications to the newborn child fortunately are rare, it is important to emphasize the potential significance of this problem and its frequent iatro- genic etiology. The authors present 7 cases of genitourinary trauma in newborns, including surgical management and follow-up.
Methods: The authors relate 7 recent cases of genitourinary trauma in newborns from a children's hospital in a major metropolitan area.
Results: Case 1 and 2: Two infants suffered degloving inju- ries to both the prepuce and penile shaft from a Gomco clamp. Successful full-thickness skin grafting using the pre- viously excised foreskin was used in 1 child. Case 3, 4, and 5: A Mogen clamp caused glans injuries in 3 infants. In 2, hemorrhage from the severed glans was controlled with topical epinephrine; the glans healed with a flattened appear- ance. Another infant sustained a laceration ventrally, requir- ing a delayed modified meatal advancement glanoplasty to
correct the injury. Case 6: A male infant suffered a ventral slit and division of the ventral urethra before placement of a Gomco clamp. Formal hypospadias repair was required. Case 7: An emergent cesarean section resulted in a grade 4-perineal laceration in a female infant.
The vaginal tear caused by the surgeon's finger, extended up to the posterior insertion of the cervix and into the rectum. The infant successfully underwent an emergent multilayered repair.
Conclusions: Genitourinary trauma in the newborn is rare but often necessitates significant surgical intervention. Cir- cumcision often is the causative event. There has been only 1 prior report of a perineal injury similar to case 7, with a fatal outcome. J Pediatr Surg 36:235-239. Copyright © 2001 by W.B. Saunders Company.
INDEX WORDS: Newborn genitourinary trauma, circumci- sion injuries, birth trauma.
T RAUMATIC INJURIES to the external genitalia in the newborn period are relatively infrequent. The
medical literature is replete with reports of traumatic genital injury in older children 1-4 mainly as a result of varying forms of accidental, self-inflicted, or abuse- related trauma. However, it is evident from the published literature that the newborn child belongs to a distinct group of patients who are victims of iatrogenic injuries more often than older children. 5-8
Circumcisions and cesarean sections are among the most common procedures performed in the United States. The controversy surrounding nonritual circumcisions con- tinues to rage. 942 Complications from circumcisions, the most frequently performed operation in the United States, and the treatment thereof, are elegantly covered else- where, t3 Also, despite the reduction in morbidity and mor- tality from birth trauma, probably related to improved perinatal care, the actual incidence of external birth trauma has not always shown a proportionate decrease. 6,s,14
The purpose of this report is not to discuss the pros and cons of circumcision and cesarean section, but rather to highlight the iatrogenic nature of genitourinary injuries in the newborn. By themselves, these injuries usually are not life threatening but are a significant cause of anxiety for obstetricians, pediatricians, and the parents of the injured newborn child.
The possibility of serious morbidity, permanent dis-
ability, as well as litigation are all issues that compound the problem that the pediatric surgeon has to deal with. This report, which includes 7 cases referred to our center as well as 1 additional case submitted by another pedi- atric surgeon in response to a prior report of our seventh case, serves 3 purposes: (1) it highlights the iatrogenic nature of these injuries; (2) it provides management options, some of which have not been described previ- ously; (3) it emphasizes the importance of reporting these injuries to gain broader experience so that practi- tioners who perform the majority of circumcisions and cesarean sections hopefully will institute appropriate preventive measures.
MATERIALS AND METHODS
All patients referred to the pediatric surgical service between July 1995 and June 1998 for genitourinary injuries were included. These patients were all newborn children (6 boys and 1 girl), and all sustained
From the Division of Pediatric Surgery, The Floating Hospital for Children, Boston, MA.
Presented at the 31st Annual Meeting of the American Pediatric Surgical Association, Orlando, Florida, May 25-29, 2000.
Address reprint requests to Haroon L Patel, MBBCh, One BMC Place, Dowling 2, Suite 2414, Boston, MA 02118.
Copyright © 2001 by W.B. Saunders Company 0022-3468/01/3601-0044503. 00/0 doi: l O.l O53/jpsu.2001.20062
Journal of Pediatric Surgery, Vol 36, No 1 (January), 2001: pp 235-239 235
236 PATEL ET AL
B
/ / /
\
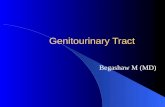
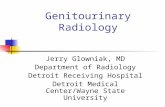
Fig 1, (A) Photograph and (B) diagram of a denudation injury (case 2). Too much penile skin was drawn up into the Gomco clamp and excised,
injuries related to either circumcision or cesarean section. We excluded injuries beyond the perinatal period (7 days). There were no other injuries in any of these neonates. There were no deaths in this series, and follow-up (1 to 4 years) examination showed satisfactory func- tional and cosmetic results. There were no immediate or delayed complications related to the salvage procedures. The cases are outlined below and are grouped together based on the mechanism of injury.
Cases 1 and 2
These 2 infants suffered degloving injuries to both the prepuce and penile shaft from a Gomco clamp. Too much skin had been drawn up and severed (Fig 1). In the first patient, the error was only realized after the skin had been disposed of, and it was noticed that there was a denuded area of penile shaft. This healed by secondary intention (Fig 2). In the second case, the previously excised foreskin was salvaged
and successfully sewn on as a full-thickness skin graft. Both these patients had satisfactory healing. However, the child who underwent grafting recovered sooner, required fewer dressing changes that were painful, and we believe had a superior cosmetic result.
Cases 3, 4, and 5
A Mogen clamp caused glans injuries in these 3 neonates. The patients in cases 3 and 4 had minor amputations of the glans. In both cases, persistent hemorrhage from the severed glans drew attention to the injury. Hemostasis was achieved by intermittently placing a solu- tion of epinephrine 1:1,000 on the bleeding glans using a cotton tipped applicator. The glans healed with a flattened appearance in both these patients. The patient in case 5 had, in addition to the partial glans amputation, a laceration that extended ventrally. A delayed modified meatal advancement glanoplasty was required at 6 months to correct the injury.
Case 6
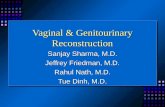
This male infant had an injury to the ventral urethra before place- ment of a Gomco clamp. The pediatrician, in trying to get the bell of the Gomco clamp to fit, performed a ventral instead of dorsal slit, produc- ing this injury (Fig 3). A formal tubularized, incised plate urethroplasty, as described by Snodgrass 15 was required.
Case 7
This unfortunate female neonate sustained a grade 4 perineal lacer- ation during an emergent cesarean section. The vaginal tear extended up to the posterior insertion of the cervix as well as into the rectum. The patient successfully underwent an emergent multilayered repair.
Based on the published report of this case, ~6 a pediatric surgeon from New York (see acknowledgment) submitted his experience with a very similar case. The injury in his patient was similarly caused by the obstetrician's finger during a difficult and emergent cesarean section. The injury was almost identical with the exception of more swelling of the clitoris and urethral meatus. He similarly repaired this injury emergently with a successful outcome both functionally and cosmeti- cally.
D I S C U S S I O N
It is wel l k n o w n tha t t r a u m a is a m a j o r cause o f
m o r b i d i t y and mor ta l i ty in the pedia t r ic popula t ion . 5,7
T h e n e w b o r n ch i ld is re la t ive ly spa red f r o m t r a u m a un t i l
they are m o r e mob i l e . Unfo r tuna t e ly , h o w e v e r , they are
no t as p ro tec ted aga ins t i a t rogen ic injur ies . A l t h o u g h
gen i tou r ina ry t r a u m a is dea l t w i th c o m p r e h e n s i v e l y in
m a n y reports , 1-4 these ser ies i l lus t ra te the ra r i ty of non i -
a t rogen ic n e w b o r n gen i tou r ina ry injur ies . C i r c u m c i s i o n s
and b i r th t r a u m a acco u n t for the ma jo r i t y of cases.
Ex te rna l b i r t h t r a u m a an d its r epor t ing var ies f r o m
reg ion to region. 6,a,~4 It is r e la ted to m a n y factors , in-
c luding , a m o n g others , i nc r ea sed fetal size; m a n i p u l a t i o n
du r ing difficult , p ro longed , or i n s t r u m e n t a l de l iver ies ; as
wel l as v a ry i n g per ina ta l prac t ices . 8,14 C e s a r e a n sec t ion
con t inues to b e p e r f o r m e d f requen t ly to p r e v e n t b i r th
t rauma, an d the ra te o f c e sa r ean sec t ion in N o r t h A m e r -
ica is the h i g h es t in the d e v e l o p e d world . M a n y d i f fe ren t
sys t em in jur ies re la ted to b o t h diff icul t de l ive r ies and
ce sa r ean sec t ions h a v e b e e n descr ibed , 6,8 bu t the geni to-
u r inary sys t em is i n v o l v e d in f requent ly , M o s t of these

GENITOURINARY INJURIES 237
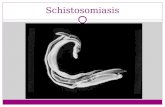
Fig 2. (A) Photograph and (B) diagram of case 1 shows exudate on the denuded area left to heal by secondary intention. (C) Final result after approximately 6 weeks.
injuries are relatively minor, eg, bruising, and often go unreported. Breech delivery and the associated fetal manipulation have been associated with scrotal and tes- ticular injuries? 7 Bhat et all 8 reported the first case in the literature of a fatal perineal tear in a female neonate from
attempted breech delivery. A subsequent rectovaginal tear in a neonate after cesarean section (case 7) was reported by 2 of the current authors. 16 Since then, we were made aware of a similar unpublished case, which was successfully salvaged by a pediatric surgeon (see

238 PATEL ET AL
A
\
\
!
B
J J
/ / /
/
/ /
/ i
Fig 3. (A) Photograph and (B) diagram show a circumcised phal- lus with the hypospadic meatus secondary to the ventral slit (case 6).
acknowledgment). These 3 cases are the only 3 that we are aware of from a review of the English-language literature. This experience would indicate that prompt repair of these complex injuries by an experienced pedi- atric surgeon is essential for a successful outcome. From the report by Bhat et al, 1. it appears that a significant delay accounted in large part for the fatal outcome from sepsis. This report hopefully will encourage others to report similar cases so we may better manage these devastating injuries and provide guidelines for the pre- vention of such iatrogenic trauma.
The majority of our cases involved circumcision- related trauma. Despite the heated debate over, as well as strong opinion about, nonritual circumcision, 9 13 this pro- cedure, which is probably the oldest known surgical
operation, m will continue to be performed by many different specialties. As pediatric surgeons, we will con- tinue to see the complications that arise, and it is there- fore important to be aware of the possible injuries as well as options with regard to their management.
There are many isolated case reports of circumcision- related injuries. Most of these involve the various clamps that are available. The true incidence of these injuries is probably higher because relatively minor injuries may not be reported. The nature of the injury usually is either a degloving i n j u r y 19 as in our first 2 cases (Figs 1 and 2), or, more commonly, some degree of amputation. 2°-24 In the series of degloving injuries by Sotolongo et al, 19 they treat their patients nonoperatively with a satisfactory cosmetic outcome. We would agree with this for the most part, but would also suggest using the excised skin and prepuce if possible as a full-thickness skin graft for immediate coverage. This allowed for fewer painful dressing changes as well as a better cosmetic result in case 2 compared with the patient in case 1 (Fig 2) who was allowed to heal by secondary intention.
Amputation injuries can involve varying amounts of the penis with early reattachment shown to be success- ful. 21,23,24 Sherman et al, 23 in their series of 7 cases, recommend reanastomosis even when there is a delay of surgical repair up to 8 hours. Izzidien 24 reported a case of successful replantation of a traumatically amputated pe- nis in a neonate, without suturing the corpora and no reanastomosis of any vessels. The patients in cases 3 and 4 in our series had partial amputations of the glans only and healed with a flattened appearance. Interestingly, continued hemorrhage from the glans is what drew at- tention to these injuries, and this was readily controlled with topical epinephrine 1:1,000 solution. The patients in cases 5 and 6 had more extensive injuries and required formal hypospadias repair. Case 6 in particular (Fig 3) emphasizes the need for a thorough understanding of prepuce anatomy by primary care physicians who per- form the majority of circumcisions.
Genitourinary injuries in the newborn fortunately are rare. However, because of their iatrogenic etiology as well as the assured continuation of common procedures like circumcision and cesarean section, these complica- tions inevitably will occur. Nonetheless, they are pre- ventable, and ongoing education of our nonsurgical col- leagues is essential. Furthermore, the reporting of these injuries is important so that we can better appreciate the incidence of these injuries as well as provide surgical options for pediatric surgeons and urologists who man- age these injuries.
ACKNOWLEDGMENT
The authors thank Kenneth Kenigsberg, MD, from Garden City, NY for sharing his experience of repairing a grade IV perineal tear with us.

GENITOURINARY INJURIES 239
REFERENCES
1. Ezell WE, Smith EI, McCarthy RP, et al: Mechanical traumatic injury to the genitalia in children. J Urol 102:788-792, 1969
2. Sterioff S Jr, Izant RJ Jr, Persky L: Perineal injuries in children. J Trauma 9:56-61, 1969
3. Pokorny SF: Genital trauma. Clin Obstet Gynecol 40:219-225, 1997
4. Cass AS, Gleich P, Smith C: Male genital injuries from external trauma. Br J Urol 57:467-470, 1985
5. Rivera FP, Brownstein DR: Injury control, in Behrman RE, Kliegman RM, Arvin AM (eds): Nelson Textbook of Pediatrics (ed 15). Philadelphia, PA, Saunders, 1996, pp 226-232
6. Kliegman RM: Birth trauma, in Behrman RE, Kliegman RM, Arvin AM (eds): Nelson Textbook of Pediatrics (ed 15). Philadelphia, PA, Saunders, 1996, pp 465-471
7. Kissoon N, Dreyer J, Walia M: Pediatric trauma: Differences in pathophysiology, injury patterns and treatment compared with adult trauma. Can Med Assoc J 142:27-34, 1990
8. Cyr RM, Usher RH, McLean FH: Changing patterns of birth asphyxia and trauma over 20 years. Am J Obstet Gynecol 148:490-498, 1984
9. Preston EN: Whither the foreskin? A consideration of routine neonatal circumcision. JAMA 213:1853-1858, 1970
10. Nasrallah PF: Circumcision: Pros and cons. Prim Care 12:593- 605, 1985
11. Van Howe RS: Letter to the Editor. J Urol 158:550, 1997 12. Swayze S: Clamping down on circumcision. Nursing 29:73,
1999
13. Baskin LS, Canning DA, Snyder HM, et al: Treating complica- tions of circumcision. Pediatr Emerg Care 12:62-68, 1996
14. Benjamin B, Khan MR: Pattern of external birth trauma in southwestern Saudi Arabia. J Trauma 35:737-741, 1993
15. Snodgrass W: Tubularised, incised plate urethroplasty for distal hypospadias. J Urol 151:464-465, 1994
16. Lickstein DA, Moriarty KP, Feins NR: Neonatal rectovaginal tear during cesarean section. J Pediatr Surg 33:1315-1316, 1998
17. Birth trauma in vaginal breech delivery (editorial). Br Med J 1:320-321, 1978
18. Bhat BV, Jagdish S, Pandey KK, et al: Intrauterine perineal tear: A rare birth injury. J Pediatr Surg 27:1614-1615, 1992
19. Sotolongo JR Jr, Hoffman S, Gribetz ME: Penile denudation injuries after circumcision. J Urol 133:102-103, 1985
20. Neulander E, Walfisch S, Kaneti J: Amputation of distal penile glans during neonatal ritual circumcision--A rare complication. Br J Urol 77:924-925, 1996
21. Gluckman GR, Stoller ML, Jacobs MM, et al: Newborn penile glans amputation during circumcision and successful reattachment. J Urol 153:778-779, 1995
22. Strimling BS: Partial amputation of glans penis during Mogen clamp circumcision. Pediatrics 97:906-907, 1996
23. Sherman J, Borer JG, Horowitz M, et al: Circumcision: Suc- cessful glanular reconstruction following traumatic amputation. J Urol 156:842-844, 1996
24. Izzidien AY: Successful replantation of a traumatically ampu- tated penis in a neonate. J Pediatr Surg 16:202-203, 1981