
Accreditation Schemes for Energy Assessors Scheme re-launch 25 th February 2010.

GAC 1.1: 2012 - Accreditation Schemes and General Procedure Chapter I. Accreditation schemes and General Procedure 1. Introduction
1. LEPL "The Unified National Body of Accreditation - Accreditation Center" (hereafter GAC) operates on the basis of Georgian under the law "Code on safety and free movement of products" and creates accreditation system in accordance with the international requirements. 2. Accreditation is the official Expert assessment. By granting an accreditation certificate, GAC officially recognizes the competency of the CAB to perform activities determined by the field (specific) of conformity assessment. 1. Terms and Definitions
For purpose of this document the terms and definitions which are stated and explained in the Georgian Law “Code on Safety and Free movement of Products”, SST ISO/IEC 17000 : 2010 and SST ISO IEC 17011 : 2010 are valid. 2. GAC schemes 1. GAC performs assessment of various testing laboratories, calibration laboratories; medical laboratories, product certification bodies, personnel certification bodies performing certification of persons, management systems certification bodies, inspection bodies. 2. GAC forms and uses for its activities accreditation schemes in compliance with international ISO/IEC standards. Each scheme covers:
a) Accreditation criteria (standard according to which the assessment is carried out); b) Accreditation rules and procedures to regulate relations between GAC and applicants; c) International accreditation guides. GAC uses international guides published by the European
3. Accreditation Cooperation (EA), International Laboratory Accreditation Cooperation (ILAC), International accreditation Forum (IAF) and other sectorial international organization documents. Accreditation schemes are available on GAC’s web (www. gac.gov.ge). GAC gives information regarding type of documents (whether the document is mandatory, guidance, informative). The schemes might also include explanatory documents approved by the relevant Technical Committee of the GAC with necessary recommendations. 4. Accreditation schemes are used, for the fields that are regulated by Georgian National legislation as well as based on voluntary choice. 5. The normative documents determined by law shall be used for the fields that are regulated by Georgian National legislation.
3. GAC uses the following schemes: a) The accreditation scheme for testing and calibration laboratories:
Accreditation criteria (assessment document)
SST ISO/IEC 17025 : 2010 “General requirements for the competence of testing and calibration laboratories”
Rule/procedure of GAC GAC 1.3:2012 - Rules and Procedures for accreditation of testing and calibration Laboratories on conformity with SST/ISO/IEC 17025 : 2010 standard.
Guiding documents See on website www.gac.gov.ge in the relevant accreditation scheme

b) Accreditation scheme for medical laboratories:
Criteria for accreditation Accreditation criteria (assessment document)
SST ISO 15189 : 2012/2015 “Medical laboratories - Requirements for quality and competence”.
Rule/procedure of GAC GAC 1.4 : 2012 – Rules and procedures for accreditation medical laboratories on conformity with SST/ISO 15189 : 2012/2015 standard. Annexes - See on website www.gac.gov.ge in the relevantaccreditation scheme
Guiding documents See on website www.gac.gov.ge in the relevant accreditation scheme
c) Accreditation scheme for product certification bodies:
Criteria for accreditation Accreditation criteria (assessment document)
SST ISO/IEC 17065:2012/2014 “General requirements for bodies operating product certification systems”
Rule/procedure of GAC GAC 1.5:2012 – Rules and procedures for accreditation of product certification bodies on conformity with SST ISO/IEC 17065:2012/2014 standard.
Guiding documents See on website www.gac.gov.ge in the relevant accreditation scheme
d) Accreditation scheme for personnel certification bodies:
Criteria for accreditation Accreditation criteria (assessment document)
SST ISO/IEC 17024:2012/2014 “Conformity assessment - General requirements for bodies operating certification of persons”.
Rule/procedure of GAC GAC 1.6:2012 - Rules and procedures for accreditation of certification bodies for persons on Conformity with SST ISO/IEC 17024:2012/2014 standard. Annexes - See on website www.gac.gov.ge in the relevant accreditation scheme
Guiding documents See on website www.gac.gov.ge in the relevant accreditation scheme
e) Accreditation scheme for the bodies performing audit and certification of management systems:

Criteria for accreditation Accreditation criteria (assessment document)
ISO/IEC 17021:2011/2014 “Conformity assessment -Requirements for bodies providing audit and certification of management systems”.
Rule/procedure of GAC GAC 1.7:2012 – Rules and procedures for accreditation of bodies performing audit and certification of management systems on conformity with ISO/IEC 17021:2011/2014 standard.
Guiding documents See on website www.gac.gov.ge in the relevant accreditation scheme
f) Accreditation scheme for accreditation of inspection bodies:
Criteria for accreditation Accreditation criteria (assessment document)
SST ISO/IEC 17020:2010 “Conformity assessment - Requirements for the operation of various types of bodies performing inspection”
Rule/procedure of GAC GAC 1.8:2012 – Rules and procedures for accreditation of inspection bodies on Conformity with SST/ ISO/IEC 17020:2010 standard.
Guiding documents See on website www.gac.gov.ge
g) Accreditation scheme for proficiency testing providers:
Criteria for accreditation Accreditation criteria (assessment document)
SST ISO/IEC 17043:2010/2016 “Conformity assessment -- General requirements for proficiency testing”
Rule/procedure of GAC GAC 1.13:2016 – Rules and procedures for accreditation of proficiency testing providers on conformity with SST/ ISO/IEC 17043:2010/2016 standard. See application forms on website: www.gac.gov.ge
Guiding documents See on website www.gac.gov.ge 1. GAC carries out surveillance and supervision of accredited bodies in accordance with GAC 1.2: 2012 – “Rules of monitoring and surveillance of Accredited Bodies”. 2. Decision on granting accreditation, suspension, renewal, withdrawal, extension or reduction of accreditation scope and other issues related to accreditation process is carried out in accordance with GAC 1.9 – “Rules and procedures of accreditation committee”. 3. GAC maintains the register of the accredited bodies in accordance with GAC 1.10: 2012 – “Rule for Registry of accredited bodies”. 4. Reviewing of appeals and complains submitted to Accreditation Center is carried out in accordance to GAC 1.11: 2012 – Procedures for reviewing appeals and complains”. 5. Use of accreditation logo, accreditation symbol by accredited bodies is regulated by GAC 1.12: 2012 – “Accreditation Logo, accreditation symbol and rules for use”.

6. GAC publishes its policies regarding the participation of inspection bodies and laboratories in PT and ILC on its website – www.gac.gov.ge in accordance with the international requirements.
Chapter II. Accreditation Process 4. General provisions 1. Accreditation Centre carries out the following procedures regarding any accreditation schemes:
a) Assessment of the competency of the applicant body with the aim of the initial accreditation. b) Repeated assessment of the competency of the accredited body with the aim of re-accreditation. c) Granting, suspension, renewal, extension and reduction of scope of accreditation. d) Review of appeals regarding accreditation. e) Actualization of the scope of the accreditation of the accredited body with the aim of making technical
changes to the accreditation scope. f) Periodic surveillance of the accredited body with the aim of meeting accreditation requirements 2.
Assessment of the competency by the Accreditation Centre covers the following stages: a) Acceptance and registration of application for accreditation; b) Resource’s review, decision-making on application; c) Preparation and signing of contract; d) Review of the set of documents submitted with the application; e) Preliminary visit (upon the request of an applicant); f) Documents and records review; g) Preparation for assessment; h) On-site assessment; i) Analysis of findings and assessment report; j) Decision-making on granting of accreditation.
2. The requirements for persons seeking accreditation and accredited persons are determined by the relevant accreditation scheme. Each accreditation scheme specifies particular procedures of the accreditation, considering the peculiarities of the accreditation object. 3. During the accreditation process, the ability to perform in accordance with the documents established by the accreditation scope is also assessed. 5. Application on accreditation 1. Body interested in the accreditation shall complete the appropriate official accreditation application form and submit it to GAC. The application must be accompanied by the set of documents in Georgian prepared in accordance with GAC Rules and Procedures in electronic format on CD (font type: Sylfaen). The application forms and relevant annexes are available on GAC website – “Electronic Application”. 2. Application will be registered at administrative department, if the application and accompanying set of documents are completed in compliance with GAC rules and procedures. 6. Resource review 1. After the registration of application, GAC determines:
a) If the application is a subject to accreditation; b) If the application corresponds to legislation and established requirements.
2. If the requirements above are not met GAC does not carry out the accreditation process and provides a written explanation to the applicant.

3. If the requirements are met, GAC concludes contract on accreditation. Accreditation fee is calculated according to the “Rule for calculation of payment for services provided by the accreditation center”. The accreditation fees are approved by Resolution of the Cabinet of Ministers of Georgia on 13.012017.
4. The applicant is obliged to cover all costs related to the accreditation process despite the result on decision of accreditation.
5. The applicant can pay for registration of application, preliminary visit and for basic activities (initial assessment, surveillance, etc.) separately.
6. GAC appoints a responsible person from the staff for dealing with applications – a case manager. Case manager is responsible for administrative management of the case throughout the whole process of accreditation. Technical side of the accreditation is covered by the lead assessor (including analysis of documentation, on-site assessment, preparing of assessment report). Lead assessor can be a case manager as well, as an invited technical specialist who has been qualified as a lead assessor after the training conducted by the Accreditation Center according to “GAC Training procedure. The Lead assessor should provide the case manager detailed information on the case (including reports, correspondence with the applicant, etc.).
7. Subcontracting the assessment GAC does not use subcontracting in the field of accreditation assessment. 8. Preliminary Visit/Assessment
1. The Accreditation Center carries out a preliminary visit/ assessment. A preliminary visit shall be conducted on the basis on applicant’s written request. With the written request the applicant shall submit an accreditation scope formed in accordance with relevant accreditation scheme. The applicant covers all costs determined for a preliminary visit. 2. Preliminary visit consists of:
a) Revision of application, relevant documents and visit of applicant’s premises by a lead assessor. The GAC director appoints lead assessor/case manager. The goal of the visit is to determine readiness for accreditation. During preliminary visit, lead assessor makes a general overview of standards relevant to the claimed scope of accreditation and management system documentation and current conditions of the applicant to fulfill the accreditation criteria;
b) After preliminary visit, the lead assessor prepares a report and sends it to the applicant by post or by e-mail within 15 business days after finishing the visit.
3. Preliminary visit does not include preparation of any kind of documents or consultations. 4. Results presented in the report of preliminary visit are not reflected on the final decision regarding to accreditation. 9. Preparation for Assessment
1. During preparation for assessment, GAC carries out the following: a) Case manager proposes the formation of the appropriate assessment team. the Assessment team consists
of a lead assessor, invited specialist on contractual basis (technical assessor and/or expert) and in case of necessity a representative of the competent governmental institution (with an observer’s status);
b) Case manager informs the applicant about the composition of the assessment team by means of e-mail or personally. If the applicant does not agree with the composition of assessment team CAB shall provide objective arguments in the written form.
c) It is important to ensure that technical competence of all assessors and experts is in line with the applied scope of accreditation. GAC requires from assessors and experts that they keep confidentiality and impartiality on which an agreement “Declaration of Confidentiality” is made between the GAC

and particular persons. In addition, the representative of the competent governmental institution (if involved) signs a declaration of confidentiality and impartiality;
d) The lead assessor determines particular work for each assessor in order to cover requested scope of accreditation.
e) The accredited (person seeking accreditation) CAB should consider the obligation to allow the GAC representatives to attend the conformity assessment process as observers in the contract it signs with its clients.
f) If lead assessor is competent enough to assess technical field, he/she should also perform as technical assessor.
10. Document and record review
1. Lead assessor coordinates the application review and document analysis conducted by assessment team. 2. Within 25 business days after the payment of accreditation costs, lead assessor sends the results of the document review together with the revealed nonconformities (if any) to the applicant by post or e-mail or by handing hardcopy. The applicant is given 3 months for corrective actions from receiving the information form GAC. 3. The applicant shall provide the corrected documents to the lead assessor for further revision. 4. In case of the applicant’s failure to correct the non-conformities within the period of 3 months, GAC will suggest the applicant on carrying out on-site assessment. If on-site assessment is not carried out because of the applicant (failure to pay fee, unavailability of a written consent on the acceptance of assessment team, etc.) within the period of 6 months from making an agreement, then GAC on the basis of the report of case manager/lead assessor the Accreditation committee makes a decision on termination of the accreditation procedure. Applicant will be informed about the decision by post or e-mail or personally. 5. After termination of the case the body can reapply for the accreditation again.
11. On-site assessment 1. Lead Assessor introduces the assessment program to the applicant 5 days before the on-site assessment and sends to applicant e-mail or informs him/her personally. 2. The on-site assessment of GAC’s competency is conducted through the of GAC assessment team to the applicant. The assessment starts with the opening meeting of the assessment. The lead assessor, all technical assessors and experts are presented at this meeting. 3. During the opening meeting, the lead assessor expresses the aim and criterions of the assessment and clarifies the assessment program together with the applicant. 4. The applicant shall provide an isolated working environment for assessment team, if required. 5. Assessment team assesses the compliance of applicant with accreditation criteria. In order to prepare the objective and reliable assessment report, the sufficient number of fields should be assessed from the applied accreditation scope during the initial assessment. 6. The applicant should provide detailed information regarding the PT and ILC participation results and further participation plan. 7. GAC performs the witnessing of the practical activities of accredited (body seeking accreditation) CAB. The applicant is obligated to allow the GAC assessment team to all working areas/branches. Also, upon request, ensure that the assessment team performs the witnessing and assessment of the practical activities process, within the established accreditation scope. In the case that CAB is unable to find a customer in the certain applied accreditation scope during the accreditation, GAC provides a witnessing of simulated activities. 8. If during the second surveillance visit GAC finds out that CAB did not have client the accreditation scope in certain field will be reduced.

9. If serious nonconformities were revealed the working process and implemented quality management system, the lead assessor should revise the assessment program and increase the timeframe for assessment and volume of activities to be assessed. 10 On-site assessment shall be completed within 6 months after concluding the contract with the applicant. Exceptions can be technical and legislative reasons. 12. Analysis of findings and assessment report
1. After the completion of assessment, the assessment team analyzes the assessment results and determines the compliance of the established scope with standards and accreditation criteria. The assessment team informs the applicant regarding the results on the final management meeting.
2. In case of nonconformities, the lead assessor informs the applicant about their level and writes them in nonconformity sheet. The representatives of CAB may ask questions and express their opinion on results and revealed nonconformities.
3. Grading of Non-conformities includes: a) Minor - non-conformity can be corrected in the process of assessment and/or the correction will be
checked by the Accreditation Center until the next planned surveillance or during its implementation following the agreement between the parties.
b) Serious - In case of the initial assessment if the serious non-conformities are detected accreditation will not be granted until the elimination of non-conformity. In case of the initial assessment, reasonable term (not longer than 6 months) is fixed by mutual agreement to correct non- conformities. Elimination of non-conformities depends on the applicant body. During surveillance, maximum term for the correction of non-conformity of this type can be defined as 1 month.
c) Critical - In case of the initial assessment if the critical non-conformities are detected accreditation is not granted until the correction of non-conformity. In case of the initial assessment a reasonable term (not more than 6 months) is established by mutual agreement for correction of non-conformity. Elimination of non-conformity is the responsibility of the applicant. In case of critical non- conformity the assessment team may request for re-assessment of the object (partially or fully depending on non-conformity), on which a record will be made on the sheet of non-conformity and in the assessment report. The applicant shall cover the expenses of reassessment (fully or partially depending on the re-assessment work). During surveillance, maximum term for correction of non-conformity can be one week. Other term may be defined if the matter is transferred to the technical committee. Critical non-conformity may become a cause for full or partial suspension of the scope of accreditation. If the same critical nonconformity is identified during the surveillance or supervision an during the previous assessment, the accreditation or the person will be suspended for up to 3 months partially or fully depending on the nonconformity. If the accreditation scope is fully suspended, this will cause the withdrawal of accreditation
4. The results of on-site assessment are completed in the form of “assessment report” during the 15 business days after finishing of on-site assessment. The final report shall be signed by the lead assessor and sent to applicant by post or e-mail or handed to the applicant personally. The applicant shall submit a corrective actions plan and the timetable for elimination of the identified non-conformities for review to the lead assessor within 7 business days. Lead assessor assesses the sufficiency and adequacy or the corrective actions, it they are not sufficient, the lead assessor requires additional information.
5. For the purpose of examining the sufficiency and efficiency of the corrective actions, the assessment team may conduct the additional on-site visit. In this case, the applicant should cover the costs of additional assessment partially or completely depending on the scope to be examined.

6. If the applicant fails to correct non-conformities within the timeframe mentioned in the 3rd paragraph of this article, the Accreditation Committee on the basis the Case manager’s report makes a decision to terminate the accreditation process and the CAB (if desired) can reapply for the accreditation.
7. After the completion of the on-site assessment and complete elimination of nonconformities, on the basis of assessment results and agreement with applicant, the assessment team forms the final accreditation scope and submits the case to the accreditation committee for decision-making.
13. Decision-making and Granting Accreditation 1. All finalized cases of initial accreditation assessments, periodic surveillance, reassessments,
extraordinary surveillance actions and visits are closed by the means of decision-making concerning accreditation. Decisions are made according to GAC – 1.9: 2012 “Rules and procedures of accreditation committee”.
2. GAC’s General Director or Deputy General Director reviews accreditation committee decision during 7 business days, and in case of acceptance issue an order on granting accreditation. GAC grants Certificate registered in Accreditation Registry and its annex – Accreditation scope. Information about Accredited Body and it’s scope is placed on GAC’s web-page – www.gac.gov.ge
3. The accreditation certificate is issued with validity for 4 years.. According to the Georgian legislation, Accreditation Certificate belongs to the category of strictly controlled documents.
4. The number of the accreditation certificate has the following structure: 1 2 3 GAC - XX - XXXX– 1 - GAC - the acronym of the Accreditation Center with Latin alphabet; 2 - XX - type of the conformity assessment body:
• TL - testing laboratories; • CL - calibration laboratories; • ML - medical laboratories; • PRC - product certification bodies; • PC- certification bodies for persons; • MSC - management system certification bodies; • IB - inspection bodies; • PT – proficiency testing provider.
3 - XXX - the CAB’s number in the register; Example: testing laboratory - GAC – TL – 001.
5. If the accredited body has several business locations/branches, accreditation certificate will be issued with indication of the address of the head office and its separate locations will be indicated in appropriate scope of accreditation.
6. In case accreditation is granted a case manager develops an annual surveillance plan GAC notifies the CAB. 7. If the accredited body changes location or title, the new accreditation certificate is issued with new
registration number and date, but the validity period of accreditation stays the same. 8. Reference to the accredited status is not allowed after the expiration date of the accreditation certificate,
complete suspension or withdrawal of accreditation. 14. Appeals If the applicant disagrees with GAC decision, it should send the appeal to GAC within one month after the receipt of letter. Appeals are reviewed in accordance with GAC 1.11 - Appeals and Complaints Procedure.

Chapter III. Surveillance and Supervision 15. Periodic surveillance and Supervision
1. After granting accreditation GAC controls the accredited bodies through monitoring. The purpose of
monitoring is to verify that the accredited bodies continue to comply with the accreditation criteria. 2. Within the surveillance, accreditation center conducts following activities:
a) Annual planned surveillance of accredited body by means of assessment; b) Unplanned surveillance of accredited body by means of assessment c) In case of significant changes and amendments in normative acts and accreditation criteria; d) In order to renew the accreditation of the persons, whose accreditation had been suspended on the basis
of their request. e) Ensure that the accredited bodies submit relevant information to GAC on their activities upon the
request (including updates from quality manuals). In case the accredited body doesn’t provide or doesn’t fully provide the requested information, it can be the cause the surveillance or suspension of accreditation.
3. The terms for carrying out annual planned monitoring is every year ±2 months after issuing the accreditation certificate. It should be no longer than 16 months. Accredited person shall apply to Accreditation Centre 2 months before the expiration of one year after the date of issuance of Accreditation certificate. Otherwise, accreditation certificate will be suspended.
4. On the basis of complaints on a specific case of violation of the accreditation requirements submitted by an administrative or civil bodies, or any other body the Accreditation Center carries out supervision of accredited body. The surveillance shall be carried out in case of availability of argumentative information.
5. The surveillance and supervision is carried out in accordance with GAC 1.2:2012 - Rule for Carrying Out surveillance and Supervision of Accredited Bodies.
Chapter IV: Extension, suspension, withdrawal, reduction of the accreditation scope, reaccreditation
16. Extension of the Scope of Accreditation 1. The extension of accreditation scope is performed through accreditation in additional scope. For this
purpose, accredited CAB must submit the application to GAC. 2. The accreditation committee makes a decision to extend CAB’s accreditation scope on the basis of
application, enclosed set of documents and conducted assessment. Accredited body interested to extend the scope of accreditation shall pay the corresponding fees.
3. The assessment performed in order to extend accreditation scope is identical to assessment process of accreditation. The accreditation of additional scope can be conducted during the periodic surveillance.
4. Lead assessor writes the final results in assessment report and transfers it to accreditation committee for decision making.
5. General Director order on accreditation scope extension is issued, relevant changes are made in the annex of the accreditation certificate and the registry of accredited bodies.
17. Suspension, withdrawal or reduction of scope of accreditation
1. Suspending, withdrawing, reducing of scope of accreditation is carried out by the Accreditation Centre in the following circumstances:
a) On the basis of the written application from the accredited body. In this case, renewal of the accreditation is possible through non-periodic surveillance. It is important that the CAB submits written application to the Accreditation Centre and covers relevant costs within 6 months after suspension of the accreditation; otherwise accreditation will be withdrawn.

b) If the accredited body is not able to assure the periodic surveillance within the fixed terms (Once a year ± 2 months after the issue of accreditation certificate). In this case, renewal of accreditation is possible through non-periodic surveillance. The CAB should submit written application to the Accreditation Centre and cover relevant costs within 6 months after suspension of the accreditation, otherwise accreditation will be withdrawn.
c) In case of identification of the critical nonconformities during surveillance or supervision or if the non-conformities were not corrected within the given time terms indicated in the records of nonconformities, the issue will be reviewed by the accreditation committee. Decision will be made on partial or complete suspension of the scope of accreditation of the accredited body depending on the degree of non-conformity. Renewal of accreditation is possible through extension of accreditation (in case of partial suspension of scope) or reaccreditation (in case of withdrawal of accreditation). The CAB should submit written application to the Accreditation Centre and cover relevant costs of assessment.
2. If the same critical nonconformities were identified during surveillance or supervision as on previous assessment, the accreditation will be suspended partially or completely for up to 3 months, depending on the degree of non-conformity. In case of complete suspension, the accreditation will be withdrawn. Renewal of accreditation is possible through extension of accreditation (in case of partial suspension of scope) or reaccreditation (in case of withdrawal of accreditation). The CAB should submit written application to the Accreditation Centre and cover relevant costs of assessment. 3. Upon suspending, withdrawing, reducing, renewal of accreditation is issued order by the General Director of the Accreditation Centre; appropriate changes are made to the registry of the accredited bodies and explanations are send to the accredited CAB by post and/or e-mail or delivered personally on the addresses indicated in the application. 18. Reaccreditation
1. In case of reaccreditation, the assessment of management system and activities is performed and it is similar to initial assessment. 2. It is recommended that the accredited body submits the application (including annexes and documentation regarding the performed changes) at least 6 months before the expiration of the validity of the accreditation to ensure that the accredited body does not have interruption in accreditation. Chapter V. Publicity 19. Publicity and accessibility of information 1. GAC manages the registry of accredited bodies and provides public information to the interested parties on
the basis of written request. The information regarding the accreditation schemes and full list of accredited bodies (with relevant scopes) is published on GAC webpage: gac.gov.ge.
2. Upon GAC request, the accredited bodies are obligated to provide the information regarding their activities to GAC.
3. GAC’s policy regarding the measurement traceability is published on GAC webpage. 4. GAC’s policy regarding participation of laboratories in PT and ILC is published on GAC webpage.
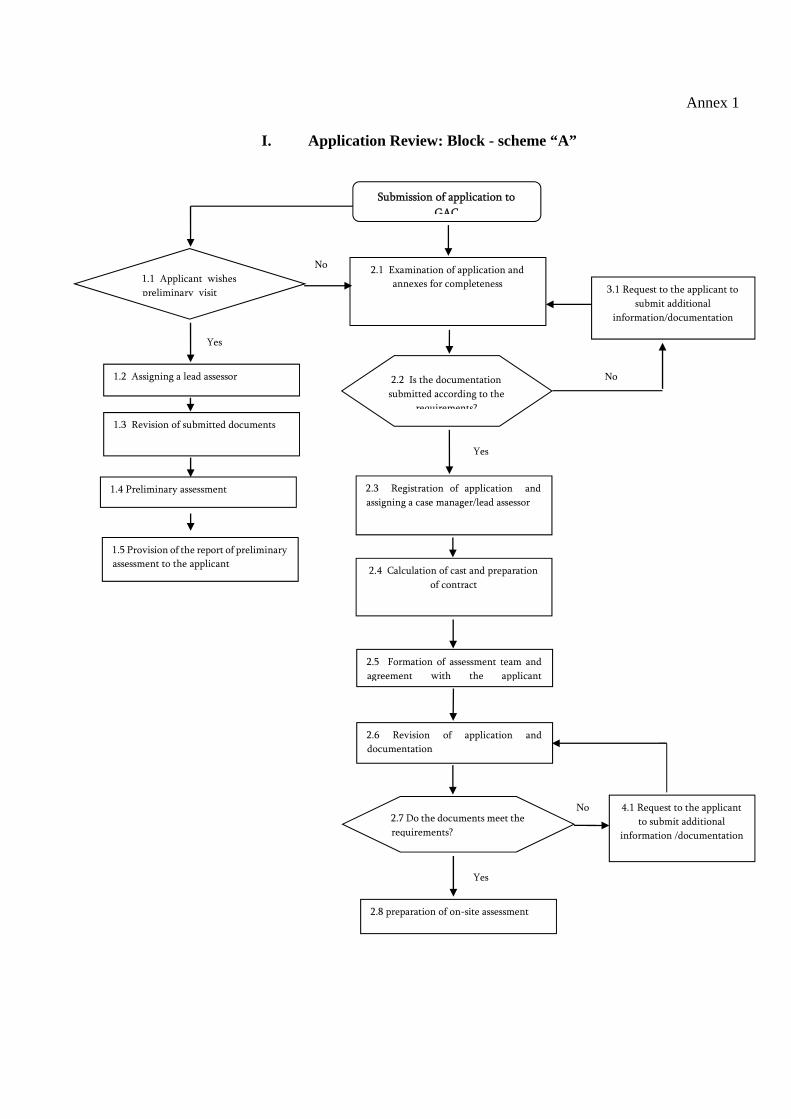
Annex 1
I. Application Review: Block - scheme “A”
4.1 Request to the applicant
to submit additional
information /documentation
3.1 Request to the applicant to
submit additional
information/documentation
Submission of application to
GAC
2.1 Examination of application and
annexes for completeness
2.3 Registration of application and
assigning a case manager/lead assessor
2.4 Calculation of cast and preparation
of contract
1.4 Preliminary assessment
1.1 Applicant wishes
preliminary visit
Yes
2.2 Is the documentation
submitted according to the
requirements?
2.5 Formation of assessment team and
agreement with the applicant
2.6 Revision of application and
documentation
2.7 Do the documents meet the
requirements?
2.8 preparation of on-site assessment
Yes
1.2 Assigning a lead assessor
No
1.3 Revision of submitted documents
1.5 Provision of the report of preliminary
assessment to the applicant
No
Yes
No

II. On-site Assessment. Block scheme “B”
1.1 Initial meeting on-site
1.2 Assessment of documentation, records
and personnel of the applicant
1.3 witnessing of practical activities
1.4 Assessment of working areas/branches
1.5 Identification of non-conformities
1.7 Preparation and delivery of assessment
report in writing to the applicant
1.8 Elaboration of corrective actions by
applicant
1.9 On-site assessment is
required
2.1 Planning additional visit
for on-site assessment
1.10 Documented evidence of carried
out corrective activities
1.11 transferring the case to the
Accreditation Committee for discussion
1.12 Decision on granting accreditation
1.6 Final meeting with the applicant and
informing about non-conformities
No
Yes

III. Decision on accreditation. block scheme “C”
2.1 Appeal is discussed in accordance with
GAC 1.11 – Appeals and Complaints
Procedures
1.1 discussion of the issue on
accreditation committee and decision on
accreditation
1.2 Appeal
1.3 Issue of accreditation certificate and
its appendix with information on the
scope
1.4 Registration of accredited body in the
accredited body’s registry
1.5 Publishing information of the
accredited body on the website
No
Yes

GAC 1.2: 2012 - Rules for Surveillance and Supervision
1. Sphere of Application 1. This document establishes the procedure for surveillance, and supervision of accredited bodies. 2. After granting accreditation, GAC controls the CABs through surveillance. The purpose of periodic
surveillance is to verify that the accredited bodies continue to comply with the accreditation criteria and accreditation schemes.
3. Within the surveillance, accreditation center conducts following activities: a) Annual planned surveillance of accredited body by means of assessment; b) Unplanned surveillance of accredited body by means of assessment
b.a) In case of significant changes and amendments in normative acts and accreditation criteria; b.b) In order to renew the accreditation of the persons, whose accreditation had been suspended on the
basis of their request. c) Ensure that the accredited bodies submit relevant information to GAC on their activities upon the request
(including updates from quality manuals). In case the accredited body doesn’t provide or doesn’t fully provide the requested information, it can be the cause the surveillance or suspension of accreditation.
4. The requirements of the present rule are mandatory to the accredited bodies. 2. Periodic surveillance
1. After granting accreditation, the Accreditation Center carries out surveillance of the accredited bodies in form of annual surveillance procedure. 2. The terms for carrying out annual planned surveillances every year ±2 months after issuing the accreditation certificate. It should be no longer than 16 months. Accredited person shall apply to Accreditation Centre 2 months before the expiration of one year after the date of issuance of Accreditation certificate. Otherwise, accreditation certificate will be suspended. The goal of surveillance is to check the conformity of the activities of accredited bodies with the requirements of the accreditation scheme. 4. The accredited body shall inform the Accreditation Center in writing on their consent or refusal on carrying
out surveillance prior to the starting date of surveillance. With the purpose of carrying out surveillance, the accredited body makes corresponding agreement with the Accreditation Center and pays the established fee.
5. If the accredited body fails to carry out surveillance within the established terms their accreditation will be suspended based on the order of General Director of the Accreditation Center, and corresponding record will be made in the register of the accredited body.
6. Surveillance shall be planned in a way that it covers full scope of accreditation in 4-year term of the validity of accreditation certificate. Certain parts of the scope of accreditation will be assessed each year, the plan of which is agreed previously by the case manager and the accredited body after granting the accreditation. If during the second surveillance visit GAC finds out that CAB did not have client the accreditation scope in certain field will be reduced.
7. The assessment team carries out surveillance of the activities of an applicant in order to make sure that there are no errors between the established requirements and the process of conformity assessment. Surveillance means attendance at the process of implementing practical activities and their assessment.
8. In case of revealed nonconformities, the lead assessor shall inform the applicant of the degree of nonconformities making corresponding records on the sheet of nonconformity. The representatives of applying body are given possibilities to put questions and express their opinions on the results and on nonconformities.
9. The degrees of nonconformities include:

a) Minor – nonconformity can be corrected in the process of assessment and/or the correction will be checked by the Accreditation Center until the next planned surveillance or during its implementation as it will be agreed by the parties; b) Serious – in case of the first assessment accreditation will not be granted until correction of nonconformity. In case of the first assessment, reasonable term (no longer than 6 months) is defined by mutual agreement to correct nonconformities. Correction of nonconformities depends on the applicant body. In case of surveillance, maximum term for correction of the nonconformity of this type can be defined as one month. c) Critical – in case of the first assessment accreditation is not granted until correction of the nonconformity. In case of the first assessment a reasonable term (not more than 6 months) is established by mutual agreement for correction of nonconformity. Correction of nonconformity is the responsibility of the applicant. In case of critical nonconformity, the assessment team may request for re-assessment of an object (partially or fully depending on nonconformity), on which a record will be made on the sheet of nonconformity and in the assessment report. The applicant shall cover the expenses of reassessment (fully or partially depending on the re-assessment work). In case of surveillance, maximum term for correction of nonconformity can be defined as one week. Critical nonconformity may become a cause for full or partial suspension of the scope of accreditation. 10. Critical nonconformity is: a) Nonconformity which is related to the technical activities and which shows incompetence or incorrect
practice; b) Nonconformity in the management that creates threat to the full management system; c) Actions that make direct influence on the results of conformity assessment and in this regard, create threat
to the human health, property or environment. 11. Lead assessor develops the surveillance report in 15 working days after finishing the surveillance procedure
that is signed by the members of the assessment team and the report will be sent to the applicant at the mailing or e-mail address indicated in the application, or will be delivered personally.
12. If the accredited body fails to carry out the planned surveillance within the established terms (every year ±2 months after issuing the accreditation certificate) their accreditation will be suspended. In this case, renewal of accreditation is possible by carrying out unplanned surveillance, on which the applicant submits a written application to the Accreditation Center and pays corresponding fee within 6 months after suspension, or otherwise, the accreditation will be withdrawn.
13. During the monitoring or supervision a). In case of identification of the critical nonconformities during surveillance or supervision or if the nonconformities were not corrected within the given time terms indicated in the records of nonconformities, the issue will be reviewed by the accreditation committee. Decision will be made on partial or complete suspension of the scope of accreditation of the accredited body depending on the degree of non-conformity. Renewal of accreditation is possible through extension of accreditation (in case of partial suspension of scope) or reaccreditation (in case of withdrawal of accreditation). The CAB should submit written application to the Accreditation Centre and cover relevant costs of assessment. b) If the same critical nonconformities were identified during surveillance or supervision as on previous assessment, the accreditation will be suspended partially or completely for up to 3 months, depending on the degree of non-conformity. In case of complete suspension, the accreditation will be withdrawn. Renewal of accreditation is possible through extension of accreditation (in case of partial suspension of scope) or reaccreditation (in case of withdrawal of accreditation). The CAB should submit written application to the Accreditation Centre and cover relevant costs of assessment. 14. In case of suspension of accreditation General Director of the Accreditation Center issues an order, also corresponding record will be made in the register of accredited bodies, and the well-augmented letter will be sent to the other party at the mailing or e-mail address indicated in the application, or will be delivered personally.

15. If the accredited body disagrees with the decision of the Accreditation Center, they shall submit an appeal to the Accreditation Center within one month after receipt of the letter of refusal from the Accreditation Center. The appeal shall be discussed in accordance with GAC 1.11 – Appeals and Complaints Procedure.
3. Unplanned Surveillance 1. GAC conducts unplanned surveillance assessment in case of significant changes and amendments in
normative acts and accreditation criteria and in order to renew the accreditation of the persons, whose accreditation had been suspended on the basis of their request.
2. Unplanned surveillance is conducted on the basis of written agreement between GAC and accredited body 3. During unplanned surveillance, the issues that necessitated carrying out of the unplanned surveillance will
be a subject to assessment. 4. Procedures for carrying out unplanned surveillance are similar to those of planned surveillance. 4. Supervision of Accredited Body 1. On the basis of complaints on a specific case of violation of the accreditation requirements submitted by an
administrative or civil bodies, or any other body the Accreditation Center carries out supervision of accredited body. The surveillance shall be carried out in case of availability of argumentative information.
2. Under the guidance of General Director, the person responsible for the case investigates the materials related to the complaint. In case of necessity, General Director of the Accreditation Center makes decision to organize a visit to the body, and this will be informed to the accredited body.
3. Surveillance is carried out by assessment team appointed by the Accreditation Center. In case of necessity, the Accreditation Center invites the representatives of interested administrative or civil bodies with the status of observers and informs of this to the accredited body. The refusal on carrying out supervision from the side of accreditation body may be followed by suspension, withdrawal or reduction of the scope of accreditation.
4. Results of supervision are recorded in assessment report in which actual state of accredited body is evaluated. The report will be sent to the accredited body at the mailing or e-mail address indicated in the application, or will be delivered personally.
5. The report of supervision will be submitted to the Accreditation Committee for discussion, which can make decision on suspension (full or partial), withdrawal or reduction of the scope of accreditation.
6. See the procedure for suspension or renewal of the scope of accreditation by carrying out of supervision in paragraph 13, Article 2.
7. The Accreditation Center carries out supervision of accredited bodies on their own expenses.

GAC 1.3: 2012 - Rules and Procedures for Accreditation of Calibration and Testing
Laboratories on Conformity with SST ISO/IEC 17025:2010
Chapter 1. General Provisions
Article 1. Sphere of Application
1. The present document has been developed in anticipation with international accreditation
practice and represents a guiding document for accreditation of testing and calibration laboratories.
2. The present document determines specific procedures of the Accreditation Center for assessment
of testing and accreditation laboratories on conformity with SST ISO/IEC 17025:2010 General
Requirements for the Competences of calibration and Testing Laboratories. Accreditation procedures are
carried out in case of payment of established fee.
3. General accreditation procedures are defined in GAC 1.1: 2012.
4. The international guiding docuemtns applied in the accreditation process including documents of
EA, ILAC, IAF and other sectoral international organizations are published on the website of the
Accreditation Center (www.gac.gov.ge) within the scope of full description of corresponding
accreditation scheme with indication of the status of documents.
Article 2. Terms and Definitions
The present document uses terms and definitions applied in the Georgian Code on Products Safety and
Free Movement as well as SST ISO/IEC 17000:2010.
Chapter II. Procedures Related to Accreditation of Calibration and Testing laboratories
Article 3. Application
1. Body interested in the accreditation shall complete the appropriate official accreditation application
form and submit it to GAC. The application must be accompanied by the set of documents in Georgian
prepared in accordance with GAC Rules and Procedures in electronic format on CD (font type: Sylfaen).
The application forms and relevant annexes are available on GAC website – “Electronic Application”.
2. The application submitted for accreditation is registered in the administrative department of the
Accreditation Center provided that the accompanying documents submitted are complete according to
the rules and procedures of the Accreditation Center.
3. An applicant shall submit detailed information on testing/calibration laboratory including
corresponding standards and calibration methods, as well as the results of participation of the laboratory
in proficiency testing and interlaboratory comparison schemes, and the plan for future participation in
interlaboratory comparison schemes.
4. If the scope presented in the application is a subject of accreditation and meets the requirements
determined by legislation the Accreditation Center designates a responsible person – case manager who
represents a member of the personnel of the Accreditation Center who is responsible for the management
and administration of the application throughout the full process of application. Lead assessor is
responsible for the fulfillment of technical part of accreditation (including arrangements for document
analysis, on-site assessment, and preparation of assessment report). Lead assessor can be a case manager
himself or an invited specialist according to the decision of the Accreditation Center.
Article 4. Preliminary Visit/Assessment
1. At the applicant’s request, the Accreditation Center carries out preliminary visit/assessment.
2. Application on preliminary visit shall be considered as ground for carrying out preliminary visit. The
application shall be accompanied with information on the scope of accreditation covered with
corresponding accreditation scheme.
3. The applicant pays a fee determined for preliminary visit.
Article 5. Documents and Records Analysis
1. The assessment team designated by the Accreditation Center and agreed on with the applicant
conducts analysis of documents under the coordination of lead assessor, also assessment of submitted
quality manual and management procedure to determine conformity with SST ISO/IEC 17025:2010
standard. Objective of the accreditation team is to ascertain the claimed scope of accreditation.
2. Lead assessor informs the applicant about the results of document analysis with indication of
revealed nonconformities (if such exist) for the correction of which the applicant is given 3 months after
sending the information.
3. In case of failure to correct nonconformities within the term of three months the Accreditation
Center suggests the applicant on carrying out on-site assessment. If on-site assessment is not carried out
for the reason of the applicant (non-payment of corresponding fee, unavailability of written consent on
the acceptance of assessment team, etc.) within 6 months after making an agreement the accreditation
committee makes a decision on termination of the case on the basis of the report submitted by a lead
assessor on which the applicant will be informed by mail or e-mail indicated in the application, or by
handing a written notification in person.
4. After termination of the case, a body seeking accreditation shall submit a new application on
accreditation at their will.
Article 6. On-site Assessment of Laboratory
1. On-site laboratory assessment begins with the meeting of the assessment team and the
management board of the applicant body on which a lead assessor introduces the applicant in detail on
the purpose and criteria of assessment, also discusses the final program and time necessary for assessment
together with the applicant, also explains that the assessment may require additional time. In case of
necessity, the applicant and/or the assessment team may revise the assessment program by mutual
consent to make certain changes in it.
2. On-the spot laboratory assessment is a an important action through which the assessors shall get
convinced in the competence of the laboratory personnel, shall make sure that the laboratory personnel
has the knowledge of standards and methods that are relevant to its activities, and that the applied tools
and equipment comply. This includes calibration of equipment and their maintenance.
3. Assessment team will assess the effectiveness of the management system in order to get convinced
that there are no errors or ambiguity in test records or in the process of report writing.
4. The plan for participation in proficiency testing will be assessed, as well as frequency of
participation. Results of inter-laboratory comparison will also be assessed.
5. Assessment team will assess the reports of tests and calibration certificates issued. Each method of
testing/calibration covered with the scope of accreditation will also be assessed.
6. Assessment team will observe certain calibration/testing work carried out by laboratory personnel.
See the extent witness audit to be done out in Annex 2 of GAC 1.1 : 2012.
7. When assessing testing/calibration work the assessment team shall assess the abilities of the
laboratory to perform measurement according to uncertainties established for each parameter being
examined.

8. In order to determine the competence of the personnel specific calibration work chosen by
assessors can be assessed.
9. If scope of accreditation covers opinions and interpretations to be included in the test report the
assessors shall assess the corresponding procedure and examine to what extent the procedure is applied in
the practical work of the laboratory. The assessors will also assess the competence, training, knowledge
and experience of responsible personnel. The assessment team shall also assess the conformity of opinions
and interpretations included in the test report against accreditation requirements.
10. Data obtained from on-site assessment that require quick and immediate actions shall be explained
to a client on the spot by the assessment team.
11. If important nonconformities are revealed during assessment in relation with the working process
or the quality management system a lead assessor of the Accreditation Center will make revision of the
assessment program to increase the volume of work to be assessed, as well as time of assessment.
Article 7. Organization with several working areas/branches
1. In the application, the laboratory shall indicate each working area/branch, which is located
remote from headquarters, and where the work is carried out. During the first assessment, the assessment
team will assess each working area/branch where work is carried out.
2. Throughout the 4-year term of accreditation the Accreditation Center will visit and assess each
working area/branch at least once and the headquarters annually in the framework of monitoring.
3. The Accreditation Center shall be informed of any changes in location or activities, or about
founding a new working area/branch in advance before starting activities. Assessment of new working
area/branch shall be discussed and included in monitoring plan.
Article 8. Taking a sample
1. If the laboratory takes samples with the purpose of future testing or calibration on the spot or
beyond its territory, the laboratory should have corresponding plan and procedure of sampling.
2. Assessors will assess whether the described procedure and plan is included in the quality
management system and will make visits to a corresponding working areas/branches where sampling
takes place.
Article 9. Analysis of obtained data and assessment report
1. After completing the assessment, the assessment team makes analysis of assessment results to
determine conformity of claimed scope with corresponding standards and accreditation criteria, which is
presented to the laboratory management on a summarizing meeting. In case of revealed nonconformities
the assessment team informs the applicant of the level of nonconformity which is recorded on the
nonconformities sheet by a lead assessor. The representatives of the applicant are given an opportunity to
put questions or express their opinions about the results of assessment or nonconformities.
2. The results of on-site assessment are developed in the assessment report within 15 working days
after completing the assessment. The report will be signed by a lead assessor and provided to the applicant
by sending it to mail or e-mail address indicated in the application, or will be delivered in person. With
the purpose of eliminating nonconformities, the applicant determines the corrective actions, also terms of
implementation and submits it to a lead assessor within 7 days after on-site assessment. The lead assessor
will organize revision of carried out corrective actions. During the revision, sufficiency and effectiveness
of the corrective actions will be assessed. If corrective actions are insufficient, the lead assessor will
request for additional information.
3. See the gradation of nonconformities in Paragraph 3, Article 12, GAC 1.1:2012.

4. Maximum term for correction of nonconformities (if necessary for reassessment) is no later than 6
months after provision of assessment report.
5. Assessment team can make additional visit to the spot if this is necessary for attesting the
sufficiency and effectiveness of corrective actions carried out to correct nonconformities. In such a case,
the applicant shall pay expenses of reassessment work (in full or its part, adequately to the scope to be
reexamined).
6. If the applicant fails to correct nonconformities within the term indicated in paragraph 4 of the
present article the accreditation committee makes a decision on termination of the accreditation process
based on the report submitted by a case manager, and a body seeking accreditation shall have to submit a
new application for accreditation at their will.
7. After completion of on-site assessment and correction of all nonconformities the assessment team
finally determines the scope of accreditation based on the assessment results and in agreement with the
applicant, and the accreditation committee discusses the question to make decision on granting
accreditation.
Article 10. Monitoring
1. After granting accreditation the Accreditation Center carries out surveillance of accredited bodies
within the framework of planned annual monitoring. The terms for carrying out annual planned
monitoring is every year ±2 months after issuing the accreditation certificate. It should be no longer than
16 months. Accredited person shall apply to Accreditation Centre 2 months before the expiration of one
year after the date of issuance of Accreditation certificate. Otherwise, accreditation certificate will be
suspended.
2. Monitoring is carried out according to GAC 1.2:2012 – Rule for carrying out monitoring and
supervision of accredited bodies, on which the accredited body makes corresponding agreement with the
Accreditation Center and pays established fee.

GAC 1.4 : 2012 - Rules and Procedures for Accreditation of Medical Laboratories on
Conformity with SST ISO 15189:2012/2015
Chapter I. General Provisions
Chapter 1. Sphere of Application
1. The present document has been developed in anticipation with international accreditation practice
and it represents a guiding document for accreditation of medical laboratories.
2. The present document determines specific procedures of the Accreditation Center for assessment
of the conformity of medical laboratories with international standard SST ISO 15189:2012/2015
Medical Laboratories – Specific Requirements for Quality and Competence. Accreditation procedures
are carried out in case of payment of established fee.
3. General accreditation procedures are defined in GAC 1.1 : 2012.
Article 2. Terms and Definitions
The present document uses terms and definitions applied in the Georgian Code on Products Safety
and Free Movement as well as SST ISO/IEC 17000:2010 and SST ISO/IEC 15189:2012/2015.
Chapter II. Procedures Related to Accreditation of Medical Laboratories
Article 3. Application
1. Body interested in the accreditation shall complete the appropriate official accreditation
application form and submit it to GAC. The application must be accompanied by the set of documents
in Georgian prepared in accordance with GAC Rules and Procedures in electronic format on CD (font
type: Sylfaen). The application forms and relevant annexes are available on GAC website – “Electronic
Application”.
2. Application submitted for accreditation is registered in the administrative department of the
Accreditation Center provided that the accompanying documents submitted are complete according
to the rules and procedures of the Accreditation Center.
3. Applicant shall submit detailed information on medical laboratory, as well as the results of
participation of laboratory in proficiency testing and interlaboratory comparison schemes, also plan
for future participation in interlaboratory comparison schemes.
4. If the scope presented in the application is a subject of accreditation and meets the requirements
determined by the legislation the Accreditation Center designates a responsible person – case
manager who represents a member of the personnel of the Accreditation Center who is responsible
for the management and administration of the application throughout the full process of application.
Lead assessor is responsible for the fulfillment of technical part of accreditation (including
arrangements for document analysis, on-site assessment, and preparation of assessment report). Lead
assessor can be a case manager himself or an invited specialist according to the decision of the
Accreditation Center.
Chapter 4. Preliminary Visit/Assessment
1. At the applicant’s will the Accreditation Center carries out preliminary visit/assessment.

2. Application on preliminary visit shall be considered as ground for carrying out preliminary visit.
The application shall be accompanied with information on the scope of accreditation covered by
corresponding accreditation scheme.
3. The applicant pays a fee determined for preliminary visit.
Article 5. Documents and Records Analysis
1. The assessment team designated by the Accreditation Center and agreed with the applicant body
conducts analysis of documents under the coordination of lead assessor, also assessment of submitted
quality manual and management procedure on the conformity with SST ISO/IEC 15189:2012/2015
standard. Objective of the accreditation team is to determine claimed scope of accreditation.
2. Lead assessor informs the applicant about the results of document analysis with indication of
revealed nonconformities (if such exist) for the correction of which the applicant is given 3 months
after sending the information.
3. In case of failure to correct nonconformities within the term of three months, the Accreditation
Center suggests the applicant on carrying out on-site assessment. If on-site assessment is not carried
out for the reason of the applicant (non-payment of corresponding fee, unavailability of written
consent on the acceptance of assessment team, etc.) within 6 months after making an agreement the
accreditation committee makes a decision on termination of the case on the basis of the report
submitted by a lead assessor on which the applicant will be informed by mail or e-mail indicated in
the application or by handing a written notification in person.
4. After termination of the case a person seeking accreditation shall have to submit a new
application on accreditation.
Article 6. On-site Assessment of Laboratory
1. On-site laboratory assessment begins with meeting of the assessment team and the management
board of the applicant body on which the lead assessor introduces the applicant in detail on the
purpose and criteria of assessment, discuss the final program and time period necessary for
assessment, also explains that the assessment may require additional time. In case of necessity, the
applicant and/or the assessment team may revise the assessment program by mutual consent to make
certain changes in it.
2. On-site laboratory assessment is a an important action through which the assessors should get
convinced in the conformity of material and information resources of laboratory and competences of
the personnel in relation with submitted tests.
3. Knowledge of methods selected for corresponding activities of the laboratory will be assessed, as
well as precision of tools that includes calibration and maintenance of equipment. Assessment team
will assess pre-examination and post-examination procedures and will make revision of the list of
contractor laboratories selected by the laboratory.
4. Assessment team will assess the effectiveness of the management system in order to make sure that
there are no errors or ambiguity in test records or in the process of analysis and report writing.
Analytical procedures will also be assessed.
5. Plan for participation in proficiency testing will be assessed, as well as frequency of participation.
Results obtained from participation in inter-laboratory comparison schemes will also be assessed.
6. Assessment team will assess the reports of tests and calibration certificates issued. Each method of
testing/calibration covered by the scope of accreditation will also be assessed.

7. Assessment team will witness particular tests carried out by laboratory personnel. See the amount
of witness work to be carried out in Appendix 2 of GAC 1.1 : 2012.
8. Data obtained from on-site assessment that requires quick and immediate actions shall be
explained to a client on the spot by the assessment team.
Article 7. Organization with several working areas/branches
1. In the application, the laboratory shall indicate each working area/branch, which is located
remote from headquarters where the work is carried out. During the first assessment, the assessment
team will assess each working area/branch where the work is carried out.
2. If important nonconformities are revealed during assessment in relation to working process or
the quality management system the lead assessor of the Accreditation Center will make revision of
the assessment program to increase the volume of work to be assessed, as well as time of assessment.
3. Throughout the 4-year term of accreditation, the Accreditation Center will visit and assess each
working area/branch at least once and the headquarters annually in the framework of monitoring.
4. The Accreditation Center shall be informed of any changes in location or activities, or about
founding a new working area/branch in advance before starting activities. Assessment of new
working area/branch shall be necessarily discussed and included in the monitoring plan.
Article 8. Taking a sample
1. If laboratory takes samples with the purpose of future testing or calibration on the spot or beyond
its territory, the laboratory should have a developed plan and procedure of sampling.
2. Assessors will assess whether the described procedure and plan is included in the quality
management system and will make visits to a corresponding working areas/branches where sampling
takes place.
Article 9. Analysis of obtained data and assessment report
1. After completing the assessment, the assessment team makes analysis of the assessment results to
determine conformity of claimed scope with corresponding standards and accreditation criteria
which is presented to the laboratory management on a summarizing meeting.
2. In case of revealed nonconformities the assessment team informs the applicant of the level of
nonconformity which is recorded on the nonconformities sheet by a lead assessor.
3. The results of on-site assessment are recorded in the form of assessment report within 15 working
days after completing the assessment. The report will be signed by a lead assessor and provided to the
applicant by sending to mail or e-mail address indicated in the application or will be delivered in
person. With the purpose of eliminating nonconformities, the applicant determines the corrective
actions, terms for their implementation and submits it to a lead assessor within 7 days after on-site
assessment. The lead assessor organizes revision of assessment results. During revision, sufficiency
and effectiveness of the corrective actions are assessed. If the corrective actions are insufficient, the
lead assessor will request for additional information.
4. See the gradation of nonconformities in Paragraph 3, Article 12, GAC 1.1:2012.
5. Maximum term for correction of nonconformities (if necessary for reassessment) is no later than
6 months after provision of assessment report.
6. Assessment team can make additional visit to the spot if this is necessary for attesting the
sufficiency and effectiveness of corrective actions carried out to correct nonconformities. In such a

case, the applicant shall pay expenses of reassessment work (on the whole or in part, adequately to
the spheres to be reexamined).
7. If the applicant fails to correct nonconformities within the terms indicated in paragraph 4 of the
present article the accreditation committee makes a decision on termination of the accreditation
process on the basis of the report submitted by a case manager, and the body seeking accreditation
will have to submit a new application for accreditation at their will.
8. After completion of on-site assessment and correction of all nonconformities, the assessment
team finally determines the scope of accreditation based on the assessment results in agreement with
the applicant, and the accreditation committee discusses the question to make decision on granting
accreditation.
Article 10. Monitoring
1. After granting accreditation the Accreditation Center carries out surveillance of accredited bodies
within the framework of planned annual monitoring. The terms for carrying out annual planned
monitoring is every year ±2 months after issuing the accreditation certificate. It should be no longer
than 16 months. Accredited person shall apply to Accreditation Centre 2 months before the
expiration of one year after the date of issuance of Accreditation certificate. Otherwise, accreditation
certificate will be suspended.
2. Monitoring is carried out according to GAC 1.2:2012 – Rule for carrying out monitoring and
supervision of accredited bodies, on which the accredited body makes corresponding agreement with
the Accreditation Center and pays the established fee.

GAC 1.5: 2012 - Rules and Procedures for Accreditation of bodies certifying
products, processes and services on Conformity with SST ISO/IEC 17065:2012/2014
Article 1. Sphere of Application
Chapter I. General Provisions
1. The present document has been developed in anticipation with international accreditation practice
and represents a guiding document for accreditation of Product (including services and processes)
certification bodies.
2. The present document determines specific procedures of the Accreditation Center for assessment of
product (services, processes) certification bodies on conformity with the international standard SST
ISO/IEC 17065:2012/2014 Requirements for bodies certifying products, processes and services.
Accreditation procedures are carried out in case of payment of established fee.
3. General accreditation procedures are defined in GAC 1.1: 2012.
4. The international guiding documents applied in the accreditation process including the documents
of EA, IAF and other sectorial international organizations are published on the website of the
Accreditation Center (www.gac.gov.ge) within the scope of full description of corresponding
accreditation scheme with indication of the status of documents (mandatory, recommended,
informative).
Chapter II. Terms and Definitions
Article 2. Terms and Definitions
The present document uses terms and definitions applied in the Georgian Law on Products Safety and
Free Movement as well as those applied in SST ISO/IEC 17000:2010 and in SST ISO/IEC
17065:2012/2014.
Chapter III. Procedures Related to Accreditation of Certification Body
Article 3. Application
1. Body interested in the accreditation shall complete the appropriate official accreditation application
form and submit it to GAC. The application must be accompanied by the set of documents in Georgian
prepared in accordance with GAC Rules and Procedures in electronic format on CD (font type:
Sylfaen). The application forms and relevant annexes are available on GAC website – “Electronic
Application”.
2. Application submitted for accreditation is registered in the administrative department of the
Accreditation Center if the accompanying documents submitted are complete according to the rules
and procedures of the Accreditation Center.
3. An applicant shall submit detailed information on product (services, processes) certification body
including documentation on quality management, activities, organizational structure, products and
services, applied procedures and certification schemes.
4. If the scope presented in the application is a subject of accreditation and meets the requirements
determined by legislation the Accreditation Center designates a responsible person – case manager
who represents a member of the personnel of the Accreditation Center who is responsible for the
management and administration of the application throughout the full process of application. The
lead assessor is responsible for fulfillment of the technical part of accreditation (including
arrangements for document analysis, on-site assessment, preparation of assessment report). Lead

assessor can be a case manager himself or an invited specialist according to the decision of the
Accreditation Center.
Article 4. Preliminary Visit/Assessment
1. Accreditation Center carries out preliminary visit/assessment on the basis of the applicant’s request.
2. Application on preliminary visit shall be considered as ground for carrying out preliminary visit.
The application shall be accompanied with information on the scope of accreditation required by
corresponding accreditation scheme.
3. The applicant pays a fee determined for preliminary visit.
Article 5. Documents and Records Analysis
1. The assessment team designated by the Accreditation Center and agreed on with the applicant
conducts analysis of documents under the coordination of lead assessor, also assessment of submitted
quality manual and management procedure on conformity with SST ISO/IEC 17065:2012/2014.
Objective of the accreditation team is to ascertain the claimed scope of accreditation.
2 Lead assessor informs the applicant about the results of document analysis with indication of
revealed nonconformities (if such exist) for the correction of which the applicant is given 3 months
after sending the information.
3. In case of failure to correct nonconformities within the term of three months the Accreditation
Center suggests the applicant on carrying out on-site assessment. If on-site assessment is not carried
out for the reason of the applicant (non-payment of corresponding expenses, unavailability of written
consent on the acceptance of assessment team, etc.) within 6 months after making an agreement the
accreditation committee makes a decision on termination of the case on the basis of the report
submitted by a lead assessor on which the applicant will be informed by mail or e-mail address
indicated in the application, or by handing a written notification in person. After termination of the
case, a person seeking accreditation shall have to submit a new application for accreditation.
Article 6. On-site Assessment of Product (Services, Processes) Certification Bodies
1. On-site product certification body assessment begins with the meeting of the assessment team and
the management board of the applicant body on which the lead assessor introduces the applicant in
detail on the purpose and criteria of assessment, defines the final program, the time period necessary
for assessment, also explains that the assessment may require additional time. In case of necessity, the
applicant and/or the assessment team may revise the assessment program by mutual consent to make
certain changes in it.
2. On-site product certification body assessment is a an important action through which the assessors
should get convinced in the competence of the personnel of product certification body and in their
knowledge of corresponding certification schemes and standards related to their activities.
3. Assessment team will supervise the practical work of the applicant in order to make sure that
there are no errors or ambiguity between the requirements of the certification scheme and the
certification process.
4. The assessment team will check the issued certificates and their accuracy against records. If
important nonconformities are revealed during assessment in relation to working process or the
adopted quality management system the lead assessor of the Accreditation Center will make revision
of the assessment program to increase the volume of work to be assessed, as well as time of assessment.

Article 7. Organization with several working areas/branches
1. In the application, the certification body shall indicate each working area/branch, which is
located remote from headquarters, and where the work is carried out. During the first assessment, the
assessment team will assess each working area/branch where work is carried out.
2. Throughout the 4-year term of accreditation, the Accreditation Center will visit and assess each
working area/branch at least once and the headquarters annually in the framework of monitoring.
3. The Accreditation Center shall be informed of any changes in terms of location or activities or
founding a new working area/branch in advance before starting activities. Assessment of new working
area/branch shall be discussed and included in the monitoring plan.
Article 8. Analysis of obtained data and assessment report
1. After completing the assessment, the assessment team makes analysis of assessment results to
determine conformity accreditation criteria and certification schemes claimed in the scope of
accreditation which is presented to the management of certification body on the final meeting.
2. In case of revealed nonconformities the assessment team informs the applicant of the level of
nonconformity which is recorded on the nonconformities sheet by a lead assessor. The representatives
of the applicant are given an opportunity to put questions or express their opinions on the results and
nonconformities.
3. The results of on-site assessment are recorded in the assessment report within 15 working days
after completing the assessment. The report will be signed by a lead assessor and provided to the
applicant by sending it to the mail or e-mail address indicated in the application or will be delivered
in person. With the purpose of eliminating nonconformities, the applicant determines the corrective
actions, terms for their implementation and submits it to a lead assessor within 7 days after on-site
visit. The lead assessor organizes revision of assessment results. During the revision, sufficiency and
effectiveness of the corrective actions are assessed. If the corrective actions are insufficient, the lead
assessor will request for additional information.
4. See the gradation of nonconformities in Paragraph 3, Article 12, GAC 1.1:2012.
5. Maximum term for correction of nonconformities (if necessary for reassessment) is no later than 6
months after provision of assessment report.
6. The assessment team can make additional visit to the spot if this is necessary for attesting the
sufficiency and effectiveness of corrective actions. In such a case, the applicant shall pay expenses of
reassessment work (in full or partially, adequately to the spheres to be reexamined).
7. If the applicant fails to correct nonconformities within the terms indicated in paragraph 4 of the
present article the accreditation committee makes a decision on termination of the accreditation
porocess on the basis of the report submitted by a case manager, and a body seeking accreditation shall
have to submit a new application for accreditation at their will.
8. After completion of on-site assessment and correction of all nonconformities the assessment team
finally determines the scope of accreditation on the basis of the assessment results in agreement with
the applicant, and the accreditation committee discusses the question to make decision on granting
accreditation.
Article 9. Monitoring
1. After granting accreditation the Accreditation Center carries out surveillance of accredited bodies
within the framework of planned annual monitoring. The terms for carrying out annual planned
monitoring is every year ±2 months after issuing the accreditation certificate. It should be no longer
than 16 months. Accredited person shall apply to Accreditation Centre 2 months before the expiration

of one year after the date of issuance of Accreditation certificate. Otherwise, accreditation certificate
will be suspended.
2. Monitoring is carried out according to GAC 1.2:2012 – Rule for carrying out monitoring and
supervision of accredited bodies, on which the accredited body makes corresponding agreement with
the Accreditation Center and pays established fee.

GAC 1.6 : 2012 - Rules and Procedures for Accreditation of Personnel Certification
Bodies on Conformity with SST ISO/IEC 17024:2012/2014
Chapter 1. General Provisions
Article 1. Sphere of Application
1. The present document has been developed in anticipation with international accreditation
practice and represents a guiding document for accreditation of personnel certification bodies.
2. The present document establishes specific procedures of the Accreditation Center for assessment
of personnel certification bodies (including for accreditation of professional organizations of accountants
and/or auditors) on conformity with SST ISO/IEC 17024:2012/2014 General Requirements for Personnel
Certification Bodies. Accreditation procedures are carried out in case of payment of established fee.
3. General accreditation procedures are defined in GAC 1.1: 2012.
4. The international guiding documents applied in the accreditation process including documents of
EA and IAF and other sectorial international organizations are published on the website of the
Accreditation Center (www.gac.gov.ge) within the scope of full description of corresponding
accreditation scheme with indication of the status of the documents (mandatory, recommended,
informative).
Article 2. Terms and Definitions
The present document uses terms and definitions applied in the Georgian Code on Products Safety
and Free Movement as well as SST ISO/IEC 17000:2010 and SST ISO/IEC 17024:2012/2014.
Chapter II. Procedures Related to Accreditation of Personnel Certification Bodies
Article 3. Application
1. Body interested in the accreditation shall complete the appropriate official accreditation
application form and submit it to GAC. The application must be accompanied by the set of documents in
Georgian prepared in accordance with GAC Rules and Procedures in electronic format on CD (font type:
Sylfaen). The application forms and relevant annexes are available on GAC website – “Electronic
Application”.
2. The application submitted for accreditation is registered in the administrative department of the
Accreditation Center if the accompanying documents submitted are complete according to the rules and
procedures of the Accreditation Center.
3. An applicant shall submit detailed information on personnel certification body including
documents on quality management, its activities, structure, applied certification schemes and procedures.
4. If the scope presented in the application is a subject of accreditation and meets the requirements
determined by legislation the Accreditation Center designates a responsible person – case manager who
represents a member of the personnel of the Accreditation Center and who is responsible for the
management and administration of the application throughout the full process of application. Lead
assessor is responsible for fulfillment of the technical part of accreditation (including analysis of
documents, on-site assessment, and preparation of assessment report). Lead assessor can be a case manager
himself or invited specialist according to the decision of the Accreditation Center.
Article 4. Preliminary Visit/Assessment
1. At the applicant’s request, the Accreditation Center carries out preliminary visit/assessment.
2. Application on preliminary visit shall be considered as ground for carrying out preliminary visit.
The application shall be accompanied with information on the scope of accreditation anticipated by
corresponding accreditation scheme.
3. The applicant shall pay a fee established for preliminary visit.
Article 5. Documents and Records Analysis
1. The assessment team designated by the Accreditation Center and agreed with the applicant
conducts analysis of documents under the coordination of lead assessor, also assessment of submitted
quality manual and management procedure on conformity with SST ISO/IEC 17024:2012/2014 standard.
The objective of the assessment team is to ascertain the claimed scope of accreditation.
2. Lead assessor informs the applicant about the results of document analysis with indication of
revealed nonconformities (if such exist) for the correction of which the applicant is given 3 months after
sending the information.
3. In case of failure to correct nonconformities within the term of three months the Accreditation
Center suggests the applicant on carrying out on-site assessment. If on-site assessment is not carried out
for the reason of the applicant (non-payment of corresponding fee, unavailability of written consent on
acceptance of assessment team, etc.) within 6 months after making an agreement the accreditation
committee makes a decision on termination of the case on the basis of the report submitted by a lead
assessor which will be informed to the applicant by mail or e-mail address indicated in the application, or
by handing a written notification in person.
4. After termination of the case, a person seeking accreditation shall have to submit a new
application on accreditation.
Article 6. On-site Assessment of Personnel Certification Bodies
1. On-site assessment of personnel certification body begins with meeting of the assessment team
and the management board of the applicant body on which the lead assessor introduces the applicant in
detail on the purpose and criteria of assessment, defines the final program, time necessary for assessment,
and explains that the assessment may require additional time. In case of necessity, the applicant and/or
the assessment team may revise the assessment program by mutual consent to make certain changes in it.
2. On-the spot laboratory assessment is a an important action through which the assessors should get
convinced in the competence of the personnel of personnel certification body and in their knowledge of
corresponding certification schemes and standards related to their activities.
3. Assessment team will observe the practical work of the applicant in order to make sure that there
are no errors or ambiguity between the requirements of the certification scheme and the certification
process. See the amount of witnessed work in Appendix 2 of GAC 1.1:2012.
4. The assessment team will check the issued certificates and their accuracy against available records.
If important nonconformities are revealed during the assessment in relation to working process or the
adopted quality management system the lead assessor of the Accreditation Center will make revision of
the assessment program to increase the volume of work to be assessed, as well as time of assessment.
Article 7. Organization with several working areas/branches
1. In the application, the certification body shall indicate each working area/branch, which is remote
from headquarters, and where the work is carried out. During the first assessment, the assessment team
will assess each working area/branch where work is carried out.
2. Throughout the 4-year term of accreditation, the Accreditation Center will visit and assess each
working area/branch at least once and the headquarters annually in the framework of monitoring.
3. The Accreditation Center shall be informed of any changes in terms of location or activities or
founding a new working area/branch in advance before starting activities. Assessment of new working
area/branch shall be discussed and included in the plan of monitoring work.
Article 9. Analysis of obtained data and assessment report
1. After completing the assessment, the assessment team makes analysis of assessment results to
determine conformity accreditation criteria and certification schemes claimed in the scope of
accreditation which is presented to the management of certification body on the final meeting.
2. In case of revealed nonconformities the assessment team informs the applicant of the level of
nonconformity which is recorded on the nonconformities sheet by a lead assessor. The representatives of
the applicant are given an opportunity to put questions or express their opinions on the results and
nonconformities.
3. The results of on-site assessment are recorded in the assessment report within 15 working days
after completing the assessment. The report will be signed by a lead assessor and provided to the applicant
by sending it to the mail or e-mail address indicated in the application or will be delivered in person.
With the purpose of eliminating nonconformities, the applicant determines the corrective actions, terms
for their implementation and submits it to a lead assessor within 7 days after on-site visit. The lead
assessor organizes revision of assessment results. During the revision, sufficiency and effectiveness of the
corrective actions are assessed. If the corrective actions are insufficient, the lead assessor will request for
additional information.
4. Maximum term for correction of nonconformities (if necessary for reassessment) is no later than 6
months after provision of assessment report.
5. The assessment team can make additional visit to the spot if this is necessary for attesting the
sufficiency and effectiveness of corrective actions. In such a case, the applicant shall pay expenses of
reassessment work (in full or partially, adequately to the spheres to be reexamined).
6. If the applicant fails to correct nonconformities within the terms indicated in paragraph 4 of the
present article the accreditation committee makes a decision on termination of the accreditation process
based on the report submitted by a case manager, and a body seeking accreditation shall have to submit a
new application for accreditation at their will.
7. After completion of on-site assessment and correction of all nonconformities, the assessment team
finally determines the scope of accreditation based on the assessment results in agreement with the
applicant, and the accreditation committee discusses the question to make decision on granting
accreditation.
Article 9. Monitoring
1. After granting accreditation the Accreditation Center carries out surveillance of accredited bodies
within the framework of planned annual monitoring. The terms for carrying out annual planned
monitoring is every year ±2 months after issuing the accreditation certificate. It should be no longer than
16 months. Accredited person shall apply to Accreditation Centre 2 months before the expiration of one

year after the date of issuance of Accreditation certificate. Otherwise, accreditation certificate will be
suspended.
2. Monitoring is carried out according to GAC 1.2:2012 – Rule for Carrying out Monitoring and
Supervision of Accredited Bodies, on which the accredited body makes corresponding agreement with
the Accreditation Center and pays established fee.

GAC 1.7: 2012 - Rules and Procedures for Accreditation of Audit and Management
Certification Bodies on Conformity with SST ISO/IEC 17021:2012/2014
Chapter I. General Provisions
Article 1. Sphere of Application
1. The present document has been developed in anticipation with international accreditation practice
and represents a guiding document for accreditation of audit and management certification bodies.
2. The document establishes specific procedures of the Accreditation Center for assessment of audit
and management certification bodies on conformity with SST ISO/IEC 17021:2011/2014. Accreditation
procedures are carried out in case of payment of established fee.
3. General accreditation procedures are defined in GAC 1.1: 2012.
4. International guiding documents applied in the accreditation process including the documents of EA
and IAF are published on the website of the Accreditation Center (www.gac.gov.ge) within the scope
of the full description of corresponding accreditation scheme with indication of the status of the
documents (mandatory, recommended, informative).
Article 2. Terms and Definitions
The present document uses terms and definitions applied in the Georgian Code on Products
Safety and Free Movement as well as SST ISO/IEC 17000:2010 and SST ISO/IEC 17021:2011/2014.
Article 3. Application
1. Body interested in the accreditation shall complete the appropriate official accreditation application
form and submit it to GAC. The application must be accompanied by the set of documents in Georgian
prepared in accordance with GAC Rules and Procedures in electronic format on CD (font type:
Sylfaen). The application forms and relevant annexes are available on GAC website – “Electronic
Application”.
2. Application submitted for accreditation is registered in the administrative department of the
Accreditation Center if the accompanying documents submitted are complete according to the rules
and procedures of the Accreditation Center.
3. Applicant shall submit detailed information on audit and management certification body including
documents on quality management, its activities, structure, applied certification schemes and
procedures. For accreditation of food safety management system certification bodies corresponding EA
guideline is applied.
4. If the scope presented in the application is a subject of accreditation and meets the requirements
determined by legislation the Accreditation Center designates a responsible person – case manager
who represents a member of the personnel of the Accreditation Center and who is responsible for the
management and administration of the application throughout the full process of application. Lead
assessor is responsible for fulfillment of the technical part of accreditation (including document
analysis, on-site assessment, preparation of assessment report). Lead assessor can be a case manager
himself or an invited specialist according to the decision of the Accreditation Center.

Article 4. Preliminary Visit/Assessment
1. Accreditation Center carries out preliminary visit/assessment on the basis of the applicant’s request.
2. Application on preliminary visit shall be considered as ground for carrying out preliminary visit.
The application shall be accompanied with information on the scope of accreditation anticipated by
corresponding accreditation scheme.
3. The applicant shall pay a fee established for preliminary visit.
Article 5. Documents and Records Analysis
1. The assessment team designated by the Accreditation Center and agreed with the applicant
conducts analysis of documents under the coordination of lead assessor, also assessment of submitted
quality manual and management procedure on conformity with SST ISO/IEC 17021:2011/2014
standard.
2. Lead assessor informs the applicant about the results of document analysis with indication of
revealed nonconformities (if such exist) for the correction of which the applicant is given 3 months after
sending the information.
3. In case of failure to correct nonconformities within the term of three months the Accreditation
Center suggests the applicant on carrying out on-site assessment. If on-site assessment is not carried
out for the reason of the applicant (non-payment of corresponding expenses, unavailability of written
consent on acceptance of assessment team, etc.) within 6 months after making an agreement the
accreditation committee makes a decision on termination of the case on the basis of the report
submitted by a lead assessor on which the applicant will be informed by mail or e-mail address
indicated in the application, or by handing a written notification in person.
4. After termination of the case, a person seeking accreditation shall have to submit a new application
on accreditation.
Article 6. On-site Assessment of Audit and Management Certification Bodies
1. On-site assessment of audit and management certification body begins with meeting of the
assessment team and the management board of the applicant body on which the lead assessor
introduces the applicant in detail on the purpose and criteria of assessment, defines the final program,
time necessary for assessment, also explains that the assessment may require additional time. In case of
necessity, the applicant and/or the assessment team may revise the assessment program to make certain
changes in it by mutual consent.
2. On-site assessment is an important action through which the assessors should examine the
competence of the personnel of management certification body and their knowledge of corresponding
certification schemes and standards related to their activities. The assessment team shall assess each
direction defined by the scope of accreditation.
3. Assessment team will observe the practical work of the applicant in order to make sure that there
are no errors or ambiguity between the requirements of the certification scheme and the certification
process.
4. The assessment team will check the issued certificates and their accuracy against available records.
Article 7. Organization with several working areas/branches
1. In the application, the certification body shall indicate each working area/branch that is remote
from headquarters, and where the work is carried out. During the first assessment, the assessment
team will conduct assessment in accordance with IAF Mandatory Document for the Certification of
Multiple Sites Based on Sampling.
2. If, during the assessment of the working area/branch, serious nonconformities were identified
regarding the working process, implemented quality management system, the lead assessor should
review the assessment program and increase the terms and quantity of activities to be assessed.
3. Throughout the 4-year term of accreditation, the Accreditation Center will visit and assess each
working area/branch and the headquarters in accordance with IAF Mandatory Document for the
Certification of Multiple Sites Based on Sampling.
4. The Accreditation Center shall be informed of any changes in terms of location or activities or
founding a new working area/branch in advance before starting activities. Assessment of new working
area/branch shall be discussed and included in the plan of monitoring work.
Article 8. Analysis of obtained data and assessment report
1. After completing the assessment, the assessment team makes analysis of assessment results to
determine conformity accreditation criteria and certification schemes claimed in the scope of
accreditation which is presented to the management of certification body on the final meeting.
2. In case of revealed nonconformities the assessment team informs the applicant about the level of
nonconformity which is recorded on the nonconformities sheet by a lead assessor.
3. The results of on-site assessment are recorded in the form of assessment report within 15 working
days after completing the assessment. The report will be signed by a lead assessor and provided to the
applicant by sending it to the mail or e-mail address indicated in the application or will be delivered in
person. With the purpose of eliminating nonconformities the applicant determines the corrective
actions, terms for their implementation and submits it to a lead assessor within 7 days after on-site
visit. The lead assessor makes arrangement for their revision. During revision, sufficiency and
effectiveness of the corrective actions are assessed. If the corrective actions are insufficient, the lead
assessor will request for additional information.
4. See the gradation of nonconformities in Paragraph 3, Article 12, GAC 1.1:2012.
5. Maximum term for the correction of nonconformities (if necessary for reassessment) is no later
than 6 months after provision of assessment report.
6. The assessment team can make additional visit to the spot if this is necessary for attesting the
sufficiency and effectiveness of corrective actions for nonconformities. In such a case, the applicant
shall pay expenses of reassessment work (in full or partially, adequately to the spheres to be
reexamined).
7. If the applicant fails to correct nonconformities within the terms indicated in paragraph 4 of the
present article the accreditation committee makes a decision on termination of the accreditation
process based on the report submitted by a case manager, and a body seeking accreditation shall have
to submit a new application for accreditation at their will.

8. After completion of on-site assessment and correction of all nonconformities the assessment team
finally determines the scope of accreditation based on the assessment results and in agreement with the
applicant, and the accreditation committee discusses the issue to make decision on granting
accreditation.
Article 9. Monitoring
1. After granting accreditation the Accreditation Center carries out surveillance of accredited bodies
within the framework of planned annual monitoring. The terms for carrying out annual planned
monitoring is every year ±2 months after issuing the accreditation certificate. It should be no longer
than 16 months. Accredited person shall apply to Accreditation Centre 2 months before the expiration
of one year after the date of issuance of Accreditation certificate. Otherwise, accreditation certificate
will be suspended.
2. Monitoring is carried out according to GAC 1.2:2012 – Rule for carrying out monitoring and
supervision of accredited bodies, on which the accredited body makes corresponding agreement with
the Accreditation Center and pays the established fee.
GAC 1.8: 2012 - Rules and Procedures for Accreditation of Inspection Bodies
on Conformity with SST ISO/IEC 17020:2012/2013
Chapter 1. General Provisions
Article 1. Sphere of Application
1. The present document has been developed in anticipation with international accreditation practice
and represents a guiding document for accreditation of inspection bodies.
2. The document establishes specific procedures of the Accreditation Center for assessment of
Inspection bodies on conformity with SST ISO/IEC 17020:2012/2013 General Criteria for Activities of
Different Types of Inspection Bodies. Accreditation procedures are carried out in case of payment of
established fee.
3. In order to conduct inspections in the spheres regulated by Georgian legislation (where inspection
of particular entity is mandatory), the accredited inspection body is required to be of A type (Except
inspection bodies that conduct inspection of Control equipment (tachograph), that records vehicle
motion parameters. These inspection bodies can be of C type.) as it is required by SST ISO/IEC
17020:2012/2013, and to meet the requirements of corresponding legislation.
4. Accreditation of inspection a body performing inspection of vehicles and measurement equipment
is carried out according to the accreditation scheme of inspection bodies.
5. General accreditation procedures are defined in GAC 1.1: 2012.
Article 2. Insurance of Inspection Body
1. Inspection body is required to have adequate responsibility insurance.
2. According to the Georgian Law Code on Product Safety and Free Movement the accredited
inspection body carrying out regular inspection of the safety of certain entities is required to have
adequate responsibility insurance in addition to the insurance of inspection bodies of OECD member
states the responsibility insurance of which covers territory of Georgia as well.
Chapter II. Terms and Definitions
Article 3. Terms and Definitions
The present document uses terms and definitions applied in the Georgian Code on Products
Safety and Free Movement as well as SST ISO/IEC 17000:2010 and SST ISO/IEC 17010:2012/2013.
Chapter III. Procedures Related to Accreditation of Inspection Body
Article 4. Application
1. Body interested in the accreditation shall complete the appropriate official accreditation application
form and submit it to GAC. The application must be accompanied by the set of documents in Georgian
prepared in accordance with GAC Rules and Procedures in electronic format on CD (font type:
Sylfaen). The application forms and relevant annexes are available on GAC website – “Electronic
Application”.

2. The application submitted for accreditation is registered in the administrative department of the
Accreditation Center provided that the accompanying documents submitted are complete according
to the rules and procedures of the Accreditation Center.
3. An applicant shall submit detailed information on inspection body including documentation on
quality management, activities, organizational structure, products and services, applied procedures
and certification schemes.
4. If the scope presented in the application is a subject of accreditation and meets the requirements
determined by legislation the Accreditation Center designates a responsible person – case manager
who represents a member of the personnel of the Accreditation Center and who is responsible for the
management and administration of the application throughout the full process of application. Lead
assessor is responsible for the fulfillment of the technical part of accreditation (including
arrangements for document analysis, on-site assessment, preparation of assessment report). Lead
assessor can be a case manager himself or an invited specialist according to the decision of the
Accreditation Center.
Article 5. Preliminary Visit/Assessment
1. At the applicant’s request, the Accreditation Center carries out preliminary visit/assessment.
2. Application on preliminary visit shall be considered as ground for carrying out preliminary visit.
The application shall be accompanied with information on the scope of accreditation anticipated by
corresponding accreditation scheme.
3. The applicant shall pay a fee established for preliminary visit.
Article 6. Documents and Records Analysis
1. The assessment team designated by the Accreditation Center and agreed with the applicant
conducts analysis of documents under the coordination of lead assessor, also assessment of submitted
quality manual and management procedure on conformity with SST ISO/IEC 17020:2012/2013
standard. Objective of the accreditation team is to define the claimed scope of accreditation.
2. The applicant shall submit detailed information on the results of participation in proficiency
3. Testing and interlaboratory comparison schemes (if the activities involve testing), also plan for
future participation.
4. Lead assessor informs the applicant about the results of document analysis with indication of
revealed nonconformities (if such exist) for the correction of which the applicant is given 3 months
after sending the information.
5. In case of failure to correct nonconformities in the term of three months the Accreditation Center
suggests the applicant on carrying out on-site assessment. If on-site assessment is not carried out for
the reason of the applicant (non-payment of corresponding expenses, unavailability of written
consent on acceptance of assessment team, etc.) within 6 months after making an agreement the
accreditation committee makes a decision on termination of the case on the basis of the report
submitted by a lead assessor on which the applicant will be informed by mail or e-mail address
indicated in the application or by handing a written notification in person.
6. After termination of the case a person seeking accreditation shall have to submit a new application
on accreditation.

Article 7. On-site Assessment of Inspection Bodies
1. On-site laboratory assessment begins with meeting of the assessment team and the management
board of applicant body on which the lead assessor introduces the applicant in detail on the purpose
and criteria of assessment, defines the final program, time necessary for assessment together with the
applicant, also explains that the assessment may require additional time. In case of necessity, the
applicant and/or the assessment team may revise the assessment program to make certain changes in it
by mutual consent.
2. On-the spot laboratory assessment is a an important action through which the assessors should get
convinced in the competence of the personnel of inspection body and their knowledge of
corresponding certification schemes and standards related to their activities.
3. Assessment team will observe the practical work of the applicant in order to make sure that there
are no errors or ambiguity between the requirements of the certification scheme and the certification
process. See the amount of witnessed work in Appendix 2 of GAC 1.1:2012.
4. The assessment team will witness inspection work carried out by inspection body, their
competences, also will examine conformity of all necessary means and equipment with their purpose,
their calibration and maintenance. Witnessing means attendance of the assessment team on practical
work within the limits of the scope of accreditation, and making assessment of performed work.
5. Results of participation in proficiency testing and inter-laboratory comparison schemes will be
assessed, as well as corrective actions (if such actions were carried out).
6. In cases where none of the inspectors is able to cover particular scope entirely, more than one
inspector will be assessed for that particular scope.
7. If serious nonconformities are revealed in relation with working process or quality management
system a lead assessor of the Accreditation Center will make revision of the assessment program to
increase the volume of the work to be assessed and corresponding time period.
Article 8. Organization with several working areas/branches
1. In the application, the inspection body shall indicate each working area/branch that is remote of
headquarters, and where the work is carried out. During the first assessment, the assessment team
will assess each working area/branch where work is carried out.
2. Throughout the 4-year term of accreditation, the Accreditation Center will visit and assess each
working area/branch at least once and the headquarters annually in the framework of monitoring.
3. The Accreditation Center shall be informed of any changes in terms of location or activities or
founding a new working area/branch in advance before starting of activities. Assessment of new
working area/branch shall be necessarily discussed and included in the plan of monitoring work.
Article 9. Analysis of obtained data and assessment report
1. After completing the assessment the assessment team makes analysis of assessment results to
determine conformity of accreditation criteria with the inspection schemes claimed in the scope of
accreditation which is presented to the management of inspection body on the final meeting.
2. In case of revealed nonconformities the assessment team informs the applicant of the level of
nonconformity which is recorded on the nonconformities sheet by a lead assessor. The

representatives of the applicant are given an opportunity to put questions or express their opinions on
the results and nonconformities.
3. The results of on-site assessment are developed in form of assessment report within 15 working
days after completing the assessment. The report will be signed by a lead assessor and provided to the
applicant by sending it to the mail or e-mail address indicated in the application or will be delivered
in person. With the purpose of correction of nonconformities, the applicant determines the
corrective actions, terms for their implementation and submits it to a lead assessor within 7 days after
on-site visit. The lead assessor makes arrangement for their revision. During the revision, sufficiency
and effectiveness of the corrective actions are assessed. If the corrective actions are insufficient, the
lead assessor will request for additional information.
4. See the gradation of nonconformities in Paragraph 3, Article 12, GAC 1.1:2012.
5. Maximum term for correction of nonconformities (if necessary for reassessment) is no later than 6
months after provision of assessment report.
6. The assessment team can make additional visit to the spot if this is necessary for attesting the
sufficiency and effectiveness of corrective actions. In such a case, the applicant shall pay expenses of
reassessment work (in full or partially, adequately to the spheres to be reexamined).
7. If the applicant fails to correct nonconformities within the term indicated in paragraph 4 of the
present article the accreditation committee makes a decision on termination of the accreditation
process on the basis of the report submitted by a case manager, and a body seeking accreditation shall
have to submit a new application for accreditation at their will.
8. After completion of on-site assessment and correction of all nonconformities, the assessment team
finally determines the scope of accreditation based on the assessment results and in agreement with
the applicant, and the issue is discussed by the accreditation committee to make decision on granting
accreditation.
Article 10. Monitoring
1. After granting accreditation the Accreditation Center carries out surveillance of accredited bodies
within the framework of planned annual monitoring. The terms for carrying out annual planned
monitoring is every year ±2 months after issuing the accreditation certificate. It should be no longer
than 16 months. Accredited person shall apply to Accreditation Centre 2 months before the
expiration of one year after the date of issuance of Accreditation certificate. Otherwise, accreditation
certificate will be suspended.
2. Monitoring is carried out according to GAC 1.2:2012 – Rule for Carrying out Monitoring and
Supervision of Accredited Bodies, on which the accredited body makes corresponding agreement with
the Accreditation Center and pays established fee.
3. The inspections bodies are required to create photo or video materials of the inspection object, as
well as keep the copies of documentation provided by the applicant about inspected units, engines and
details and submit them to the accreditation center if it’s required and during the monitoring.

GAC 1.9: 2012 – Rules and procedures of Accreditation Committee
Chapter I. General provisions
Article 1. Purpose This document establishes the structure, responsibilities and work organization of GAC accreditation Committee. Article 2. General Requirements The Committee is an advisory body, which reviews current and periodical issues of accreditation scope and makes appropriate decisions. The Committee's work is guided by the laws of Georgia, Statute of the Accreditation Center, accreditation system rules, international agreements and treaties. Article 3. Committee Composition and Structure
1. Permanent members of the Committee shall be established by order of the General Director of GAC.
2. Permanent members of the Committee have the right to vote, when it comes to voting. 3. If necessary, the Committee can invite experts and representatives of interested parties, without
right of voting, to give explanations about the issues under consideration and / or with the observer status. At that time, invited parties should abide by the principles of impartiality and confidentiality.
Chapter II. The Committee's functions and work procedures
Article 4. Functions of the Committee
1. Accreditation Committee has the following functions: a. Reviewing assessment results of applicants and getting recommendations about granting
accreditation or its refusal; b. Reviewing disputes (complaints, appeals) and making decisions in accordance with GAC
1.11:2012 - "Procedures for reviewing appeals and complains”; c. Reviewing surveillance and supervision issues and getting recommendations about granting,
renewing and confirming/extending/suspending/withdrawing/reducing of accreditation; d. Reviewing guidance documents, programs, legislative projects, regulatory acts and other
information related to GAC activities, including giving appropriate recommendations; e. Developing proposals to increase the efficiency of accredited bodies.
2. By carrying out its functions the Committee is responsible for: a. Completeness and accuracy of its rights and duties; b. The objectivity of the received recommendations and decisions; c. Confidentiality of information obtained as a result of Committee composition activities.
Article 5. The decision on granting accreditation
1. GAC’s General Director or Deputy General Director transmits assessment report, information about the implementation of corrective actions and other supplementary materials to one or more Accreditation Committee members who did not participate in the assessment for reviewing and developing recommendations for granting/refusal of accreditation during 7 business days and submitting their recommendations to the General Director in writing.

2. Recommendation documents shall be submitted to General Director of GAC, who will review them during 7 business days and in case of approval issue an order about granting accreditation.
3. If there are inaccuracies and / or nonconformities in work, or additional information is needed, the General Director or Deputy General Director is authorized to suspend final decision on accreditation and send the matter back to the Committee and / or forward the issue to technical Committee of GAC.
4. Accreditation certificate is issued based on General Director’s order. Article 6. Reviewing of surveillance and supervision results
1. GAC’s General Director or Deputy General Director transmits surveillance and supervision reports and supplementary materials to one or more Accreditation Committee members who did not participate in the assessment for reviewing and developing recommendations. Committee submits recommendations in writing to General Director or Deputy General Director during 7 business days. GAC’s General Director or Deputy General Director reviews accreditation committee recommendations during 7 business days, and issues corresponding order.
2. By reviewing surveillance and supervision issues, Committee can get recommendations about extending/suspending/withdrawing/reducing of accreditation.
3. Based on recommendations given by Committee, general director or deputy general director makes final decision about extending/suspending/withdrawing/reducing of accreditation. Article 7. Committee meeting
1.Committee meeting reviews: a. Accredited body supervision results; b. Complaints and appeals; c. guidance documents, programs, legislative projects, regulatory acts and other information
related to GAC activities and develops proposals; d. Activities to increase the efficiency of accredited bodies and develops recommendations; e. Issues regarding the registration of inspection bodies accredited in OECD and EU.
2. Committee reviews supervision results, as well as complaints and appeals, when more than half
of its permanent members are present. The voting right can only be used by a member, who was not involved in assessment / surveillance.
3. The meeting is headed by the General Director of GAC, and in case of his absence by his deputy.
4. The frequency of meetings depends on a number of incoming issues. The information and supplementary materials related to issues should be submitted to Committee members 3 days before the meeting.
5. The issues are mooted by the case manager or other person designated by the head of the Committee meeting. A person who mooted the issue is responsible for the proper presentation and authenticity of the materials.
6. In exceptional cases, if the issue does not necessarily require its review on meeting, decision on issue may be taken by the survey of the Committee members. The issue is sent to all permanent members of the Committee.
7. The Committee is authorized to invite experts and representatives of interested organizations and / or administrative bodies on meeting to discuss the issue; they should be notified about this 3 days before the meeting.
8. The Committee meeting results should be recorded in the form of a protocol during ten business days. The protocol consists of its serial number, the date of the meeting, contents of reviewed issue, and the names of the members present. The permanent members of the Committee and secretary should sign the protocol.

GAC 1.10:2012 – procedure for Registry of the Accredited Bodies Paragraph 1. Scope 1. This Registry procedure determines structure of the registry of the Accreditation System; its content and rule of use. 2. Administrative department of the Accreditation center is responsible for maintaining registry according to the given rule. Paragraph 2. Terms and definitions 1. Registry of Accreditation System – (hereinafter – registry) is a document for recording official/public information about the Accreditation bodies. 2. Registration-Keeping records of the accredited bodies in registry and giving registration numbers to the accredited bodies. (Registration number is the same as the number of the Accreditation Certificate) Paragraph 3. Keeping Registry and usage 1. Administrative department is responsible for registration, withdrawal, updating information, etc. about the accredited bodies. 2. Using the data from the registry accreditation center can provide the interested parties with public information about the accredited bodies. 3. GAC publishes information from the registry on the website of the Accreditation Center. 4. Accreditation Center uses Registry information for Accreditation and inspection control procedures. 5. Registry exists in electronic version ( Annex 1) 6. In the Notes, it is indicated additional information on Accredited bodies, for example: Partial or complete suspension of Accredited scope, Withdrawal, expansion (accreditation of additional scope), reducing, also expiration of accreditation date, replacing the number of the Accreditation Certificate. Paragraph 4. Accreditation Certificate Number and Structure Accreditation Certificate Number has next structure: GAC - XX - XXXX, where: a) GAC - the acronym of the Accreditation Center with Latin alphabet b) XX - type of the conformity assessment body b.a) testing laboratories - TL b.b) Calibration Laboratories - CL b.c) Medical laboratories - ML b.d) product certification bodies - PRC b.e) personnel certification bodies - PC b.f) management system certification bodies - MSC b.g) inspection bodies - IB c) XXXX - the body’s number in the register; Example: testing laboratory - GAC – TL – 0001.

2. If one legal entity has several working branches, Accreditation Certificate is issued, with indication of Central Office address, but in annex of certificate is indicated branch office address and scope.
Annex # 1 Accreditation Registry #
Organization Name, Address, Telephone number, Email, Name and Surname of Manager
Type of conformity assessment body Accreditation Scope
Accreditation Certificate data Note
Dat
e of
Acc
redi
tatio
n ce
rtifi
cate
Issu
ing
Dat
e of
A
ccre
dita
tion
Cert
ifica
te
wor
king
an
d en
ding
dat
es
Reg
istra
tion
Num
ber
(Acc
redi
tatio
n Ce
rtifi
cate
num
ber
1 2 3 4 5 6 7 8

List of changes
R
evis
ion
Actual Chapter Date Content
1 Annex 1 15.01.14 New column “Type of conformity assessment body” is added

GAC 1.11:2012 – Procedure for Appeals and Complaints
Terms and Definitions 1. Appeal – request by a CAB for reconsideration of any adverse decision made by the accreditation body related to its desired accreditation status.
Adverse decisions include: a) refusal to accept an application, b) refusal to proceed with an assessment, c) corrective action requests, d) changes in accreditation scope, e) decisions to deny, suspend or withdraw accreditation, and any other action that impedes the
attainment of accreditation . 2. Complaint – Expression of discontent by a person or organization on the activities of an accreditation body or an accredited CAB in expectation of a response. 3. Terms used in this document fully complies with standards of ISO/IEC 17000 series and guiding documents of conformity assessment for accreditation.
2. Appeals and Complaints 1. Appeals and/or complaints shall be registered at the administrative department of the Accreditation Center. 2. An appeal shall be registered at the Accreditation Center within one month from the date of the issue of the document being a subject to appeal to the appealing party. 3. A complaint shall be submitted to the Accreditation Center within one month from the date of identification of the cause for complaint. 4. The appeal procedures for initial assessment, surveillance and reassessment are identical.
3. Contents of Appeals and Complaints 1. Submitted appeal or complaint shall contain the following information:
a) Identification data of a body/person submitting an appeal or complaint (such as name and address), date, signature;
b) Subject of appeal or complaint; c) Reasons for appeal or complaint; d) Possible ways for solving the issue.
2. If there are object-lesson (proof evidences) available, they have to be submitted together with clime/application in order to review appeal or complaint. 3. If submitted appeal or complaint fail to comply with the requirements as described above, the Accreditation Center has the authority to ask the body/person for additional information and to suspend revision of appeal/complaint until receipt of additional information by GAC office.
4. Payment of Expenses 1. If the given evidences has proved true/vindicated, the expenses of an investigation/processing of appeal or complaint incurred by an appellant/complainant shall be covered by the party under complaint/appeal. 2. Expenses of appeals or complaints incurred by the activities of the Accreditation Center shall be covered according to the existing legislation of Georgia.
5. Reaction to Appeals 1. It is unacceptable that the requirements and criteria defined in the corresponding ISO/IEC standards or the guiding documents of regional organizations of accreditation, or the internationally recognized accreditation requirements be a subject to appeal or complaint. 2. It is unacceptable to submit an complaint (not an „appeal”) if based on arguments a person/body considers that the assessment of the assessment team or the activities of any of its members is incorrect, incompetent or discriminating. 3. The following issues related to accreditation can be appealed:
a) Denial of granting accreditation;
b) Suspension of accreditation; c) Withdrawal of the scope of accreditation or its part; d) the request for additional corrective actions, refusal of application, refusal to continue the
accreditation procedure 4. General Director of the Accreditation Center is responsible for making decision on appeals which is based on:
a) A proposal that includes reaction to an appeal based on submitted evidence and obtained information;
b) Proposals of the Accreditation Committee; c) Results of revision of appeal by the Technical Advisory Committee, if applicable.
5. To proceed an appeal the General Director appoints a person responsible for the appeal who investigates the issue and submits proposals to the Accreditation Committee for d i s c u s s i o n . The appointed person has to be independent from the responsibility concerning the activities under clime. 6. In case of necessity, with the purpose of gaining additional information the General Director may send the issue to an appropriate technical Committee of the Accreditation Center. 7. In case of necessity an authorized representative of the appellant party can be invited to attend the meeting of the Accreditation Committee when discussing the corresponding issue. 8. The Accreditation Committee shall make records when discussing an appeal. The records should include date, names of participants, signatures, brief description of the case and decisions (conclusions?) made by the Committee. 9. Final decision on appeal is made by the General Director of the Accreditation Center. 10. The Accreditation Center shall take decision on appeal in 25 working days from the date of entry. 11. The Accreditation Center shall inform the appellant in writing of the final decision within 5 days from making the decision. 12. If more than one month is required for investigation of essential circumstances in relation to the case with the purpose of revision of submitted appeal the Accreditation Center is authorized to make decision to extend the term of revision of appeal with one month. Decision shall be made in 7 days from entry the appeal, and shall be informed to the appellant body/person.
6. Appeals submitted on GAC Decision made on Appeal It is not admitted to submit a new appeal on the GAC decision made on appeal. If the appellant is not satisfied with the decision of GAC regarding the appeal, they can act according to the rules set in the legislation of Georgia. 7. Reaction to Complaints 1. Complaint which is not related to the activities of the Accreditation Center shall be returned to the complainant by the administrative department in 10 days with indication of reasons of return. Decisions on complaints that are related to the completion of the accreditation criteria by the accredited CAB’s are made in accordance with the rules and procedures of the Accreditation Center. 2. The Accreditation Center shall not admit that the complaint is discussed by the structural unit or the person on which the complaint is submitted. 3. When handling a complaint the General Director appoints a person responsible for the complaint who investigates the issue and submits proposals to the Accreditation Committee for discussion. 4. In case of necessity, with the purpose of gaining additional information the General Director may send the issue to the complaint and to the corresponding technical Committee of the Accreditation Center. 5. In case of necessity, an authorized representative of the complainant party can be invited to attend the meeting of the Accreditation Committee when discussing the corresponding issue.

6. In case of necessity, the Accreditation Committee is authorized to invite the parties interested in the case as observers. 7. When reacting to complaints they shall be studied taking into account their content but not what the complainant wishes or whom it refers to or by what reason it is submitted. Real circumstances shall be discussed fully and objectively on the basis of available information. 8. When discussing a complaint, records shall be made by the Committee that shall include date, names of participants, brief description of the case and decisions made. 9. Final decision on complaint is made by the General Director of the Accreditation Center. 10. The Accreditation Center shall take decision on complaint in 25 days from the date of its entry. 11. The Accreditation Center shall inform the complainant in writing of GAC final decision within 5 days after making decision on complaint. 12. If more than one month is required for investigation of essential circumstances in relation to the case with the purpose of revision of submitted complaint the Accreditation Center is authorized to make decision to extend the term of revision of complaint with one month. The decision shall be made within 7 days from entry the complaint and shall be informed to the complainant body/person.
8. Resubmission of Complaint The Accreditation Center admits revision of re-submitted complaint if new circumstances in relation with the case are identified.

GAC 1.12: 2012 – GAC’s Logo, Accreditation Symbol and Rules for their Use
1. Scope of application
1. The present rule determines the form and content of the logo of the Accreditation Center,
conditions for the use of text reference to accreditation status, and the use of accreditation symbol
by accredited testing/calibration and medical laboratories and certification and inspection bodies;
2. The present rule has been developed with anticipation of the requirements of SST ISO/IEC
17011:2010.
3. Accredited conformity assessment Bodies have to use the accreditation symbol to demonstrate
their accreditation status.
2. Terms and Definitions
1. Logo of the Georgian Accreditation Center – applied by the Georgian Accreditation Center only
for their identification.
2. Symbol of accreditation – issued by the Georgian Accreditation Center to accredited conformity
assessors to demonstrate their accreditation status.
3. Logo of the Georgian Accreditation Center and Accreditation Symbol
1. Logo of the Georgian Accreditation Center and symbol of accreditation is determined by the
Georgian Accreditation Center.
2. The Georgian Accreditation Center establishes the official symbol of accreditation in order that
conformity assessment bodies demonstrate their accreditation status.
4. Logo of the Georgian Accreditation Center
1. The Georgian Accreditation Center uses the logo of the Georgian Accreditation Center.
2. Personnel of the accreditation Center use the logo.
3. Accreditation certificates, applied official forms, letters and assessment reports are marked with
the logo.
4. Information on the form, color and parameters of the logo of the Georgian Accreditation Center
are published on the website of the Georgian Accreditation Center.
5. Symbol of Accreditation and Conditions for its Use
1. Accredited conformity assessment bodies shall apply the symbol of the Georgian Accreditation
Center. GAC publishes its accreditation symbols on its web-site.
2. Accredited CABs shall apply the accreditation symbol with the documents that are directly
related with their accredited activities; particularly the symbol shall be applied to testing
reports/calibration certificates, conformity certificates, inspection reports, etc.
3. The accreditation symbol is recommended to be placed in the upper right corner of a CAB
report or certificate.
4. The accreditation symbol shall not be applied in conditions that may mislead clients on the
status of accreditation and scope of accreditation.
5. Accredited bodies are responsible for proper use of the accreditation symbol.

6. Accredited body can place the accreditation symbol on an official letterheads or advertising
materials. 6. Description of the Symbol of the Accreditation
1. The Accreditation symbol is composed of the following components:
a) Logo of the Accreditation Center;
b) Title – “Georgian Accreditation Center”;
c) Reference to the standard in conformity with which the CAB is accredited;
d) Number of accreditation certificate.
7. Use of Accreditation Symbol by accredited CAB in Case of Granting Accreditation for Several
conformity assessment activities
Bodies accredited for several conformity assessment activities (e.g. testing and calibration; testing and
certification,) shall apply only one accreditation symbol for each activity. 8. Use of Text reference instead of Accreditation Symbol
1. Accredited conformity assessment bodies can apply text reference instead of accreditation
symbol in order to demonstrate their accreditation status. The text reference shall contain:
Name of the conformity assessment body
Name of the Georgian Accreditation Center;
Reference to the standard in conformity with which a person is accredited.
GAC recommends to use following wording e.g. “ (Name of the conformity assessment body” is
accredited by GAC against xxxx standard, with the accreditation certificate number GAC -xx-xxxx..
9. Rules for the Use of Accreditation Symbol and Text Reference to Accreditation Status by
Accredited Bodies
1. Only the conformity assessment bodies accredited by the Georgian Accreditation Center can
use the accreditation symbol.
2. Accredited conformity assessment bodies have the right to use the accreditation symbol with
the documents that are directly related with accredited services, particularly with calibration
certificates, test reports, conformity assessment certificates, inspection reports/certificates.
3. Accredited bodies are responsible to their clients for the proper use of accreditation symbol and
text reference.
4. If an accredited body carries out activates in several working locations/branches out of which at
least one is not accredited the accreditation symbol and text reference is used only for accredited
working location/branch.
5. If a body is accredited in one part of its activities only, the accreditation symbol and text reference
shall be applied only for these particular activities.
6. Certificates or reports or accompanying documents that contain the accreditation symbol but also
includes other non-accredited results, shall have the remark/note/* - “These results are not covered
by accreditation”.

10. Suspension, Withdrawal of the Validity of Accreditation Certificate
1. Accredited body whose accreditation was suspended shall terminate the use of accreditation
symbol and text reference.
2. After withdrawal of accreditation a conformity assessment body shall immediately terminate the
references that the CAB is accredited, also shall terminate the use of advertising materials that
contain the accreditation symbol and text reference to accreditation status.
11. Non-accredited activities
The term accreditation shall not be referred to, applied or meant for non-accredited activities.
12. Documents and Media
1. Text reference to accreditation shall be used by accredited bodies without any ambiguity.
2. The accreditation symbol and text reference can be used with advertising and public materials
if at least a part of the information is related with accreditation activities. The accredited activities
and scope of accreditation has to be clearly identified.
13. Document Containing Accreditation Results
1. Accredited body shall apply the accreditation symbol or text reference with the documents that
are directly related to accreditation services, particularly to calibration certificates, test reports,
conformity certificates, inspection reports/certificates.
2. Application of accreditation symbol or text reference does not mean that the Georgian
Accreditation Center is responsible for the accuracy of the results of certification, calibration,
inspection or tests.
3. Use of accreditation symbol or text reference does not mean that the decision on the product,
services, and management system or personnel competences was made by the Georgian
Accreditation Center.
4. Accreditation symbol or text reference to the status of accreditation shall not be applied to the
reports or certificates that do not contain accredited results.
14. Opinions and interpretations in relation with investigatory activities
If the laboratory test report contains the interpretations of the results, explanations that are
developed according to the requirements of investigatory activities where the laboratory
discussions exceed the limits of the scope of accreditation, there should be the reference “The
opinions and interpretations given in this report are beyond the accreditation limits (are not
covered by the scope of accreditation” placed beside the text of opinions or interpretations.
15. Users of Accredited Services
1. Organizations certified by the accredited management systems certification body can apply the
accreditation symbol or text reference to the accreditation status together with the certification
logo only, within the limits of the scope of accreditation of the certification body.
2. Clients of the accredited product certification body can place the accreditation symbol directly
on p r o d u c t s o r their packages together with the certification logo/mark. The c e r t i f i c a t i o n
logo/mark is mandatory in this case.

3. Clients of the accredited laboratories can refer to the accreditation status of laboratory only on
their advertising materials. In such a case, the accredited laboratories shall have internal policy and
procedures on applying their logo, accreditation symbol and text reference to accreditation by their
clients. Clients of accredited laboratories can apply the accreditation symbol or text reference to
accreditation only together with the laboratory’s logo.
4. Clients of the accredited personnel certification bodies have no right to apply the symbol of
the Georgian Accreditation Center though they can demonstrate their status by a certificate issued
by the accredited certification body.
16. Misuse
In case of unlawful use of the accreditation symbol or text reference to accreditation status, or the
accreditation logo the Georgian Accreditation Center can carry out corresponding measures against
the body violating the above descried rules, suspend or withdraw accreditation if necessary and/or
impose legal or other kinds of sanctions against the body.


















