GASTROINTESTINAL BLEEDING · gastrointestinal (GI) conditions and certain hepatobiliary and...
20
DOI 10.2310/7800.2064 12/12 gastrointestinal tract and abdomen GASTROINTESTINAL BLEEDING Ezra N. Teitelbaum, MD, and Eric S. Hungness, MD, FACS Despite recent advances in therapeutic endoscopy and the widespread use of antisecretory medications, upper gastrointestinal bleeding (UGIB), defined as bleeding that occurs proximal to the ligament of Treitz, continues to be one of the more common reasons for surgical consultation. It also remains a significant source of mortality for both emergency admissions (11%) and inpatients (33%). 1 The most common causes of UGIB are esophageal and gastric varices, Mallory-Weiss tears, acute hemorrhagic gastritis, gastric and duodenal ulcers, and neoplasms. 1 Less common causes include various other gastrointestinal (GI) conditions and certain hepatobiliary and pancreatic disorders. Lower gastrointestinal bleeding (LGIB), defined as abnor- mal hemorrhage into the lumen of the bowel from a source distal to the ligament of Treitz, usually derives from the colon; however, the small bowel is identified as the source of bleeding in as many as one third of cases. 2 In as many as 11% of patients presenting with hematochezia, brisk UGIB is identified as the source. 3 The most common causes of LGIB are colonic, with diverticular disease being the most common and accounting for 30 to 40% of all cases. 4 Arterio- venous malformations (AVMs), although extensively described in the literature, are considerably less common causes, accounting for 1 to 4% of cases. 5 Other less common causes include inflammatory bowel disease (IBD), benign and malignant neoplasms, ischemia, infectious colitis, benign anorectal disease, coagulopathy, use of nonsteroidal antiinflammatory drugs (NSAIDs), radiation proctitis, AIDS, and small bowel disorders. Presentation and Initial Management Gastrointestinal bleed- ing (GIB) may present as severe bleeding with hematemesis (UGIB), hema- tochezia (UGIB or LGIB), and/or symptoms of hy- potension or severe anemia (syncope, light-headedness, dyspnea, chest pain). UGIB may be gradual, presenting with melena, or occult, presenting with symptoms of chron- ic anemia (fatigue, dyspnea). The initial steps in the evalua- tion of patients with GIB are based on the perceived rate of bleeding and the degree of hemodynamic stability. Hemodynamically stable patients who show no evidence of active bleeding or comorbidities may be treated on an outpatient basis, 6 whereas patients who show evidence Financial disclosure information is located at the end of this chapter before the references. of serious bleeding should be managed aggressively and hospitalized. In the acute setting, the airway, breathing, and circulation should be rapidly assessed, and the examiner should note whether the patient has a history of or currently exhibits hematemesis, melena, or hematochezia. Blood should be sent to the blood bank for typing/crossmatching, complete blood count, blood chemistries (including tests of liver func- tion and renal function), and measurement of the prothrom- bin time and the partial thromboplastin time. If UGIB is suspected, the patient should be given an intravenous (IV) proton pump inhibitor (PPI) empirically (e.g., omeprazole 80 mg bolus dose followed by a 8 mg/hr continuous infu- sion in high-risk patients) as preendoscopy PPI administra- tion has been shown to decrease the need for endoscopic therapy for bleeding peptic ulcers. 7,8 If the patient is stable and shows no evidence of recent or active hemorrhage, the surgeon may proceed with the work- up. If the patient is unstable or shows evidence of recent or active bleeding, short, large-bore IV lines should be placed before the workup is begun to ensure that immediate IV access is possible should the patient subsequently become unstable. He or she should be taken to an intensive care unit and resuscitated immediately. Resuscitation of an unstable patient is begun by establishing a secure airway and ensur- ing adequate ventilation. 9 Oxygen should be given, with a low threshold for endotracheal intubation. Much as in trauma resuscitation, either short, large-bore, peripheral IV lines or a single-lumen 8 French catheter in the femoral vein should then be placed, through which lactated Ringer solution or 0.9% normal saline should be infused at a rate high enough to maintain tissue perfusion. A urinary catheter should be inserted and urine output monitored. Blood prod- ucts should be given as necessary, and any coagulopathies should be corrected. Transfusion should aim at maintaining both a hemoglobin level of 7 g/dL or greater and adequate end-organ perfusion (as measured by urine output, mental status, etc.). It is all too easy to forget these basic steps in a desire to evaluate and manage massive GI hemorrhage. Every effort should be made to resuscitate and stabilize the patient sufficiently to allow clinical evaluation and diag- nostic testing to help determine the cause of the bleeding and direct subsequent care. Only if the patient remains unstable and continues to bleed despite maximal supportive measures should he or she be taken to the operating room (OR) for intraoperative diagnosis. Clinical Evaluation Only after the initial measures to protect the airway and stabilize the patient have been completed should an attempt be made to establish the cause of the bleeding. The history should focus on known causes of GIB (e.g., previous GIB, peptic ulcer disease, diverticulosis, AVM, esophageal vari- ces, liver disease, alcohol abuse, and IBD) and on the possi- ble use of medications that interfere with coagulation (e.g., © 2012 Decker Intellectual Properties Scientific American Surgery
Transcript of GASTROINTESTINAL BLEEDING · gastrointestinal (GI) conditions and certain hepatobiliary and...

DOI 10.2310/7800.2064
12/12
gastrointestinal tract and abdomen
G A S T R O I N T E S T I N A L B L E E D I N G
Ezra N. Teitelbaum, MD, and Eric S. Hungness, MD, FACS
Despite recent advances in therapeutic endoscopy and the widespread use of antisecretory medications, upper gastrointestinal bleeding (UGIB), defi ned as bleeding that occurs proximal to the ligament of Treitz, continues to be one of the more common reasons for surgical consultation. It also remains a signifi cant source of mortality for both emergency admissions (11%) and inpatients (33%).1 The most common causes of UGIB are esophageal and gastric varices, Mallory-Weiss tears, acute hemorrhagic gastritis, gastric and duodenal ulcers, and neoplasms.1 Less common causes include various other gastrointestinal (GI) conditions and certain hepatobiliary and pancreatic disorders.
Lower gastrointestinal bleeding (LGIB), defi ned as abnor-mal hemorrhage into the lumen of the bowel from a source distal to the ligament of Treitz, usually derives from the colon; however, the small bowel is identifi ed as the source of bleeding in as many as one third of cases.2 In as many as 11% of patients presenting with hematochezia, brisk UGIB is identifi ed as the source.3 The most common causes of LGIB are colonic, with diverticular disease being the most common and accounting for 30 to 40% of all cases.4 Arterio-venous malformations (AVMs), although extensively described in the literature, are considerably less common causes, accounting for 1 to 4% of cases.5 Other less common causes include infl ammatory bowel disease (IBD), benign and malignant neoplasms, ischemia, infectious colitis, benign anorectal disease, coagulopathy, use of nonsteroidal antiinfl ammatory drugs (NSAIDs), radiation proctitis, AIDS, and small bowel disorders.
Presentation and Initial Management
Gastrointestinal bleed-ing (GIB) may present as severe bleeding with hematemesis (UGIB), hema-tochezia (UGIB or LGIB), and/or symptoms of hy-potension or severe anemia (syncope, light-headedness, dyspnea, chest pain). UGIB may be gradual, presenting with melena, or occult, presenting with symptoms of chron-ic anemia (fatigue, dyspnea). The initial steps in the evalua-tion of patients with GIB are based on the perceived rate of bleeding and the degree of hemodynamic stability. Hemodynamically stable patients who show no evidence of active bleeding or comorbidities may be treated on an outpatient basis,6 whereas patients who show evidence
Financial disclosure information is located at the end of this chapter before the references.
of serious bleeding should be managed aggressively and hospitalized.
In the acute setting, the airway, breathing, and circulation should be rapidly assessed, and the examiner should note whether the patient has a history of or currently exhibits hematemesis, melena, or hematochezia. Blood should be sent to the blood bank for typing/crossmatching, complete blood count, blood chemistries (including tests of liver func-tion and renal function), and measurement of the prothrom-bin time and the partial thromboplastin time. If UGIB is suspected, the patient should be given an intravenous (IV) proton pump inhibitor (PPI) empirically (e.g., omeprazole 80 mg bolus dose followed by a 8 mg/hr continuous infu-sion in high-risk patients) as preendoscopy PPI administra-tion has been shown to decrease the need for endoscopic therapy for bleeding peptic ulcers.7,8
If the patient is stable and shows no evidence of recent or active hemorrhage, the surgeon may proceed with the work-up. If the patient is unstable or shows evidence of recent or active bleeding, short, large-bore IV lines should be placed before the workup is begun to ensure that immediate IV access is possible should the patient subsequently become unstable. He or she should be taken to an intensive care unit and resuscitated immediately. Resuscitation of an unstable patient is begun by establishing a secure airway and ensur-ing adequate ventilation.9 Oxygen should be given, with a low threshold for endotracheal intubation. Much as in trauma resuscitation, either short, large-bore, peripheral IV lines or a single-lumen 8 French catheter in the femoral vein should then be placed, through which lactated Ringer solution or 0.9% normal saline should be infused at a rate high enough to maintain tissue perfusion. A urinary catheter should be inserted and urine output monitored. Blood prod-ucts should be given as necessary, and any coagulopathies should be corrected. Transfusion should aim at maintaining both a hemoglobin level of 7 g/dL or greater and adequate end-organ perfusion (as measured by urine output, mental status, etc.). It is all too easy to forget these basic steps in a desire to evaluate and manage massive GI hemorrhage.
Every effort should be made to resuscitate and stabilize the patient suffi ciently to allow clinical evaluation and diag-nostic testing to help determine the cause of the bleeding and direct subsequent care. Only if the patient remains unstable and continues to bleed despite maximal supportive measures should he or she be taken to the operating room (OR) for intraoperative diagnosis.
Clinical Evaluation
Only after the initial measures to protect the airway and stabilize the patient have been completed should an attempt be made to establish the cause of the bleeding. The history should focus on known causes of GIB (e.g., previous GIB, peptic ulcer disease, diverticulosis, AVM, esophageal vari-ces, liver disease, alcohol abuse, and IBD) and on the possi-ble use of medications that interfere with coagulation (e.g.,
© 2012 Decker Intellectual PropertiesScientific American Surgery

12/12
gastro gastrointestinal bleeding — 2
Assessment and Management ofGastrointestinal Bleeding
Perform initial assessment and management
Patient presents with GI bleeding
Manage UGIB source
Gastric neoplasm
Evaluate airway, breathing, and circulation.
Look for past or current hematemesis, melena,or hematochezia.
Draw blood for CBC, blood chemistries,measurement of PT and PTT, and typing andcrossmatching.
Acute hemorrhagic gastritis
Stop NSAIDs.Give H2 receptor blockers, omeprazole, sucralfate, or antacids. Give anti–Helicobacter pylori therapy. If bleeding stops: observe.If bleeding continues: consider IV somatostatin (250 µg bolus, then 250 µg/hr) or intra-arterial vasopressin (10 U/hr). If this step is effective, observe; if not, perform total or near-total gastrectomy [search for
astric and uodenal isease].
Patient is stable
Proceed with workup.
If active bleeding is present:insert large-bore IV linebefore workup.
Patient stabilizes
Proceed with workup.
Duodenal ulcer
[See Figure 1.]
Gastric ulcer
[See Figure 1.] Gastricvarices
[See Figure 4.]
Esophagealvarices
[See Figure 4.]
Patient remains unstable
Proceed to OR forintraoperative diagnosisand management.
Lesion is benign
Perform wedgeexcision of lesion.
Lesion is malignant
Attempt endoscopiccontrol of bleeding.
If bleeding stops:excise lesion electively.
If bleeding continues:excise resectable lesionspromptly; nonresectablelesions call for anonoperative approach.
Patient is unstable
Give oxygen by mask or byET tube and ventilator.
Insert large-bore IV line, and infuse lactated Ringersolution.
Insert urinary catheter, andmonitor urine output.
Give blood as needed.
Correct any coagulopathies.
Mallory-Weiss tear
Lesion usually stopsbleeding without therapy.If it does not, controlbleeding endoscopically.
If bleeding stops:observe.
If bleeding continues:perform anteriorgastrotomy with directsuture ligation of tear.
the publicationprocedures for benign and malignant g d d
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 3
Hiatal hernia
Manage LGIB source[See Figure 5.]
Occult bleeding source
Perform capsule endoscopyPerform double balloon enteroscopy.
Paraesophageal hernia(type II–IV hiatal hernia)
Sliding hernia (type I hiatal hernia)
Repair surgically (eithervia open laparotomy orvia minimally invasiveapproach) [search
for open
and minimally invasive sophageal rocedures].
Duodenal diverticula
Excise lesion, with or without the aid of intraoperativeendoscopy.
Give PPI and, if applicable, anti–H. pylori therapy.
If bleeding stops: continue medical therapy.
If bleeding continues: perform Nissen fundoplication [search the publication for open esophageal procedures and minimally invasive esophageal procedures].
Hemobilia
Perform arteriographicembolization of affectedportion of liver.
Other options are hepaticartery ligation and hepaticresection.
Dieulafoy lesion
Attempt endoscopiccontrol. Mark site withIndia ink.
If bleeding stops: observe.
If bleeding continues:ligate or excise vessel.
Aortoenteric fistula
Resect aortic graft.
Close enteric site offistula.
Place extra-anatomicor in situ arterial graft.
Vascular ectasias
Attempt endoscopic control of bleeding.Consider IV somatostatin (250 μg bolus, then 250 μg/hr).
If bleeding stops: observe.
If bleeding continues: resect lesion.
Hemosuccus pancreaticus
Perform distal pancreatectomy[search the publication for
isease], including excision of pseudocyst and ligation of bleeding vessel.
Work up patient
Obtain history, focusing on known causes ofGI bleeding and suspect medications.
Perform physical examination.
Perform NG aspiration.
Perform esophagogastroduodenoscopy and/orcolonoscopy [search for
astrointestinal ndoscopy].
Use other tests as appropriate:• tagged red cell scans• arteriography• intraoperative endoscopic exploration
the publicationg e
procedures for benign and malignant pancreatic d
thepublication esophageal procedures
e p
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 4
warfarin, aspirin, clopidogrel, dabigatran, and NSAIDs) or alter hemodynamics (e.g., beta blockers and antihyperten-sive agents). Of particular importance in taking the history is to ascertain the nature and duration of the bleeding, including stool color, frequency, and volume. The patient should also be asked about any associated symptoms of potential signifi cance (e.g., abdominal pain, changes in bowe l habits, fever, urgency, tenesmus, or weight loss). Knowledge of the patient’s cardiac history is useful to assess the patient’s ability to withstand varying degrees of anemia.
The physical examination is seldom of much help in determining the exact site of bleeding, but determination of postural vital signs can accurately estimate intravascular volume status. A drop in the orthostatic blood pressure greater than 10 mm Hg or an increase in the pulse rate greate r than 10 beats/min indicates that more than 800 mL of blood (> 15% of the total circulating blood volume) has been lost. Marked tachycardia and tachypnea in association with hypotension and depressed mental status indicate that more than 1,500 mL of blood (> 30% of the total circulating blood volume) has been lost. A complete abdominal exami-nation, including digital rectal examination and anoscopy, should be performed as it may reveal jaundice, ascites, or other signs of hepatic disease; a tumor mass; or a bruit from an abdominal vascular lesion.
A nasogastric (NG) tube should be placed for gastric lavage. If lavage yields positive results (i.e., the aspirate contains gross blood or so-called coffee grounds), UGIB is confi rmed and esophagogastroduodenoscopy (EGD) is indi-cated. An aspirate that contains no blood and copious amounts of bile is strongly suggestive of LGIB, and the workup proceeds accordingly. The choice is less clear-cut with a clear aspirate. In the absence of bile, such an aspirate cannot rule out a duodenal source for the bleeding. Accord-ingly, there is some degree of latitude for clinical judgment: depending on the overall clinical picture, the surgeon may choose either to perform EGD to rule out a duodenal bleed-ing source or to proceed with colonoscopy on the assump-tion that the source of the bleeding is in the lower GI tract.
Several clinical prediction scores have been developed to risk-stratify patients presenting with UGIB and can help guide the sequence of diagnostic tests and subsequent man-agement. The two most commonly used are the Blatchford score10 and the Rockall score.11 The Blatchford score predicts the need for clinical intervention (blood transfusion, endo-scopic, or operative treatment) based on clinical variables obtained on presentation (blood urea, hemoglobin, pulse, blood pressure, presenting symptoms, and comorbidities) [see Table 1]. It has an area under the receiver operating char-acteristic (ROC) curve of 0.92 and a sensitivity of 99% (for a score ≥ 1), so it is best used as an initial screening tool to alert emergency department personnel of patients who may have serious UGIB and therefore need more urgent diagnostic evaluation. The Rockall score incorporates clinical and EGD fi ndings (age, level of shock, comorbidities, endoscopic diagnosis, and the presence of stigmata of recent hemor-rhage) to predict hospital mortality and the risk of rebleed-ing [see Table 2]. As such, it is used after the initial EGD
evaluation and may help predict patients who will go on to need a surgical intervention.
Separate risk stratifi cation scores also exist for LGIB. Strate and colleagues developed and validated a prediction model based on the presence of seven clinical variables (heart rate ≥ 100 beats/min, systolic blood pressure ≤ 115 mm Hg, syncope, a nontender abdomen, rectal bleeding in the fi rst 4 hours of evaluation, aspirin use, and more than two medical comorbidities) to predict the risk of need for blood transfusion, surgical intervention, and mortality.12 In this study, patients with four of more of these risk factors were determined to be at high likelihood for severe bleeding, and therefore in general patients meeting this criterion should be triaged to receive emergent intervention.
UGIB Investigative Tests
esophagogastroduodenoscopy
EGD almost always reveals the source of UGIB; its utility and accuracy have been well document-ed in the literature.13 Per-formance of this procedure requires considerable skill: identifi cation of bleeding sites in a blood-fi lled stomach is far from easy. Hematemesis is an indication for emergency EGD, usually within 1 hour of presentation. If the rate of bleeding is high, saline lavage may be performed to clear the stomach of blood and clots. If the rate of bleeding is moderate or low, as is often the case in patients with melena, urgent EGD is indicated. In these cases, EGD should be performed within 24 hours of presen-tation, and several studies have shown that EGD within 12 hours results in shorter hospital stays and possibly decreased rates of rebleeding and mortality in high-risk patients.14–16 Erythromycin can be given prior to endoscopy to facilitate gastric emptying as pretreatment has been shown to decrease the need for multiple endoscopic evaluations.17
EGD is not only an excellent diagnostic tool but also a valuable therapeutic modality. Indeed, most UGIB may be controlled endoscopically, although the degree of success to be expected in individual cases varies according to the expertise of the endoscopist and the specifi c cause of the bleeding. Therapeutic endoscopic maneuvers include injection, thermal coagulation, and mechanical occlusion of bleeding sites (clip application or variceal banding). The choice of therapy depends on the cause, the site, and the rate of bleeding.
other ugib imaging
Tagged red blood cell (RBC) scans may confi rm the pres-ence of an active bleeding site; however, scans are fairly nonspecifi c with respect to determining the anatomic loca-tion of the bleeding.18 Arteriography may demonstrate that a lesion is present, but it cannot reliably identify a bleeding site unless the bleeding is brisk (> 1 mL/min). Occasionally, arteriography reveals the cause of the bleeding even if the bleeding has stopped. Angiography may also be considered a therapeutic modality for high-risk surgical patients. These tests, in conjunction with EGD, should allow the surgeon to establish the cause of UGIB more than 90% of the time.
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 5
colonoscopy
Several large series that evaluated the diagnostic utility of colonoscopy in patients with LGIB found this modality to be moderately to highly accurate, with overall diagnostic yields ranging from 53 to 97%.3,20,21 In studies reporting morbidity, colonoscopy was safe, with an average complication rate of 0.5%. Colonoscopy has both a higher diagnostic yield and a lower complication rate than arteriography in this setting.3,21 A randomized, controlled trial in 2005 demonstrated that early colonoscopy (< 8 hours from presentation) was better able to localize and identify the source of LGIB than stan-dard care (elective colonoscopy or radionuclide scanning followed by angiography in patients with ongoing bleed-ing).22 An argument has been made that colonoscopy should be considered the procedure of choice for structural evalua-tion of LGIB and that arteriography should be reserved for patients with massive, ongoing bleeding in whom endos-copy is not feasible or colonoscopy fails to reveal the source of the hemorrhage.23
As with EGD, early colonoscopy (within 12 hours) results in higher diagnostic yields and increased opportunity for endoscopic intervention. One study showed that a therapeu-tic intervention was successful in 29% of colonoscopies performed within 12 hours, 13% of those between 12 and 24 hours, 4% in those between 24 and 48 hours, and none
LGIB Investigative Tests
A number of diagnostic techniques are available for determining the source of LGIB, including colo-noscopy radionuclide scanning, computed tomo-graphy (CT), and angio-graphy (in the form of selective mesenteric arteriography), as well as enteroscopy and capsule endoscopy (CE) to localized small bowel etiolo-gies. The goal of these tests is to locate the site of bleeding accurately so that defi nitive therapy can be properly directe d as the potential source ranges from the ligament of Treitz to the anus. The diagnostic test chosen for a specifi c patient depends on several factors, including the hemodynamic sta-bility of the patient, the bleeding rate, patient comorbidities, therapeutic options, and local expertise available. Unlike radionuclide and CT scanning, arteriography and colonos-copy provide a therapeutic option. Arteriography has a lower diagnostic yield and a higher complication rate than colonoscopy does; therefore, it is reasonable to attempt colo-noscopy fi rst and to reserve angiography for patients in whom the volume of bleeding is such that colonoscopy would be neither safe nor accurate.19
Table 1 Blatchford Prediction Score for Upper Gastrointestinal Bleeding10
Score
Variable 0 1 2 3 4 6
Blood urea (mmol/L) < 6.5 6.5–8 8–10 10–25 > 25
Hemoglobin (g/dL) for men > 13 12–13 10–12 < 10
Hemoglobin for women > 12 10–12 < 10
Systolic BP > 109 100–109 90–99 < 90
Other markers Pulse ≥ 100 beats/min, presentation with melena
Presentation with syncope, hepatic disease, cardiac failure
BP = blood pressure.
Table 2 Rockall Prediction Score for Upper Gastrointestinal Bleeding11
Score
Variable 0 1 2 3
Age (yr) < 60 60–79 ≥ 80
Shock Systolic BP ≥ 100 mm Hg and pulse < 100 beats/min
Systolic BP ≥ 100 mm Hg and pulse ≥ 100 beats/min
Systolic BP < 100 mm Hg
Comorbidites No major comorbidities Heart failure, ischemic heart disease, other major comorbidity
Renal failure, liver failure, metastatic cancer
Diagnosis Mallory-Weiss tear, no lesion identified, and no stigmata of recent hemorrhage
All other diagnoses Upper GI malignancy
Stigmata of recent hemorrhage
None or dark spot only Blood in upper GI tract, adherent clot, visible or spurting vessel
BP = blood pressure; GI = gastrointestinal.
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 6
performed later than 48 hours after presentation.24 The merits of colonic preparation have been extensively debated in the literature.3,25 Although no fi rm conclusion has been reached, adequate colonic preparation may improve both the diagnostic yield and the safety of colonoscopy. Given the absence of any defi nitive data suggesting that bowel prepa-ration either reactivates or increases bleeding, one should consider administering an oral bowel preparation after the patient has been adequately resuscitated.
If the entire colon has been adequately visualized and no source for the bleeding has been identifi ed, the ileum should be intubated; fresh blood in this region suggests a possible small bowel source. If no active bleeding is observed in the ileum, upper GI endoscopy should be performed to rule out a UGIB site.
When colonoscopy identifi es a bleeding source, endoscopi c treatment may be an option. Endoscopic modalities used to treat LGIB include use of thermal contact probes, laser photocoagulation, electrocauterization, injection of vasocon-strictors, application of metallic clips, and injection sclero-therapy. The choice of a specifi c modality often depends on the nature of the offending lesion and on the expertise and resources available locally. A 1995 survey of members of the American College of Gastroenterology found that endo-scopic therapy was used in 27% of patients presenting with LGIB.26
radionuclide scanning
Radionuclide scanning is highly sensitive for lower LGIB, capable of detecting bleeding at rates as slow as 0.1 to 0.4 mL/min.27 The patient’s RBCs are labeled with technetium-99m (99mTc), which can be detected on images as long as 24 to 48 hours after injection [see Figure 1]. The high sensitivity of 99mTc-labeled RBC scanning (80 to 98%) is well attested, but there is considerable disagreement in the literature with regard to its specifi city in identifying the anatomic site of bleeding.28,29 For example, a 1997 study found radiolabeled RBC scanning to be 97% accurate for localizing bleeding in 37 patients undergoing surgical resection,29 whereas a 1990 study reported a 42% rate of incorrect resection when surgi-cal therapy was based solely on this modality.28 In 2005, one group retrospectively reviewed 127 bleeding scans in an effort to identify factors that might predict a positive scan.30 The investigators found that tagged RBC scans were 48% accurate in localizing bleeding sites later confi rmed by endoscopy, surgery, or pathologic evaluation. Multivariate analysis demonstrated that both the number of units of blood transfused in the 24 hours preceding the scan and the lowest recorded hematocrit differed signifi cantly between patients with positive scans and those with negative scans. However, the clinical signifi cance of a positive scan was unclear in this study in that the rate of endoscopy was not signifi cantly different between patients who had positive scans and those who did not. For this reason, an anatomi-cally selective colon resection for LGIB should not be per-formed based on localization obtained through radionuclide scanning alone.
Given that radionuclide scanning has no therapeutic inter-vention capabilities, its best use is in patients with non–life-threatening LGIB as a prelude and a guide to mesenteric angiography after active hemorrhage has been confi rmed.
However, one should keep in mind that many intervention-al radiologists may be reluctant to perform an angiography without fi rst confi rming bleeding with a positive radionu-clide study.
Radionuclide scanning is also useful for diagnosing a Meckel diverticulum, a rare cause of LGIB. Patients are injected with 99mTc pertechnetate, which is taken up by the ectopic gastric mucosa. Although studies in the pediatric population have demonstrated high diagnostic accuracy, the sensitivity of the scan is only 60 to 70% in the adult population.31
mesenteric angiography
Selective mesenteric arteriography is somewhat less sensi-tive than radionuclide scanning for lower GI hemorrhage: bleeding must be occurring at a rate of at least 0.05 to 1 mL/min to be detectable with this test.32,33 The procedure involves percutaneous placement of a transfemoral arterial catheter for evaluation of the superior mesenteric, inferior mesenteric, and celiac arteries. A positive test result is defi ned as extravasation of contrast into the lumen of the bowel. The probability of a positive study increases with the severity of bleeding. A systolic blood pressure less than 90 mm Hg and the need for fi ve or more units of blood transfusion result in an 85% positive predictive value for bleeding localization.34
In several large series, the overall diagnostic yield of arte-riography ranged from 27 to 67%.16,29,35,36 The complication rate for arteriography performed for LGIB ranges from 2 to 4%.2,37 Reported complications include contrast allergy, renal failure due to contrast nephropathy, bleeding and/or pseudoaneurysm formation at the arterial puncture site, and embolism from a dislodged thrombus.23 Diagnostic use of angiography in patients with LGIB can often be followed by angiographic therapy. The two main angiographic treat-ment options are intra-arterial injection of vasopressin and transcatheter embolization.
Vasopressin acts to control bleeding by causing arteriolar vasoconstriction and bowel wall contraction. Once the bleed-ing site has been localized angiographically, the catheter is positioned in the main trunk of the vessel. Infusion of vasopressin is initiated at a rate of 0.2 U/min and can be increased to a rate of 0.4 U/min. Within 20 to 30 minutes, angiography is performed again to determine whether the bleeding has ceased. If the bleeding is under control, the catheter is left in place and vasopressin is continuously infused for 6 to 12 hours. If the bleeding continues to be controlled, infusion is continued for an additional 6 to 12 hours at 50% of the previous rate. Finally, vasopressin infusion is replaced by continuous saline infusion, and if bleeding does not recur, the catheter is removed.38
The vasoconstrictive action of vasopressin can have dele-terious systemic side effects, including myocardial ischemia, peripheral ischemia, hypertension, dysrhythmias, mesenteri c thrombosis, intestinal infarction, and death. Occasionally, simultaneous IV administration of nitroglycerin is necessary to counteract these systemic effects. The reported success rate of vasopressin in controlling LGIB ranges from 60 to 100%, and the incidence of major complications ranges from 10 to 20%.39-41 Rebleeding rates as high as 50% have been reported.39,40
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 7
Figure 1 An algorithm for management of bleeding from duodenal or gastric ulcers. OR = operating room; PPI = proton pump inhibitor.
Recently, transcatheter embolization has largely replaced vasopressin infusion due to the above-mentioned complica-tions and high rebleeding rates. In this technique, a catheter is superselectively placed into the identifi ed bleeding vessel and an embolizing agent (e.g., a gelatin sponge, a microcoil, polyvinyl alcohol particles, or a balloon) is injected. Several small series found this technique to be 90 to 100% successful at stopping bleeding.41-43 Equally impressive was the fi nding that the rebleeding rates in these series were 0%. The com-plication rates of this procedure are generally reasonable as well; however, intestinal infarction has been reported.44,45
The use of small microcatheters and the ability to super-selectively embolize individual vessels have reduced the potential for ischemic perforation. It is possible that as more experience is gained with these techniques, superselective embolization may entirely replace catheter-directed vaso-constrictive therapy, thus obviating the potential deleterious systemic effects of vasopressin administration. Some researchers have suggested that with the exception of cases
of diffuse bleeding lesions or cases whose demands exceed the technical limitations of superselective catheterization, embolization therapy should be the fi rst choice for angio-graphic treatment of LGIB.45,46
If embolization is not possible, once the bleeding vessel has been localized angiographically, the area must be marked so that it can be successfully identifi ed intraoperatively; this is commonly accomplished by infusing methylene blue into the bleeding artery or leaving a transfemoral catheter to the offending vessel in place [see Figure 2].37 In a minority of patients, obscure bleeding persists despite negative fi ndings from endoscopy, mesenteric arteriography, and radiolabeled RBC scanning. This obscure bleeding presents a consider-able diagnostic challenge, which some investigators have proposed addressing by means of so-called provocative angiography.47 Provocative angiography involves the use of short-acting anticoagulant agents (unfractionated heparin, vasodilators, thrombolytics, or combinations thereof) in association with angiography. Once the bleeding point has
Patient has bleeding from duodenalor gastric ulcer
Bleeding continues
Bleeding continues
Patient has duodenal ulcer Patient has gastric ulcer
Bleeding stops
Initiate medical management.• PPI infusionAttempt to control bleeding endoscopically.
Repeat attempt atendoscopic control.
Consider angiography and embolization.Proceed to OR for surgical treatment.
Perform duodenotomy andoversew ulcer.
Consider truncal vagotomy(if patient is unstable) orhighly selective vagotomy(if patient is stable).
Treat according to ulcer type.• Type I: wedge resection• Type II/III: antrectomy, Billroth I reconstruction, and vagotomy• Type IV: Csendes procedure or ligation of left gastric artery with oversewing of ulcer• Type V: as for acute hemorrhagic gastritis
Continue medical management.• PPI infusion• H. pylori therapy, if necessary
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 8
been localized (in up to 89% of cases in a recent study),48 superselective embolization can be attempted or methylene blue is injected and the patient is immediately brought to the OR for surgical treatment.
computed tomography
With the ongoing improvements in high-speed abdominal CT scanning, interest has been growing in the evaluation of GIB with CT angiography.49 Helical CT scanners can provide direct or indirect evidence of the source of GIB. Typical fi nd-ings that can facilitate localization of bleeding sites include spontaneous hyperdensity of the peribowel fat, contrast enhancement of the bowel wall, vascular extravasation of the contrast medium, thickening of the bowel wall, polyps, tumors, and vascular dilatation.
CT evaluation of GIB has several noteworthy advantages: the scanners typically are readily available, mobilization of special teams or units is not required, the scans can be completed rapidly in the emergency department, and bowel
preparation is unnecessary. In one experimental study, CT scanners were able to detect arterial bleeding at rates as low as 0.07 mL/min, which suggests that CT scanning is more sensitive than angiography for this purpose.50 In addition, CT scans are noninvasive and carry little morbidity. Unfor-tunately, like radionuclide scanning, CT has no therapeutic capability.
A 2003 study of 19 patients with GI hemorrhage compared triphasic helical CT evaluation with colonoscopy and sur-gery for localization of bleeding sites.50 In this series, fi ve patients had small bowel bleeding sites and 14 patients had colonic sites. Helical CT scanning correctly identifi ed four of the fi ve small bowel lesions and 11 of the 14 colonic lesions. A 2012 study of CT evaluation in 114 patients demonstrated a sensitivity of 80% in patients with severe bleeding and 64% in those with mild bleeding.51 Additionally, CT was able to identify both upper and lower sources of bleeding. This ability to rapidly distinguish between UGIB and LGIB may be of particular value in patients with severe hematochezia
Ampulla of Vater
Common Bile Duct
Pancreatic Duct
AnteriorPancreaticoduodenal
Artery
Gastroduodenal Artery
Proper Hepatic Artery
Common HepaticArtery
CeliacTrunk
Splenic Artery
Transverse Pancreatic Artery
Three-Point Ligation ofBleeding Duodenal Ulcer
Aorta
Stay Suture
Stay Suture
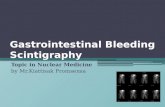
Figure 2 Technique for duodenotomy and three-point ligation of a bleeding duodenal ulcer.
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 9
when NG lavage is inconclusive. These fi ndings, although preliminary, suggest that CT is a potentially valuable evalu-ation method in certain cases of GIB. Perhaps CT scanning can eventually replace radionuclide scanning, which is often inaccurate. One potential drawback to the use of CT in this setting is the excessive dye load if angiography is employed as well. Additionally, a specifi c CT protocol employing timed angiography is required, and the surgeon should discuss this with the radiologist and CT technician prior to performing the study to ensure optimal sensitivity.
ct enterography
A novel method for evaluating occult GIB with a suspecte d origin in the small bowel is CT enterography. As opposed to CT scanning to evaluate for acute bleeding in the upper GI tract or colon, patients undergoing CT enterography are given oral contrast after fasting for 4 hours. Multiphase CT is then performed with additional IV contrast, and timed images are taken at arterial, enteric (50 seconds after injec-tion), and delayed (90 seconds after injection) phases. A 2011 study of 58 patients with occult GIB found CT enterography to be superior to CE in localizing the bleeding source, with sensitivities of 100% and 33%, respectively.52 This method may be an attractive option in the future as this test can be performed much more quickly than CE, although it requires a specifi c CT protocol and CT technicians and radiologists who are experienced in the technique.
enteroscopy
When other tests fail to locate a bleeding source, enteros-copy may be helpful to localize the LGIB. This procedure can be carried out in several ways. It can be performed purely endoscopically with a pediatric colonoscope. Termed “push” endoscopy, this approach generally requires a high level of skill on the part of the endoscopist in that the lack of retroperitoneal attachments of the small intestine makes endoscopic navigation extremely challenging. In most cases, only the proximal 150 cm of the small intestine can be evaluated in this way. Depending on the indication and on the technique employed, the diagnostic yield from push enteroscopy has ranged from 13 to 78%.53 Typically, yields are highest (40 to 60%) in patients with signifi cant GI hemorrhage.
Recently, double-balloon enteroscopy (DBE) has evolved as an effective method of identifying and endoscopically treating occult LGIB. Using this technique, the entire length of the small intestine can be examined in up to 50% of cases using combined antegrade (transoral) and retrograde (trans-anal) insertion by milking the bowel in a push/pull tech-nique between two balloons.54 A recent study demonstrated that 66% of occult bleeding sources were identifi ed using DBE. DBE should be considered the fi rst choice in stable patients with occult active bleeding.
capsule endoscopy
Another option for stable patients with occult GIB is CE, in which a miniature camera is swallowed and intermittent images are taken along the entire length of the GI tract as the capsule advances. Recent studies, including a prospective, blinded trial and several meta-analyses, have demonstrated that the diagnostic yield of CE is similar to that of DBE,
although CE does not allow for therapeutic intervention.54–56 Because it is less invasive, however, CE should be consid-ered the fi rst choice in stable patients in whom occult bleeding has stopped.
Failure of Nonoperative Intervention
If nonoperative measures, including endoscopy and angi-ography with embolization, fail and the patient continues to bleed despite maximal supportive measures, should he or she be taken to the OR for intraoperative diagnosis and management? If UGIB is the etiology, the abdomen should be opened through an upper midline incision, and an ante-rior duodenotomy should be performed at the duodenal bulb. If inspection does not reveal the source of the bleeding or if bleeding is from a duodenal ulcer, the duodenotomy can be extended proximally, or a separate gastrotomy can be performed, to examine the stomach. Bleeding from the proximal stomach may be diffi cult to verify, but it should be actively sought if no other bleeding site is identifi ed. Intra-operative endoscopy should be considered in this situation.
For LGIB, intraoperative options for bleeding site localiza-tion include colonoscopy (to allow for this option, patients should always be placed in the lithotomy position), EGD, and transoral passage of a pediatric colonoscope for enteros-copy with simultaneous intraperitoneal assistance for small bowel manipulation. If the bleeding site is identifi ed, directed segmental resection is the procedure of choice: it is associated with rebleeding rates less than 10% and low mortality rates ranging from 0 to 13%.44 Blind segmental colectomy without accurate localization of the bleeding lesion should never be performed as it is associated with rebleeding rates as high as 75% and mortality rates as high as 50%.57 If the bleeding site still cannot be accurately local-ized, subtotal colectomy (with end ileostomy if the patient remains hemodynamically unstable) is the procedure of choice. This procedure is associated with high morbidity,58 which underscores the importance of accurate preoperative localization of bleeding before surgical intervention.
Discussion and Management of Specifi c Sources of UGIB
duodenal ulcer
The development of effective medical regimens for controlling uncompli-cated duodenal ulcers has led to a drastic reduction in the number of elective surgical procedures per-formed for this purpose. Nevertheless, the incidence of bleeding from duodenal ulcers that is severe enough to necessitate emergency endoscopic or operative intervention has not decreased over the past decade.59
Once EGD has demonstrated that a duodenal ulcer is the source of the bleeding, the fi rst question that must be addressed is whether active bleeding is present. If it is, an attempt should be made to control the hemorrhage endoscopically [see Figure 1]. Because ongoing blood loss eventually leads to coagulopathy, the surgeon must exercise
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 10
good judgment in deciding how long to pursue endoscopic treatment before concluding that such treatment has failed and that surgical treatment is necessary. In general, substantial bleeding (six units or more) or bleeding that is not controlled endoscopically is an indication for surgical intervention. Likewise, ongoing hemorrhage in a hemody-namically unstable patient (especially an elderly one) calls for immediate surgical therapy. An ulcer should be inspected for stigmata of recent hemorrhage. These include (in descending order of risk of further bleeding) active pulsatile bleeding, active oozing, presence of a visible vessel, an adherent clot, a fl at, pigmented spot, and a clean-based ulcer [see Table 3].60
If bleeding is controlled endoscopically, then if not already initiated, PPI therapy, such as pantoprazole, should be given intravenously, either in a bolus twice daily or by continuous infusion.61 Normal gastric mucosa should be biopsied on initial EGD to pathologically evaluate for Helicobacter pylori infection. If H. pylori is present, appropri-ate antibiotic therapy (e.g., a 7 to 14-day course of amoxicil-lin 1 g p.o., b.i.d.; omeprazole, 20 mg p.o., b.i.d.; and clarithromycin, 500 mg p.o., b.i.d.) should be given as such therapy has been shown to reduce rebleeding rates after antacid medication has been stopped.62 Food need not be withheld unless the likelihood of rebleeding is high because resumption of oral feeding does not appear to affect rebleed-ing rates.63 If bleeding recurs despite medical and endoscopi c therapy, a second attempt at endoscopic control should be made. Repeat endoscopic treatment reduces the need for surgery without increasing the risk of death and is associated with fewer complications than is surgery.64
If endoscopy fails to control bleeding or bleeding recurs after initial endoscopic therapy, angiographic embolization can be considered a therapeutic alternative to surgery. A systematic review of studies evaluating embolization therapy for nonvariceal UGIB found a mean 84% technical success rate and a 67% clinical success rate.65 A comparison of angiographic embolization with surgical intervention for UGIB after failed endoscopic therapy found a lower rate of
bleeding recurrence after surgery (13% versus 34%) but a higher rate of complications (68% versus 41%).66 Based on this evidence, embolization may be best targeted toward patients at higher risk for complications after surgical intervention.
In patients whose UGIB cannot be controlled via other means, surgical management may be accomplished either laparoscopically or via an open approach, although laparos-copy should not be attempted in hemodynamically unstable patients [search for more information]. The latter begins with an upper midline incision. The duodenum is mobilized using a Kocher maneuver, and an anterior longi-tudinal duodenotomy is performed at the duodenal bulb as the most common source of bleeding is the gastroduodenal artery (GDA), which lies behind the posterior wall of the fi rst portion of the duodenum. The GDA is ligated with non-absorbable sutures at sites proximal and distal (i.e., superior and inferior) to the bleeding point. A third stitch is placed medial to the bleeding vessel to prevent back-bleeding from the transverse pancreatic artery [see Figure 2]. Pains must be taken to avoid injury to the common bile duct during the placement of these sutures, and cannulation of the duct through the ampulla of Vater may be helpful in identifying its course. The duodenotomy is then closed. If a truncal vagotomy is to be performed, the duodenotomy should extend through the pylorus and be closed transversely to perform a pyloroplasty.
A decision is then made whether to perform an acid-reducing procedure. Options are a truncal vagotomy with or without an antrectomy and Billroth I or II reconstruction. The recommendation for truncal vagotomy is based on data from studies done before PPIs and H. pylori therapy came into use. Subsequent studies and a 2004 Cochrane review that evaluated rebleeding rates with current medical regi-mens demonstrated much lower rebleeding rates.67 Further-more, it seems probable that long-term PPI therapy (the medical equivalent of vagotomy), in conjunction with eradication of H. pylori and avoidance of NSAIDs, should reduce rebleeding rates signifi cantly. Studies from the United States59 and the United Kingdom68 have shown that a vagotomy is performed less than 50% of the time during surgical treatment of an acute bleeding duodenal ulcer. Therefore, although there are no prospective, randomized studies to support it, one may consider an alternative treat-ment approach in patients who have not been receiving ulcer therapy before the bleeding began—namely, ligation of the bleeding vessel, postoperative administration of PPIs, and H. pylori therapy. This approach avoids the complica-tions associated with truncal vagotomy.
Another option for preventing postvagotomy symptoms when operating on stable patients for bleeding duodenal ulcer is to perform a highly selective vagotomy (HSV). This procedure is considered preferable to truncal vagotomy because of the decreased incidence of gastric atony, alkaline refl ux gastritis, dumping, and diarrhea; however, HSV is associated with a higher recurrence rate than is truncal vagotomy and takes signifi cantly longer to perform.69
gastric ulcer
Gastric ulcers are classifi ed according to their location and to the role (if any) that gastric acid hypersecretion plays in
Table 3 Forrest Classifi cation for Stigmata of Recent Hemorrhage Used to Evaluate Bleeding Ulcers and Prevalence Data for Each Class from
Enestvedt et al60
Stigmata of Recent Hemorrhage
Forrest Classifi cation
Prevalence (%)
Active bleeding
Active spurting IA 12 (spurting and oozing combined)
Active oozing IB
Recent hemorrhage
Nonbleeding vessel IIA 8
Adherent clot IIB 8
Flat pigmented spot IIC 16
No signs of hemorrhage
Clean-based ulcer III 55
Scientific American Surgery
the publication

12/12
gastro gastrointestinal bleeding — 11
not resected, a biopsy of the ulcer should be performed to rule out malignancy, taking care to avoid further exacerbating bleeding as a result of the biopsy.
esophageal varices
The value of endoscopy in the diagnosis and management of variceal bleeding cannot be overemphasized. Even in patients with known varices, the site of bleeding is frequentl y nonvariceal; endoscopy is therefore essential.71 If bleeding varices are identifi ed, rubber banding or intravariceal sclero-therapy with a sclerosing agent (1.5% sodium tetradecyl sul-fate, ethanolamine, sodium morrhuate, or absolute alcohol) is performed [see Figure 4].72 If these measures do not control the hemorrhage, balloon tamponade is indicated.73 Success-ful balloon tamponade is followed by endoscopic variceal injection or variceal banding.
IV somatostatin should be administered in conjunction with the above-mentioned steps. Vasopressin may also be given; however, it causes diffuse vasoconstriction, and nitro-glycerin may be required to alleviate cardiac side effects. Somatostatin has proved superior to placebo in controlling variceal hemorrhage when used in conjunction with endo-scopic sclerotherapy.74 It is as effective as vasopressin while giving rise to fewer side effects. Octreotide, a synthetic analogue of somatostatin, shares many of the properties of somatostatin but perhaps not all. Both agents decrease secre-tion of gastric acid and pepsin; however, the decreased gastric blood fl ow observed with somatostatin administra-tion has not been reported with octreotide administration. Nevertheless, most clinicians in the United States elect to use octreotide (25 to 50 µg/hr) in place of IV somatostatin because the former tends to be more widely available.
Cirrhotic patients presenting with acute variceal bleeding should also be given prophylactic antibiotics (e.g., ceftriax-one 1 g IV, q.d. for 7 days). Antibiotic administration has been shown to decrease rates of infection, including sponta-neous bacterial peritonitis, and may even decrease overall mortality.75 Human recombinant activated factor VII (rHuF-VIIa) has gained recent attention for use in patients with massive hemorrhage and coagulopathy, including patients with esophageal variceal bleeding due to liver failure. How-ever, a 2012 Cochrane meta-analysis of randomized trials comparing rHuFVIIa with conventional treatment failed to show an advantage in terms of mortality or other clinical outcomes.76 Based on the existing evidence, rHuFVIIa should not be used in patients with bleeding esophageal varices outside an investigational setting.
After the acute variceal bleeding has been controlled, any remaining varices should be subjected to injection sclerotherapy or banding at 2-week intervals until they too are obliterated.
The main indications for surgical intervention in patients with bleeding esophageal varices are uncontrolled hemor-rhage and/or persistent rebleeding despite endoscopic and medical therapy. When such intervention is considered, it is essential to determine whether the patient is a transplant candidate. If so, operation should be avoided and bleeding managed by decompressing the portal venous system with a transjugular intrahepatic portosystemic shunt (TIPS). A TIPS signifi cantly reduces rebleeding rates but poses a risk of encephalopathy.77
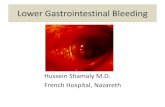
their development. Type I ulcers are located on the lesser curvature and are not associated with acid secretion. Type II ulcers are associated with high acid secretion and are located on the lesser curvature, occurring in synchrony with duodenal ulcers. Type III ulcers are also associated with acid hypersecretion but occur in the prepyloric region. Type IV ulcers are not associated with acid secretion and are located in the cardia near the esophagogastric junction [see Figure 3]. Type V ulcers are diffuse and are related to the use of med-ications (e.g., NSAIDs) [see Acute Hemorrhagic Gastritis, below].
Bleeding is less common than with duodenal ulcers, but initial management of a bleeding gastric ulcer is the same as that of a duodenal ulcer (i.e., endoscopic control) [see Figure 1]. To prevent aggravation of the bleeding, early biopsy generally is not recommended; repeat endoscopy and biopsy are done at a later date. The indications for emer-gency surgical intervention for gastric ulcers are the same as those for duodenal ulcers.
Bleeding gastric ulcers that necessitate operative interven-tion should be treated with resection. For type I ulcers, wedge resection is typically performed. For type II and III ulcers, the usual approach consists of antrectomy with Bill-roth I reconstruction and truncal vagotomy. Type IV ulcers can pose a technical challenge as a consequence of their close proximity to the esophagogastric junction. A distal gastrectomy with a tongue-shaped extension upward along the lesser curvature to incorporate the ulcer, followed by a Roux-en-Y reconstruction (the Csendes procedure), is often required.70 Another option is ligation of the left gastric artery followed by oversewing of the ulcer. If the bleeding ulcer is
IV
I
III
II
Figure 3 Anatomic locations of gastric ulcers according to the mod-ifi ed Johnson classifi cation. Type I lies along the lesser curvature. Type II are multiple ulcers, one in the gastric body and one or more in the duodenum. Type III is a prepyloric ulcer. Type IV is a proximal ulcer. Type V (not shown) is an ulcer due to nonsteroidal antiinfl am-matory drug use, which can occur in any anatomic location.
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 12
Figure 4 An algorithm for management of bleeding from esophageal or gastric varices. IV = intravenous; PTFE = polytetrafl uoroethylene.
If the patient is not a transplant candidate and is not actively bleeding, a distal splenorenal shunt (DSRS) is preferable.78 In the emergency setting, a central portacaval shunt may be placed. Esophageal transection is also a rea-sonable choice. This procedure is associated with a lower incidence of encephalopathy than a portacaval shunting procedure; however, it is associated with higher rates of rebleeding (particularly late rebleeding) and can be diffi cult
to perform when active bleeding is present. Suture ligation of the bleeding varices with devascularization (the Sugiura procedure) should also be considered.
In general, the prognosis is related to the underlying liver disease. For example, patients with varices that are secondary to chronic extrahepatic portal venous or splenic venous occlusion generally have a much better prognosis than those whose portal hypertension is secondary to
Patient has bleeding from esophageal orgastric varices
Bleeding stops
Patient is a transplant candidate Patient is not a transplant candidate
Bleeding continues
Bleeding stops
Patient is stable Patient is unstable
Bleeding does recur
Initiate surgical management
Bleeding recurs Bleeding continues
Attempt to control hemorrhage endoscopicallywith intravariceal injection sclerotherapy or rubber banding (gastric varices are lessamenable to sclerotherapy). Give IV somatostatin (250 µg bolus, then 250 µg/hr).Octreotide (25–50 µg/hr) is an altemative.
If any varices remain, repeat injectionsclerotherapy or banding at 2 wk intervalsuntil varices are gone. Give propranolol p.o.
Decompress portal venous system with transjugularintrahepatic portosystemic shunt (TIPS). Proceedwith transplantation when suitable organ is obtained.
Procedure of choice depends on patient status.
Pass 4-port Minnesota tube andperform balloon tamponade.
Perform intravariceal injectionsclerotherapy or rubber banding.If any varices remain, repeat sclero-therapy or banding at 2 wk intervalsuntil varices are gone. Give propranolol p.o.
Obtain arteriograms with views of portal veinand left renal vein.If tenous anatomy is suitable: perform distalsplenorenal shunting procedure.If tenous anatomy is not suitable: consideresophageal transection (for esophageal varicesonly) or mesocaval or portacaval shunt.
Perfom central portacaval shuntingprocedure (usually side to side or withshort PTFE interposition graft).Alternatively, consider esophagealtransection (for esophageal varices only)or suture ligation of bleeding gastricvarices.
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 13
hepatic parenchymal causes. The severity of the cirrhosis also determines short-term and long-term survival and may infl uence the decision whether to perform a shunting procedure.
Several prospective, randomized trials have shown that propranolol (40 mg b.i.d., p.o.) decreases the incidence of fi rst-time variceal bleeding and the incidence of recurrent variceal bleeding.79,80 However, propranolol should not be used during active bleeding but rather should be started only after bleeding stops.
gastric varices
Gastric varices due to portal hypertension are managed in much the same way as esophageal varices [see Figure 4], although they are less amenable to sclerotherapy.81 Other endoscopic treatments (e.g., ligation or sclerotherapy plus ligation) and interventional radiologic treatments (e.g., TIPS or intravascular balloon occlusion) should be considered before surgical management (i.e., DSRS, portosystemic shunting, or suture ligation with gastric devascularization). If the patient is a suitable candidate, liver transplantation may be performed as an alternative to shunting. Occasion-ally, UGIB can be due to gastric varices secondary to left-sided, or sinistral, portal hypertension. This is usually the result of pancreatic pathology (pancreatitis, pseudocyst, neoplasm) causing splenic vein thrombosis and selective left-sided portal hypertension. Clinical suspicion should be high when varices are present only in the gastric fundus in a patient without liver disease. Treatment in these patients consists of splenectomy, which is usually curative; the pro-cedure may be performed laparoscopically if the patient is hemodynamically stable.82
mallory-weiss tears
Mallory-Weiss tears are linear mucosal tears at the esoph-agogastric junction that are usually caused by vomiting. Any patient who presents with vomiting that initially is not bloody but later turns so should be suspected of having a Mallory-Weiss tear. As a rule, these lesions stop bleeding without therapy. If bleeding is substantial or persistent, however, endoscopic injection, clipping, banding, or coagu-lation may be necessary.83,84 In rare instances, the tear will have to be oversewn at operation. This is accomplished via an anterior gastrotomy and direct suture ligation of the tear.
acute hemorrhagic gastritis
Bleeding from gastritis is virtually always managed med-ically with H2 blockers, PPIs, sucralfate, or antacids (either alone or in combination), along with antibiotics if H. pylori is present.85 Somatostatin may be benefi cial. Sometimes administration of vasopressin via the left gastric artery is needed to control bleeding. In rare cases, total or near-total gastrectomy is required; however, the mortality associated with this operation in this setting is high. Stress ulcer pro-phylaxis in severely ill or traumatized patients is essential to prevent this problem.86 The gastric pH should be kept as close to neutral as possible. If the gastritis is relatively mild, a biopsy specimen should be obtained and tested for H. pylori. Treatment consists of acid reduction and H. pylori therapy.
neoplasms
Benign tumors of the upper GI tract (e.g., gastro-intestinal stromal tumors [GISTs], hamartomas, and hemangiomas) occasional-ly bleed. Wedge excision of the offending lesion is the procedure of choice. GISTs (previously classifi ed as leiomy-omas or leiomyosarcomas) run the gamut from benign to highly aggressive. They typically present as a submucosal mass that may cause bleeding as a result of mucosal ulcer-ation. The bleeding may be treated with wedge excision of the tumor, which can be challenging when the GIST is located in the gastric cardia. Such excision can often be accomplished laparoscopically or even through a laparo-scopic intragastric approach.87 A combined intragastric laparoscopic approach using a fl exible endoscope for visual-ization and specimen retrieval may be helpful in reducing the number and size of laparoscopic trocars required.88 Bleeding from malignant neoplasms, whether early stage or late stage, generally can be controlled initially by endoscopi c means; however, rebleeding rates are high.89 If the lesion is resectable, it should be excised promptly once the patient is stable (provided that it has been appropriately staged). If disease is advanced, however, surgical options are limited, and a nonoperative approach, although necessarily imperfect, is preferable.
hiatal hernia
Not infrequently, the source of chronic enteric blood loss is a hiatal hernia. Major bleeding is rare in this condition but may occur as a result of linear erosions at the level of the diaphragm (Cameron lesions),90 gastritis within the hernia, or torsion of a paraesophageal hernia. Endoscopy is gener-ally diagnostic, although the sources of chronic blood loss are not always obvious. Recognition that the bleeding derives from a Cameron lesion should incline the surgeon toward operative intervention; this lesion is usually mechanically induced and therefore tends to be less respon-sive to antacid therapy.
Chronic bleeding from a type I hiatal hernia should be treated initially with a PPI. H. pylori therapy should be added if biopsy shows this organism to be present. Operative management (i.e., laparoscopic Nissen fundopli-cation) should be considered for fi t patients who have complications associated with their hiatal hernia and for all symptomatic patients with type II, III, or IV hiatal hernias (laparoscopic paraesophageal hernia repair).91
dieulafoy lesion
A Dieulafoy lesion is the rupturing of a 1 to 3 mm bleed-ing vessel through the GI mucosa without surrounding ulceration. This lesion is most commonly found high on the lesser curvature of the stomach, but it can also occur anywhere throughout the GI tract. Histologic studies have not revealed any intrinsic abnormalities either of the mucosa or of the vessel.
Initial treatment consists of either endoscopically based coagulation of the bleeding vessel with a heater probe or
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 14
mechanical control with clips or rubber bands; local injec-tion of epinephrine may help control acute hemorrhage while this is being done. In skilled hands, endoscopic therap y has a 95% success rate, and long-term control is excellent. If endoscopic therapy fails, surgical options, including ligation or excision of the vessel involved, come into play.92 Having the endoscopist mark the site with India ink is helpful for localization.
hemobilia
Hemobilia should be suspected in all patients who pres-ent with the classic triad of epigastric and right upper quad-rant pain, GIB, and jaundice; however, only about 40% of patients with hemobilia present with the entire triad. Hemobilia should also be suspected in any patient who had previous liver trauma, percutaneous transhepatic cholangi-ography, TIPS, or other liver instrumentation. Endoscopy demonstrating blood coming from the ampulla of Vater points to a source in the biliary tree or the pancreas (hemo-succus pancreaticus).
Arteriography may provide the defi nitive diagnosis: a bleeding tumor, a ruptured artery from trauma, or another cause. Arteriographic embolization of the affected portion of the liver is the preferred treatment option; hepatic artery ligation (selective if possible) or hepatic resection may be required.
hemosuccus pancreaticus
Bleeding into the pancreatic duct, generally from erosion of a pancreatic pseudocyst into the splenic artery, is signaled by upper abdominal pain followed by hematochezia.93 If
endoscopy is performed when hematochezia is present, the bleeding site may not be seen; however, if endoscopy is per-formed when pain is fi rst noted, blood may be seen coming from the ampulla of Vater. The combination of signifi cant GIB, abdominal pain, a history of alcohol abuse or pancre-atitis, and hyperamylasemia should suggest the diagnosis. If there are no pancreatitis-related indications for surgery, angiographic embolization can be defi nitive treatment.94 If there are pancreatitis-related indications for operation, angiographic embolization may allow an elective operative procedure based on the structural changes observed in the pancreas. If embolization fails, pancreatic resection is usually required, often on an emergency basis.
aortoenteric fistula
Aortoenteric fi stulas may occur spontaneously as a result of rupture of an aortic aneurysm or perforation of a duode-nal lesion (primary); more often, they arise after aortic sur-gery (secondary).95 The most common cause is a graft infec-tion, resulting in graft erosion into the posterior aspect of the third section of the duodenum. A common initial manifesta-tion of an aortoenteric fi stula is small herald or “sentinel” bleeding that is followed a few days later by a massive hem-orrhage. Patients often present with the triad of GI hemor-rhage, a pulsatile mass, and infection; however, not all of these symptoms are invariably present. A high index of sus-picion facilitates diagnosis. Endoscopy may show an aortic graft eroding into the enteric lumen, but this is an uncom-mon fi nding. CT scanning is the procedure of choice for diagnosis. The fi nding of air around the aorta or the aortic
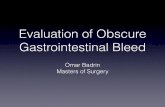
Figure 5 An algorithm for management of lower gastrointestinal bleeding (LGIB). AVM = arteriovenous malformation; IV = intravenous; OR = operating room; TIPS = transjugular intrahepatic portosystemic shunt.
Diverticulosis Colonic AVMs Neoplasm
If bleeding detected at time of colono-scopy or angio-graphy,attempt endoscopic treatment or emboli-zation
LGIB source found. Manage specific sources
If bleeding from endosco-pic poly-pectomy site, attemptendosco-pic control
Segmental resection if localized
Subtotal colectomy if not localized
If continued bleeding or re-bleeding occurs, to OR resection If stops –
observe
If bleeding continues, repeat attempt at endoscopic control
If second attempt fails, to OR for resection
Attempt endoscopic control of bleeding
Treat lesion according to oncolo-gic prin-ciples [search the
for
cinoma of the colon and
]
Benign Anorectal
Colitis
Small Intestine Source
Attempt direct control with packing and suture ligation
If portal hyperten-sion and continued bleeding, consider TIPS
If AVM, treate endo-scopically or angio-graphicallydepending on initial diagnostic test
If con-tinued bleeding, to OR for seg-mental resection
Colonic Ischemia
If no peri-tonitis, initiate bowel rest, IV fluids and anti-biotics and discontinue vasopressor agents if applicable
If peri-tonitis, to OR for resec-tion and ostomy
Consider intraoperative endoscopic guidance to help localize lesion
Treat underlying disease process [search
for
]
adenocar-
the
fulminant ulcerative colitis and Crohn disease
Scientific American Surgery
publication
publication
rectupm

12/12
gastro gastrointestinal bleeding — 15
graft is diagnostic and is an indication for emergency explo-ration. The preferred surgical treatment is extra-abdominal bypass (e.g., axillary-femorofemoral bypass) with subse-quent excision of the graft and closure of the aorta proxi-mally and aorta or common iliac arteries distally. Some authorities, however, advocate resection of the graft with in situ graft replacement.96 Some now advocate endovascular stent repair for high-risk patients without evidence of infection.97
vascular ectasias
Vascular ectasias (also referred to as vascular dysplasia, angiodysplasia, angiomata, telangiectasia, and AVMs) may bleed briskly. As a rule, gastric lesions can be readily identi-fi ed and the bleeding controlled by endoscopic means.98 Lesions that continue to bleed, either acutely or chronically, despite endoscopic measures should be excised. Some patients have multiple and extensive lesions that necessitate resection of large portions of the stomach. Pharmacotherapy and hormone therapy have been tried; the results have been mixed.
duodenal diverticula
Duodenal diverticula are rare causes of UGIB. Accurate identifi cation of a bleeding site within a given diverticulum is diffi cult, but an attempt should be made to accomplish this by means of per oral enteroscopy or video-CE. Excision is the preferred treatment and is accomplished by means of segmental resection.99 Great care must be taken in the treat-ment of duodenal diverticula in the region of the ampulla of Vater to ensure that the pancreatic duct and the bile ducts are not injured during excision.
Discussion and Management of Specifi c Sources of LGIB
diverticulosis
The vast majority of colonic diverticula are actually false diverticula (pseudodiverticula) that contain only serosa and mucosa. They occur at weak points in the colonic wall where the vasa recta penetrate the muscularis to supply the mucosa; as the diverticulum expands, these vessels are dis-placed. A 1976 anatomic study of colonic specimens from patients with diverticular bleeding used angiography to demonstrate that in all cases, the vasa recta overlying the diverticulum ruptured into the lumen of the diverticulum, not into the peritoneum.100
It has been estimated that approximately 17% of patients with colonic diverticulosis experience bleeding, which may range from minor to severe and life-threatening. Endoscopic treatment of diverticular hemorrhage can be diffi cult because of the high bleeding rate and the location of the bleeding point within the diverticulum. In 2000, one group of investigators reported their experience with endoscopic therapy for severe hematochezia and diverticulosis in a pro-spective series of 121 patients.101 In this series, none of the patients treated endoscopically with epinephrine injections, bipolar coagulation, or both required surgery and none experienced recurrent bleeding episodes. A 2001 study from another group, however, reported high rates of recurrent bleeding episodes in both the early and the late posttreat-ment periods.102 In the absence of prospective, randomized
trials, it is diffi cult to draw defi nitive conclusions about the utility of endoscopic therapy in treating diverticular hemorrhage.
Fortunately, most diverticular hemorrhages stop sponta-neously. In one series, surgery was unlikely to be necessary if fewer than four units of packed RBCs were transfused in a 24-hour period, whereas 60% of patients receiving more than four units of packed RBCs in a 24-hour period required surgical intervention.103 Semielective surgical therapy is usually offered after a second diverticular bleeding episode because once a second such episode has occurred, the risk that a third will follow exceeds 50%. In a series of 83 conser-vatively managed cases of diverticular disease, the predicted yearly recurrence rates were 9% at 1 year, 10% at 2 years, 19% at 3 years, and 25% at 4 years.104
In general, patients who require more than four units of blood in a 24-hour period to remain hemodynamically stable, who have not stopped bleeding after 72 hours, or who experience rebleeding within 1 week after an initial episode should undergo surgery.
colonic avms
The term arteriovenous malformation includes vascular ecta-sias, angiomas, and angiodysplasias. AVMs are ectatic blood vessels seen in the mucosa and submucosa of the GI tract. They are degenerative lesions of the GI tract, occurring more frequently with advancing age. In patients older than 50 years, the incidence of colonic AVMs is estimated to range from 2 to 30%.105
Colonic AVMs are believed to derive from chronic coloni c wall muscle contraction, which leads to chronic partial obstruction of the submucosal veins, causing the vessels to become dilated and tortuous. This process eventually renders the precapillary sphincters incompetent, resulting in direct arteriovenous communication. Colonic AVMs are most commonly found in the cecum. They have been associ-ated with several systemic diseases, including atheroscle-rotic cardiovascular disease, aortic stenosis, chronic renal disease, collagen vascular disease, von Willebrand disease, chronic obstructive pulmonary disease, and cirrhosis of the liver; to date, however, no defi nite causal relation to any of these conditions has been established.4
The diagnosis of a colonic AVM is made at the time of angiography or colonoscopy. During angiography, visual-ization of ectatic, slow-emptying veins, vascular tufts, or early-fi lling veins establishes the diagnosis.90 During endos-copy, angiodysplasias appear as red, fl at lesions about 2 to 10 mm in diameter, sometimes accompanied by a feeding vessel.
Typically, the bleeding caused by colonic AVMs is chroni c, slow, and intermittent. Although these lesions can cause severe lower GI hemorrhage, they are a relatively uncom-mon cause. The bleeding stops spontaneously in 85 to 90% of cases106 but recurs in 25 to 85%.107 Accordingly, defi nitive surgical or colonoscopic treatment should be rendered once the lesion has been identifi ed.
Colonic AVMs are usually amenable to endoscopic treat-ment. That these lesions are frequently found in the right colon makes perforation a concern; this complication is reported in approximately 2% of patients. Good success rates have been reported with both injection and thermal
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 16
methods.108 In one series, endoscopic fulguration was successful in 87% of patients, and no rebleeding episodes occurred over a 1- to 7-year follow-up period.108 Bleeding from multiple telangiectatic lesions in the distal colon result-ing from radiation injury can be treated with thermal contact probes, lasers, or noncontact devices such as the argon plasma coagulator.
neoplasia
Signifi cant GIB from colorectal neoplasia accounts for 7 to 33% of cases of severe lower GI hemorrhage.3,25 Such bleeding is believed to result from erosions on the luminal surface. Adenomatous polyps are implicated in 5 to 11% of cases of acute LGIB.109
LGIB, either immediate or delayed, is the most common reported complication after endoscopic polypectomy, occur-ring in 0.2 to 6% of cases.3,104 Immediate postpolypectomy bleeding is believed to result from incomplete coagulation of the stalk before transection. Delayed bleeding has been reported as long as 15 days after polypectomy and is thought to be secondary to sloughing of the coagulum; it is less common than immediate bleeding, occurring in only 0.3% of cases.110 Postpolypectomy hemorrhage can often be success-fully treated by endoscopic means. Methods used include simple resnaring of the stalk while pressure is maintained94; electrocauterization, with or without epinephrine injection; endoscopic band ligation; and placement of metallic clips.
benign anorectal disease
Hemorrhoids, ulcer or fi ssure disease, and fi stula in ano must not be overlooked as causes of GI hemorrhage: in one review comprising almost 18,000 cases of LGIB, 11% were attributable to anorectal pathology. It is therefore imperative to perform a digital rectal examination and anoscopy in all patients with LGIB. However, identifi cation of a benign anorectal lesion does not eliminate the possibility of a more proximal cause of hemorrhage. Patients with hemorrhoids identifi ed on physical examination should therefore still undergo thorough endoscopic evaluation of the colon to rule out other pathologic conditions. For patients whose bleeding is attributable to benign anorectal causes, endo-scopic therapy may include epinephrine injection, sclerosant injection, or band ligation of internal hemorrhoids.111
Portal hypertension, congestive heart failure, and splenic vein thrombosis can cause colonic or anorectal varices, which can result in massive lower GI hemorrhage. The reported incidence of anorectal varices in patients with por-tal hypertension ranges from 78 to 89%.112 If local measures fail to control hemorrhage, some form of portosystemic shunting is indicated.
colitis
The broad term colitis includes IBD, infectious colitis, radiation colitis, and idiopathic ulcers. IBD, in turn, includes Crohn disease and ulcerative colitis. Patients with IBD usu-ally present with bloody diarrhea that is not life-threatening; however, 6 to 10% of patients with ulcerative colitis have LGIB severe enough to necessitate emergency surgical resec-tion, and 0.6 to 1.3% of patients with Crohn disease have acute life-threatening LGIB.113 In one review, 50% of patients
with intestinal hemorrhage from IBD experienced spontane-ous cessation of bleeding.113 Approximately 35% of patients whose bleeding stops without intervention will have anoth-er bleeding episode. Because of this high recurrence rate, semielective surgery is recommended after the fi rst episode of severe GIB secondary to IBD.
Colitis caused by various infectious agents (e.g., typhi, Escherichia coli O157:H7, Clostridium diffi cile, and cytomega-lovirus) can result in severe LGIB, but this is a relatively rare occurrence.
Increasing use of radiation therapy to treat pelvic malig-nancies has led to a corresponding increase in the incidence of chronic radiation proctitis. Radiation therapy damages bowel mucosa, resulting in the formation of vascular ecta-sias that are prone to bleeding. From 1 to 5% of cases of acute LGIB from radiation-induced proctocolitis are severe enough to necessitate hospitalization.86 In a survey of patients with prostate cancer who underwent pelvic irradia-tion, 5% of the patients reported hematochezia daily.114 Initial therapy for clinically signifi cant hematochezia related to radiation proctitis should include some form of endoscopi c treatment (e.g., argon-beam coagulation). Surgery should be reserved for unstoppable hemorrhage or other major complications, such as fi stulas and strictures.
coagulopathy
LGIB or UGIB can be a presenting symptom for both patients with iatrogenic coagulopathy from heparin or war-farin therapy and patients with a hematologic coagulopathy from thrombocytopenia. It is unclear, however, whether severe coagulopathy leads to spontaneous hemorrhage or whether it predisposes to bleeding from an existing lesion.115 In an early series of leukemic patients with thrombocytope-nia and severe GI hemorrhage, 50% of bleeding patients had platelet counts lower than 20,000/µL without any identifi able mucosal lesions; furthermore, when the platelet count rose above 20,000/µL, the incidence of bleeding decreased to 0.8%.115 The investigator concluded that severe thrombocytopenia led to spontaneous GI hemorrhage. Other investigators subsequently challenged this conclusion, argu-ing that spontaneous bleeding from coagulopathy is, in fact, rare. In one report, the distribution of pathologic lesions in patients with GIB who were taking heparin or warfarin was essentially equivalent to that in the general population.116 Regardless of what the precise relation between coagulopa-thy and GI hemorrhage may be, a thorough investigation for an anatomic lesion is imperative in the workup of patients with LGIB even in the face of coagulopathy or thrombocytopenia.
colonic ischemia
Acute LGIB can also be a presenting symptom of colonic ischemia. In several large series, colonic ischemia accounted for 3 to 9% of cases of acute lower GI hemorrhage.104,109 Other vascular diseases reported as potential causes are polyarteritis nodosa, granulomatosis with polyangiitis, and rheumatoid vasculitis. The resultant vasculitis can cause ulceration, necrosis, and, ultimately, hemorrhage.
More than 80% of patients with colonic ischemia respond to bowel rest, IV fl uids, and antibiotics and do not require surgical intervention.117 When exploration is indicated
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 17
because of peritonitis or recalcitrant disease, all questionable bowel should be resected with stoma creation unless a second-look operation is planned.
small intestinal sources
Small intestinal sources account for 0.7 to 9% of cases of acute LGIB.3,104 About 70 to 80% of cases of small bowel hem-orrhage are attributable to AVMs; other, less common causes are jejunoileal diverticula, Meckel diverticulum, neoplasia, regional enteritis, and aortoenteric fi stulas. Accurate local-ization of a bleeding site in the small intestine can be highly challenging: the length and the free intraperitoneal position of the small bowel make endoscopic examination diffi cult, and the nature of the overlying loops makes angiographic localization imprecise. For these reasons, the small intestine is usually left for last in the attempt to localize the source of LGIB and is examined only after sources in the colon, upper GI tract, and anorectum have been ruled out.
aids
The etiology of LGIB in patients with AIDS differs from that in the general population. In AIDS patients, LGIB is caused predominantly by conditions related to the underly-ing HIV infection. Cytomegalovirus colitis is the most com-mon cause of such bleeding in this population, occurring in 39% of cases. AIDS patients with hemorrhoids or anal fi ssures often experience signifi cant bleeding as a result of HIV-induced thrombocytopenia. A 1998 study reported that in 23% of AIDS patients hospitalized for LGIB, benign anorectal disease was the cause.118 Other signifi cant causes of lower GI hemorrhage in this population are colonic histoplasmosis, Kaposi sarcoma of the colon, and bacterial colitis.118
nsaids
Although the association between NSAID use and UGIB is well known, current data suggest that NSAIDs have a toxic effect on colonic mucosa as well. An epidemiologic study estimated the incidence of NSAID-associated large bowel bleeding to be seven in 100,000.119 A retrospective review found that patients who had experienced LGIB were twice as likely to have taken NSAIDs as those who had not.120 NSAIDs have also been linked to diverticular hemor-rhage. The exact mechanism of NSAID-induced colonic injury is unknown.
Summary
Despite recent advances in diagnostic and therapeutic capabilities, in-hospital mortality rates have remained signifi cant in patients presenting with both upper and lower GIB. Starting with the initial evaluation in the emergency department, these patients should be managed with the same sense of clinical urgency that is now standard for severely injured trauma patients and patients with sepsis. Such prompt diagnostic and resuscitative efforts can stabi-lize patients early in their clinical course and save them from unnecessarily invasive interventions further on. Although the widespread use of PPI therapy and advances in less invasive procedures such as fl exible endoscopy and angio-graphy have decreased the volume of surgery for peptic
ulcers and other causes of GIB, there will always be a role for surgery for bleeding that is refractory to other therapies. The surgical techniques for management of such critically ill patients remain an essential component of any general surgery training program.
Financial Disclosures: None Reported.
References
1. Rockall TA, Logan RF, Devlin HB, et al. Incidence of and mortality from acute upper gastrointestinal haemorrhage in the United Kingdom. Steering Committee and members of the National Audit of Acute Upper Gastrointestinal Haemorrhage. BMJ 1995;311:222.
2. Koval G, Benner KG, Rosch J, et al. Aggressive angio-graphic diagnosis in acute lower gastrointestinal hemor-rhage. Dig Dis Sci 1987;32:248.
3. Jensen DM, Machicado GA. Diagnosis and treatment of severe hematochezia: the role of urgent colonoscopy after purge. Gastroenterology 1988;95:1569.
4. Foutch PG, Rex DX, Lieberman DA. Prevalence and natural history of colonic angiodysplasia among healthy asymptomatic people. Am J Gastroenterol 1995;90:564.
5. Krevsky B. Detection and treatment of angiodysplasia. Gastrointest Endosc Clin North Am 1997;7:509–24.
6. Cebollero-Santamaria F, Smith J, Gioe S, et al. Selective outpatient management of upper gastrointestinal bleeding in the elderly. Am J Gastroenterol 1999;94:1242.
7. Lau JY, Leung WK, Wu JC, et al. Omeprazole before endoscopy in patients with gastrointestinal bleeding. N Engl J Med 2007;356:1631–40.
8. Sreedharan A, Martin J, Leontiadis GI, et al. Proton pump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding. Cochrane Database Syst Rev 2010;(7):CD005415.
9. Liebler JM, Benner K, Putnam T, et al. Respiratory compli-cations in critically ill medical patients with acute upper gastrointestinal bleeding. Crit Care Med 1991;19:1152.
10. Blatchford O, Murray WR, Blatchford M. A risk score to predict need for treatment for upper-gastrointestinal haemorrhage. Lancet 2000;356:1318–21.
11. Rockall TA, Logan RF, Devlin HB, Northfi eld TC. Risk assessment after acute upper gastrointestinal haemor-rhage. Gut 1996;38:316–21.
12. Strate LL, Saltzman JR, Ookubo R, et al. Validation of a clinical prediction rule for severe acute lower intestinal bleeding. Am J Gastroenterol 2005;100:1821–7.
13. Savides TJ, Jensen DM. Therapeutic endoscopy for non-variceal upper gastrointestinal bleeding. Gastroenterol Clin North Am 2000;29:465.
14. Jairath V, Kahan BC, Logan RF, et al. Outcomes following acute nonvariceal upper gastrointestinal bleeding in rela-tion to time to endoscopy: results from a nationwide study. Endoscopy 2012;44:723–30.
15. Lim LG, Ho KY, Chan YH, et al. Urgent endoscopy is asso-ciated with lower mortality in high-risk but not low-risk nonvariceal upper gastrointestinal bleeding. Endoscopy 2011;43:300–6.
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 18
16. Bjorkman DJ, Zaman A, Fennerty MB, et al. Urgent vs. elective endoscopy for acute non-variceal upper-GI bleed-ing: an effectiveness study. Gastrointest Endosc 2004;60:1–8.
17. Barkun AN, Bardou M, Martel M, et al. Prokinetics in acute upper GI bleeding: a meta-analysis. Gastrointest Endosc 2010;72:1138–45.
18. Jacobson AR, Cerqueira MD. Prognostic signifi cance of late imaging results in technetium-99m-labeled red blood cell-gastrointestinal bleeding studies with early negative images. J Nucl Med 1992;33:202.
19. Dempsey DT, Burke DR, Reilly RS, et al. Angiography in poor-risk patients with massive nonvariceal upper gastrointestinal bleeding. Am J Surg 1990;159:282.
20. Richter JM, Christensen MR, Kaplan LM, et al. Effective-ness of current technology in the diagnosis and manage-ment of lower gastrointestinal hemorrhage. Gastrointest Endosc 1995;41:93.
21. Ohyama T, Sakurai Y, Ito M, et al. Analysis of urgent colonoscopy for lower gastrointestinal tract bleeding. Digestion 2000;61:189.
22. Green BT, Rockey DC, Portwood G, et al. Urgent colonos-copy for evaluation and management of acute lower gas-trointestinal hemorrhage: a randomized controlled trial. Am J Gastroenterol 2005;100:2395–402.
23. Zuccaro G Jr. Management of the adult patient with acute lower gastrointestinal bleeding. American College of Gastroenterology Practice Parameters Committee. Am J Gastroenterol 1998;93:1202.
24. Strate LL, Syngal S. Timing of colonoscopy: impact on length of hospital stay in patients with acute lower intesti-nal bleeding. Am J Gastroenterol 2003;98:317–22.
25. Caos A, Benner KG, Manier J, et al. Colonoscopy after Golytely preparation in acute rectal bleeding. J Clin Gastroenterol 1986;8:46.
26. Peura DA, Lanza FL, Gostout CJ, et al. The American Col-lege of Gastroenterology. Bleeding Registry: preliminary fi ndings. Am J Gastroenterol 1997;92:924.
27. Mariani G, Pauwels EK, AlSharif A, et al. Radionuclide evaluation of the lower-gastrointestinal tract. Nucl Med 2008;49:776–87.
28. Hunter JM, Pezim ME. Limited value of technetium 99m-labeled red cell scintigraphy in localization of lower gastrointestinal bleeding. Am J Surg 1990;159:504.
29. Ng DA, Opelka FG, Beck DE, et al. Predictive value of technetium Tc 99m-labeled red blood cell scintigraphy for positive angiogram in massive lower gastrointestinal hemorrhage. Dis Colon Rectum 1997;40:471.
30. Olds GD, Cooper GS, Chak A, et al. The yield of bleeding scans in acute lower gastrointestinal hemorrhage. J Clin Gastroenterol 2005;39:273.
31. Lin S, Suhocki PV, Ludg KA, Shetzline MA. Gastrointesti-nal bleeding in adult patients with Meckel’s diverticulum: the role of -technetium 99m pertechnetate scan. South Med J 2002;95:1338–41.
32. Nusbaum M, Baum S. Radiographic demonstration of unknown sites of gastrointestinal bleeding. Surg Forum 1963;14:374–5.
33. Baum S, Athanasoulis CA, Waltman AC. Angiographic diagnosis and control of large-bowel bleeding. Dis Colon Rectum 1974;17:447.
34. Pennoyer WP, Vignati PV, Cohen JL. Mesenteric angiogra-phy for lower gastrointestinal hemorrhage: are there predictors for a positive study? Dis Colon Rectum 1997;40:1014–8.
35. Pennoyer WP, Vignati PV, Cohen JL. Management of angiogram positive lower gastrointestinal hemorrhage: long term follow-up of non-operative treatments. Int J Colorectal Dis 1996;11:279.
36. Rantis PC Jr, Harford FJ, Wagner RH, et al. Technetium-labelled red blood cell scintigraphy: is it useful in acute lower gastrointestinal bleeding? Int J Colorectal Dis 1995;10:210.
37. Athanasoulis CA, Moncure AC, Greenfi eld AJ, et al. Intra-operative localization of small bowel bleeding sites with combined use of angiographic methods and methylene blue injection. Surgery 1980;87:77.
38. Rahn NH 3rd, Tishler JM, Han SY, et al. Diagnostic and interventional angiography in acute gastrointestinal hemorrhage. Radiology 1982;143:361.
39. Clark RA, Colley DP, Eggers FM. Acute arterial gastroin-testinal hemorrhage: effi cacy of transcatheter control. AJR Am J Roentgenol 1981;136:1185.
40. Browder W, Cerise EJ, Litwin MS. Impact of emergency angiography in massive lower-gastrointestinal bleeding. Ann Surg 1986;204:530.
41. Matolo NM, Link DP. Selective embolization for control of gastrointestinal hemorrhage. Am J Surg 1979;138:840.
42. Peck DJ, McLoughlin RF, Hughson MN, et al. Percutane-ous embolotherapy of lower gastrointestinal hemorrhage. J Vasc Interv Radiol 1998;9:747.
43. Gady JS, Reynolds H, Blum A. Selective arterial emboliza-tion for control of lower gastrointestinal bleeding: recom-mendations for a clinical management pathway. Curr Surg 2003;60:344.
44. Leitman IM, Paull DE, Shires GT 3rd. Evaluation and man-agement of massive lower gastrointestinal hemorrhage. Ann Surg 1989;209:175.
45. Funaki B. Microcatheter embolization of lower gastrointes-tinal hemorrhage: an old idea whose time has come. Cardiovasc Intervent Radiol 2004;27:591.
46. Darcy M. Treatment of lower gastrointestinal bleeding: vasopressin infusion versus embolization. J Vasc Interv Radiol 2003;14:535.
47. Bloomfeld RS, Smith TP, Schneider AM, et al. Provocative angiography in patients with gastrointestinal hemorrhage of obscure origin. Am J Gastroenterol 2000;95:2807.
48. Shetzline MA, Suhocki P, Dash R, et al. Provocative angi-ography in obscure gastrointestinal bleeding. South Med J 2000;93:1205.
49. Yamaguchi T, Yoshikawa K. Enhanced CT for initial local-ization of active lower-gastrointestinal bleeding. Abdom Imaging 2003;28:634.
50. Ernst O, Bulois P, Saint-Drenant S, et al. Helical CT in acute lower gastrointestinal bleeding. Eur Radiol 2003;13:114.
51. Sun H, Jin Z, Li X, et al. Detection and localization of active gastrointestinal bleeding with multidetector row compu-ted tomography angiography: a 5-year prospective study in one medical center. J Clin Gastroenterol 2012;46:31–41.
52. Huprich JE, Fletcher JG, Fidler JL, et al. Prospective blinded comparison of wireless capsule endoscopy and
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 19
multiphase CT enterography in obscure gastrointestinal bleeding. Radiology 2011;260:744–51.
53. Lin S, Branch MS, Shetzline M. The importance of indica-tion in the diagnostic value of push enteroscopy. Endos-copy 2003;35:315.
54. Kamesa N, Higuchi K, Masatsugu S, et al. A prospective single-blind trial comparing wireless capsule endoscopy and double--balloon enteroscopy in patients with obscure gastrointestinal bleeding. J Gastroenterol 2008;43:434–40.
55. Pasha SF, Leighton JA, Das A, et al. Double-balloon enter-oscopy and capsule endoscopy have comparable diagnos-tic yield in small-bowel disease: a meta analysis. Clin Gastroenterol Hepatol 2008;6:671–6.
56. Chen X, Ran ZH, Tong JL. A meta-analysis of the yield of capsule endoscopy compared to double-balloon enter-oscopy in patients with small bowel diseases. World J Gastroenterol 2007;13:4372–8.
57. Eaton AC. Emergency surgery for acute colonic haemor-rhage—a retrospective study. Br J Surg 1981;68:109.
58. Setya V, Singer JA, Minken SL. Subtotal colectomy as a last resort for unrelenting, unlocalized, lower gastrointestinal hemorrhage: experience with 12 cases. Am Surg 1992;58:295.
59. Reuben BC, Stoddard G, Glasgow R, et al. Trends and pre-dictors for vagotomy when performing oversew of acute bleeding duodenal ulcer in the United States. J Gastroin-test Surg 2007;11:22.
60. Enestvedt BK, Gralnek IM, Mattek N, et al. An evaluation of endoscopic indications and fi ndings related to nonvari-ceal upper-GI hemorrhage in a large multicenter consor-tium. Gastrointest Endosc 2008;67:422–9.
61. Barkun AN, Cockeram AW, Plourde V, et al. Review arti-cle: acid suppression in non-variceal acute upper gastroin-testinal bleeding. Aliment Pharmacol Ther 1999;13:1565.
62. Graham DY, Hepps KS, Ramirez FC, et al. Treatment of Helicobacter pylori reduces the rate of rebleeding in peptic ulcer disease. Scand J Gastroenterol 1993;28:939.
63. Laine L, Cohen H, Brodhead J, et al. Prospective evaluation of immediate versus delayed refeeding and prognostic value of endoscopy in patients with upper gastrointestinal hemorrhage. Gastroenterology 1992;102:314.
64. Lau JY, Sung JJ, Lam YH, et al. Endoscopic retreatment compared with surgery in patients with recurrent bleeding after initial endoscopic control of bleeding ulcers. N Engl J Med 1999;340:751.
65. Mirsadraee S, Tirukonda P, Nicholson A, et. al. Emboliza-tion for non-variceal upper gastrointestinal tract haemor-rhage: a systematic review. Clin Radiol 2011;66:500–9.
66. Wong TC, Wong KT, Chiu PW, et al. A comparison of angiographic embolization with surgery after failed endo-scopic hemostasis to bleeding peptic ulcers. Gastrointest Endosc 2011;73:900–8.
67. Gisbert JP, Khorrami S, Carballo F, et al. H. pylori eradica-tion therapy vs. antisecretory non-eradication therapy (with or without long-term maintenance antisecretory therapy) for the prevention of recurrent bleeding from peptic ulcer. Cochrane Database Syst Rev 2004;(2):CD004062.
68. Gilliam AD, Speake WJ, Lobo DN, et al. Current practice of emergency vagotomy and Helicobacter pylori eradica-tion for complicated peptic ulcer in the United Kingdom. Br J Surg 2003;90:88.
69. Chan VM, Reznick RK, O’Rourke K, et al. Meta-analysis of highly selective vagotomy versus truncal vagotomy and pyloroplasty in the surgical treatment of uncomplicated duodenal ulcer. Can J Surg 1994;37:457.
70. Csendes A, Braghetto I, Calvo F, et al. Surgical treatment of high gastric ulcer. Am J Surg 1985;149:765.
71. Cook DJ, Guyatt GH, Salena BJ, et al. Endoscopic therapy for acute nonvariceal upper gastrointestinal hemorrhage: a meta-analysis. Gastroenterology 1992;102:139.
72. Hartigan PM, Gebhard RL, Gregory PB. Sclerotherapy for actively bleeding esophageal varices in male alcoholics with cirrhosis. Gastrointest Endosc 1997;46:1.
73. Panes J, Teres J, Bosch J, et al. Effi cacy of balloon tampon-ade in treatment of bleeding gastric and esophageal varices: results in 151 consecutive episodes. Dig Dis Sci 1988;33:454.
74. Avgerinos A, Nevens F, Raptis S, et al. Early administra-tion of somatostatin and effi cacy of sclerotherapy in acute oesophageal variceal bleeds: the European Acute Bleeding Oesophageal Variceal Episodes (ABOVE) randomised trial. Lancet 1997;350:1495.
75. Chavez-Tapia NC, Barrientos-Gutierrez T, Tellez-Avila FI, et al. Antibiotic prophylaxis for cirrhotic patients with upper gastrointestinal bleeding. Cochrane Database Syst Rev 2010;(9):CD002907.
76. Marti-Carvajal AJ, Karakitsiou DE, Salanti G. Human recombinant activated factor VII for upper gastrointestinal bleeding in patients with liver diseases. Cochrane Data-base Syst Rev 2012;(3):CD004887.
77. Khan S, Tudur Smith C, Williamson P, et al. Portosystemic shunts versus endoscopic therapy for variceal rebleeding in patients with cirrhosis. Cochrane Database Syst Rev 2006;(4):CD000553.
78. Warren WD, Henderson JM, Millikan WJ, et al. Distal splenorenal shunt versus endoscopic sclerotherapy for long-term management of variceal bleeding: preliminary report of a prospective, randomized trial. Ann Surg 1986;203:454.
79. Conn HO, Grace ND, Bosch J, et al. Propranolol in the pre-vention of the fi rst hemorrhage from esophagogastric varices: a multicenter, randomized clinical trial. Hepatol-ogy 1991;13:902.
80. Groszmann RJ, Bosch J, Grace ND, et al. Hemodynamic events in a prospective randomized trial of propranolol versus placebo in the prevention of a fi rst variceal hemor-rhage. Gastroenterology 1990;99:1401.
81. Ryan BM, Stockbrugger RW, Ryan JM. A pathophysio-logic, gastroenterologic, and radiologic approach to the management of gastric varices. Gastroenterology 2004;126:1175.
82. Jaroszewski DE, Schlinkert RT, Gray RJ. Laparoscopic splenectomy for the treatment of gastric varices secondary to sinistral portal hypertension. Surg Endosc 2000;14:87.
83. Huang SP, Wang HP, Lee YC, et al. Endoscopic hemoclip placement and epinephrine injection for Mallory-Weiss syndrome with active bleeding. Gastrointest Endosc 2002;55:842.
84. Park CH, Min SW, Sohn YH, et al. A prospective, random-ized trial of endoscopic band ligation vs. epinephrine injection for actively bleeding Mallory-Weiss syndrome. Gastrointest Endosc 2004;60:22.
Scientific American Surgery

12/12
gastro gastrointestinal bleeding — 20
85. Metz CA, Livingston DH, Smith JS, et al. Impact of multi-ple risk factors and ranitidine prophylaxis on the develop-ment of stress-related upper gastrointestinal bleeding: a prospective, multicenter, double-blind, randomized trial. Crit Care Med 1993;21:1844.
86. Tryba M. Prophylaxis of stress ulcer bleeding: a meta-analysis. J Clin Gastroenterol 1991;13 Suppl 2:S44.
87. Kimata M, Kubota T, Otani Y, et al. Gastrointestinal stromal tumors treated by laparoscopic surgery: report of three cases. Surg Today 2000;30:177.
88. Wilhelm D, von Delius S, Burian M, et al. Simultaneous use of laparoscopy and endoscopy for minimally invasive resection of gastric subepithelial masses—analysis of 93 interventions. World J Surg 2008;32:1021–8.
89. Loftus EV, Alexander GL, Ahlquist DA, et al. Endoscopic treatment of major bleeding from advanced gastroduode-nal malignant lesions. Mayo Clin Proc 1994;69:736.
90. Cameron AJ, Higgins JA. Linear gastric erosion: a lesion associated with large diaphragmatic hernia and chronic blood loss anemia. Gastroenterology 1986;91:338.
91. Stylopoulos N, Gazelle GS, Rattner DW. Paraesophageal hernias: operation or observation? Ann Surg 2002;236:492.
92. Norton ID, Petersen BT, Sorbi D, et al. Management and long-term prognosis of Dieulafoy lesion. Gastrointest Endosc 1999;50:762.
93. Stabile BE. Hemorrhagic complications of pancreatitis and pancreatic pseudocysts. In: Beger HG, Warshaw AL, Buchler MW, et al, editors. The pancreas: a clinical text-book. Oxford: Blackwell Scientifi c Publications; 1998. p. 606–13.
94. Sakorafas GH, Sarr MG, Farley DR. Hemosuccus pancre-aticus complicating chronic pancreatitis: an obscure cause of upper gastrointestinal bleeding. Langenbecks Arch Surg 2000;385:124.
95. Lemos DW, Raffetto JD, Moore TC, et al. Primary aorto-duodenal fi stula: a case report and review of the literature. J Vasc Surg 2003;37:686.
96. Walker WE, Cooley DA, Duncan JM, et al. The manage-ment of aortoduodenal fi stula by in situ replacement of the infected abdominal aortic graft. Ann Surg 1986;205:727.
97. Kotsis T, Lioupis C, Tzanis A, et al. Endovascular repair of a bleeding secondary aortoenteric fi stula with acute leg ischemia: a case report and review of the literature. J Vasc Interv Radiol 2006;17:563.
98. Weiner FR, Simon DM. Gastric vascular ectases. Gastroin-test Endosc Clin North Am 1996;6:681.
99. Mathis KL, Farley DR. Operative management of symp-tomatic duodenal diverticula. Am J Surg 2007;193:305.
100. Meyers MA, Alonso DR, Gray GF, et al. Pathogenesis of bleeding colonic diverticulosis. Gastroenterology 1976;71:577.
101. Jensen DM, Machicado GA, Jutabha R, et al. Urgent colonoscopy for the diagnosis and treatment of severe diverticular hemorrhage. N Engl J Med 2000;342:78.
102. Bloomfeld RS, Rockey DC, Shetzline MA. Endoscopic ther-apy of acute diverticular hemorrhage. Am J Gastroenterol 2001;96:2367.
103. McGuire HH Jr. Bleeding colonic diverticula: a reappraisal of natural history and management. Ann Surg 1994;220:653.
104. Longstreth GF. Epidemiology and outcome of patients hospitalized with acute lower gastrointestinal hemorrhage: a population-based study. Am J Gastroenterol 1997;92:419.
105. Zuckerman G, Benitez J. A prospective study of bidirec-tional endoscopy (colonoscopy and upper endoscopy) in the evaluation of patients with occult gastrointestinal bleeding. Am J Gastroenterol 1992;87:62.
106. Boley SJ, Sprayregen S, Sammartano RJ, et al. The patho-physiologic basis for the -angiographic signs of vascular ectasias of the colon. Radiology 1977;125:615.
107. Helmrich GA, Stallworth JR, Brown JJ. Angiodysplasia: characterization, diagnosis, and advances in treatment. South Med J 1990;83:1450.
108. Santos JC Jr, Aprilli F, Guimaraes AS, et al. Angiodysplasia of the colon: endoscopic diagnosis and treatment. Br J Surg 1998;75:256.
109. Peura DA, Lanza FL, Gostout CJ, et al. The American Col-lege of Gastroenterology. Bleeding Registry: preliminary fi ndings. Am J Gastroenterol 1997;92:924.
110. Habr-Gama A, Waye JD. Complications and hazards of gastrointestinal endoscopy. World J Surg 1989;13:193.
111. Trowers EA, Ganga U, Rizk R, et al. Endoscopic hemor-rhoidal ligation: preliminary clinical experience. Gastroin-test Endosc 1998;48:49.
112. Chawla Y, Dilawari JB. Anorectal varices—their frequency in cirrhotic and non-cirrhotic portal hypertension. Gut 1991;32:309.
113. Robert JR, Sachar DB, Greenstein AJ. Severe gastrointesti-nal hemorrhage in Crohn’s disease. Ann Surg 1991;213:207.
114. Crook J, Esche B, Futter N. Effect of pelvic radiotherapy for prostate cancer on bowel, bladder, and sexual function: the patient’s perspective. Urology 1996;47:387.
115. Gaydos LA, Freireich EJ, Mantel N. The quantitative rela-tion between platelet count and hemorrhage in patients with acute leukemia. N Engl J Med 1962;266:905.
116. Mittal R, Spero JA, Lewis JH, et al. Patterns of gastrointes-tinal hemorrhage in hemophilia. Gastroenterology 1985;88:515.
117. Theodoropoulou A, Koutroubakis IE. Ischemic colitis: clinical practive in diagnosis and treatment. World J Gastroenterol 2008;14:7302–8.
118. Chalasani N, Wilcox CM. Etiology and outcome of lower gastrointestinal bleeding in patients with AIDS. Am J Gastroenterol 1998;93:175.
119. Davies NM. Toxicity of nonsteroidal anti-infl ammatory drugs in the large intestine. Dis Colon Rectum 1995;38:1311.
120. Holt S, Rigoglioso V, Sidhu M, et al. Nonsteroidal antiin-fl ammatory drugs and lower gastrointestinal bleeding. Dig Dis Sci 1993;38:1619.
Acknowledgment
Figures 2 and 3 Christine Kenney
Scientific American Surgery