GENERAL ORIENTATION TO - Weebly
29
ORIENTATION TO NICU ROTATION Neonatal Intensive Care Unit Montreal Children’s Hospital 2016-2017
Transcript of GENERAL ORIENTATION TO - Weebly

ORIENTATION TO NICU ROTATION
Neonatal Intensive Care Unit Montreal Children’s Hospital
2016-2017

Welcome to the NICU! This document is prepared to serve as an outline of the NICU rotation. It provides information on organizational and educational aspects of our rotation. We hope that it will help you in making your rotation a great learning experience! ROTATION COORDINATOR: Medical coordinators: Dr Alexandre Barbier Office B05.2712 Ext 24452 [email protected] Administrative coordinator: Mr Roch Saillant Office B05.2039 Tel 412-4452 Fax 412-4356 [email protected] GENERAL INFORMATION: 1) Daily ward schedule: 7:30 AM: Sign-in; Please be PUNCTUAL to accommodate teaching and discharge rounds. Weekend sign in for residents and clinical assistants is at 8:00 a.m. 8:00 AM: Teaching sessions. 9:00 AM: Patient assessment and preparation for rounds. 9:30 AM: Ward rounds. Fluid orders need to be completed BEFORE noon every day. 5:00 PM: First sign out. Second sign out is at 8:00 pm
• A schedule of teaching sessions is posted on the bulletin board at the work station. • Continuity Clinics: Residents are expected to sign out their patients to their colleagues
or the attending before leaving for their continuity clinic. • In the case of illness or other serious difficulty preventing attendance or delaying
arrival in the NICU, the trainee must communicate with the supervising neonatologist and, for pediatric residents, the chief resident on call as soon as possible.
2) Sign out: Sign out is done in team, in the conference room, using ISBAR. Please sign out concisely, but include all relevant information. Prepare your sign out.
2

Identify: The patient AND unique ID number Situation: The one-liner summary statement. Sets the clinical context and Severity
(STABLE, WATCHER, UNSTABLE) Background: Provide RELEVANT information only (events leading to admission, hospital
course, ongoing issues (by problems or diagnoses) • Deciding what is relevant requires preparation • Don’t forget ‘less is more’ • Include aspects of history, examination, investigations and management where relevant
Assessment: State what you think is going on. Give your interpretation of the situation Recommendation and Read-back: State what needs to be done
• Clarify mutual expectation • Ask and remain open to questions
Principles of Sign In and Sign Out:
• NEED TIME KEEPER TO KEEP EVERYONE ON SCHEDULE • Vsign updated overnight and printed out by team
o Focus on active patients and over night issues o Confirmation of stability of patients to be discharged / transferred o For all other patients - who were not seen or called for - status quo
• At the beginning of a block or after weekend, neonatologists will do the detailed sign in on Friday night.
• A copy of the admission note will be given to the team and only overnight issues will be mentioned.
V-Sign is used to prepare the Sign out document and can also be used to elaborate the Progress Note. 3) The teams: Team members Neonatal Nurse Practitioners have been providing clinical coverage in the NICU since 1994. The NNP’s follow the same group of patients consistently from admission to discharge and function in a collaborative fashion reporting to the neonatologist on service. In addition to clinical practice, the NNP’s are also involved in educational, administrative and research activities. Clinical Assistants: Some Pediatricians interested in neonatal care are also part of the treating team. Respiratory therapists are valued members of the 9C team who have an important role in the management of our patients. Many RTs have an advanced role, either as members of our transport team or an educator. Social Workers: There will be 2.5 FTE to support the patients and families in the NICU. 3

Nutritionists: Three nutritionists will be making rounds with the three teams. On weekend, one nutritionist will take care of new TPNs (maximum 8). Occupational Therapist: There is one Occupational Therapist Pharmacists: Two Pharmacists will be making rounds with the three teams on alternate days. Another Pharmacist will be in the Pharmacy to prepare the orders as they come in. Function During daytime, there will be three medical teams (Blue, Yellow and Silver) to cover NICU patients in addition to the Birthing Center, transport and prenatal consultations. Every day, there will be a team rotation between the 3 activities to maximize exposure. Each team will be composed of a neonatologist and three other members (fellow, resident, NNP, clinical assistant and/or students). Each team will cover a specific area (see map) of the NICU that will include about 16 to 18 patients. As well, one of the three neonatologists will be in charge and responsible for bed management. He/she will hold this responsibility for one week. Finally, there will be a night and weekend rotation of neonatologists. During nighttime, there will be one neonatologist on site and two residents/NNPs/clinical assistants. During daytime on weekend, there will be 2 neonatologists. For nights and weekends, the medical teams will divide the unit in half (A and B).
A BLUE
21-24, 26-36 39, 47, 48
YELLOW 37, 38, 40-46
B YELLOW 52-57, 60-63
SILVER 49-51, 58,59, 64-75
Below is an example of a weekly medical assignment board. Note how the responsibilities rotate on a daily basis.
MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY SATURDAY SUNDAY
Blue Yellow Silver
Blue Yellow Silver
Blue Yellow Silver
Blue Yellow Silver
Blue Yellow Silver
Team A
Team B
Team A
Team B
D T C C D T T C D D T C C D T D T T D
NIGHT NIGHT NIGHT NIGHT NIGHT NIGHT NIGHT
Team A Team B Team A Team B Team A Team B Team A Team B Team A Team B Team A
Team B
Team A
Team B
4

Teams composition: Team A- (blue) neonatologist; fellow; 1-2 residents; 1-2 NNP Team B- (yellow) neonatologist; 1 resident; 2 NNPs; 1 medical student Team C- (silver) neonatologist; 1 NNP; 1 clinical assistant; 2 medical students Based on a rotational schedule - the teams will face a different task each day - example Team A – (D) Delivery room Monday - Tuesday transport - Wednesday antenatal consult ….. Team B – (T) Transport on Monday - Tuesday antenatal consult - Wednesday delivery room …. Team C – (C) Consult on Monday - Tuesday delivery room - Wednesday transport ……. N.B. The Consult team will always sign in late and be the late team for sign out. The consult binder will be kept at the Silver Workstation. This allows for the following:
• three balanced team • equal exposure to delivery room and transport (over the month) • continuity of care (from admission to discharge) • minimize patient movement
One neonatologist from the above team will be the Coordinator of bed management for the week
• responsible to gather information from other neonatologist • huddle in the morning regarding the movement of patients - including for test / transfer /
discharge; potential admissions from referring centers or from the delivery room • will ensure that ultrasounds requests are given to the unit coordinator to be entered in
Medivisit • will give the list of patients that require a cardiac echo to be faxed by the unit coordinator • will make the list of patients for the Radiology Rounds • will remind the team regarding daily academic activities
A day in the NICU: 07:30 - Signing in of the day team AM Duties
1. Assign yourself to the patient 2. Change your Spectralink battery 3. Wipe your Spectralink 4. Write Social Service Consults 5. Share information on Discharges, Transports, Tests 6. For Weekends, decide who will need a new TPN.
08:00 Morning huddle for the Delivery Team to occur at Silver Station. 5

08:00 - 09:30 – Patients are seen and examined 09:30-12:30 – Rounds
• starting with most unstable patient first then completing the unit according to the Nurses’ availability.
The round is a time to review the patient’s status, make plans, write orders, update the patient’s note and to teach. This is a multidisciplinary activity where nurses, respiratory therapists, nutritionist, pharmacists and parents are present and participate. The RN will present overnight issues, feedings, concerns, questions and family issues. RNs will arrange their breaks around Round’s time. Thus, rounds should happen according to the nurses’ availability. The RT assigned to NICU will present the patient’s respiratory status including weaning from INO /mechanical ventilation/HFO as well as VAP status report. The goal is to identify patient who can be weaned early in the day so any planned extubation or change in therapy can occur before 5pm. It is suggested during rounds to use computer on wheels (COW), write orders while your colleague present the patient, invite parents to join in, write the note in Vsign and replenish the forms on COW. If you want to page a consultant, please do it yourself through your spectralinks to avoid the Unit Coordinator running after you. If you admit a patient, pleaseeeeee inform immediately the Unit Coordinator in order to get the patient’s MRN in a timely fashion.
14:00 - Afternoon huddle
o before bed management o phone contact by charge nurse o coordinator neonatologist must have spoken with other teams and gathered
information 17:00 - Evening sign out to late team - 30 minutes
• consultation team is staying late 20:00 - Night sign out starts
• one person identified from team to sign out • all team members are present • Patients signed out by order and reminded to the team to verify that those planned for
discharge or transferred are stable to go If an emergency occurs during sign out, it is the on call team that will respond to the emergency while the incoming team will get the sign out. 6

Nights • Each resident/fellow/clinical assistant/NNP will cover half of the unit (geographically
determined). Coverage of the delivery room will be given to the resident/fellow/clinical assistant/NNP that the less busy half. The other, will cover transport. The neonatologist will have an overview of the whole unit. In a busy unit, people will help each other.
Week- end coverage
• 2 neonatologists • 1 resident / clinical assistant • 1 NNP • medical student • The unit will also be divided in half and each team (Neonatologist and resident) will
cover Birthing center or transport. Roles (Delivery or transport) will alternate between Saturday and Sunday. Again, in busy times, teams will help each other.
Rotations: Each neonatologist on service is responsible for resident supervision and assessment of progress during the rotation. 4) Nutrition Coverage (Week Days and Weekends) During the week, 3 nutritionists will help the three teams to provide the best nutrition to our patients. Coverage Protocol during Weekend
1. There will be 1 nutritionist present for each day of the weekend and STAT days. 2. There is no possible same-day replacement in case of sickness. 3. Work day will be from 8:00-16:00, including lunch hour from 12:00-13:00. 4. The nutritionist is expected to complete a maximum of 8 TPN per day, including new
patients and modifications. 5. The Nutritionist and Pharmacist will talk to each of the two medical teams to decide who
will need a new or modified TPN. 5) Delivery Room Attendance The goal is to anticipate any identifiable situation that may require pediatric presence prior to the delivery of the newborn in a timely fashion. Clear communication Identification Identify yourself Situation ∙ Why is neonatology being called?
Briefly state the problem, what it is, when it is started or happened, and how severe
7

Background Gestational age Prenatal complications, presence or absence of major anomalies Membranes: intact, ruptured Fluid: clear, cloudy, meconium
Assessment Level of risk to the baby Plan for delivery: vaginal or c-section, level of urgency
Recommendation ∙ Categorize level of priority level anticipated, inform the neonatal team and initiate the group call if required.
Role within the Birthing Center. First, one professional within the birthing center needs to be assigned to each baby to be born. This person needs to be able to initiate resuscitation as per NRP guidelines. When a call is launched, the receivers will have the information and the room in which they need to go. Please note that the Peds Nurse (designated OB nurse for the baby) will be documenting the resuscitation. You need to inform her of your interventions. Also, you should know that mothers at risk of imminent delivery are on D06 south. GBS positive mother who received antibiotics less than 4 h before birth. Antenatal diagnosis or suspected chromosomal disorder Consult NICU post delivery for newborns born 35-37 week of gestation before they get transferred to the nursery Protocol for newborn care within the delivery room: Care to be provided without calling the NICU team. Hepatitis B vaccination and immunoglobulin according to maternal status Screening for hypoglycemia as per the CPS recommendation HIV positive mother (Follow HIV protocol) Other 5) Infection Control: 1. Wash your hands on entering the unit, and before and after touching each patient and its environment. 2. Rings, bracelets, watches or any other hand/wrist jewels, faked nails and nail polish are not allowed when on service in the NICU 3. Sleeves MUST be rolled up to the elbow; in exceptional cases only when sleeves cannot be rolled up, a clean gown covering sleeves must be worn. 4. In the presence of any symptoms or a cold or URTI symptoms, a mask MUST be worn. 5. Please read the annexed document on the Five Moments. 6. It is recommended to take the Hand washing certification on the Website of the Patient Safety Institute: http://cpsi.discoverycampus.com/en/index.html N.B. Washing your hands reduces infections by 50%!!
8

6) Communication Spectralinks: Spectralinks are attributed by Team (Blue, Yellow or Silver) and Function (Delivery/Code Pink or Transport). EACH MORNING, please wipe them and change your battery. Please note that the Code Pink spectralinks have the Push-To-Talk (PTT) feature, i.e. they also function as walkie-talkie. When you receive a call from the Birthing Center, you can use the PTT to call the rest of the team. The code pink buttons in each room, in the Birthing Center or on D06 are linked to the Code Pink spectralinks. If you are on the phone and a Code Pink is called, it will cut the conversation. Sometimes, the spectralinks stop working, just turn them off and restart them and it should reset them. VSign: There are many functionalities available, i.e. view results (soon microbiology and Xrays), know who is assigned to the patient, write and read notes to be part of handover or progress note and communication via text messages. Please assign yourself to your patients in the am to help the communication. VSign is available on PCs, Thin Clients (computers in alcoves) and Computers on Wheels via glenb06s. To access VSign on Thin clients, use vsign.muhc.mcgill.ca/VSign/ and you will be able to print your notes. TO ENSURE CONFIDENTIALITY, PLEASE DO NOT LEAVE HANDOVER SHEETS OR BRAINS THROUGHOUT THE UNIT. 7) On call: At the beginning of your call, introduce yourself to the nurse in charge, the transport RT and RN, the Resus nurse and RT. It is recommended to do a huddle with the Resus Team to decide ahead of the responsibilities of each team member. Responsibilities when On Call:
1. You should go around and examine each baby, especially the ones that are acute. 2. Verify the nursing sheet to anticipate problems. 3. Ensure that laboratory tests are ordered for the following morning. 4. Ensure that Xray requests are done for the following day. 5. Write a note for all the acute patients and the other ones for which you have made a
change. Post-call days:
• Residents who are leaving post call are expected to attend teaching sessions. 8) Orders:
1. Admissions order form is available to guide you on what needs to be prescribed. 2. Fluid orders MUST be done for each patient receiving intravenous infusions, every day,
BEFORE noon (see Annex 10).
9
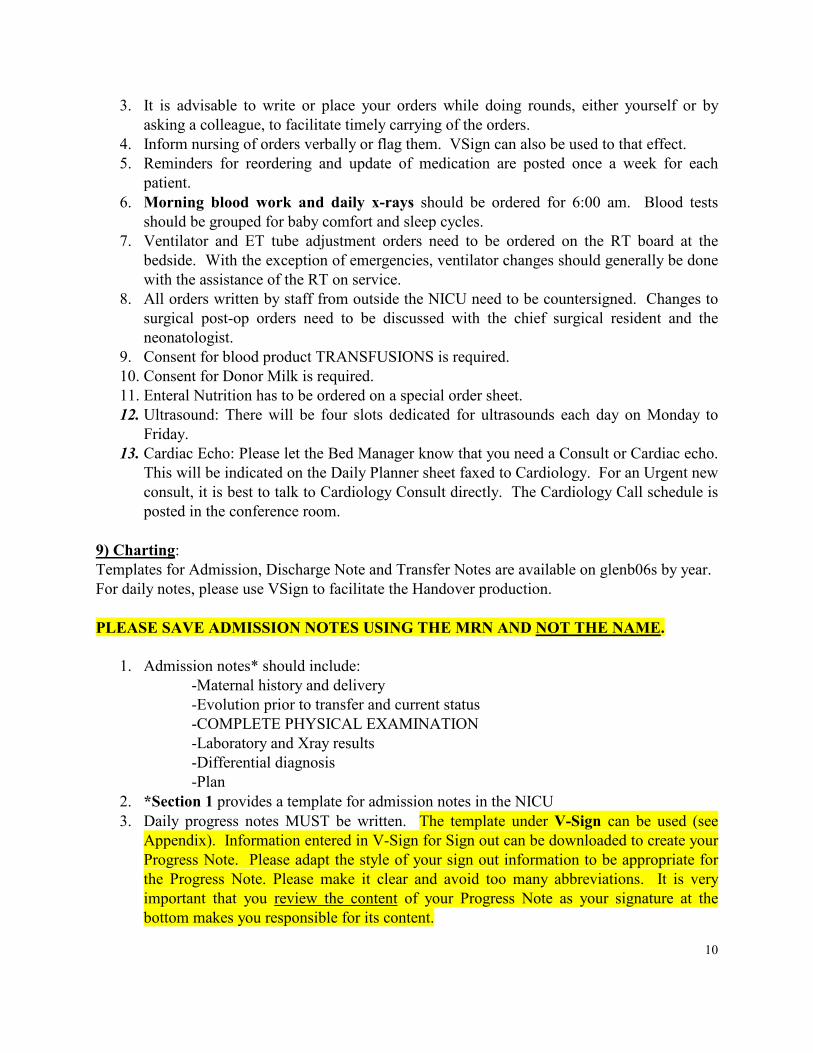
3. It is advisable to write or place your orders while doing rounds, either yourself or by asking a colleague, to facilitate timely carrying of the orders.
4. Inform nursing of orders verbally or flag them. VSign can also be used to that effect. 5. Reminders for reordering and update of medication are posted once a week for each
patient. 6. Morning blood work and daily x-rays should be ordered for 6:00 am. Blood tests
should be grouped for baby comfort and sleep cycles. 7. Ventilator and ET tube adjustment orders need to be ordered on the RT board at the
bedside. With the exception of emergencies, ventilator changes should generally be done with the assistance of the RT on service.
8. All orders written by staff from outside the NICU need to be countersigned. Changes to surgical post-op orders need to be discussed with the chief surgical resident and the neonatologist.
9. Consent for blood product TRANSFUSIONS is required. 10. Consent for Donor Milk is required. 11. Enteral Nutrition has to be ordered on a special order sheet. 12. Ultrasound: There will be four slots dedicated for ultrasounds each day on Monday to
Friday. 13. Cardiac Echo: Please let the Bed Manager know that you need a Consult or Cardiac echo.
This will be indicated on the Daily Planner sheet faxed to Cardiology. For an Urgent new consult, it is best to talk to Cardiology Consult directly. The Cardiology Call schedule is posted in the conference room.
9) Charting: Templates for Admission, Discharge Note and Transfer Notes are available on glenb06s by year. For daily notes, please use VSign to facilitate the Handover production. PLEASE SAVE ADMISSION NOTES USING THE MRN AND NOT THE NAME.
1. Admission notes* should include: -Maternal history and delivery -Evolution prior to transfer and current status -COMPLETE PHYSICAL EXAMINATION -Laboratory and Xray results -Differential diagnosis -Plan
2. *Section 1 provides a template for admission notes in the NICU 3. Daily progress notes MUST be written. The template under V-Sign can be used (see
Appendix). Information entered in V-Sign for Sign out can be downloaded to create your Progress Note. Please adapt the style of your sign out information to be appropriate for the Progress Note. Please make it clear and avoid too many abbreviations. It is very important that you review the content of your Progress Note as your signature at the bottom makes you responsible for its content.
10

4. Please remember to write procedure notes when appropriate. 5. On call, notes MUST be written EVERY night for ventilated and unstable patients. These
notes can be manuscript. 6. Off service notes have to be written on all your patients, even though you are night float. 7. Charting must be completed before leaving the hospital!
10) Lab results and others Lab Results: OACIS EEG reports are usually faxed within 24 to 48 hours; in situations where a report is needed more urgently, you need to contact the electrophysiology lab directly. EMG and nerve conduction studies’ preliminary reports are usually written in progress notes by the neurologist. ECG results are available under Document in OACIS. The cardiologist on service may be consulted for a more urgent interpretation. In fact, you can use the scanner to email the tracing to Cardiologists. Cardiac echo reports are available on PACS. Radiology Results: 1. Xrays, CT, MRI and US are available for viewing on the PACS system. 2. You should write your impression when you view an xRay. This allows better communication with the Radiologist and avoids calls for tube placement when they have already been adjusted. 3. Preliminary interpretation of some exams are available on PACS. 11) Transport Calls: Our neonatal transport system is very busy and requires tight coordination in order to maintain efficient and safe services. Here are a few recommendations regarding the reception and coordination of transport calls:
• All calls will be transferred to the Transport Spectralink (25648). NEVER USE THIS SPECTRALINK TO MAKE PHONE CALLS. The transport clipboards are available in each workstation. It contains sheets to write patient’s information. Please document well the patient’s information on the transport sheet.
11

IMPORTANT INFORMATION TO COLLECT
12

• Once completed, PLEASE NOTIFY IMMEDIATELY THE TRANSPORT TEAM or place it in the transport binder in the transport area if it is a consultation.
• Please answer the phone in French. Many referring physicians are French-speaking. When this is the case and if you do not feel comfortable to interact in French, it is recommended to offer the referring physicians the possibility to speak with a French-speaking health professional. This person can be the attending, another resident, a transport nurse, a nurse practitioner or any member of the nursing team, depending on the availability of each.
• At the time of a request to transfer a patient, the following team members need to be notified: neonatologist on service, nurse in charge, transport nurse, RT on transport and ward coordinator.
• If transfer is urgent, tell the referring physician that we will transport the patient and we will determine later where the patient will go. Please also tell the referring physician that you will call back with further advices after talking to the neonatologist. Then, notify the charge nurse (and the neonatologist) ASAP to determine our ability to admit the patient.
For the transport of unstable patients, please note that a Code blue card to call elevator is available and located in transport area. 12) Prenatal consultation: When there is a consultation for preterm labor, especially for ELBW, the meeting with the family should be with the neonatologist. Copies of consultations are placed in the filing cabinets in the work area near the conference room. Consultations and duplicates are classified by expected date of delivery and by alphabetical orders. When there is a prenatal diagnosis established of congenital anomaly, copies of consultations are also placed in the filing cabinets in the work area near the conference room. In addition, you can view the patient’s file in OACIS under Prenatal Neonatal Consultations patient list. Recommended approaches will be in the consultation. Furthermore, the patients anticipated to deliver in the month will be listed on the board in the conference room. 13) Discharges: Discharge Coordinator Role:
• Initiates the identification babies that can be moved (done in AM at medical “sign over”), communicates plan to charge nurse and unit coordinator.
• Attends AM Bed Huddle meeting. • Does CLSC referrals for all babies discharged home from the unit. • Reviews D/C plan and follow-up appointments with medical team.
13

• Return from pass babies: Is assigned to baby and works with medical team to “wrap up” discharge.
• Organizes ward visits for long term babies (could be organized for short term also, if requested).
• Organizes multimeetings. • Communicates with Nurse Manager/Charge Nurse on wards to give brief summary of
babies to be transferred. • Initiates contact with MCH D/C coordinator (Soo-Lin Ng ext. 23080) for complex cases,
TDU and organizing of equipment for home use (oxygen and suction equipment). • Does recruitment for follow-up in neonatal clinic and meets families prior to discharge. • Introduces self/role to families as needed (family centered care). • Participates in teaching at “Orientation day” (D/C coordinator role/D/C folder). • HEFP & seizure teaching for families whose babies will be followed in neonatal clinic. • Communicate with referring hospital to inquire if baby qualifies for transfer back • Introduces self/role to families as needed (family centered care).
Bridge Team Role:
1. All patients fulfilling criteria for NNFU. To be seen at the ages they would normally
have been seen in the clinic for a neuro-developmental evaluation (4 months, 9 months CGA, etc)
2. Patients having spent > 60 days in hospital (excluding the well premature babies who spend >60 days on a regular basis; they should be seen if they are still hospitalized past their term corrected gestational age)
3. Patients with poor neurologic prognosis, requiring decision-making about treatment versus palliative care
4. All patients with Broncho-pulmonary dysplasia leaving on oxygen 5. All patients with Congenital Diaphragmatic Hernia, before discharge 6. Patients with complex feeding issues (important feeding intolerance, anticipated long
term gavages, decisions about gastrostomy) 7. Anticipated complex discharges/transfers due to long hospitalization/multiple complex
issues 8. Specific questions from families about long term follow-up
Neonatal Follow up: Criteria for entry in the MCH Neonatal Follow-up Program are described in you. Discharge and Transfer Summaries.
• Recommendations for discharge summaries in the NICU are provided in Section 2. A template for discharge summaries is available for you to use at the nursing station computer.
• In order to access the file for the discharge summaries, please use the following Novell
14

account: Username: glenb06s and password: glenb06s • You must always access the Discharge Summaries folder when doing a summary on a
patient. Please NEVER use another patient discharge summary to write over it. When saving the document that you are working on, MAKE SURE you save it under the right patient.
• In cases of a TRANSFER to another ward, a distinct summary MUST be completed, identified as “NICU Transfer Summary”. A Transfer Summary template is available in the Discharge Summary Folder on the desktop of the main front desk computer.
• Francophone patients, particularly if referred from francophone centres, should have their list of diagnosis on the summary sheet done in French. Ask your attending, a colleague or NNPs for assistance.
• Prescribe enough medications for several months in case follow up plans are disrupted (i.e. repeat X 2-3)
14) Work environment The NICU can be at times, a very stressful environment. The presence of the second neonatologist is to help to decrease the stress and optimize the workload. There is a code of conduct that applies to all workers. If you have specific concerns, please feel free to contact the rotation coordinator or the Nurse manager.
15

LEARNING OUTCOMES: Please refer to the Learning Outcomes document for your level of training. COURSE CONTENT AND INSTRUCTIONAL MATERIAL: Instructional material consists primarily of clinical cases, bedside teaching, case reviews, ongoing reading around case material, and scheduled lectures. Clinical Material The NICU is especially good for exposure to these clinical learning opportunities:
1. Prenatal consultations 2. Delivery Room management 3. Prematurity 4. Transportation of sick neonates. 5. A large diversity of congenital anomalies and syndromes. 6. Pre-operative and post-operative surgical neonates. 7. Diverse complications of prematurity. 8. Infants who require advanced technology for respiratory and cardiovascular stabilization. 9. Infants with neurological problems. 10. Infants who require sub specialty evaluations and interventions. 11. Infants with complex multi system disease. 12. Infants from diverse social and cultural contexts who require specialized support services.
Formal Teaching Schedule Monday 12:30-13:30 Perinatal Rounds Monday 16:00-17:00 Radiology Rounds Tuesday 8:15-9:15 Neonatal Surgery rounds / Journal Club Tuesday 12:00-16:00 Protected teaching time (Pediatrics) Wednesday 8:00-9:00 Pediatric Grand Rounds Thursday 9:00 Mock Code Friday 13:00-14:00 McGill Neonatal Rounds Friday 14:15-15:00 Cardiology rounds Friday 14:00-16:00 Fellow Teaching In addition, there is a half-day orientation on day one with additional orientation sessions in week 1 for all residents and mock codes sessions. Residents are expected to make every effort to attend teaching sessions. **Attendance to all morning sessions i.e. from 8 to 9 AM is MANDATORY 16

MOCK CODE Residents will have the opportunity to participate to Mock Codes. This is a good opportunity to put into practice your NRP knowledge and skills. The objectives would be for: Junior Residents: 1. Learn NRP Senior Residents: 1. Be able to diagnose an emergency situation 2. Develop an action plan 3. Prioritize your interventions 4. Participate, delegate or lead the emergency intervention 2. Learn to work as a team 3. Learn to intervene in a timely fashion (including procedures) 4. Learn to communicate effectively with the team members At the end of the Mock Code, a debriefing will take place to assess your interventions and give you feedback in order to improve yourself. Included in the orientation, resident will get a NRP refresher to familiarize him/herself with the material. Mock Codes will take place on Thursday.
17

Learning Materials 5. Please consult your USB key as there is several references provided.
6. NICU WEB site: WWW.MUHCNICU.WEEBLY.COM where you will find tables, graphs
and protocols. 7. Computer Resources:
The computer in the reception area has McGill University Internet Access with complete electronic library resources (PUBMed, peruse, online journals, electronic biomedical textbooks, etc). The Red Book on-line is also available via a link on the desktop.
Physician checklists and parent guides for the more common anomalies from 'Preventive management of children with congenital anomalies' is available on H:\share on Nwfs11\Vol1\Newborn\ newborn medicine department\neonatal follow up\Congenital Anom-Synd\Checklists
8. Medication Information: Medication information is available on Lexicomp, NICU/PICU pharmacist 7 days/week, and the neonatologist! ASSIGNMENTS: Residents are generally expected to prepare a Journal Club during their month on 9C. Most present at combined neonatal/surgical teaching sessions, but there may be other opportunities to present during other neonatal teaching time. EVALUATION: Timing 1) Written monthly evaluations (ITER forms) are supplied every 4 weeks. These are
discussed with the resident. Residents and fellows are in turn expected to complete an evaluation at the end of their rotation.
2) The end of week 2 is a good point for the trainee to solicit feedback about his/her
progress. Supplemental evaluations may be available before the end of the rotation if specifically requested. It is also a good time to ask the attending to supervise a physical examination.
18

3) Informal information about progress is available on request at any time. Basis for evaluation (CanMEDS) CanMEDS evaluation forms are used to assess resident progress. Evaluation is done according to the ‘Expected Learning Outcomes’ previously detailed. It is expected that the resident will progressively acquire skills throughout his training. Medical Expert - Evaluation is made from observation of performance, technical skills, and charting during the rotation. Increasing clinical knowledge, technical competence, and autonomy in emergency care are expected. Communicator - Evaluation is made by informal (anecdotal) assessment of social skills during the rotation. Residents who experience difficulties in working with other team members are urged to discuss these with the neonatologist on service as early as possible. Collaborator - Evaluation is made by informal assessment of skills in liaising with other staff during the rotation. Manager - Evaluation is made by informal assessment of managerial skills during the rotation. Health Advocate - Performance during the rotation is assessed. Scholar - The resident is evaluated in the ward setting on evidence of ongoing reading around cases, utilization of medical literature, and the acquisition of an appropriate knowledge base. The oral presentation is also noted. Professional - The professionalism of performance during the rotation is assessed. Suggested references
1) Gomella TL Neonatology 7th edition. Management, Procedure, on-call procedures, Diseases and Drugs. 2013.
2) Textbook of NRP.
3) Fanaroff and Martin’s Neonatal-Perinatal Medicine. Diseases of the fetus and Infant, 10e.
4) Blackburn S. Maternal, Fetal and Neonatal Physiology, 4e.
5) McGraw-Hill Specialty Board-Review Neonatal-Perinatal Medicine, 2015.
19

6) Breastfeeding Handbook for Physicians, 2nd Ed. American Academy of Pediatrics
7) Avery’s Diseases of the newborn, 2012, 9th edition.
8) LactMed@ NIH
9) Smith's recognizable patterns of human malformation. 7th ed. Philadelphia: W.B.
Saunders Company, 2013.
10) Klaus Marshall H, Fanaroff Avroy A. Care of the High Risk Neonate, 6th ed. Philadelphia: W.B. Saunders Company, 2013.
11) Anderson RH, Baker EJ, Penny D, Redington AN, Rigby ML, Wernovsky G. Churchill Livingston. Pediatric Cardiology. 2010.
12) Kleinman CS and Seri I. Hemodynamics and Cardiology, 2012.
13) Remington J, Klein J. Infectious disease of the fetus and newborn infant. 8th ed. Philadelphia: W.B. Saunders Company, 2016.
14) De Alarcon P, Werner E, Christensen RD. Neonatal Hematology : Pathogenesis, Diagnosis, and Management of Hematologic Problems, 2013.
15) Thompson & Thompson Genetics in Medicine, 8th Edition, 2016.
16) Coran AG, Adzick NS, Laberge J-M, Shamberger RC, Caldamone AC. Pediatric Surgery, 7th ed, 2012.
17) Polin R, Abman S. Fetal and neonatal physiology. Vol 1 and 2. Philadelphia: W.B. Saunders Company, 4th ed. 2011.
We hope that this document may be a useful outline of the NICU residency rotation program. If you have questions or concerns, please do not hesitate to discuss them with the NICU staff or rotation coordinator. Best wishes for your NICU rotation! ©Thérèse Perreault MD, Revised August 2016
20

Section 1: Recommendations for Admission notes in NICU Following is a proposed template for admission notes in NICU. 1. ID Name, Birth date and time, Gestational age, Place of birth 2. Reason for admission 3. Maternal history Maternal age, G P A PMH & Chronic medical problems Past obstetrical history: Abortions, Previous fetal or neonatal death, including etiologies Relevant family history 4. Pregnancy LMP, Prenatal care Complications: Premature labor, Illnesses, Sick contacts, Interventions Ultrasounds & Fetal monitoring, Fetal movements, Amniotic fluid Medications, alcohol, tobacco, illicit drugs, other Serologies (HIV, Rubella, VDRL, etc…) and GBS screen (date) 5. Labor and Delivery Length of labor, Rupture of membranes incl. # hours, AF clear vs. meconium stained Presentation & Mode of delivery: Vaginal (forceps, vacuum?) or C/S (elective vs. emergency) Complications: Maternal and/or Fetal Resuscitation: O2, B+M, Intubation, Chest compressions, Drugs? Birth weight, Length & Head circumference, Apgar scores, Cord pH Vit K and ophthalmic prophylaxis 6. Course prior to MCH transfer History Treatment and Investigations
21

7. Physical exam General appearance (color, distress, posture): Current measurements: Weight / Length / Head circumference** + Plot on growth charts Vital signs: Tº / HR / RR / BP (4 limbs) Skin: Color, Rash, Birthmarks, Lesions Head & Neck: Head: Shape, Scalp, Anterior fontanelle, Sutures
Eyes: Appearance/position, Conjunctiva, Pupils, Red reflex** Ears and nose: Appearance/position, Ear canal (may be difficult to assess), Nares Mouth: Appearance/size, Gingiva, Palate, Tongue, Teeth/cysts Neck: Masses, Excess skin, Torticollis, thyroid, clavicles
Chest & cardiovascular exam: Appearance: breast buds, Shape, Retractions Lungs: Air entry, Symmetry, Adventitious sounds Heart: Precordium, Heart sounds, Murmur ( Quality, Location, Radiation)
Pulses** (brachial & femoral), Capillary refill Abdomen: Appearance, Umbilical cord ( Size, Vessels) Bowel sounds Palpation: Liver, Spleen, Kidneys, Masses Anus Genitalia: Male: Scrotum, Testes, Penis Female: Clitoris, Hymen Ambiguous MSK exam: Spine & Limbs Hips** Neurologic exam: Alertness & Activity Cranial nerves Tone and muscle strength Primitive reflexes: Suck, Grasp, Moro, Other Deep tendon reflexes & Clonus 8. Results Laboratory & Radiology tests 9. Assessment/Impressions Problem 1: “….” Problem 2: “….” Problem 3: “….” 10. Plan Monitoring & Investigations Treatment
Family support
22

Section 2: Recommendations for Discharge and Transfer Summaries in NICU The following elements should be part of a discharge summary or a transfer note from NICU:
• Brief maternal history • Relevant perinatal and delivery history • Initial status and reason for transfer to MCH • Evolution of major medical issues • Physical examination on discharge/transfer • Major tests’ results e.g. cardiac echo, cerebral imaging, special metabolic tests, etc. • Detailed plan of follow up, including different appointments in subspecialties (name of
Doctor) • Detailed discharge medication (per Kg) • Pending results of lab tests and who is responsible to follow these results
For a transfer on another ward within the Montreal Children’s Hospital, the transfer summary should be identified or entitled “NICU Transfer Summary”. It is recommended that the D/C summary is ready to be given to parents at the time of discharge, along with a consultation form for the primary pediatrician or MD. It is advisable to communicate directly with the primary MD who will be in charge of the F/U of the patient, particularly for patients with complex pathologies or with a prolonged hospitalization.
23

PATIENT LEAVING NICU OFF SERVICE
To other Home or other End of the Block departments hospitals
Transfer summary Discharge summary OFF service note
You must be logged on to NOVEL NETWORK in order to access the templates. Access as follows: Username: glenb06s Password: glenb06s Global-Share (H) drive – Public – glenb06s and choose the year “2016” • DO NOT WRITE DIRECTLY ON ANY OF THE TEMPLATES • DO NOT SAVE DOCUMENT UNDER PATIENT’S NAME • SAVE ONLY UNDER PATIENT’S UNIT NUMBER • SAVE ONLY IN THE FOLDER: 2016
NEVER SAVE ANY DOCUMENT ON THE DESKTOP OR IN FOLDER “MY DOCUMENT”
Informed consent concerning blood product transfusion
1. Information on: • Prescribed blood product, • Benefits, • Risks (see other side), • Alternatives (if necessary).
2. Answers to questions 3. Consent or refusal of the patient or authorized
representative 4. Documentation in the medical chart
Alternatives to blood transfusion
• Autologous blood transfusion • Normovolemic hemodilution • Cell recovery • Surgical technique reducing bleeding • Volume expanders (ex: Ringer Lactate, Saline,
Dextran, etc.) • Hemostatic agents (ex: aprotinin, coagulation factors,
etc.) • Therapeutic agents for (ex.: iron, folic acid, vitamin
B12, erythropoietin, etc.) This information was drawn from the document “Consentement à la transfusion de produits sanguins, Guide destiné aux médecins”, published by “le Ministère de la Santé et des Services sociaux du Québec”. (unofficial translation)
Québec


Risks associated with blood product transfusion
Global risk (excluding viral infections)
Frequencies
Benign reactions 1 out of 200 packed red blood cells 1 out of 10 pools of platelets Life threatening reactions 1 out of 6,500 products (1) Death 1 out of 128,000 products Severe to fatal reaction Frequencies Major allergic reaction 1 out of 4,000 units of plasma 1 out of 1,600 packed red blood cells Volume overload 1 out of 4,000 products Bacterial contamination 1 out of 3,000 pools of platelets 1 out of 24,000 packed red blood cells Acute hemolytic reaction 1 out of 14,000 packed red blood cells Delayed hemolytic reaction 1 out of 9,000 packed red blood cells Transfusion-related lung injury (TRALI)
1 out of 13,000 pools of platelets
Usually benign reactions Frequencies Febrile non-hemolytic reaction 1 out of 500 products Minor allergic reaction 1 out of 200 pools of platelets Viral infections Residual risk Human immunodeficiency virus (HIV)
1 out of 5 million products
Hepatitis C virus 1 out of 1.2 million products Hepatitis B virus 1 out of 275 000 products (2) Human T-cell leukemia virus (HTLV)
1 out of 5.5 million products
West Nil virus Impossible to determine in 2004 because of the absence of human cases
Other viruses (Hepatitis A virus, Parvovirus B-19, CMV, EBV)
Low
Other diseases Risks Malaria 1 on 4 million products Creutzfeldt-Jakob disease (CJD) Theory Variant of CJD (vCJD) Low
1. When the blood product is not specified, they are packed red blood cells, pools of platelets or units of plasma.
2. The risk of developing a chronic infection is lower than 1 on 2.75 million products.
Santé et Services sociaux
Québec

28

29