Genetics and Paediatric Health: Section 5 - CICH Profile · 2017-10-30 · Genetics and Paediatric...
22
Genetics and Paediatric Health: Section 5 Suggested reference: Rockman-Greenberg, C., Avard, D., Hanvey, L., Marcotte, M., & Fitzpatrick, J. (2014). Genetics and paediatric health: Section 5: Congenital anomalies. In The Health of Canada’s Children and Youth: A CICH Profile. Retrieved from http://profile.cich.ca/en/index.php/chapter2 Contributors: Writing and editing: Denise Avard Jennifer Fitzpatrick Louise Hanvey Cheryl Rockman-Greenberg Project development, research, and review: Expert Advisory Committee Laura Arbour Denise Avard Pascal Borry Pranesh Chakraborty Jennifer Fitzpatrick William Fraser Jan Friedman Louise Hanvey Anne Junker Bartha Maria Knoppers Elaine Orrbine Cheryl Rockman-Greenberg Jacques P. Tremblay Brenda Wilson Durhane Wong-Rieger Other Denise Alcock Jeannine Fraser Aspasia Karalis Meghan Marcotte Kelly McClellan Vaso Rahimzadeh Karine Sénécal Janice Sonnen Robin Walker Graphic design: Shelley Callaghan Louise Hanvey Meghan Marcotte Bert Schopf Website development: Accel Web Marketing
Transcript of Genetics and Paediatric Health: Section 5 - CICH Profile · 2017-10-30 · Genetics and Paediatric...

Genetics and Paediatric Health: Section 5
Suggested reference:
Rockman-Greenberg, C., Avard, D., Hanvey, L., Marcotte, M., & Fitzpatrick, J. (2014). Genetics and paediatric
health: Section 5: Congenital anomalies. In The Health of Canada’s Children and Youth: A CICH Profile. Retrieved
from http://profile.cich.ca/en/index.php/chapter2
Contributors:
Writing and editing: Denise Avard
Jennifer Fitzpatrick
Louise Hanvey
Cheryl Rockman-Greenberg
Project development, research, and review: Expert Advisory Committee Laura Arbour
Denise Avard
Pascal Borry
Pranesh Chakraborty
Jennifer Fitzpatrick
William Fraser
Jan Friedman
Louise Hanvey
Anne Junker
Bartha Maria Knoppers
Elaine Orrbine
Cheryl Rockman-Greenberg
Jacques P. Tremblay
Brenda Wilson
Durhane Wong-Rieger
Other Denise Alcock
Jeannine Fraser
Aspasia Karalis
Meghan Marcotte
Kelly McClellan
Vaso Rahimzadeh
Karine Sénécal
Janice Sonnen
Robin Walker
Graphic design:
Shelley Callaghan
Louise Hanvey
Meghan Marcotte
Bert Schopf
Website development:
Accel Web Marketing

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
Congenital anomalies, sometimes called birth defects, happen during prenatal development. They include abnormalities of structure, function, or metabolism. They are present at birth but may not be diagnosed until later in life. They can result in physical or mental disability, affect a child’s development, and, in severe cases, can be fatal.1
Congenital anomalies are a leading cause of death among foetuses and infants2 and can greatly influence quality of life. They are costly to both families and the healthcare system.3
1 Definition adapted from Health Canada. Congenital Anomalies in Canada — A Perinatal Health Report, 2002. Ottawa: Minister of Public Works and Government Services Canada, 2002.
2 Lowry R, Sibbald B, Bedard T. Alberta Congenital Anomalies Surveillance System Eighth Report 1980–2007. Government of Alberta Report, 1-45. Canadian Perinatal Health Report 2008 Edition (pp. 317). Ottawa: The Public Health Agency of Canada; 2009.
3 Public Health Agency of Canada and the Congenital Anomalies Surveillance Network. Towards Enhanced Congenital Anomalies Surveillance in Canada (pp. 1–14). Ottawa; 2008.
5.1.1 What Are Congential Anomalies?
Image credit: Shutterstock

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
The Canadian Congenital Anomalies Surveillance System (CCASS) gathers and collates data from hospital databases and from some provincial congenital anomalies surveillance systems. However, the collection and recording of information regarding congenital anomalies is not standardized across the country.1 Different provinces test for different conditions, use different sources of data, and assess the presence of congenital anomalies in their populations differently. For example, some include data on fetal anomalies from pregnancies terminated following a prenatal diagnosis, while others do not.1,2
1 Little J, Potter B, Allanson J, Caulfield T, Carroll JC, Wilson B. Canada: Public Health Genomics. Public Health Genomics. 2009;12:112–120.
2 Demographics and Risk Indicators Working Group, C.C.A.S.N., Public Health Agency of Canada. Congenital Anomalies Surveillance in Canada: Results of a 2006–2007 Survey on Availability of Selected Data Variables in Canadian Provinces and Territories. Ottawa: Public Health Agency of Canada, 2010
ImplicationsThe lack of standardization makes it difficult to compare data across provinces and territories. A new initiative to improve the current system by strengthening surveillance at the provincial and territorial level is underway to address the limitations in collection and reporting of data in the future. Congenital anomalies are an important cause of childhood death, chronic illness, and disability. There is a need to develop standardized methods of coding data relating to congenital anomalies, along with better registration and surveillance. Further research about the causes of congenital anomalies is needed.
5.1.2 Monitoring Congenital Anomalies
LegendAdministrative databases, perinatal databases, congenital anomalies surveillance programs
Administrative databases, perinatal databases, fetal anomaly databases
Administrative databases, perinatal databases
Administrative databasesYT
NU
SKAL
NB
PEI
BC
NWT
MN
QC
NS
ON
NL

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
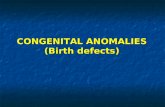
Some congenital anomalies are caused by mutations in a single gene or damage to a specific chromosome. Other congenital anomalies are due to exposure to environmental hazards or drugs during pregnancy. Others result from a combination of genetic and environmental influences. However, the cause of most congenital anomalies is unknown. Most children with congenital anomalies are born to mothers with no family history and no known risk factors.
Fig. 5.1.3 Causes of Congenital Anomalies, 1993
Graphic created by CICH using data from Health Canada. Congenital Anomalies in Canada — A Perinatal Health Report,2002. Ottawa: Minister of Public Works and Government Services Canada, 2002.
Chromosome and
single gene causes
Recognized genetic conditions:
Multifactorialinheritance*
15% to 25% are
due to recognized
genetic conditions
20% to 25% are due
to multifactorial
inheritance
Unexplained causes
40% to 60% are due
to unexplained
causes
Environmental factors:Maternal-related
conditions, drug or
chemical exposures
8% to 12% are due
to environmental
factors
75-85%
15-25%
8-12%
88-92%
75-80%
20-25% 40-60% 40-60%
* A congenital anomaly is considered to be multifactorial (or polygenic) in origin when there is a combined influence of (a number of)genes and environmental factors that interfere with normal embryologic development. Multifactorial inheritance is considered when thereappears to be a genetic component but there is no clear Mendelian pattern of inheritance. Multifactorial inheritance is the underlyingetiology of most of the common congenital anomalies.
5.1.3 Causes of Congenital Anomalies

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
In 2007, 4.1% of all births in Canada, including stillbirths, were affected by one or more congenital anomalies. It is estimated that major congenital anomalies affect an estimated 3% of all births.1 It is also estimated that this rate increases to 7% by the second year of life.2
Children can be born with multiple congenital anomalies that can range from mild to severe to life threatening. Infants born with severe anomalies (e.g., anencephaly, trisomy 13, trisomy 18, or inoperable congenital heart defects) often die. Not all congenital anomalies are serious, and many can be corrected with treatment.
1 Demographics and Risk Indicators Working Group, C.C.A.S.N., Public Health Agency of Canada. Congenital Anomalies Surveillance in Canada: Results of a 2006–2007 Survey on Availability of Selected Data Variables in Canadian Provinces and Territories. Ottawa: Public Health Agency of Canada; 2010.
2 Health Canada. Congenital Anomalies in Canada — A Perinatal Health Report, 2002. Ottawa: Minister of Public Works and Government Services Canada; 2002
5.1.4 Prevalence of Congenital Anomalies in Canada
Graphic created using a Shutterstock images and data from Health Canada. Congenital Anomalies in Canada — A Perinatal Health Report, 2002. Ottawa: Minister of Public Works and Government Services Canada, 2002.

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
Overall it appears that both the number of babies born with congenital anomalies and the rate per 10,000 total births decreased between 1998 and 2009 in Canada. The rate has decreased from 451.2 per 10,000 total births to 385.2, a decline of approximately 15%. This could be partially due to the decline in some of the common congenital anomalies, such as neural tube defects [view report], but also to inconsistencies in data collection.
It should be noted, however, that some congenital anomalies, such as gastroschisis (where the intestines are outside of the body wall), are increasing in frequency. The precise cause of this is uncertain.1 The decrease in rates among live births has been noteworthy, leading to birth prevalence below 400 per 10,000 in 2009. On the other hand, the rates of congenital anomalies in stillbirths has increased slightly, primarily because of an increase in the rate among stillbirths of very low birth weight (less than 750 g).2
1 CAPSNet 2012 Annual Report. The Canadian Pediatric Surgery Network. Version 1. February 2013. http://www.capsnetwork.org/portal/Portals/0/CAPSNet/Annual%20 Reports/CAPSNet%20AR%202012%20-%20FINAL_Feb%202013.pdf.
2 Public Health Agency of Canada. Congenital Anomalies in Canada 2013: A Perinatal Health Surveillance Report. Ottawa: Public Health Agency of Canada; 2013
Fig. 5.1.5 Birth Prevalence of Congenital Anomalies, by Year, Canada
(Excluding Quebec*), 1998 to 2009
Year
*Quebec was excluded because data were not available for all years.
Graphic adapted by CICH from Table B1.1 in ‘Congenital Anomalies in Canada 2013: A Perinatal HealthSurveillance Report’. Ottawa: Public Health Agency of Canada; 2013.
Rate per10,000
total births
0
50
100
150
200
250
300
350
400
450
500
Number
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Number
Rate per 10,000 total births
5.1.5 Birth Prevalence of Congenital Anomalies, by year, Canada (Excluding Quebec*), 1998 to 2009

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
Congenital anomalies are the second leading cause of fetal death. Between 2000 and 2008, the rate of fetal death due to congenital anomalies showed little change, varying between 4 and 5 per 10,000 total births.
Year
Fig. 5.2.1 Rate of Fetal Death 500 Grams by Cause, Canada(Excluding Ontario*), 2000 to 2008
Graphic created by CICH using data from: Public Health Agency of Canada. Perinatal Health Indicators forCanada 2011. Ottawa, 2012.
0
2
4
6
8
10
12
14
16
18
2000 2001 2002 2003 2004 2005 2006 2007 2008
Fetal deathsper 10,000total births
Congenital Anomalies Maternal Complications
Placenta/Cord/Membrane Intrauterine Hypoxia/Asphyxia
*Ontario was excluded because of data quality concerns.
5.2.1 Rate of Fetal Death ≥ 500 Grams by Cause, Canada (Excluding Ontario*), 2000 to 2008

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
Congenital anomalies are a leading cause of infant mortality. They are the leading cause of death in the period from 28 days to one year of age (postneonatal period). They are the second leading cause of death during the first 27 days of life (neonatal period).1
1 Public Health Agency of Canada. Perinatal Health Indicators for Canada 2011. Ottawa: Public Health Agency of Canada; 2012
Fig. 5.2.2 Causes of Neonatal, Postneonatal, and All Infant Death,
Canada (Excluding Ontario*), 2003 to 2007
Graphic created by CICH using data from the Perinatal Health Indicators for Canada 2011. Ottawa: Public Health Agencyof Canada; 2012.
All InfantDeaths
PostneonatalDeaths
NeonatalDeaths
23
11
306
6
4
1 19
Congenital anomalies
Asphyxia
Immaturity
Infection
Sudden infant death syndrome (SIDS)
Other
Other sudden or unexplained infant death
External causes
23
1
8
1421
10
4
19
23
14
39
3
11
0
19
*Ontario was excluded because of data quality concerns.
5.2.2 Causes of Neonatal, Postneonatal, and All Infant Death, Canada (Excluding Ontario*), 2003 to 2007

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
Although congenital anomalies are one of the leading causes of infant death in Canada, the rate is decreasing.1 The Public Health Agency of Canada stated that the decreasing rate of infant deaths is most likely a result of increasing prenatal diagnosis and termination of pregnancies when congenital anomalies are diagnosed.2
1 Public Health Agency of Canada. Perinatal Health Indicators for Canada 2011. Ottawa: Public Health Agency of Canada; 2012.2 Public Health Agency of Canada and the Congenital Anomalies Surveillance Network, 2008
ImplicationsIt is important to monitor congenital anomalies for possible associations with environmental factors, as the human genome responds to the environment in a very dynamic fashion.3 In an effort to facilitate health service planning, methods for collecting information regarding congenital anomalies in Canada could be improved for more accessible and reliable data.3 Health Canada. Congenital Anomalies in Canada — A Perinatal Health Report, 2002. Ottawa: Minister of Public Works and Government Services Canada; 2002
Fig. 5.2.3 Causes of Infant Death, Canada (Excluding Ontario*),
1999, 2004, and 2007
Graphic created by CICH with data from the Public Health Agency of Canada and the Congenital AnomaliesSurveillance Network, 2008 (1999 data), and from the Public Health Agency of Canada, Perinatal Health Indicatorsfor Canada 2011. Ottawa, 2012. (data for 2003 to 2007)
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
Congenitalanomalies
Asphyxia Immaturity Infection Sudden infantdeath
syndrome(SIDS)
Otherunexplainedinfant death
Externalcauses
Other
Rate per1,000 live
births
1999 2004 2007
*Ontario was excluded because of data quality concerns.
5.2.3 Causes of Infant Death, Canada (Excluding Ontario*), 1999, 2004, and 2007

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
There are many congenital anomalies. The module contains some more detailed information on three of the most common congenital anomalies: Down syndrome, neural tube defects, and congenital heart defects.
5.3.1 Three Common Congenital Anomalies

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
Most children with Down syndrome have an extra copy of the 21st chromosome, meaning that instead of two of these chromosomes, they have three, which is referred to as Trisomy 21. About 95% of people with Down syndrome have Trisomy 21. People with Down syndrome have wide variations in mental abilities, behaviour, and development, and their symptoms can range from mild to severe.1
While the chance of having an infant with Down syndrome increases with maternal age, a baby with Down syndrome can be born to women of any age. It is estimated 80% of children with Down syndrome are born to women younger than 35 years of age.1
1 Your Child with Down Syndrome. Canadian Down Syndrome Society. http://www.cdss.ca/images/pdf/brochures/english/your_child_with_down_syndrome_english.pdf
5.3.2 Common Congenital Anomalies - Down Syndrome
Image credit: Shutterstock

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
There has been no clear trend in the rates of Down syndrome since 1996. In 2007, the rate was 13.0 per 10,000 total births, or approximately 483 babies born with Down syndrome.
Fig. 5.3.3 Common Congenital Anomalies – Rates of Down Syndrome,
Canada, 1996 to 2007
Graphic created by CICH with data from the ‘Perinatal Health Indicators for Canada 2011'. Ottawa: Public HealthAgency of Canada; 2012
Rate per10,000
total births
Number
Year
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
0
100
200
300
400
500
600
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Number
Rate per 10,000 total births
5.3.3 Common Congenital Anomalies - Rates of Down Syndrome, Canada, 1996 to 2007

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
When looking at the combined rate of Down syndrome for the years 1998–2007, it is clear that the rate varied greatly between provinces and territories. The rates of Down syndrome ranged from 11.2 per 10,000 total births in Quebec to 24.2 in the Northwest Territories.
These differences may be due to a number of factors, such as differences in maternal age, the availability and use of prenatal screening and diagnosis, and the rate of pregnancy termination.
Fig. 5.3.4 Common Congenital Anomalies – Rate of Down Syndrome
per 10,000 Births, Canada, (Excluding Yukon ), 1998 to 2007†
Province/Territory
Graphic created by CICH using data from ‘Perinatal Health Indicators for Canada 2011'. Ottawa: Public HealthAgency of Canada; 2012.
15.9 17.019.1
14.611.2
14.2 14.7 15.1 13.4
17.6
24.221.5
0
5
10
15
20
25
30
35
40
45
NT NU
Rate per10,000
total birthsand 95%
confidenceintervals*
NL PE NS NB QC ON MB SK AB BC
* A confidence interval is “an interval of values bounded by confidence limits within which the true value of a population parameter is
stated to lie with a specified probability”. (http://dictionary.reference.com/browse/confidence%20interval) In this case, we can be 95%
confident that the provincial rates of Down syndrome per 10,000 total births is within the interval shown with the black lines.
†The rate from Yukon is not shown due to small numbers.
CanadianRate 14.1
5.3.4 Common Congenital Anomalies - Rate of Down Syndrome per 10,000 Births, Canada, (Excluding Yukon†), 1998 to 2007

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
Neural tube defects are a group of congenital abnormalities of the central nervous system that result when the bony structure that encloses the spinal cord (the vertebra) does not close completely. The causes of neural tube defects are multifactorial and are influenced by geography, ethnicity, genetics, and nutrition.
Fig. 5.3.5 Common Congenital Anomalies – Neural Tube Defects
Examples:• Anencephaly• Encephalocele• Spinal Bifida - the most
common type
Examples:• Lipomyelomeningocele• Lipomeningocele• Tethered Cord
Graphic created by CICH using information from http://www.chg.duke.edu/diseases/ntd.html
Open Neural Tube Defects Closed Neural Tube Defects
5.3.5 Common Congenital Anomalies - Neural Tube Defects

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
In 1999, in Canada, six babies were born with neural tube defects per 10,000 total births, a decline from 11.1 per 10,000 births in 1989. Between 1995 and 2007, the rate of neural tube defects in Canada decreased by about half, to 4.1 from 9.2 per 10,000 total births. Most of the decline occurred between 1995 and 2004, and there has not been a clear trend in rates since. Despite this, much of the decline is attributed to policy-making and education initiatives surrounding the role of folic acid in preventing babies from developing neural tube defects.
Fig. 5.3.6 Common Congenital Anomalies – Rate of Neural Tube Defects,Canada, 1995 to 2007*
Graphic created by CICH using data from: Perinatal Health Indicators for Canada 2011. Years 1998 to 2007.Ottawa: Public Health Agency of Canada; 2012 and Canadian Perinatal Health Report, 2008 Edition. Years 1995to 1997. Ottawa: Public Health Agency of Canada; 2008.
*Nova Scotia data were not available before 1996.
Number
0
1
2
3
4
5
6
7
8
9
10
0
50
100
150
200
250
300
350
400
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Year
Rate per10,000
total births
Number of cases
Cases per 10,000 total births
5.3.6 Common Congenital Anomalies - Rate of Neural Tube Defects, Canada, 1995 to 2007*

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
There are variations in the rates of neural tube defects across Canada, ranging from 3.8 per 10,000 total births in Quebec to 6.5 in Nova Scotia.
Fig. 5.3.7 Common Congenital Anomalies –
Rate of Neural Tube Defects, Canada*, 1998 to 2007
Graphic created by CICH using data from: Perinatal Health Indicators for Canada 2011. Ottawa: Public HealthAgency of Canada; 2012.
*The rates for Prince Edward Island, Yukon, Northwest Territories, and Nunavut are not released due to small numbers.
Province
Rate per10,000
total births
5.6
6.5
4.03.8
4.4
5.8
4.84.2
6.3
0
1
2
3
4
5
6
7
8
9
NL NS NB QC ON MB SK AB BC
CanadianRate 4.6
5.3.7 Common Congenital Anomalies - Rate of Neural Tube Defects, Canada*, 1998 to 2007

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
Research shows that women can reduce their risks of having a baby with a neural tube defect by taking folic acid, or folate, which is a B vitamin. Folic acid is essential for the development of the baby’s brain and spine. Studies have shown that women who take enough folic acid supplements and eat a healthy diet before they become pregnant and during the early part of their pregnancy are less likely to have a baby with a neural tube defect.1
In 1998, the Canadian government required that white flour, enriched pasta, and cornmeal be fortified with folic acid.2 The Public Health Agency of Canada and Health Canada recommended that all women who could become pregnant take a supplement containing 0.4mg of folic acid and suggested a higher dose for women who are at increased risk of having a baby with a neural tube defect.3
1 Lumley J, Watson L, Watson M, Bower C. Periconceptional supplementation with folate and/or multivitamins for preventing neural tube defects. Cochrane Database Syst Rev. 2001;3.
2 Millar W. Folic Acid Supplementation. Statistics Canada, Health Reports (Catalogue 82-003-XIE0). Ottawa: Statistics Canada; 2004;15(3):49–52.
3 Van Allen MI, McCourt C, Lee NS. Preconception health: folic acid for the primary prevention of neural tube defects. A resource document for health professionals, 2002. Ottawa: Minister of Public Works and Government Services Canada; 2002. Catalogue No.: H39-607/2002E
5.3.8 Common Congenital Anomalies – Neural Tube Defects – Primary Prevention Policies
Image credit: Shutterstock

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
According to the 2009–2010 Canadian Community Health Survey, nearly 60% of women aged 20 to 49 years reported taking folic acid before their last pregnancy. However, access to folic acid and prevention of neural tube defects is not equal for all women. Women aged 30 to 49 years were more likely to take folic acid than were younger women. Two-thirds of women with a post-secondary education took the supplements compared to one-third of those without a high school diploma. Moreover, 84% of women in the highest income households took folic acid compared with only 43% of women in the poorest households.
Fig. 5.3.9 Common Congenital Anomalies – Folic Acid Use
Before Pregnancy, Canada, 2009–2010
Graphic created by CICH using adapted data from the Canadian Community Health Survey PUMF, 2009–2010.
20 to 24 years 33.50%
25 to 29 years 53.20%
30 to 49 years 65.80%
Less than secondary school graduation 33.70%
Secondary school graduation 44.70%
Some post-secondary 50.00%
Post-secondary graduation 67.20%
Quintile 1 43.30%
Quintile 2 52.00%
Quintile 3 65.10%
Quintile 4 71.70%
Quintile 5 84.20%
Women Aged 20 to 49 Who Took Folic Acid
Before Their Last Pregnancy, Canada, 2009-2010 Total: 59.8%
Age
Education
Household Income
5.3.9 Common Congenital Anomalies - Folic Acid Use Before Pregnancy, Canada, 2009–2010

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
There are also differences among the provinces and territories with regards to the proportion of women taking folic acid prior to pregnancy. Approximately 49% did so in the territories compared with 68% in British Columbia.
Graphic created by CICH using adapted data from the Canadian Community Health Survey PUMF, 2009–2010.
Fig. 5.3.10 Common Congenital Anomalies – Women Aged 20 to 49 Years
Who Took Folic Acid Before their Last Pregnancy Canada, 2009–2010
Provinces/Territories
Territories
%
0 10 20 30 40 50 60 70 80 90 100
NL
PE
NS
NB
QC
ON
MB
SK
AB
BC
60.6
54.4
56.3
43
56.7
61.6
53.2
57.3
57.3
68.3
48.5
Canada59.8%
5.3.10 Common Congenital Anomalies – Women Aged 20 to 49 Years Who Took Folic Acid Before their Last Pregnancy, Canada, 2009–2010

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
According to the Canadian Maternity Experiences Survey, more than three-quarters of women in the survey knew before their pregnancy that folic acid could help prevent some birth defects. Women who knew that this was the case were more likely to take folic acid before and during their pregnancy.1
1 Public Health Agency of Canada. What Mothers Say: The Canadian Maternity Experiences Survey. Ottawa: Public Health Agency of Canada; 2009
Graphic created by CICH using data from: What Mothers Say: The Canadian Maternity Experiences Survey. Ottawa: Public Health Agencyof Canada; 2009.
Fig. 5.3.11 Common Congenital Anomalies – Women Who Took
Folic Acid by Pre-pregnancy Knowledge, Canada*, 2006–2007
* 6,421 birth mothers 15 years of age and older who had a single live born baby during the three-month period preceding the 2006
Canadian Census of Population and lived with their baby. The rates for Prince Edward Island, Yukon, Northwest Territories, and Nunavut
are not released due to small numbers.
Before pregnancy
During pregnancy
%
68.8
17.8
92.5
77.0
0
20
40
60
80
100
Knew that folic acid could help
prevent some birth defects
Did not know that folic acid could help
prevent some birth defects
5.3.11 Common Congenital Anomalies – Women Who Took Folic Acid by Pre-Pregnancy Knowledge, Canada*, 2006–2007

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
Congenital heart defects – where the heart or the blood vessels near the heart do not develop normally before birth – are the most common congenital anomalies. In Canada, 1 in 100 to 150 babies are born with a congenital heart defect.1 There has been progress in the early diagnosis and surgical treatment of congenital heart defects that has resulted in a decrease in death and illness. Sixty years ago, less than 20% of infants born with complex heart defects lived to adulthood. Today, more than 90% live to adulthood due largely to surgical procedures, the development of regional cardiac surgical centres, and improved medical care.2 Despite this progress, congenital heart defects remain the leading cause of childhood death among congenital anomalies in Canada. Children who suffer from the most serious heart defects require complex medical care and can have a greatly compromised quality of life.1
In most situations, the cause of congenital heart defects is unknown. Although many congenital heart defects can be genetic, viral infections such as rubella (measles) or drug and/or alcohol use during pregnancy are known to increase risks. Thus, the causes are multifactorial. Babies born with congenital anomalies often have other congenital or chromosomal anomalies, such as Down syndrome, trisomy 13 or 18, or Turner syndrome.2
1 Health Canada. Congenital Anomalies in Canada — A Perinatal Health Report, 2002. Ottawa: Minister of Public Works and Government Services Canada; 2002.2 Congenital Heart Defects. Heart and Stroke Foundation of Canada http://www.heartandstroke.com/site/c.ikIQLcMWJtE/b.3484063/
5.3.12 Common Congenital Anomalies – Congenital Heart Defects
Image credit: Shutterstock

The Health of Canada’s Children and Youth A CICH Profile
This page is only one section of the CICH Profile, for more interesting data on children and youth visit http://profile.cich.ca/ © 2014 Canadian Institute of Child Health
The Health of Canada’s Children and Youth: A CICH ProfileGenetics and Paediatric Health
Section 5 - Congenital Anomalies
Both the number and the rate of congenital heart defects (determined up to 30 days of age) have decreased. In 1998, the rate was 107.1 per 10,000 total births. By 2009, that rate had decreased by 21% to 85.1 per 10,000 total births.
Fig. 5.3.13 Common Congenital Anomalies – Rate of
Congenital Heart Defects, Canada (Excluding Quebec*), 1998–2009
Graphic created by CICH using data from Table B4.1 in ‘Congenital Anomalies in Canada 2013: A PerinatalHealth Surveillance Report’. Ottawa: Public Health Agency of Canada; 2013.
*Quebec was excluded because data were not available for all years.
NumberRate per10,000
total births
Year
0
20
40
60
80
100
120
0
500
1000
1500
2000
2500
3000
3500
1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Number of cases
Cases per 10,000 total births
5.3.13 Common Congenital Anomalies – Rate of Congenital Heart Defects, Canada (Excluding Quebec*), 1998–2009