GENERAL PRACTITIONERS AND THE HOSPITAL SERVICE
2
1038 showed striking improvement by this time, with complete sub- sidence of the oedema, and treatment was then changed to oral fucidin, 2g. daily. No adverse effects were observed from the use of intravenous fucidin; it is of interest that the preparation was well tolerated both in a young girl and in an old woman. Certainly in the 2nd patient, whose condition was virtually moribund, intravenous fucidin appeared to be life-saving. Wombourn, Wolverhampton, Staffs. J. A. O’GARRA. J. A. O’GARRA. HYPOGLYCÆMIA IN PANCREATITIS SIR,-We are interested in the preliminary communication of Dr. Sutton and Dr. Taghizadeh (Sept. 28, p. 712), for there seems to be some relation between their findings and our studies in patients with pancretitis. 8 patients with chronic calcific pancreatitis, due to alcohol, were given an intravenous injection of crystalline insulin (0-1 unit per kg. body-weight) after an overnight fast. 7 had diabetic glucose-tolerance tests (almost all with normal fasting blood-sugar levels) but none of the patients had previously received insulin therapy. A matched group of healthy non- obese controls, without family history of diabetes, was simit larly investigated. As the accompanying figure indicates, pancreatitis subjects responded with a slightly delayed but significantly prolonged (P < 0-05 at 45, 60, and 90 minutes) fall in plasma-glucose com- Mean % plasma-glucose fall, from fasting, in 8 patients with chronic pancreatitis and health controls after intravenous administration of insulin (0’1 unit per kg. body-weight). pared with the control group. In addition the pancreatitis patients invariably showed clinical evidence of hypoglycmmia during the latter stages of the test. The prolonged hypoglycsemia in the pancreatitis group is unlikely to have been primarily due to defective compensatory glycogenolysis, since most of the patients were previously found to have entirely normal liver function and histology. Delay in degradation of the injected insulin is a possible explanation but, like Dr. Sutton and Dr. Taghizadeh, we feel that pancreatic glucagon insufficiency may have been important. It is temp- ting to postulate that these patients, already deficient in insulin reserve,! are similarly lacking in stores of pancreatic glucagon with which to help maintain glucose homoeostasis. Recently established techniques of plasma-glucagon immunoassay,2 3 may well provide the answer. An important clinical application of these findings is to emphasise the need for caution in administering insulin to sub- jects with " pancreatic diabetes " if serious hypoglycaemia is to be avoided. This complication has previously been found to be an important cause of death in such patients.4 B. I. JOFFE S. BANK I. N. MARKS. Endocrine Research and Gastrointestinal Units, Department of Medicine, University of Cape Town, South Africa. 1. Joffe, B. I., Bank, S., Jackson, W. P. U., Keller, P., O’Reilly, I. G., Vinik, A. I. Lancet, Oct. 26, 1968, p. 890. 2. Hazzard, W. R., Crockford, P. M., Buchanan, K. D., Vance, J. E., Chen, R., Williams, R. H. Diabetes, 1968, 17, 179. 3. Eisentraut, A., Ohneda, A., Parada, E., Unger, R. H., ibid. p. 321. 4. Bank, S. S. Afr. med. J. 1966, 40, 342. GENERAL PRACTITIONERS AND THE HOSPITAL SERVICE SIR,-The joint working-party on Medical Staffing in the Hospital Service stated 1 that, without the help of 3628 foreign graduates, there would be a breakdown in the hospital service below the grade of senior registrar. Whether it is good or bad that the medical staffing of the hospital service depends, as it does, on those 3628 foreign graduates is not the question I wish to ask. According to the census of junior hospital staff carried out by the Health Departments on March 31, 1960, the numerical needs of the hospital service below the grade of senior registrar were 3587 registrar posts (some vacant), 2877 senior-house-officer posts (some vacant), and 3023 house- officer posts (registered and preregistration), a total of 9487 posts.2 A current survey made by the Birmingham Regional Hospital Board shows that 89% of the general practitioners questioned wished to work in a hospital in addition to working as a general practitioner.3 The question I now wish to ask is whether there are enough general practitioners in Great Britain to do the work now undertaken in the hospitals by registrars, senior house-officers, and house-officers, if the general practitioners were integrated into the medical staffing structure of the hospitals. On Sept. 30, 1967 there were, in England and Wales, 19,549 principals in general practice and 758 assistants,4 a total of 20,307. On the same date there were in England and Wales 4516 registrars and 2781 senior-house-officers, a total between those two grades of 7297 postS.4 To reduce the demand which the hospitals would make on the general practitioners, I am going to exclude the work now done by the house-officers, who on March 31, 1960, numbered 3023.2 Furthermore, I will confine the calculations to England and Wales, since up-to-date figures of the hospital staffs in Scotland are not available. In England and Wales, therefore, if on Sept. 30, 1967, the general practitioners had taken over the work of 4516 registrars and 2781 senior-house-officers, they would have had to provide 65,673 sessions (at 9 sessions a week) each week-taking each session as 3112 hours, the hospitals would have required 229,8551/2 hours per week. If only the principals took part in the hospital work, each would have had to give up 11 -8 hours to the hospital (229,855 -7-19,549); if the 758 assistants were included the figure would fall to 11.3 hours a week (229,855=20,307). Whether a general practi- tioner could afford between 11 and 12 hours a week in this way is unknown; but the Birmingham survey found fhat those general practitioners who did work in hospitals provided 7-8 hours a week.3 It will be remembered that 89% of the general practitioners questioned wished to do hospital work. 89% of 19,549 principals would be 17,403 general practitioners. Notionally, it would need about another 8000-12,000 more principals in England and Wales to take over the work of the existing registrars and senior-house-officers if each general practitioner can provide the hospitals with only 7-8 hours of his time per week. The Birmingham survey, however, sug- gests that the integration of general practitioners into the hospital service would not make the present registrars and senior-house-officers unnecessary. There are, at present, 27 specialties in the hospital service. Most general practitioners are interested only in general medicine, obstetrics and gynxcology, and paediatrics, and a few in geriatrics, surgery, and dermatology.3 It seems therefore that general practitioners would be willing to take over duties only in about 6 out of the 27 existing hospital specialties. The combined total of registrar and senior-house-officer posts in general medicine, obstetrics and gynaecology, and paediatrics add up to only 2477 posts out of a total of 7297. This raises the question of which doctors are going to fill the 4820 (7297-2477) hospital posts the general practitioners do not want. Nevertheless, it 1. Medical Staffing Structure in the Hospital Service: Report of the Joint Working Party; para. 96, p. 32. H.M. Stationery Office, 1961. 2. ibid. appendix 4, paras 5 and 6, p. 75. 3. Report of a Sub-Committee of the General Practice Liaison Committee of the Birmingham Regional Hospital Board, 1968. 4. See Lancet, Aug. 24, 1968, p. 448.
Transcript of GENERAL PRACTITIONERS AND THE HOSPITAL SERVICE

1038
showed striking improvement by this time, with complete sub-sidence of the oedema, and treatment was then changed to oralfucidin, 2g. daily.No adverse effects were observed from the use of intravenous
fucidin; it is of interest that the preparation was well toleratedboth in a young girl and in an old woman. Certainly in the 2ndpatient, whose condition was virtually moribund, intravenousfucidin appeared to be life-saving.
Wombourn,Wolverhampton, Staffs. J. A. O’GARRA.J. A. O’GARRA.
HYPOGLYCÆMIA IN PANCREATITIS
SIR,-We are interested in the preliminary communicationof Dr. Sutton and Dr. Taghizadeh (Sept. 28, p. 712), for thereseems to be some relation between their findings and our studiesin patients with pancretitis.
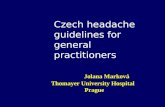
8 patients with chronic calcific pancreatitis, due to alcohol,were given an intravenous injection of crystalline insulin (0-1unit per kg. body-weight) after an overnight fast. 7 haddiabetic glucose-tolerance tests (almost all with normal fastingblood-sugar levels) but none of the patients had previouslyreceived insulin therapy. A matched group of healthy non-obese controls, without family history of diabetes, was simitlarly investigated.As the accompanying figure indicates, pancreatitis subjects
responded with a slightly delayed but significantly prolonged(P < 0-05 at 45, 60, and 90 minutes) fall in plasma-glucose com-
Mean % plasma-glucose fall, from fasting, in 8 patients with chronicpancreatitis and health controls after intravenous administrationof insulin (0’1 unit per kg. body-weight).
pared with the control group. In addition the pancreatitispatients invariably showed clinical evidence of hypoglycmmiaduring the latter stages of the test.The prolonged hypoglycsemia in the pancreatitis group is
unlikely to have been primarily due to defective compensatoryglycogenolysis, since most of the patients were previously foundto have entirely normal liver function and histology. Delay indegradation of the injected insulin is a possible explanation but,like Dr. Sutton and Dr. Taghizadeh, we feel that pancreaticglucagon insufficiency may have been important. It is temp-ting to postulate that these patients, already deficient in insulinreserve,! are similarly lacking in stores of pancreatic glucagonwith which to help maintain glucose homoeostasis. Recentlyestablished techniques of plasma-glucagon immunoassay,2 3
may well provide the answer.An important clinical application of these findings is to
emphasise the need for caution in administering insulin to sub-jects with " pancreatic diabetes " if serious hypoglycaemia is tobe avoided. This complication has previously been found to bean important cause of death in such patients.4
B. I. JOFFES. BANKI. N. MARKS.
Endocrine Research and Gastrointestinal Units,Department of Medicine,
University of Cape Town, South Africa.
1. Joffe, B. I., Bank, S., Jackson, W. P. U., Keller, P., O’Reilly, I. G.,Vinik, A. I. Lancet, Oct. 26, 1968, p. 890.
2. Hazzard, W. R., Crockford, P. M., Buchanan, K. D., Vance, J. E.,Chen, R., Williams, R. H. Diabetes, 1968, 17, 179.
3. Eisentraut, A., Ohneda, A., Parada, E., Unger, R. H., ibid. p. 321.4. Bank, S. S. Afr. med. J. 1966, 40, 342.
GENERAL PRACTITIONERS AND THE
HOSPITAL SERVICE
SIR,-The joint working-party on Medical Staffing in theHospital Service stated 1 that, without the help of 3628 foreigngraduates, there would be a breakdown in the hospital servicebelow the grade of senior registrar. Whether it is good or badthat the medical staffing of the hospital service depends, asit does, on those 3628 foreign graduates is not the questionI wish to ask. According to the census of junior hospital staffcarried out by the Health Departments on March 31, 1960,the numerical needs of the hospital service below the grade ofsenior registrar were 3587 registrar posts (some vacant), 2877senior-house-officer posts (some vacant), and 3023 house-officer posts (registered and preregistration), a total of 9487posts.2 A current survey made by the Birmingham RegionalHospital Board shows that 89% of the general practitionersquestioned wished to work in a hospital in addition to workingas a general practitioner.3 The question I now wish to ask iswhether there are enough general practitioners in GreatBritain to do the work now undertaken in the hospitals byregistrars, senior house-officers, and house-officers, if the
general practitioners were integrated into the medical staffingstructure of the hospitals.On Sept. 30, 1967 there were, in England and Wales, 19,549
principals in general practice and 758 assistants,4 a total of20,307. On the same date there were in England and Wales4516 registrars and 2781 senior-house-officers, a total betweenthose two grades of 7297 postS.4 To reduce the demand whichthe hospitals would make on the general practitioners, I am
going to exclude the work now done by the house-officers,who on March 31, 1960, numbered 3023.2 Furthermore, Iwill confine the calculations to England and Wales, since
up-to-date figures of the hospital staffs in Scotland are notavailable. In England and Wales, therefore, if on Sept. 30,1967, the general practitioners had taken over the work of4516 registrars and 2781 senior-house-officers, they wouldhave had to provide 65,673 sessions (at 9 sessions a week)each week-taking each session as 3112 hours, the hospitalswould have required 229,8551/2 hours per week. If only theprincipals took part in the hospital work, each would have hadto give up 11 -8 hours to the hospital (229,855 -7-19,549); if the758 assistants were included the figure would fall to 11.3hours a week (229,855=20,307). Whether a general practi-tioner could afford between 11 and 12 hours a week in thisway is unknown; but the Birmingham survey found fhat thosegeneral practitioners who did work in hospitals provided 7-8hours a week.3 It will be remembered that 89% of the generalpractitioners questioned wished to do hospital work. 89% of19,549 principals would be 17,403 general practitioners.
Notionally, it would need about another 8000-12,000 moreprincipals in England and Wales to take over the work of theexisting registrars and senior-house-officers if each generalpractitioner can provide the hospitals with only 7-8 hours ofhis time per week. The Birmingham survey, however, sug-gests that the integration of general practitioners into the
hospital service would not make the present registrars andsenior-house-officers unnecessary. There are, at present, 27
specialties in the hospital service. Most general practitionersare interested only in general medicine, obstetrics and
gynxcology, and paediatrics, and a few in geriatrics, surgery,and dermatology.3 It seems therefore that general practitionerswould be willing to take over duties only in about 6 out of the27 existing hospital specialties. The combined total ofregistrar and senior-house-officer posts in general medicine,obstetrics and gynaecology, and paediatrics add up to only2477 posts out of a total of 7297. This raises the question ofwhich doctors are going to fill the 4820 (7297-2477) hospitalposts the general practitioners do not want. Nevertheless, it
1. Medical Staffing Structure in the Hospital Service: Report of the JointWorking Party; para. 96, p. 32. H.M. Stationery Office, 1961.
2. ibid. appendix 4, paras 5 and 6, p. 75.3. Report of a Sub-Committee of the General Practice Liaison Committee
of the Birmingham Regional Hospital Board, 1968.4. See Lancet, Aug. 24, 1968, p. 448.

1039
has been claimed that 53-9% of patients admitted to hospitalin South-East England could have been medically cared forby a general practitioner.5
F. S. A. DORAN.General Hospital,
Bromsgrove, Worcs.
PROPRANOLOL AND 131I FOR THYROTOXICOSIS
SIR,-We are impressed with the proposal of Dr. Haddenand his colleagues (Oct. 19, p. 852) to pit propranolol againstthe symptomatic phase of hyperthyroidism, clearing the smoke,as it were, to better observe the fading fire as it is quenched byradioiodine. For the occasional hyperkinetic Graves’ diseasepatient with
" hot " hyperthyroidism, whose symptoms couldnot be subdued otherwise, propranolol with its sedative andp-receptor-blocking actions should be a’welcome agent toaccompany the administration of iodine-131.
Ordinarily control of hyperthyroidism by preliminaryadministration of antithyroid drugs and sedation with barbi-turates, reserpine, or guanethidine will allow the use of smalleryet effective doses of iodine-131. Resumption of this combinedtherapy while awaiting the suppressive action of the radioiodineneed not interfere with biochemical tests of thyroid functionif they are indicated.
It seems to us that, while the effectiveness of propranolol hasbeen demonstrated, the long-continued use of so potent anagent in other than selected patients is fraught with risk.
WILLIAM S. REVENOHERBERT ROSENBAUM.
Department of Medicine,Harper Hospital
and Wayne State UniversityCollege of Medicine,
Detroit, Michigan 48201.
CHLOROQUINE BLINDNESS?SIR,-Dr. Long’s letter (Oct. 19, p. 875) casts a shadow of
doubt on the use of the most valuable antimalarial drug that wepossess. It should not be left without comments, like those ofDr. Lovett last week (p. 972), that will magnify the question-mark appended to this alarming title.The reported history of the case is vague, and the amount of
chloroquine ingested by the patient (2 tablets of’ Nivaquine ’,corresponding to 300 mg. of chloroquine base) seems to bemuch too small to cause serious side-effects, least of all rapidloss of sight.
Legitimate concern with toxic effects of chloroquine on the eyehas been expressed over the past ten years, during which timethis drug has been used in very large doses and for long periodsfor treatment of rheumatoid arthritis and other diseases,6-9but it should be remembered that the dosage of chloro-quine for treatment and prevention of malaria is of an entirelydifferent order of magnitude. An excellent survey by Ardenand Kolb 10 of 347 patients with rheumatoid arthritis who weregiven a total dosage of 5-8 g. per kg. body-weight of chloro-quine over 26-39 months, indicated an overall incidence ofretinal changes with some impairment of vision in 13% ofpatients: this figure rose to 40% in patients who took 8 g. perkg. of chloroquine or more. For treatment of malaria the usualdose of chloroquine does not exceed 2-5 g. of base, or about 0-05g. per kg. given over 1 week. This is about 100-150 times lessthan the amount given for treatment of rheumatoid arthritisand no serious effects on the eye have been reported at thelower dosage. For prevention of malaria, chloroquine, taken inthe relatively high dosage of 100 mg. daily (instead of the usual300 mg. a week) and for several years, may produce punctatekeratitis or retinopathies. 6 cases of retinopathy in personstaking such high doses of prophylactic chloroquine for 8-105. Report of a Survey of Hospital Admissions in South East England by
the South East Faculty of the Royal College of General Practitioners.Jl R. Coll. gen. Practnrs, 1967, 14, 293.
6. Cambiaggi, A. Archs Ophthal., N. Y. 1957, 57, 451.7. Hobbs, H. E., Eadie, S. P., Somerville, F. Br. J. Ophthal. 1961, 45, 284.8. Burns, R. P. New Engl. J. Med. 1966, 275, 693.9. Carr, R. E., Gouras, P., Grunkel, R. D. Archs Ophthal., N.Y. 1966, 75,
171.10. Arden, G. B., Kolb, H. Br. med. J. 1966, i, 270.
years have been described," 112 but they constitute rather anexception than a rule.
In conclusion, it seems that in Dr. Long’s case the suspicionthat the administration of 300 mg. of chloroquine base can beresponsible for rapid blindness is unlikely, to say the least.Chloroquine remains one of our best antimalarials, with arecord of reliability and safety that is incomparably better thanthat of many other drugs.
L. J. BRUCE-CHWATT.
London School of Hygiene andTropical Medicine,London W.C.1.
R.N.A. SYNTHETIC ACTIVITY OF HUMAN OOCYTE
SIR,-The developmental sequence of oogenesis during thefoetal period in man has been clearly elucidated.13 Oocytes pro-ceed through the normal sequence up to the diplotene stage. Atthis time, during the eighth and ninth month of gestation, thediplotene chromosomes extend and enter a
" resting " stagetermed dictyotene. Though synthetic activity has been sus-pected in oocytes of this stage, little has actually been demon-strated. R.N.A. synthesis has been shown to occur in themouse,14 but not in man.
Photomicrograph of a radioautogram of a 1[1. section of humanovary, pulse-labelled for 50 minutes with [’H]-uridine.Reduced to three-quarters from x 1000.
We have cultured ovarian tissue from an eight-week-oldhuman female in the presence of [3H]-uridine for 50 minutes.Radioautographic techniques then applied to sectioned materialshowed that R.N.A. synthesis occurred within the oocyte as wellas in the surrounding follicle and stromal cells. The accom-
panying figure shows a concentration of silver grains over themeiotic chromosomes. These findings confirm the active roleof the genetic material of the human dictyotene oocyte.
L. J. BEAUREGARDS. K. GHOSALP. H. LAMARCHE.
Genetics Department,Rhode Island Hospital,
Providence, R.I. 02902, U.S.A.
11. Ravault, M. P. J. med. Lyon, 1965, 46, 1391.12. Francois, J., De Becker, L. Annls Oculist. 1965, 198, 33.13. Ohno, S., Klinger, H. P., Atkin, N. B. Cytogenetics, 1962, 1, 42.14. Odeblad, D., Magnusson, D. Acta endocr., Copenh. 1954, 17, 290.