![Chapter 14 Mendel and the Gene Idea [ Mendelian genetics: The scientific study of heredity and hereditary variation] van Leeuwenhoek (17 th century) de.](https://static.fdocuments.net/doc/165x107/5697bfc01a28abf838ca3a26/chapter-14-mendel-and-the-gene-idea-mendelian-genetics-the-scientific-study.jpg)
Genetics in medicine, genetic counselling, prevention and treatment of hereditary diseases MUDr. S....
63
Genetics in medicine, genetic counselling, prevention and treatment of hereditary diseases MUDr. S. Sytařová Lecture No. 442 Course: Heredity
-
Upload
mariah-dixon -
Category
Documents
-
view
218 -
download
0
Transcript of Genetics in medicine, genetic counselling, prevention and treatment of hereditary diseases MUDr. S....

Genetics in medicine, genetic counselling, prevention and
treatment of hereditary diseases
MUDr. S. Sytařová
Lecture No. 442
Course: Heredity

Genetic counselling

Clinical genetics
- diagnostics, complex care, ev. treatment of patients with hereditary disease
- focus not only on individual patient, but on whole family
- main goal: prevention of genetic diseases

Genetic counselling
= process of communication with whole family focused on problems of occurence or reccurence risk of genetic
disease in family
Tasks: diagnosis, prognosis for patient, risks for other family members, treatment possibilities, prevention

Indicationfor genetic couselling
- known or suspected genetic disease in patient or his family
- occurence of inborn defect or mental retardation
- advanced maternal age (over 35 years)
- atypical results of prenatal screening
- familial occurence or early onset of cancer
- repeated spontaneous abortions, infertility
- exposition of teratogene during pregnancy
- chronic disease in woman planing gravidity
- consanguinity

Genetic counselling
- detailed anamnesis including family and clinical information
- forming pedigree
- indication of genetic diagnostic examination, prenatal dg.
- other possibilities of examination, care and treatment
- examination of other persons in risk in family
- providing sufficient amount of information, careful explanation of problematics, psychology

Nondirective counselling
Geneticist just advices further procedures, patient himself decides for undergoing the examination, ev. alternative method. Patient´s informed agreement is
required for examination of his genetic material.

Hereditary diseases
- monogenic – mendelian heredity
- polygenic – multifactorial
- chromosomal aberrations
- mitochondrial
- cancer diseases – somatic mutations

Methods of diagnosis and prognosis assesment
Genealogic (pedigrees) – monogenic heredity type assesment, correct diagnosis, risk calculation for other family members, presymptomatic diagnosis, possibilities of treatment and prevention
Population (epidemiologic) – empiric risks of polygenic diseases, disease frekvencies in population, sex ratio of affected, age of disease onset, frekvency of heterozygots
Dysmorphologic examination – isolated inborn defect or multiple defects

Examination
Cytogenetical – karyotype, chromosomal aberrations
Postnatal – chromosomes of peripheral blood lymphocytes
Prenatal – AMC, CVS, fetal blood
Biochemical – assesment of metabolites, concentration of metabolites, hormons, enzyme activities – from blood, urine
Prenatal, postnatal screening
Molecular genetic – detection of mutations, prenatal, postnatal (RFLP, PCR)

Inborn defects
Malformation- morphologic defect resulting from abnormal development ( cleft lip)
Disruption - breakdown or interference with originally normal developmental process by trauma, teratogen … (deformity of extremities caused by thalidomide)
Deformation - abnormal form, shape, position caused by mechanical forces (compression of fetus in oligohydramnion)
Dysplasia - abnormal organisation of cells into tissues (achondroplasia)

Cause of inborn defects
Malformation, dysplasia – monogenic, chromosomal and multifactorial
Disruption – sporadic, environmental factor

Multiple anomalies
Sequence = multiple anomalies derived from single anomaly
(e.g. Potter sequence = renal agenesis → oligohydramnion → fetol compression → flattened face, abnormality of extremities,
pulmonary hypoplasia)
Syndrome = multiple anomalies independent, pathogenically related
(e.g. phenylketonuria)

Potter sequence
Teratogenesis
= disturbances in prenatal development leading to origin of
inborn defects

TeratogenesisEmbryotoxic effect
death
malformation
growth retardation
disorder in function
Sensitivity to teratogenes:
genotype of mother + embryo
type of teratogene and dose
permeability through placenta (do 800-1000 daltons)
period of impact

Teratogenes:
Physical
Chemical
Biological
Maternal factors

Physical: Diagnostic irradiation RTG untill 10th day after conception with more than
100mSV – letal effectLater more than 100mSv – PMR, inborn defectsBelly examination Outside uterus less than 20mSv – no effectMore than 20 mSV – consultation with radiologistMore than 100 mSV- reason for ending gravidity, risk of
inborn defects more than 50% Examination with radioisotops I 121
SA, IUGR, defects of CNS and eyes

SONO, MRI – safe methodsCT – not recomanded
Hypertermia (first six weeks of gravidity)Hot bath, sauna – 3x higher risk of inborn defectsFever >38.5oC > 1 daySA, IUGR, defects of CNS, MR, facial dysmorphia hypotonia, hypertonia, NTD
Mechanical causes:Uterus myomatosusAmnional bands

Food, medicines, drugs
A not likely (clinical studies negative)
B less likely
(no risk in animals, not known in people)
(risk in animals, not proved in people)
C (risk in animals or not known, not known in people)
D proved risk, reconsider indication
X contraindication
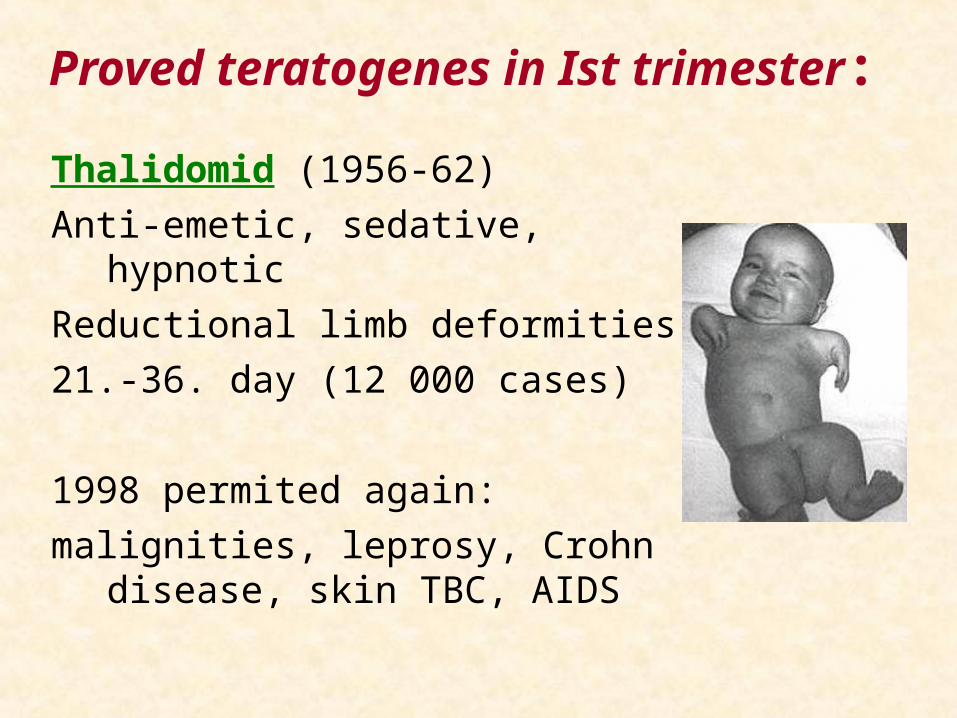
Proved teratogenes in Ist trimester:
Thalidomid (1956-62)
Anti-emetic, sedative, hypnotic
Reductional limb deformities
21.-36. day (12 000 cases)
1998 permited again:
malignities, leprosy, Crohn disease, skin TBC, AIDS

A vitamine and its analogs:
defects of CNS, craniofacial structures, auditory apparate, hearth, limbs

Warfarinbone deformities, chondrodysplasia punctata,CNS defects
Diethylstilbestrol
Years 1938-70., prevention of SA
Risk of breast ca 40% higher in users
Daughters: ca of vagina and cervix uteri, reduced fertility, 2-3x higher risk of premature climacterium
Sons: infertility and genital defects
Cytostatics - (fluoruracil, methotrexate, cyclophosphamide): cardiopathia, osteopathia, spina bifida and other defects

Other risky medicaments

Anticonvulsives:
Fetal hydantoine syndrome mental retardation hypoplasia of middle face cleft face defects limb defects

Fetal valproate syndrom
craniofacial anomalies
cleft face defects
disturbanes in neural tube development
inborn hearth defects

ACE inhibitors:I. trimester: risk of inborn hearth defects 3,7x higher,
other defects 2,7x higherII. and III. trimester: hypotension, reduced renal flow,
oligouria,renal dysgenesis, oligohydramnion, pulmonal hypolasia, craniofacial deformation, IUGR
Wet-nursing – caution in first weeks especially with premature babies - hypotension
Antagonists of angiotensinu II (sartans) – not recomanded
salicylates: higher risk of bleeding and SA (breaks effect of prostaglandines), elongation of gravidity, hearth defects, NTD, limb defects

Tetracycline ( after 20th week):
distubance in development of bones and teeth

Drugs:Caffeine:> 4 cups a day –
Lower birth weight
Premature childbirth
Cigarettes:
SA, IUGR
Cocaine:
SA, hearth defects, urogenital defects
LSD: SA, IUGR

Fetal alcohol syndrome:
Alcohol: 3/4 women, 1/3 till 3rd month of gravidity, 16% even later
Slower metabolism!
Lower birth weight
Fusion of gyri, MR ( IQ 50 – 80 )
Short eyelids, epicantus, microphtalmia
Wide nose root
Long philtrum
Narrow upper lip
Hearth defects
(dose lower than 28g – low risk)

Fetal alcohol syndrome:

Biologic:
1. viruses:
Varicela zoster:
microcephalia, MR, cataracta, chorioretinitis,
Reduction limb deformities, muscular atrofphy
Herpes: SP, IUGR, eye defects
Influenza viruses: NTD
Hepatitis viruses: biliar atresia, chronic hepatitis
Coxackie: pancarditis, memingoencefalitis
HIV : imunodeficiency, dysmorphia

RubeollaVaccination!
mikrocephalia, MR, hearth defects, cataracta, deafness

CMV infectionmicrocephalia, deafness, poliomyelitis,
chorioretinitis, hepatosplenomegalia

2. bacteria: Treponema pallidum: IUGR, chorioretinitisbone and teeth deformities

3. protozoa: Toxoplasma gondii:
hydrocephalus, microcephalus,
chorioretinitis, blindness, MR
Plasmodium malarie : IUGR

Maternal factors:
A. Nourishment:Folic acid : NTD ( 0,4-4mg/den )
Calcium, vitamin D : rachitis, hypocalcemia, tetania
Iodine : struma, MR

B. Maternal diseases:
Diabetes mellitus
SA, IUGR, hearth defects(3x), renal and limb defects, sy. of caudal regresion, NTD, holoprosencephalia
Phenylketonuria
SA, IUGR, microcephalia , MR, hearth defects, facial dysmorphia
Hypo(hyper)thyreosis
SA, growth retardation

Prevention of genetic disorders

Prevention
Primary prevention
– prevention of disease origin
Secondary prevention
– prevention of birth of affected child
(Tertiary prevention
– prevention of disease complications)

Primary prevention
= set of arrangements, that shall prevent genetic disease origin or multifactorial inborn defect
Methods:
- family planning, reproduction in optimal age
- restriction of reproduction (anticonception, sterilisation)
- preconceptional care

Preconceptional care
- gynecologic care
- adjustment of healthy state and hormonal dysbalance
- healthy lifestyle
- healthy food with enough vitamines (folic acid)
- protection against teratogenes, mutagenes, infections
= influencing of environmental factors, prevention of multifactorial defects or diseases

Secondary prevention
= prevention of birth of child with serious genetic defect or disease – care for mother during pregnancy
- prenatal screening
- invasive methods
- interruption

Screening in medicine
Screening method = inexpensive, suitably reliable method useful for examination of larger populations
– selection of subpopulations for further diagnostics only (orientational examination)
Goal – early diagnossis of disease with possiible treatment, prevention, ev. influencing of reproductional
behavior

Prenatal screening
Combined screening in I. trimester (11 – 13 week)
- biochemical markers: hCG, PAPP-A
- ultrasound markers: nuchal translucency (NT), nasal bone, omphalocoele, megavesica, abnormalities in ductus venosus flow measure, tricuspidal regurgitation

Nuchal translucency Ultrasound examination done between 11+0 and 13+6 week of gravidity /in first trimester/, thickness of liquid in backhead area of child is measured /NT/.
Healthy child Increased backhead thickness

Prenatal screening
Biochemical screening in II. trimester (16 – 18 week)
„triple test“ - AFP, hCG, uE3
AFP = risk of neural tube defects
AFP, hCG, uE3 = risk of DS

Prenatal screening
Ultrasound screening in II. trimestru (18 – 22 week)
- number of foetuses, vitality, biometry, pregnancy duration, proportionality of foetus, indirect marks of inborn defect (growth retardation, growth dysproportionality, various ultrasound markers, amniotic fluid amount, movement activity), direct identification of inborn defects

Affection risk assesment
Risk according to maternal age, week of pregnancy, biochemical marker values from maternal blood,
ultrasound abnormalities, mother´s weight
→ risk 1:250 (350) - invasive examination

Maternal age and risk of trisomy 21

Invasive prenatal methods
• AMC amniotic fluid cells examination 16 -18 week
• CVS chorionic villi cells examination 10 -12 week
• Fetal blood from umbilical cord after 20 week

Amniocentesis (AMC)
- examination of foetal cells from amniotic fluid
- long-term cultivation (14 days), cells grow in colonies on bottom of special bottle, cytogenetical analysis
- safe, reliable investigation, as a day case
(risk 0,5-1 %)
- early AMC (7 – 12 week) – higher risk (2 – 5 %)
- possibility of detection of most frequent trisomies and gonosomal abnormalities in 3 days

http://www.forumzdravi.cz

Amniotic cells colony

Chorionic villi samples (CVS)
- early method
- biopsy of vilous chorionic tissue (foetal membranes)
- direct method – villi surface cells
indirect method – log-term cultivation of internal villi cells
- risk cca 1%
- cca 2 % ambiquous results (extraembryonal tissue) – necessary to prove with other method (AMC)
Cordocentesis
- umbilical cord punction, foetal blood taking
- short-time cultivation (2 days)
- possibility of examination of other parametres (biochemical, moleculary genetical etc.)
- higher risk (2 – 5 %)
Indication of invasive prenatal examination:
• advanced maternal age ≥ 35let
• abnormal biochemical screening
• abnormality on ultrasound
• parent – carrier of balanced CHA
• psychologic
• molecular diagnostics of disease

Neonatal screening
- examinaton of dry blood drop from child´s heel
- 13 diseases in CZ – mostly metabolic
- goal – early detection of disease and possibility of medical influence of
complications
- e.g. diet in phenylketonuria

Other screening possibilities
Presymptomatic screening- detection of disease before its onset
- e.g. breast cancer, colon cancer in individuals with predisposition
- Huntington´s disease – problematic (no possible treatment, onset after reproduction, psychiatric
problems in tested individuals)

Other screening possibilities
Detectin of individuals in risk
- screening of carriers (AR diseases)
- e.g. thalassemia in Sardinia
- screening of CF heterozygots in CZ?

Treatment of genetic diseases:
- restriction of potentionally toxic enviromental agents - dietary therapy (phenylketonuria, hypercholesterolemia)
- replacement of deficient product (antihemophilic factor, vitamin D)
- induction of enzyme by medicaments (barbiturates in nonhaemolytic icterus)
- transplantation of organs (lungs - CF, hepar – Wilson)
- removal of organs (colon – fam. polyposis coli)
- operation (heart disease)

Thank you for your attention.