Gametogenesis
33
GAMETOGENESIS AND INFERTILITY CHOYTOO Shiksha 17
-
Upload
shiksha-choytoo -
Category
Health & Medicine
-
view
141 -
download
2
Transcript of Gametogenesis

GAMETOGENESIS AND INFERTILITY
CHOYTOO Shiksha17

OVERVIEW
• GAMETOGENESIS Formation of gametes ( ovum and sperm) from
gonads (testes and ovaries)• Males: Spermatogenesis
SPERMATOGONIA
PRIMARY SPERMATOCYT
E
SECONDARY SPERMATOCYT
E
SPERMATIDS SPERMS

• Females: oogenesis
• Note: Meiosis is the 1st stage of gametogenesis (separation of homologous chromosomes into haploid daughter cells)
Meiosis generates tremendous genetic diversity. How many different types of gametes can be generated by an individual (male or female) with 23 different chromosomes? More than 223 or 8,000,000 different gametes
OOGONIA
PRIMARY OOCYTE
SECONDARY OOCYTE
OVUM ( if fertilization occurs)

• The time of meiosis differs in males and females.
• In males Spermatogonia enters meiosis at puberty and
continues till death
• In females The process is more complex. - The first meiotic division starts before birth but
stops at diplotene stage of prophase I.
- About one month before ovulation, the 1st meiosis is completed and the secondary oocyte is arrested in the metaphase state of meiosis II unless fertilization occurs


SPERMATOGENESIS
•Spermatogenesis can be discussed into 3 stages
-spermatocytogenesis -meiosis I and II -spermiogenesis (there is metamorphosis)

SPERMATOCYTOGENESIS• There are 3 types of spermatogonia
-Dark type A (Ad) - Pale type A (Ap) - Type B
• At puberty, Ad cells starts to divide by mitosis (stimulation of androgen). Ad cells produce more Ad cells.
However, some division gives rise to Ap cells (divides mitotic ally)
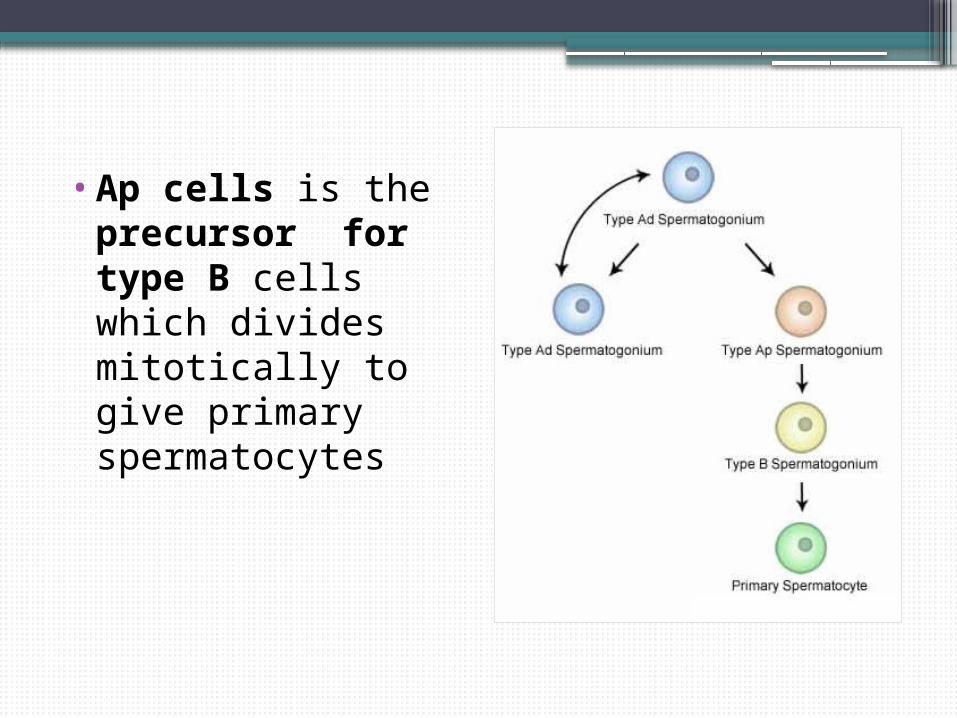
•Ap cells is the precursor for type B cells which divides mitotically to give primary spermatocytes

MEIOSIS I AND II


SPERMIOGENESIS• It is the process whereby
the spermatid undergoes metamorphosis to become sperm cells
• First, during golgi phase the hydrolytic enzymes accumulates in golgi vesicles subsequently coalesce into a single large acrosomal vesicle close to the nucleus.

•The pair of centrioles migrates to the opposite posterior pole. The distal centriole begins to generate a circular arrangement of nine microtubule doublets surrounding a central pair.

• In the cap phase, the acrosomal vesicle flattens and envelops the anterior half of the nucleus to form an acrosomal cap.
•The axonemal complex continues to extend into the developing tail region


CAPACITATION
• When sperms are first expelled in the semen, they are unable to perform their duties in fertilizing the ovum.
• On coming in contact with the fluids of the female genital tract, multiple changes occur that activate the sperm for the final processes of fertilization.
• These collective changes are called capacitation of the spermatozoa.

ACROSOMAL REACTION• Stored in the acrosome of the sperm are
large quantities of hyaluronidase and proteolytic enzymes
• When the ovum is expelled from the ovarian follicle into the fallopian tube, it still carries with it multiple layers of granulosa cells.
• Before a sperm can fertilize the ovum, it must dissolute these granulosa cell layers,and then it must penetrate though the the zona pellucida.
• It does so by releasing the enzymes that creates a pathway for the sperm head to penetrate the ovum.

OOGENESIS• The formation of secondary oocyte from oogania
• The process starts before birth.
• Oogenesis can also be described into 3 phases:
1. follicular phase 2. ovulation 3. Luteal phase

FOLLICULAR PHASEMonth 4 :
Oogonia is grouped in clusters in the cortical part of the
ovaries (SOME of the oogonia differentiate into primary oocyte enters prophase I)
Month 7: Most oogonia are transformed
into primary oocyte. They enters the diplotene state of
prophase I in which they remain until birth

Oogonia grouped in
clusters
Primary oocyte ( in prophase)
Primordial follicle (single layer of follicular cells)

• At birth: Primary oocyte have primodial follicle- throughout
childhood provides nourishment and secretes oocyte maturation inhibiting factors
• At pubery: - Few days before female sexual cycle, FSH and LH (ant pituitary) is secreted
- proliferation of granulosa cells
-spindle cells derived from interstitium of the ovary forms a layer – theca -Theca-two layers: Interna- secretes estrogen Externa- capsule of granulosa cells

• Granulosa cells starts secreting follicular fluid (estrogen)
• The accumulation of fluid forms the atrum within the granulosa cell mass.
• The enlarge follicular cells continues to grow and becomes vesicular follicle
• The ovum also grows in size.

•At the same time Primary oocyte undergo meiosis to
become seconday oocyte.

SECONDARY OOCYTE

OVULATION• The process whereby a
secondary oocyte is discharged from the ovary.
• The outer wall of the follicle swells rapidly and a small area of the capsule protrudes outside – stigma
• Fluid starts to ooze from the stigma causing it to rupture
• The secondary oocyte moves outside carried by the viscous fluid and is surrounded by corona radiata.

LUTEAL PHASE
• Remaining theca and granulosa cells in the ovary are converted to luteal cells- becomes enlarged and filled with yellowish fluid
• Mass is called corpus luteum- well developed vascular supply and secretes progesteron
• 12 days after ovulation ( if there is no fetilisation)
corpus luteum looses secretory functions and yellowish lipid characteristics
• Now called corpus albicans (white). – replaced by connective tissue.


Male Infertility
• Inflamation of testes – bilateral orchitis
Caused by mumps and it results in sterility
•Effect of temperature Inc. in temp cause degradation of
most of cells of seminiferous tubules (excpt spermatogonia)

•Cryptorchidism Failure of testes to
descend from the abdomen to the scrotum during fetal life.
Degeneration of tubular epithelium due to high temp
•Loss of sperm count normal: 120 million
sperm in 3.5 ml of semen

•Effect of sperm morphology and motility on fertility
The sperm count may be normal but about half of the cells are physically abnormal.
Loose motility

Female Infertility
•Fallopian tube may not be patent. ( Damage due to pelvic infections, surgeries, endometriosis..)
Normal Abnormal

•Failure to ovulate due to hormonal disturbances
•Cervical problems Abnormal mucous secretion in cervix-
sperm cannot pass and fertilisation does not occur
•Uterine causes Abnormal anatomy of the uterus; the
presence of polyps and fibroids

•Endometriosis A condition
whereby the endometrium grows in different regions and the tissues respond the same way to hormones as the endometrial lining.
The symptoms are pain and infertility

THANK YOU