
GASTROINTESTINAL LYMPHOMAS Boudová, Fakan, Mukenšnabl, Daum Vaněček, Šíma, Němcová, Michal...
42
GASTROINTESTINAL LYMPHOMAS Boudová, Fakan, Mukenšnabl, Daum Vaněček, Šíma, Němcová, Michal
-
Upload
archibald-morgan -
Category
Documents
-
view
215 -
download
0
Transcript of GASTROINTESTINAL LYMPHOMAS Boudová, Fakan, Mukenšnabl, Daum Vaněček, Šíma, Němcová, Michal...
GASTROINTESTINAL
LYMPHOMAS
Boudová, Fakan, Mukenšnabl, Daum
Vaněček, Šíma, Němcová, Michal
PLZEŇ

Primary GI lymphomas
Most common extranodal lymphomas
Heterogeneous
Extranodal lymphomas: 1/3 of all lymphomas
GIT, skin; CNS, testis, bone, soft tissue salivary glands, thyroid, Waldeyer ring, lung kidney, liver, spleen, female genital tract

GI lymphomasType B
DLBCL, MALT
MCL, FL T
EATLSite Stomach Intestines (ileocaec., jejunum, duodenum)

MALT lymphoma
stomach, intestine (IPSID)
chronic antigenic stimulation
- Helicobacter pylori
Regulation: specific activated T-cells
Slow progression- 90%: stage IE, IIE
(bone marrow involvement: rare, 10%)

MALT lymphoma
Different sites
common features
ArchitectureCytologyImmunophenotype

MALT lymphomamonocytoid B-cells
(centrocyte-like, small lymphocytes) plasma cells, Dutcher bodies

MALT lymphomaLEL
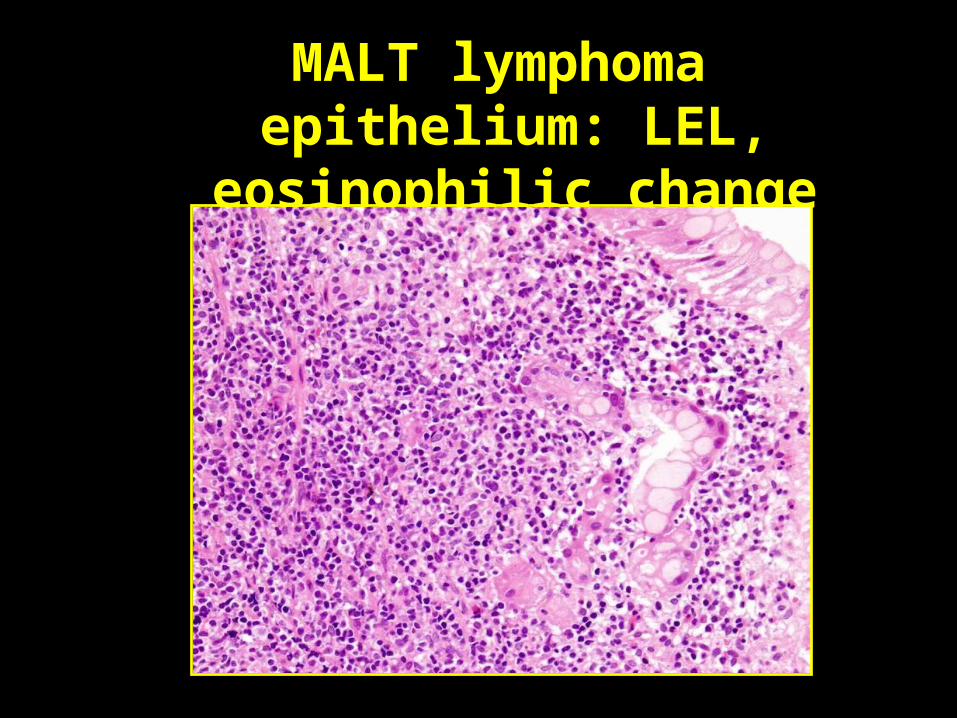
MALT lymphoma epithelium: LEL, eosinophilic change

MALT lymphoma - LEL (CD20)

MALT lymphoma
Immunohistochemistry
No specific MALT lymphoma markerPositivity: CD20, CD79a; Ig light chains; Ig
heavy chains: IgM; CD43Negativity: CD5, CD10, bcl6, IgD, cyclin D1
CD21, CD10, Ki-67: residual lymphoid follicles

MALT lymphoma
diagnostic problems
Large blasts (< 10%)
Follicular colonization
B-cell monoclonality

MALT lymphoma - diagnostic problemsLarge blasts (< 10%)
Ki-67

MALT lymphoma - diagnostic problemsFollicular colonization
Bacon J Clin Path 06

MALT lymphoma
Differential diagnosis
HP gastritis
other lymphomas: DLBCL, MCL, FL…
Integrated approachfavoring MALT lymphoma:dense lymphoid infiltrate prominent LELDutcher bodiesinfiltration of muscularis mucosaeatypia of lymphoid cellsB - cell monoclonality

MALT lymphoma

Macroscopy: often noncharacteristic
Microscopy: Wotherspoon criteria - spectrum
0 normal mucosa
1 chronic active gastritis
2 chronic active gastritis with lymphoid follicles
3 suspicious lymphoid infiltrate,
probably reactive
4 suspicious lymphoid infiltrate,
probably lymphoma
5 MALT lymphoma

B-cell monoclonality detection
Imunohistochemistry
Ig light chainsMolecular biology
PCR
IgH rearrangement
CDR III

B-cell monoclonality detection
Monoclonal IgH rearrangement
Polyclonal IgH rearrangement

It is often not possible to establish a clear diagnosis in a single biopsy.
repeat the biopsy; sampling
MALT lymphoma/gastritis?
Large cell component?

Correct diagnosis and treatment
• Interdisciplinary communication
• Repeated biopsies
• Specialized methods

MALT lymphoma after therapy
• Response: regression of lymphoid infiltrate and LEL
• Gastric mucosa: atrophy, intestinal metaplasia, empty, fibrotic, basal lymphoid aggregates
• Always assess Helicobacter pylori
• B-cell clonality assessment by PCR: not clear

Gastric MALT lymphomaRecurrent genetic abnormalities
• t(11;18)(q21;q21)/ API2-MALT1
usually the sole genetic abnormality, 25% of g. MALT l., H. p. neg., no response to ATB
• t(14;18)(q32;q21)/ IgH-MALT1
non-gastric
• t(1;14)(p22;q32)/ IgH-BCL10; t(1;2)(p22;p12)

MALT lymphoma versus DLBCL
Gastric DLBCL de novotransformation of a low-grade lymphoma
clonal progression in timeIndependent coexistence of 2 clones:
low /high grade component
DO NOT USE “HIGH-GRADE MALT LYMPHOMA“

Diffuse large B-cell lymphoma of the stomach
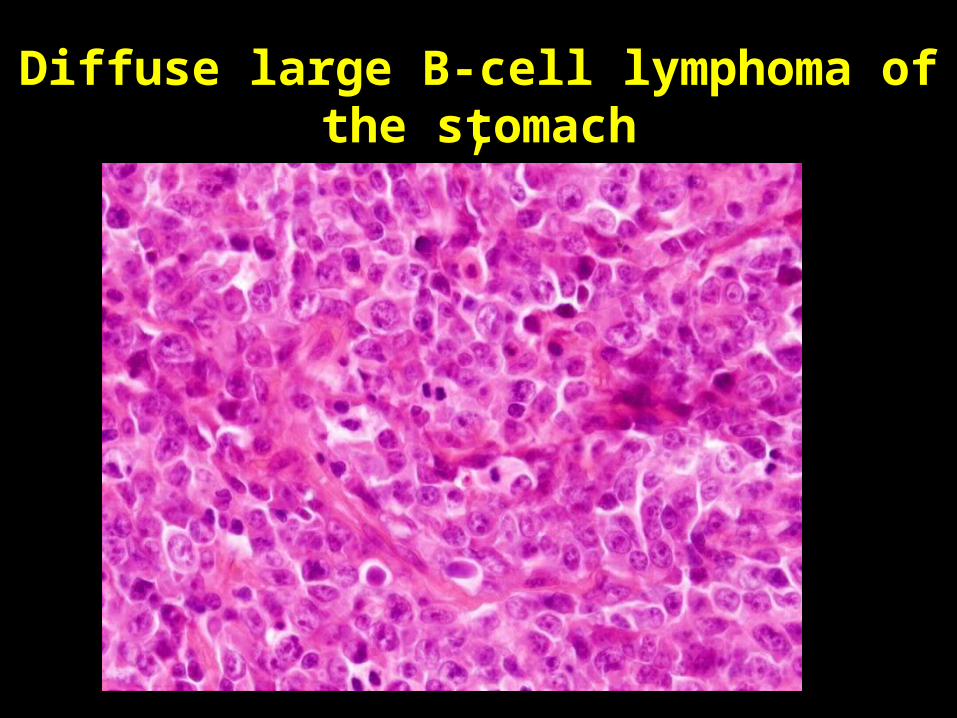
;Diffuse large B-cell lymphoma of the stomach

Multiple lymphomatous polyposis
Mantle cell lymphoma
Follicular lymphoma
MALT lymphoma

Mantle cell lymphoma
Multiple lymphomatous polyposis
M60 bad prognosis imunohistochemistry genetics WHO 2001

Mantle cell lymphoma

Mantle cell lymphoma
CD5 Cyclin D1
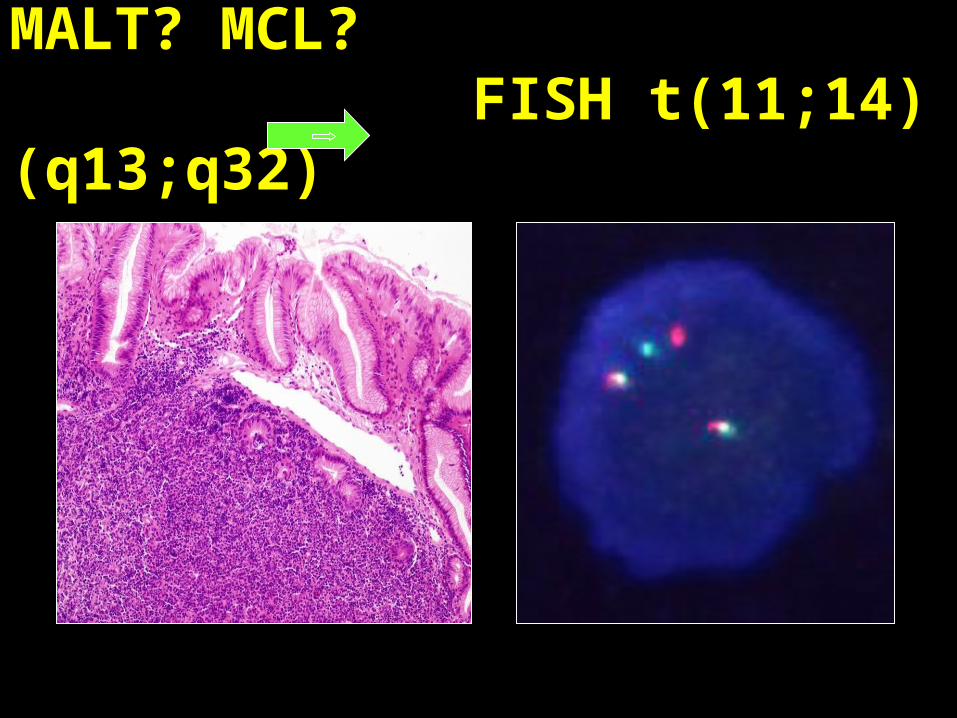
MALT? MCL? FISH t(11;14)(q13;q32)

Lymphomatous polyposis:follicular lymphoma g. 1 of the colon
M, 55, 2 polyps; stage IE, no therap, no disease 3 ys after the diagnosis
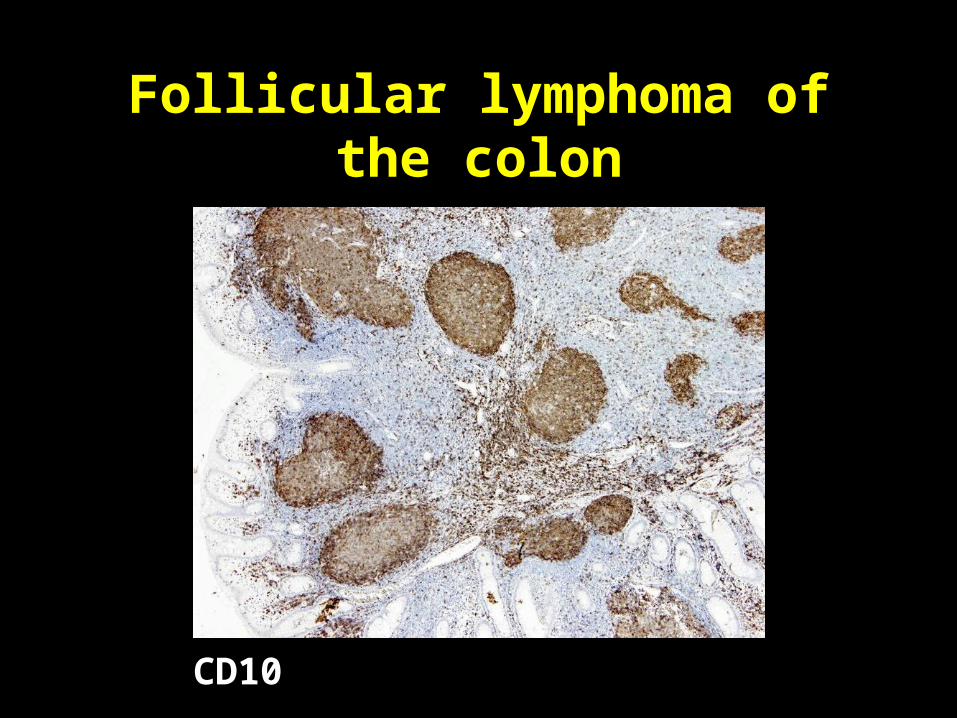
Follicular lymphoma of the colon
CD10
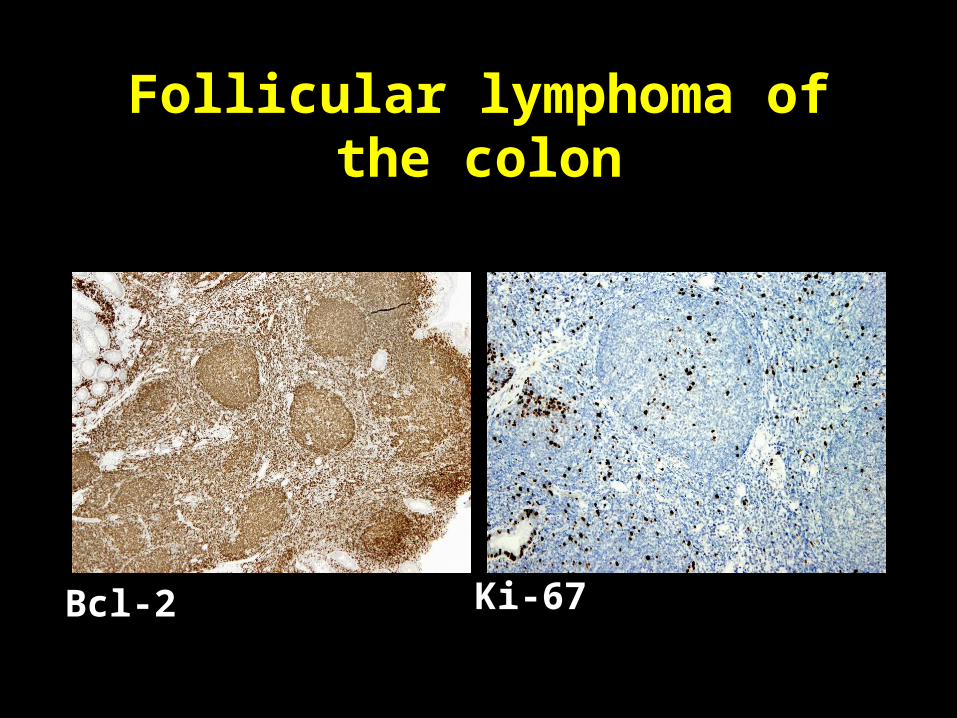
Follicular lymphoma of the colon
Bcl-2 Ki-67

F, 53-ys,“ileocaecal carcinoma“
follicular lymphoma stage IV, 7x CHOP; no disease detected 4 ys after the diagnosis
Bcl-2ileum
appendix
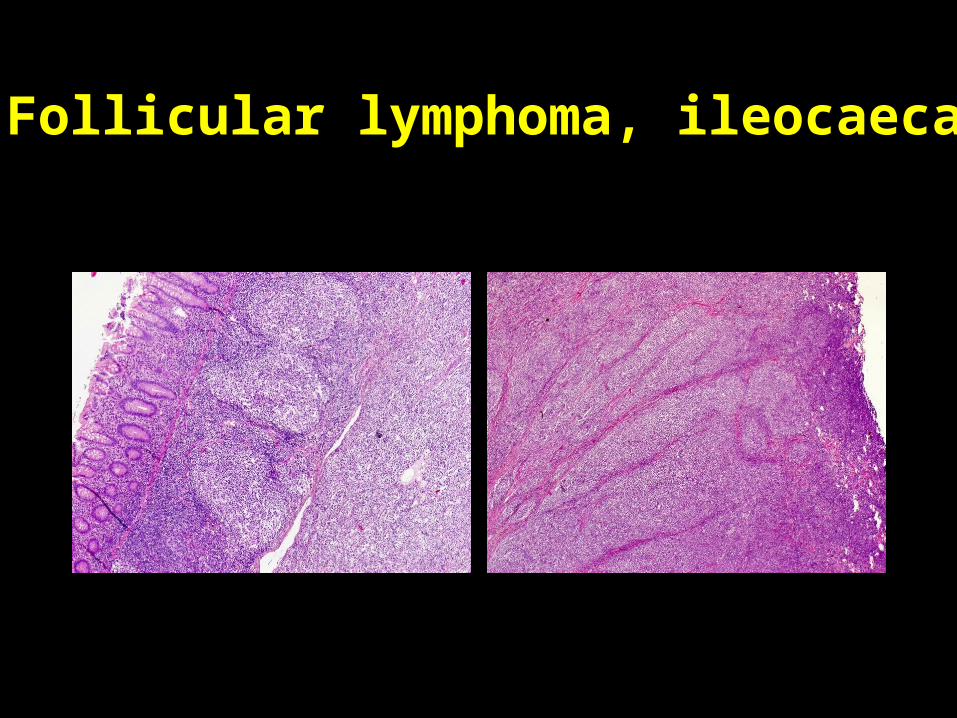
Follicular lymphoma, ileocaecal

Enteropathy-associated T-cell lymphoma
Proximal jejunum Very rare x most common GI T-cell lymphoma
Acute abdomen (40%) – emergency surgeryObstruction/perforation, peritonitis, sepsis, death
Non-acute: pain, weight loss, malabsorption
Age 60, M=F

Enteropathy-associated T-cell lymphoma
Multifocal ulcers

Enteropathy-associated T-cell lymphoma
Striking association with celiac disease
Histology and immunomorphology
Anaplastic/pleomorphic (80%)
Cel.+, enteropathy +, CD56-Monomorphic (20%)
Cel.-, enteropathy+/-, CD56+
Half of the patients die soon after the manifestation

Enteropathy-associated T-cell lymphoma
Anaplastic/pleomorphic
T-cells, plasma cells, eosinophils

Enteropathy-associated T-cell lymphoma
CD8 CD3

TCR gamma - PCR
TGGE
ABI PRISM
Enteropathy assoc. T-cell lymphoma
CGH marker: 9q gain (70%; Zettl 2007)

Molecular-genetic laboratoryDept. of Pathol., Plzeň, Czech Republic
















