
G8 b-thall Chromatogram Interpretation Guide1 b-thall Chromatogram... · 2 Transportstraat 4 EC REP...
58
1
-
Upload
truongphuc -
Category
Documents
-
view
222 -
download
0
Transcript of G8 b-thall Chromatogram Interpretation Guide1 b-thall Chromatogram... · 2 Transportstraat 4 EC REP...

1

2
EC REP
Introduction This “Chromatogram Interpretation Guide” is intended to give a brief overview of Haemoglobin and Haemoglobinopathies. This guide also provides you with a detailed explanation about Thalassaemia and the different types of Thalassaemia. The largest part of the guide is dedicated on the interpretation of chromatograms based on the original chromatogram or a piano chromatogram. If you require further assistance with the interpretation of unusual chromatograms, please contact your Tosoh Bioscience representative. TOSOH CORPORATION 3-8-2, Shiba, Minato-ku TOKYO 105-8623 (JAPAN) Tel.: +81-(0)3-5427 5181 Fax: +81-(0)3-5427 5220 TOSOH BIOSCIENCE N.V. Transportstraat 4 B-3980 TESSENDERLO (BELGIUM) Tel.: +32-(0)13-66 88 30 Fax: +32-(0)13-66 47 49
La Cite Internationale, 34, Quai Charles de Gaulle F-69006 Lyon (FRANCE) Tel.: +33-(0)437 48 87 50 Fax: +33-(0)437 48 87 58
Zettachring 6 D-70567 STUTTGART (DEUTSCHLAND) Tel.: +49-(0)711 13 25 760 Fax: +49-(0)711 13 25 762
TOSOH BIOSCIENCE SRL Corso Susa 299/A I-10098 RIVOLI-TORINO (ITALY) Tel.: +39-011-95 19 333 Fax: +39-011-95 19 329 TOSOH BIOSCIENCE AG Zentrum Fanghöfli 8 CH-6014 LITTAU-LUZERN (SWITZERLAND) Tel.: +41-(0)41-250 44 80 Fax: +41-(0)41-250 50 64 TOSOH BIOSCIENCE Ltd. The Business Centre, Edward Street, Redditch B97 6HA WORCESTERSHIRE (UNITED KINGDOM) Tel.: +44-(0)1527-59 29 01 Fax: +44-(0)1527-59 29 02

3
Table of Content 1. Haemoglobin ..................................................................................................... 2. Haemoglobinopaties ........................................................................................ 3. Common Haemoglobinopaties........................................................................ 4. Thalassaemias .................................................................................................. 5. G8 β-Thalassaemia principle ........................................................................... Chromatograms 1. Chromatogram Analyses ................................................................................. 2. Original Chromatogram ................................................................................... 3. Piano Chromatogram ....................................................................................... 4. Chromatogram Examples ................................................................................
Normal patient ............................................................................................... β-Thalassaemia patient ................................................................................. α+β-Thalassaemia patient ............................................................................. Hereditary Persistent Fœtal Hb patient ......................................................... Possible HbD patient ..................................................................................... Possible HbAS patient ................................................................................... Possible HbAC patient................................................................................... Possible HbAE patient ................................................................................... Possible HbAJ (Baltimore) patient................................................................. Possible HbAJ (Meerut) patient..................................................................... Possible HbSC patient................................................................................... Possible HbSS patient ................................................................................... Possible HbCC patient .................................................................................. Possible HbEE patient ................................................................................... Possible HbAS and α-Thalassaemia patient................................................. Possible neonatal patient .............................................................................. Possible neonatal HbAS patient ....................................................................
Basic Operations 1. Daily Care .......................................................................................................... 2. Calibration ......................................................................................................... 3. Filter Change ..................................................................................................... 4. Column Change ................................................................................................ 5. Buffer Change ................................................................................................... 6. Needle Change ..................................................................................................

4
7. Mode Change .................................................................................................... 8. Paper Change.................................................................................................... Additional Operations 1. Perform Drain Flush ......................................................................................... 2. Saving Results to Disk ..................................................................................... 3. Recalculation of Results .................................................................................. 4. Reprinting of Results ....................................................................................... 5. Transportation of the results to the host ....................................................... 6. Changing Parameters....................................................................................... 7. Adding Comments ............................................................................................ 8. Programming Flags .......................................................................................... 9. Programming the Timer ................................................................................... Instrument Care 1. Daily Care .......................................................................................................... 2. Half yearly Care................................................................................................. 3. Annual Maintenance......................................................................................... Specifications Performance 1. Linearity / Dilution ............................................................................................ 2. Correlation......................................................................................................... 3. Intra-Precision................................................................................................... 4. Inter-Precision................................................................................................... 5. Interferences ..................................................................................................... Reagent Information ................................................................................. References ...................................................................................................... Glossary ...........................................................................................................

5
1. Haemoglobin
Haemoglobin is the red, oxygen-carrying pigment in red blood cells. It is a globular molecule made up of 4 subunits. Each subunit contains a haem moiety conjugated to a polypeptide. Each haemoglobin molecule consists of two pairs of polypeptides. In normal human adult haemoglobin (Haemoglobin A = HbA), the two types of polypeptides are called the α (alpha) chains and the β (beta) chains. Thus HbA consists out of 2α chains and 2β chains.
(Source: Internet) Not all the haemoglobin in the blood of normal adults is HbA (α2β2). About 2.5% of the haemoglobin is HbA2, in which the β chains are replaced by δ (delta) chains (α2δ2). The blood of the human foetus normally contains foetal haemoglobin (HbF). Its structure is similar to that of HbA except that the β chains are replaced by γ (gamma) chains (α2γ2). HbF is normally replaced by adult haemoglobin soon after birth and will remain present at a concentration below 2%. However, in certain individuals it fails to disappear and persists, at a higher concentration than 2%, throughout life, this is termed Hereditary Persistence of Foetal Haemoglobin. Normal individuals have: Haemoglobin A: (α2β2): around 95% of the total Haemoglobin Haemoglobin A2: (α2δ2): between 2 and 3.5% of the total Haemoglobin Haemoglobin F: (α2γ2): less than 2% of the total Haemoglobin

6
2. Haemoglobinopathies The haemoglobinopathies are any of a group of diseases characterized by abnormalities, both quantitative and qualitative, in the synthesis of haemoglobin. Most of them are genetically inherited but occasionally they can be caused by a spontaneous mutation. They are the world's most common mono-genic, autosomal, and recessive disease in man.
Mono-genic, autosomal, recessive disease There are about 30,000 genes, which make our genetic blueprint, located on our 46 chromosomes. 44 chromosomes come in pairs (22 from the mother and 22 from the father) and are named autosomes. The two remaining chromosomes XX or XY (or sex chromosomes) are inherited as follows. Mothers who have two X-chromosomes can only give one of both. Fathers may give either the X-chromosome and then the child will be a daughter (with two X-chromosomes like the mother) or their Y chromosome and then the child will be a son (with an X and a Y chromosome like the father). Thus, a mono-genic, autosomal, recessive disease is a disease caused by a mutation on a single gene (mono-gene) which is located on one of the 44 autosomes and which does not manifest in the carrier (recessive). Why recessive? The presence of the equivalent gene, without the mutation on the other autosome, is sufficient to prevent the expression of the mutation (a disease in the case of haemoglobinopathies) in the carrier. In other words, carriers (heterozygotes) of mono-genic, autosomal, recessive diseases do not manifest in the disease.
For a haemoglobinopathy disease condition to exist, an abnormal haemoglobin or thalassaemia must be inherited from both parents resulting in a homozygous or double heterozygous condition. A trait condition (carrier state) exists when a person inherits one normal Hb gene and one abnormal Hb gene. This person is healthy under normal circumstances and often is not aware they are carrying an abnormal haemoglobin (there are some rare exceptions and extenuating circumstances where trait carriers can have symptoms). Like other recessive traits, haemoglobin traits may be passed along for many generations and not cause disease in the offspring until the time they are inherited from both parents.
Haemoglobinopathies worldwide Haemoglobinopathy carriers are protected in childhood from the fatal consequences of malaria tropica, and thus are selectively advantaged. This selection mechanism has increased the number of haemoglobinopathy carriers to, on average, 5% of the world population. However, healthy parents who are both carriers of a haemoglobinopathy may give their children both genes carrying the defect. These children are then homozygous or compound heterozygous for a haemoglobinopathy mutation. Without the compensation of a

7
normal gene to protect them, they will be affected by an incurable haemolytic anaemia. Worldwide, 300,000 severely affected children are born from healthy carrier parents each year. Frequently encountered homozygous or compound heterozygous forms of haemoglobinopathies are β-thalassaemia major and sickle cell disease (SCD). These diseases manifest soon after birth and can be extremely severe. Although a few cases may undergo a successful bone marrow transplant, these patients remain incurable and can only be intensively treated by lifelong supportive therapy.
Prevention of haemoglobinopathies Successful prevention strategies have been applied in several countries with a high frequency of haemoglobinopathy carriers. To date, the problem of prevention of haemoglobinopathies, has made an entrance in the immigration countries of Northern Europe where large sections of the population are at risk for severe haemoglobinopathies in their progeny because of their high carrier frequency, endogamy (interfamily marriages) and higher reproductive rates.
The haemoglobinopathies can be subdivided into: • Structural haemoglobin variants:
o Quantitative defects caused by a reduced/imbalanced synthesis of a normal globin chain are referred to as the “Thalassaemias”.
o Qualitative defects caused by the normal synthesis of an abnormal globin chain, often due to single amino acid substitutions in either the alpha or beta globin chains. A common example is the Glu to Val mutation at position six of the beta globin chain in sickle cell disease
• Hereditary persistence of foetal haemoglobin: o genetic defects in the switch from foetal to adult haemoglobin synthesis o foetal haemoglobin persists into adult life
3. Common Haemoglobinopathies
Sickle Cell Anaemia
The HbS gene is known to be widespread, reaching its highest incidence in equatorial Africa, but also occurring in parts of Sicily and Southern Italy, Northern Greece, Southern Turkey, the Middle East, Saudi Arabia, especially the Eastern province, and much of central India. The gene established itself in these populations presumably because its expression in a heterozygous state (sickle cell trait, less than 50% abnormal Hb) would give the patient some protection against the clinical consequences of plasmodium falciparum (or another type of plasmodium that causes malaria). The sickle cell trait has therefore reached high frequencies in malaria prone regions. Unfortunately, the homozygous state produces sickle cell disease (greater than 50% abnormal Hb), which is a chronic haemolytic anaemia and vaso-occlusive condition that usually takes the life of the individual affected. Sickle Cell Anaemia is the most common, symptomatic haemoglobinopathy worldwide. Sickle Hb (HbS) is a structural haemoglobin defect where a DNA substitution in the β-Hb chain (β6 A3 = β-chain is affected at the 6th amino acid in the A3 position of the helix) gives rise to alteration of the genetic code for haemoglobin. This substitution changes the electrical charge and behaviour of haemoglobin molecules,

8
affecting solubility, function and/or stability. Haemoglobin S has the peculiar characteristic of expressing its biochemical instability by aggregating up into long microtubular arrays called tactoids. The red blood cells containing HbS, stretch around the tactoids to form the characteristic long, pointed, slightly curved cells called “sickle cells”. Only the deoxygenated forms of HbS (deoxy-HbS; when oxygen has been given up) form these tactoids. The sickle shaped cells can then block capillaries and cause infarcts and a local inflammatory reaction and can also haemolyse resulting in chronic anaemia. The cells may return to their normal shape upon reoxygenation of the haemoglobin, however repeated sickling events cause irreversible membrane changes (making the RBCs leaky and rigid) until removal is carried out by phagocytosis in the spleen, liver and bone marrow. Clumps of cells in the spleen, fingers and heads of the femur can lead to infarcted tissue. More RBCs behind the clump release their oxygen causing the plug to increase in size.
Vaso-occlusive crises occur from blockage of micro-vasculature (may be due to infection, decreased pressure, dehydration or slow blood flow). This can be accompanied by fever (low grade), organ dysfunction and tissue necrosis. Increases in temperature, acidosis and dehydration encourage deoxygenation of Haemoglobin. The patient usually has quite a severe anaemia due to haemolysis of sickled RBC. Repeated crises in the spleen in early life causes splenic atrophy due to necrosis caused by the hypoxic, hypoglycaemic environment. Overwhelming bacterial infection can occur in the young. Gallstones are a feature of this disease and any chronic haemolytic anaemia. Cardiac hypertrophy occurs as a result of haemodynamic changes to compensate for the oxygen deficit.
Illustration of normal red blood cells (left) and sickle red blood cells (right).
(Source: Internet)
Haemoglobin C
Haemoglobin C (HbC) disease is also the result of a structural mutation of the β-Hb chain (β6 A3 = β-chain is affected at the 6th amino acid in the A3 position of the helix, but another mutation than with HbS) and causes crystal formation and aggregation of haemoglobin molecules within the red blood cells. Haemoglobin C disease (homozygous HbC) is characterized by compensated haemolysis with a normal haemoglobin level or a mild to moderate anaemia. There may be intermittent abdominal discomfort, splenomegaly, and slight jaundice.

9
Haemoglobin SC
Amongst people of West African ancestry, the next most frequent haemoglobinopathy to Sickle Cell Anaemia is Sickle Cell/haemoglobin C disease (HbSC) resulting from inheritance of one HbS gene and one HbC gene. In people that are compound heterozygous for HbS and HbC, both β-chains are abnormal, one codes for βs chains and the other for βc chains, thus HbA1 is absent. This disease is nearly as severe as homozygous HbS. Inside the RBCs the haemoglobin concentration is increased and HbC tends to aggregate and this potentiates the sickling of HbS. The clinical signs and symptoms are similar to mild Sickle Cell anaemia. So these patients can develop vaso-occlusive crises with complications, splenomegaly is prominent and they can develop a mild to moderate normocytic, normochromic anaemia.
Haemoglobin D
Several variants can be categorised under Haemoglobin D (HbD), including HbDPunjab, which is non-sickling and heterozygotes (HbAD) are asymptomatic. The most common mutation is HbD β121. Heterozygous and homozygous states are asymptomatic. Homozygotes may occasionally have an increase in target cells and osmotic fragility. When combined with the HbS gene however, mild sickling of erythrocytes can be observed.
Haemoglobin E
Haemoglobin E (HbE) is the third most prevalent haemoglobinopathy worldwide and is found mainly in South East Asia. This mutation (β26 = β-chain is affected at the 26th amino acid) results in slightly unstable HbE that causes red blood cells to reduce in size. Heterozygotes for HbE are asymptomatic whilst homozygotes (HbEE) characteristically suffer only mild hypochromic microcytic anaemia with reduced red blood cell life span. Combinations of Hb E with β-Thalassaemia genes however, can cause severe symptoms; HbE/β0-Thalassaemia causes poor development of abdomen and skeleton whilst HbE/β+ Thalassaemia symptoms are much milder.
Haemoglobin O-Arab
Haemoglobin OArab is another β-chain variant and is most commonly found in the Balkan Region and the Middle East. HbOArab, in the heterozygous form, has no clinical or haematological consequences and homozygous HbOArab is associated with a mild to moderate anaemia. When combined with the HbS gene however, HbOArab is associated with a sickling anaemia similar in severity to sickle cell disease and clinically patients resemble those with sickle cell anaemia. Double heterozygous HbO/β+-Thalassaemia is associated with a relatively severe microcytic anaemia.

10
4. Thalassaemias
The term thalassaemia is used to describe globin gene disorders that result from a diminished rate of synthesis of one or more globin chains and consequently a reduced rate of synthesis of the haemoglobin or haemoglobins of which that chain constitutes a part; α thalassaemia indicates a reduced rate of synthesis of the α globin chain; similarly, β, δ, δβ and εγδβ thalassaemias indicate a reduced rate of synthesis of the β, δ, δ+β and ε+γ+δ+β chains, respectively. Thalassaemia is the most common single gene disorder known.
A significantly reduced rate of synthesis of one type of globin chain leads to unbalanced chain synthesis, with excess of a normal globin chain contributing to the pathological effects, either causing damage to erythroid precursors and thus inducing ineffective erythropoiesis or causing injury to mature erythrocytes and thus inducing haemolytical anaemia. The genes controlling globin synthesis are on chromosome 11 (each chromosome carries 1 β-, 1 δ-, 1 ε- and 2 identical γ- genes) and on chromosome 16 (each chromosome carries 2 identical α- and 2 identical ζ- genes). Mutations and deletions of the α and β genes are of potential significance since there is a reduced rate of synthesis of haemoglobin A, the major haemoglobin present in adult life (90%). A serious clinical disorder is usually only observed when both the β genes or three or four of the α-genes are affected.
γ-Thalassaemia will only be of potential significance in intrauterine and early neonatal life when HbF is a major haemoglobin; however, since there are four γ genes, significant disease is unlikely. δ-Thalassaemia is of no clinical significance except that its presence may interfere with the diagnosis of coexisting β-thalassaemia. Thus, in the thalassaemia patient, a mutation or deletion of the genes that control globin production occurs. This will lead to a decreased production of the corresponding globin chains and an abnormal haemoglobin ratio. This abnormal ratio leads to a decreased synthesis of haemoglobin and the expression of thalassaemia. The globin that is produced in normal amounts winds up in excess and will form red cell aggregates or inclusions. These aggregates become oxidized and damage the cell membrane, leading either to haemolysis, ineffective erythropoiesis, or both. The quantity and properties of these aggregates determine the characteristics and severity of the thalassaemia.
Demographics Thalassaemia traits and diseases are found in all populations, but are seen most often in people of the following ancestry:
• Southeast Asian (Vietnamese, Laotian, Thai, Singaporean, Filipino, Cambodian, Malaysian, Burmese and Indonesian)
• Chinese • East Indian • African • Middle Eastern • Greek • Italian • Transcaucasian (Georgian, Armenian and Azerbaijani)

11
α-Thalassaemia The α-thalassaemias are caused by a decreased synthesis of α globin chains due to a deletion or mutation of one or more of the four α globin genes. As α-chain production is evenly divided amongst the four genes, the failing of one or more of these genes will results in an excess of beta globins, which leads to the formation of β globin tetramers (β4) called haemoglobin H (HbH). These haemoglobin tetramers are more stable and soluble than the ones formed in the case of β-thalassaemia (α4), but under special circumstances, they can lead to haemolysis, generally shortening the red blood cell life span. Conditions of oxidant stress cause HbH to precipitate, interfering with membrane function and leading to red cell breakage. The α-thalassaemias can be categorized as follows:
• α-Thalassaemia trait: This trait is characterised by two dysfunctional α-genes. The gene defect can
occur on the same chromosome (cis-type α-thalassaemia trait) or on each of the chromosome pair (trans-type α-thalassaemia trait). The cis-type is most common in people of Southeast Asian, Chinese or Mediterranean ancestry, while the trans-type is most common in people of African descent. The α-thalassaemia trait results in mild anaemia with microcytosis, erythrocytosis and hypochromia. Individuals with the α-thalassaemia trait will experience no significant health problems except a possible slight anaemia, which cannot be treated with iron.
• Haemoglobin H Disease: This disease is characterized by three dysfunctional α-genes. The severe
imbalance between the α chain synthesis and the β chain synthesis causes an accumulation of β chains inside the RBCs. Normal β chains only associate with α chains but in the case of HbH disease the β chains begin to associate in groups of four, producing the abnormal haemoglobin, called haemoglobin H (in the foetal life, the γ chains associate in groups of four to form an abnormal haemoglobin, called haemoglobin Bart’s). This haemoglobin variant, HbH, does not function as a normal haemoglobin and has a high oxygen affinity (it holds on to oxygen longer making it unavailable for use by the body). Patients with HbH disease have a persistent stable state of anaemia, which may be accentuated by increased haemolysis during viral infections and by exposure to oxidant medications, chemicals and foods. As the RBCs mature they loose their ability to withstand oxidant stress and HbH precipitates, which results in the damaging of the RBC membrane and eventually in haemolysis. The patients are characterised by a moderate anaemia, hypochromia, microcytosis and red cell fragmentation. Uncommon occurrences in a child with HbH can be severe anaemia, cholelithiasis, skin ulceration and splenomegaly requiring splenectomy. Unlike in β thalassaemic individuals, haemosiderosis is rare in HbH disease.
• Haemoglobin H –Constant Spring: This disease shows a more severe course than HbH disease.
These patients have a more severe anaemia with febrile illnesses and viral infections, often requiring transfusion, and have splenomegaly more frequently.
• α-Thalassaemia major (Foetal Hydrops Syndrome): In this case, all four α genes are dysfunctional.
The γ chains produced during foetal life associate in groups of four to form abnormal haemoglobin, called haemoglobin Bart’s. Since α globins are required for synthesis of foetal and adult haemoglobin, the foetus suffers from significant hypoxia and a very severe haemolytic anaemia. The anaemia is so severe that the disorder is lethal with foetal demise usually occurring in the third trimester. The mother frequently exhibits toxaemia and can develop postpartum haemorrhage. These patients will require life-long transfusions and other medical support.

12
β-Thalassaemia The β-thalassaemias are a group of conditions resulting from a reduced rate of synthesis of the β globin chain. More than 200 β gene mutations have been identified, occurring in a wide range of ethnic groups, and within each geographic population there are unique mutations. The β-thalassaemia syndromes are much more diverse than the α-thalassaemia syndromes due to the diversity of the mutations that can generate the defects in the β globin chain, with the severity of the defect being very variable. Unlike the deletions that constitute most of the α-thalassaemias, the vast majority of the β-thalassaemias are caused by mutations on chromosome 11 that affect all aspects of the β globin chain production (transcription, translation and the stability of the β globin product). Since there are a large number of β thalassaemia mutations, compound heterozygosity may also occur with patients having two mutant genes but no normal β gene. β thalassaemia mutations are divided into two broad categories, β0 (β-zero) thalassaemia and β+ (β-plus) thalassaemia. In β0 thalassaemia there is either an abnormal gene that is not expressed or, less often, gene deletion. In β+ thalassaemia there is reduced, but not absent, expression of the abnormal gene so that even in the homozygous state there is still some haemoglobin A production. Compound heterozygotes for β thalassaemia may have two different β0 thalassaemia genes, two different β+ thalassaemia genes or both a β0 and a β+ thalassaemia gene. β thalassaemia can be divided into three general categories: • β thalassaemia trait: This state is characterized by heterozygosity of one deleted or mutated gene and
one normal functioning gene, and may therefore also be referred to as β thalassaemia minor. Individuals with this trait are usually completely asymptomatic. In conditions of haemopoietic stress, for example during pregnancy or intercurrent infections, the patient may become anaemic and even require blood transfusion. Occasionally patients have splenomegaly.
• β thalassaemia intermedia: This state refers to a clinical phenotype with diverse genetic explanations.
These individuals will have a homozygous or heterozygous β globin mutation that causes a decrease in β chain production, but not to the degree that chronic transfusion therapy is necessary. In comparison with a typical patient with β thalassaemia trait, there are significant clinical problems such as anaemia, splenomegaly, leg ulcers and bony deformities. The condition differs from the β thalassaemia major in that the affected individual is not dependent on transfusions for survival, although transfusions may be needed occasionally or may become necessary later in life. The severity of β thalassaemia intermedia varies from a mild condition that resembles the β thalassaemia trait but with a greater degree of anaemia and splenomegaly, to a condition in which survival without transfusion is barely possible, accompanied by growth retardation and bony deformity. In some patients the explanation for a thalassaemia intermedia rather than a thalassaemia major or minor phenotype is not clear. Some genotypes are consistently associated with thalassaemia intermedia whereas there are others sometimes associated with thalassaemia major and sometimes with the intermedia.

13
• β thalassaemia major or Cooley’s anaemia: β thalassaemia major refers to patients with homozygosity or compound heterozygosity for β thalassaemia who are dependent on blood transfusions to maintain life beyond early childhood. They have both ineffective erythropoiesis and a shortened red cell life span leading to severe anaemia. This disease usually presents itself in the first year of life, from the age of 3 months onwards. The affected individuals show a markedly increased erythropoiesis, both in an expanded bone marrow compartment and at extramedullary sites. The expansion of haematopoietic bone marrow leads to bony deformities, particularly in the skull and facial bones. There is also bone pain and tenderness and an increased incidence of fractures consequent on thinning of the cortical bone. Erythropoiesis at extramedullary sites leads to gross hepatomegaly and splenomegaly. In turn, the splenomegaly may lead to hypersplenism. Ineffective haematopoiesis and shortened red cell life span lead to mild jaundice and an increased incidence of gallstones. There is wasting of the limbs and stunting of growth. Many of the adverse effects of β thalassaemia major can be largely avoided by blood transfusion. However, this leads to serious iron overload, which in turn can lead to cardiac and hepatic damage and delayed puberty. In the absence of treatment, children with homozygous β0 thalassaemia usually die at 3 to 4 years of age, whereas children with homozygous β+ may survive to late childhood.
δ Thalassaemia Since this type of genetic disruption only affects the synthesis of haemoglobin A2, δ thalassaemia is of no clinical significance. However, it is important in relation to the diagnosis of a β thalassaemia trait, since inheritance of δ thalassaemia, in cis or trans to β thalassaemia, means that haemoglobin A2 will not be elevated and the diagnosis of β thalassaemia heterozygosity may be missed. Both δ0 and δ+ mutations exist. Both the hetero- and homozygotes for δ+ thalassaemia have a reduced percentage of haemoglobin A2; in δ0 heterozygotes HbA2 is reduced, in δ0 homozygotes HbA2 is absent.
δβ Thalassaemia δβ0 thalassaemia results from deletion of both the δ and the β gene but with preservation of the γ genes. The heterozygotic phenotype resembles that of the β-thalassaemia trait but the haemoglobin A2 percentage tends to be reduced to about half of the normal levels (normal +/- 2.5%), whereas HbF is consistently elevated, varying from 5 to 20% (normal < 2%). Because of the increased synthesis of HbF, homozygotes and compound heterozygotes who also have a severe β+ or β0 mutation may have thalassaemia intermedia rather than thalassaemia major. Homozygotes for δβ have 100% HbF. There are at least eight known mutations giving rise to δβ thalassaemia. This type of thalassaemia is observed in many ethnic groups but particularly around the Mediterranean (Italy and Greece).
εγδβ Thalassaemia There are at least eight mutations that either deletes the entire β gene cluster or that inactivate all genes of the cluster. They are correctly referred to as εγδβ thalassaemias but are more commonly called γδβ thalassaemias. All are rare and recognized only in the heterozygous form as the homozygous state would be incompatible with life. The phenotype resembles that of the beta-thalassaemia trait but without any elevation of haemoglobin A2 or F.
γ Thalassaemia This type of thalassaemia refers to a reduced rate of γ chain synthesis and therefore of haemoglobin F. This condition manifest maximally during intrauterine life and, since there are four γ genes, clinical sequences are likely to be minor.

14
Diagnoses In all cases, laboratory diagnosis is essential to confirm the exact diagnosis and to allow genetic counselling for parents and affected individuals. The following tests are used to screen and diagnose thalassaemia disease and/or trait: • Complete Blood Count (CBC) • High Performance Liquid Chromatography (HPLC) for quantification of HbA2 and HbF • Free erythrocyte-protoporphyrin (or ferritin or other studies of serum iron levels)
15
Salt concentration
high
Sample Column Detector
low
1 2 3
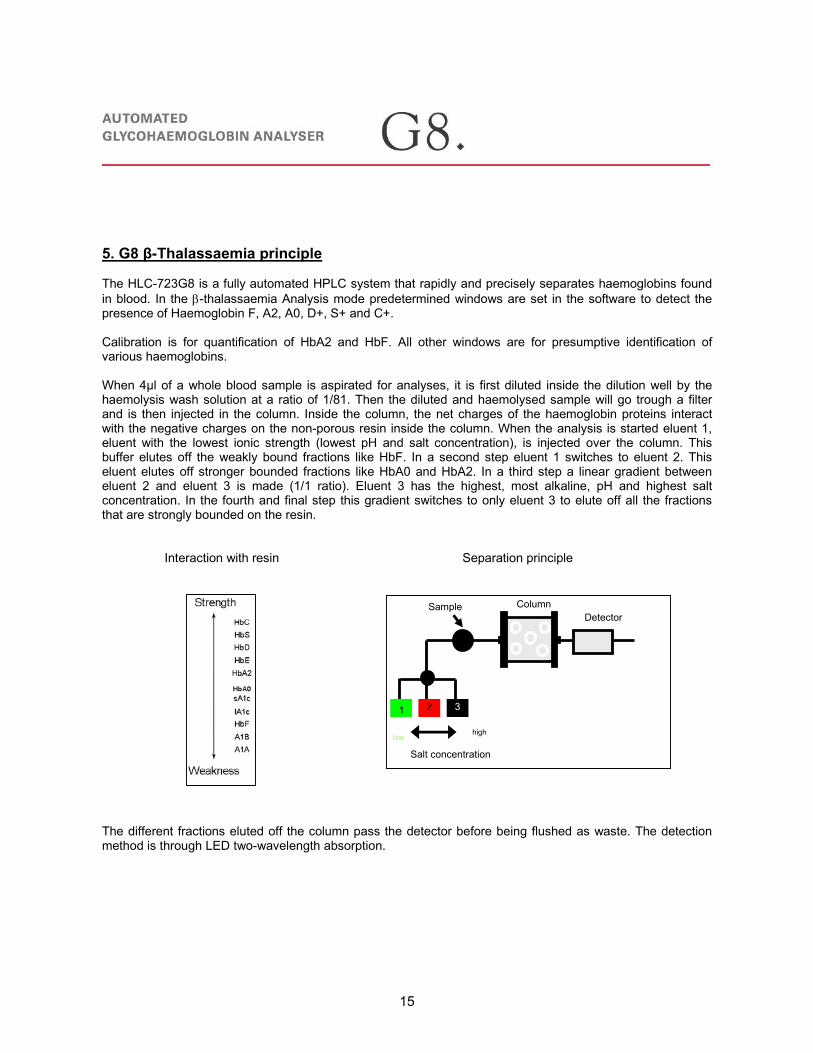
5. G8 β-Thalassaemia principle The HLC-723G8 is a fully automated HPLC system that rapidly and precisely separates haemoglobins found in blood. In the β-thalassaemia Analysis mode predetermined windows are set in the software to detect the presence of Haemoglobin F, A2, A0, D+, S+ and C+. Calibration is for quantification of HbA2 and HbF. All other windows are for presumptive identification of various haemoglobins. When 4µl of a whole blood sample is aspirated for analyses, it is first diluted inside the dilution well by the haemolysis wash solution at a ratio of 1/81. Then the diluted and haemolysed sample will go trough a filter and is then injected in the column. Inside the column, the net charges of the haemoglobin proteins interact with the negative charges on the non-porous resin inside the column. When the analysis is started eluent 1, eluent with the lowest ionic strength (lowest pH and salt concentration), is injected over the column. This buffer elutes off the weakly bound fractions like HbF. In a second step eluent 1 switches to eluent 2. This eluent elutes off stronger bounded fractions like HbA0 and HbA2. In a third step a linear gradient between eluent 2 and eluent 3 is made (1/1 ratio). Eluent 3 has the highest, most alkaline, pH and highest salt concentration. In the fourth and final step this gradient switches to only eluent 3 to elute off all the fractions that are strongly bounded on the resin.
Interaction with resin Separation principle
The different fractions eluted off the column pass the detector before being flushed as waste. The detection method is through LED two-wavelength absorption.

16
Chromatograms
The following pages contain examples of haemoglobin variants determined on the Tosoh G8 in ß-Thalassaemia Analysis Mode. For the different types of haemoglobin variants, we included the original chromatograms as well as the chromatogram in piano. For all the types we also have templates available to build up the piano library. Please note that the print outs from piano chromatograms can look a little bit different than described in the guide. This depends on the piano software. On each chromatogram there is a clarification of the peaks and a presumptive analysis. We want to point out that analysis of the result is based on the G8 β-Thalassemia chromatogram and a secondary method but that all types of variants are only presumptive.
In order to fully analyse the results, chromatograms are required together with the patient’s complete blood count. Note that ß-Thalassaemia mode is a screening technique and positive variant identification can only be done by DNA-analysis. 1. Chromatogram Analyses • Be sure that the problem is patient related (only a single problem chromatogram in a run) • Check that total area is within the recommended area • Check the retention times for each of the fractions • Check the TP value • Check that all peaks are present and that the peak is properly integrated. • Check that possible flag errors are present • Check whether F and A2 are in the normal range • Check possible significant other factions

17
2. Original Chromatogram
Sample number of the day: starts with one and will be reset as power is switched off. Barcode or rack, position number: when barcode is used, barcode will appear here. In case of no barcode or unreadable barcode, identification is given for the rack number and the position in the rack. Percentage for F and A2: normal range for F is less than 2% and for A2 between 2-3.5%. Calibration equation for F and A2: calibration equation for A2 must be less than 2. Theoretical plate: number for the quality of the separation, calculated on the A2 peak: must be over 700. Retention time for each fraction: F: 0.50-0.90; A0: 2.05-2.65; A2: 2.60-3.40. Total area: sum of all peak areas: acceptable: 2000-7000; recommended: 2200-6000. Flag field: field where error will occur if present. See p 47. HbA1c fraction: is eluting around 1.80 minutes but value is not calibrated.
Date and time of analyses
Software version
Sample number of the day
Barcode or rack, position number Calibration equation F
and A2
Theoretical plate Different Hb fractions
Percentage for each fraction
Retention time for each fraction
Area for each fraction
Total area
Percentage for F and A2
F fraction
A0 fraction
A2 fraction
Remaining fractions
Flag field
Fraction around 1.80 min is HbA1c

18
3. Piano Chromatogram
Date of printout
Patient information
Barcode or rack, position number
Sample number of the day
Date of analyses
Theoretical plate
Different Hb fractions
Percentage for each fraction
Calibration equation F and A2
Retention time for each fraction
Area for each fraction
Total area
A0 fraction F fraction A2 fraction
HbA1c fraction: 1.83 min

19
4. Chromatogram Examples
A0 around 80%
F and A2 in normal range
No other significant peaks
Result can be reported
Normal patient

20
β-Thalassemia patient
F in normal range
A2 too high
No other significant peaks
Result can be reported Remark: A2 too high

21
α+β-Thalassemia patient
F in normal range
A2 too high
No other significant peaks
Result can be reported Remark: A2 too high
α-Thalasseamia is determined by DNA analyses. No signs in HPLC
chromatogram

22
Hereditary Persistent Foetal Hb patient
F too high
A2 in normal range
No other significant peaks
Result can be reported Remark: F too high

23
Possible HbAD patient
F in normal range
A2 too high
Significant peak in D+ window
Result can not be reported
for A2 interference Remark: Possible HbAD

24
Possible HbAS patient
F in normal range
A2 in normal range
Significant peak in S+ window
Result can be reported
Remark: Possible HbAS

25
Possible HbAC patient
F in normal range
A2 in normal range
Significant peak in C+ window
Result can be reported
Remark: Possible HbAC

26
Possible HbAE patient
F in normal range
A2 > 10% Co-elution of variant
A2 can not be determined
Result can not be reported
for A2 Remark: Possible HbAE

27
Possible HbAJ (Baltimore) patient
F in normal range
A2 in normal range
Significant P04 peak
Result can be reported Remark: Possible HbAJ
Baltimore

28
Possible HbAJ (Meerut) patient
F in normal range
A2 in normal range
Significant P05 peak P04 can be glycated
fraction
Result can be reported Remark: Possible HbAJ
Meerut

29
Possible HbSC patient
F in normal range
A2 raised but less important due to SC
Result can not be reported Remark: Possible HbSC
Significant peak in S+ and C+ window
No A0 present

30
Possible HbSS patient
F is too high
A2 in normal range
Significant peak in S+ window
Result can be reported
Remark: Possible HbSS
No A0 present

31
Possible HbCC patient
F in normal range
A2 in normal range
Significant peak in C+ window
No A0 present
Result can be reported
Remark: Possible HbCC

32
Possible HbEE patient
F in normal range
A2 > 10% Co-elution of variant
No A0 present
Result can not be reported Remark: Possible HbCC

33
Possible HbAS and α-thall patient
F is too high
A2 in normal range
Significant S+ peak but lower than normal
HbAS patient
A0 lower than normal
Result can be reported
Remark: Possible HbAS α-Thall patient

34
Possible neonatal patient
F is 0.0% wrong integration
A2 in normal range
Actual F peak is in P03 peak and is too
high
Result can not be reported Remark: Possible neonatal
patient

35
Possible neonatal HbAS patient
F is 0.0% wrong integration
Actual F peak is in P02 peak and is too
high
A2 is too low
Result can not be reported Remark: Possible neonatal
HbAS patient
Small peak in S+ window: formation of
HbS

36
Basic Operations 1. Daily Care
Start-up Instrument
• Switch the main power on if necessary and press the “ ” button to start up the instrument. • During the initialisation the instrument performs a pump clean and buffer prime during 9 minutes. • After the initialisation the analyser goes automatically into stand-by mode (1). • Check buffers and Haemolysis Wash solution and replace if necessary. Replacing the buffers, see p 10. • Check and discard the waste. • Check whether the correct mode on top of the main screen (2) is displayed. For changing mode see p13. • Check paper. See p13 for replacement. • Check injections on filter. For replacement see p 10.
Figure 1: Main screen
Analysing Controls
Reconstitution of Controls
• Reconstitute the controls with 200µl of de-ionised water and let them stand at room temperature. The
reconstituted controls are stable for 5 days when stored at 2-8°C. • Make a dilution of 1/41 in a sample cup for both controls (10µl control and 400µl deionised water) and
put the cups in a sample rack. • The minimum required volume for a control is 150µl. • Place the rack on the instrument. • Press the START button. • The instrument will analyse the controls as patient samples.
1
2

37
Analysing Patient Samples • Place the whole blood samples in a sample rack with the barcode label to the front of the rack, so the
barcode reader can easily read the label. The minimum volume for a whole blood sample is 1000µl. • When the whole blood sample volume is insufficient a manual dilution of 1/81 can be made using G8 β-
Thalassemia Diluting solution (e.g. 10µl whole blood and 800µl Diluting solution) in a sample cup. • The cups are placed in a rack. • Place the rack with the samples on the instrument. • Press the START button.
Note: Calibrators and controls are analysed in sample cups. The instrument will not dilute them because they are recognised as manually pre-diluted samples. Patient samples analysed in primary tubes will be diluted by the instrument itself at a ratio of 1/81.
Ending Assay • Assay results will be printed and the instrument will automatically end assaying when empty rack is
detected. • Thereafter the washing procedure will be executed and the analyser will enter the STAND-BY modus. • When you press the “STOP” button during analyses, the last result is given before the analyser switches
to its wash cycle. • When pressing the “STOP” button twice the analyser will go into its wash cycle without finishing the
analyses it was performing.
Note: Make sure that the analyser completes its wash procedure when the assay is finished, otherwise sample will remain in the column and the column life span will be reduced.
• When the wash cycle is completed and the analyser has switched to the STAND-BY modus, press the
“ ” button to switch the analyser off. Main power may stay on at all times.

38
2. Calibration Each Laboratory must monitor QC results according to good laboratory practices to determine when to recalibrate. Calibration frequency should be based upon QC results and chromatogram quality. The analyser is calibrated with one calibrator with different assigned values for HbF and HbA2. Use the "G8 Hemoglobin F&A2 Calibrator" for calibration (P/N: 021932). Be sure to calibrate in the following situations: • After column replacement
Never fail to execute calibration after a new column has been installed. • When control values assayed are out of range
Calibrate when the control assay value falls outside the standard range. Measure the control sample again to confirm that it falls within the standard range before assaying a real sample.
• After analyser maintenance Be sure to calibrate after analyser maintenance or repair. • After changing analysis mode
Make sure to calibrate the instrument every time it is switched from β-Thalassaemia mode to HbA1c mode and visa versa.
• At least 1 time per month Use the “G8 Hemoglobin F&A2 Control Set” (P/N: 021933) together with the calibrator for the control of daily test results.
Reconstitution of calibrators • Reconstitute the calibrator by adding 200µl of deionised water and let it stand at room temperature. The
reconstituted calibrator is stable for 5 days when stored at 2-8°C. • After reconstitution the calibrator must be diluted 1/41 eg. 10µl calibrator on 400µl deionised water. • The minimum required volume for the calibrator is 400µl in a sample cup. • The cup with calibrator is placed in a sample rack where controls and patient samples can also be
placed. Place the rack on the instrument and place after the racks with samples an empty rack to indicate the end of the run.
Perform Calibration
• Press the CALIB button in the main screen. • Verify the calibrator assigned values which are printed on the calibrator bottles. • Select CALIB_1 (F) by touching the field. Put in the correct HbF value for the calibrator. • Select CALIB_1 (A2) and put in the correct HbA2 value for the calibrator. • Close the window by pressing the X in the right corner. • Press start key to perform calibration.

39
Figure 2: Calibration Set Screen • The instrument presumes that this is the calibrator and will analyse it 3 times. • The obtained HbF and HbA2 values for the 3 chromatograms will be compared and when the difference
is less than 0.3%, calibration is accepted. • The instrument calculates the new calibration factor for HbF and HbA2 and automatically updates the
calibration factors in the main screen. • Also the date of calibration will appear on the main screen. • If there are controls and patient samples placed behind the calibrator in the rack, the instrument will
analyse the rest of the samples.
3. Filter Change
Note: Filter needs to be changed after 200 injections
• Make sure that the analyser is in the STAND-BY mode. • Open the door and remove the filter top outlet tubing (4). • Loosen top of the filter holder assembly by turning counter clockwise and remove the filter holder by
pulling straight out (5). • Press the top of the filter holder to take out of the old filter (6). • Place the new filter with the grey side inside (up) the element. • Firmly tighten the top of the filter holder assembly by hand (7). • Connect the outlet side tubing (9). • Go to MAINTE, REAGENT CHANGE, press FILTER RESET, press ok.
Figure 3: Filter replacement
Gray surface is outlet (up)
4)
5)
9)
7)
6)

40
4. Column Change • Make sure that the analyser is in the STAND-BY mode. • Open the door and the column oven. Remove the old column. • Remove the protecting plugs of the new column and connect the new column. • Make sure that the direction of the arrow on the column and the arrow on the column oven are identical. • Go to MAINTE, REAGENT CHANGE, press COLUMN RESET and press ok. 5. Buffer Change • Make sure that the analyser is in the STAND-BY mode. • Replace buffers or Haemolysis Wash solution by new ones. • Squeeze all the air out of the aluminium packages • (not necessary for HW). • Fasten the bottle cap on the package. • Go to MAINTE and press REAGENT CHANGE.
Figure 4: Reagent Change Screen
• Highlight the corresponding key to replace reagent. Highlight #1 if you want to change buffer 1 (H/W is for the Haemolysis/Wash solution).
• Then press CHANGE and confirm by clicking on OK. • New reagent automatically replaces the reagent in the flow path and the buffer volume will be reset to
100% on the visual reagent level chart.

41
6. Needle Change
• Press the key and turn main power switch off to stop analyser operations during replacement. • Use a screw driver to remove the sampling cover screws shown in figure 7.
Figure 5: G8 Front View
• Open the unscrewed door by pulling the cover straight forward.
• The sampling needle unit is situated in the middle. Grasp the upper part of the sampling needle unit by hand and slowly pull the unit forward as much as possible.
• By hand, loosen and remove the joint connected to the 3-way block.
• Remove the screws on the upper section of the sampling needle. Be careful not to drop the screws or the holding plate inside the machine.
• Remove the tube from the black clip.
Figure 6: Sampling Needle Replacement
Screws
Holding plate
Screws 2
Pull
Screw (1 location)

42
• Slowly lift up the sampling needle to remove. • Insert the new sampling needle and secure the upper plate with the screws. • Fix the flow line by the black clip so that it doesn’t twist, and then securely connect the joint to the 3-way
block. • Move the sampling needle unit back and forth and confirm that the flow line does not catch on anything. • Push the sampling needle unit back, close the sampling unit cover by following the procedure in reverse,
and secure the screws. • Turn on the main power and switch analyser back on. • Assay a dummy sample or control to confirm that the sample aspiration is processed correctly (check
that the total area in the result is about the same as before the sampling needle replacement).
7. Mode Change (β-Thalassaemia Mode- Variant Mode ) • First change the buffers and column, see p9. • Go to menu, utility, mode change and select the other mode. • Press ok to confirm and analyser will switch off. • Automatically analyser will switch back on in the correct mode. • Initialisation must be performed completely in the new mode. • When analyser is in STAND-BY samples can be placed on the instrument. 8. Paper Change • Lift the printer cover (upper lid) open.
Figure 7: Changing Paper Figure 8: Changing Paper • Switch the blue paper holder level to the front to remove old paper. • Take new paper and place the mandrel inside the paper. • Place paper in position and switch blue paper holder backwards.
Printer cover
Paper feed
Lift Mandrel
Paper holder

43
Additional Operations 1. Perform Drain Flush
Drain flush needs to be performed when air is inside the instrument. The chromatogram is not correct and a zigzag pattern is visible. Air inside the instrument can be caused by buffer which was running low or was completely empty during analysis or warming up.
• Go to MAINTE, REAGENT CHANGE and press drain flush. • The instrument asks to open the drain valve. • The drain valve is situated behind the left cover door of the instrument. Drain Valve
• Open the drain valve not more than 90° and press ok. • After the full removal of the air, the instrument asks to close the drain valve. • Tightly close the drain valve when drain flush is finished.
• Switch instrument off and back on by pressing .
Open
Close
Door

44
2. Saving Results to Disk • Press the key on the main screen to display the RECALC screen. • The assayed results, which are stored in the analyser’s memory (RESULT) or on a Smart Media Card,
can be printed, retransmitted to a host, and recalculated with different calibration factors.
Note: Results can only be transported, recalculated or reprinted when data of analyses is known.
Display Content:
• Assay date of sample (same as the folder name) • First number (No on the chromatogram print out) of the results • Last number (No on the chromatogram print out) of the results • FACTOR_A1C A (can be changed when results must be recalculated using alternative calibration
factors). • FACTOR_A1C B (can be changed when results must be recalculated using alternative calibration
factors).
3. Recalculation of Results
• Give in the date (year/month/date) when samples were analysed. • Give in from which till which sample recalculation must be performed. • Give in proper factor for A and B if required and press “LOCK”. • Select from where samples must be calculated. • Press RSLT/CARD to select either the internal memory (RSLT) or the Smart Media Card (CARD). • When this key is not selected they come from the internal memory. • Press EXECUTE to perform recalculation. • Automatically recalculated results are printed out.
1
2
3
4
5

45
4. Reprinting of Results • Same actions are performed as for the recalculation of the results but factor A or B are not adjusted or
locked.
5. Transportation of the results to the host
• Same actions are performed as for the recalculation of the results (excluding the change of A and B). • Press the TRANS key and press EXECUTE. 6. Changing Parameters
Explanation of different parameters
• Go to MENU and press f or changing various parameter settings
• On Page 1 the calibrator values are displayed. • On Page 2 factors for A for HbF and HbA2 after calibration are displayed. • FORMAT: Printout format (0 or 9).
Note: It is advisable to use format 9 to print out the chromatograms
Format 0 Detailed peak information on the chromatogram (no TP value) Format 9 The most detailed information on the chromatogram

46
Page 3:
• RAW AUTO SAVE: Automatically saves the assay results to the Smart Media Card (0: no save, 1: save)
• LST AUTO SAVE: Automatically saves the list data to the Smart Media Card (0: no save, 1: save)
Note: list data is only the percentage of HbF, HbA1c and total A1. • LIST AUTO CLEAR: Clears results each time START is pressed
(0: do not clear, 1: clear) • OFF TIMER: Time from STAND-BY mode entry until power shut-off. The unit is hour. (0 ~ 3: 0 indicates
no automatic power shut-off) • COPY: Number of printout copies (0 ~ 3) Page 4: • LOADER SMP MODE: Designates the sample container type:
Container Primary tube Sample vial
0 Whole blood Diluted sample 1 Whole blood Whole blood 2 Diluted sample Diluted sample 3 Specified by host
• WASH MODE: WASH mode settings must always be on 0 • FLOW FACTOR: Pump flow factor. This factor can be adjusted when retention times are not falling in the
suggested range.
Note: Never adapt the flow factor more than 10% of the initial flow factor which is indicated on the door to the column oven.
• #100mm TUBE: Setting for the primary tube length
If you are using a combination of 75 mm and 100 mm tubes, set to 100 mm (0: 75 mm, 1: 100 mm)
47
• Select the proper line by clicking on it and automatically the PARAMETER input screen opens. • Press the CLR key to clear existing values and use the numerical keys to input value. • Confirm that the correct value is displayed in the input field and
press the key and close the input screen.
All settings and analyser parameter changes should be executed in the same way, as indicated above.
7. Adding Comments It is possible to put a comment on top of each chromatogram. • Go to MENU, UTILIY and press COMMENT. • Type in the name of the lab or hospital. • The comment will appear on the top of each chromatogram.
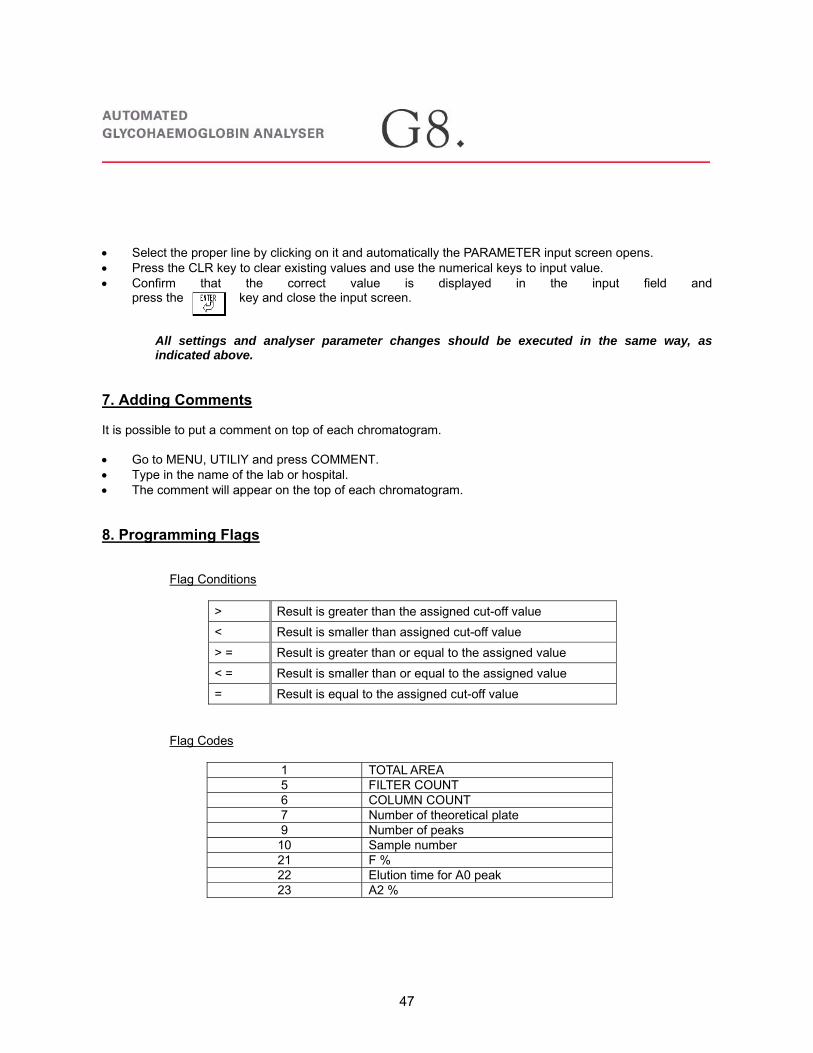
8. Programming Flags
Flag Conditions
> Result is greater than the assigned cut-off value < Result is smaller than assigned cut-off value > = Result is greater than or equal to the assigned value < = Result is smaller than or equal to the assigned value = Result is equal to the assigned cut-off value
Flag Codes
1 TOTAL AREA 5 FILTER COUNT 6 COLUMN COUNT 7 Number of theoretical plate 9 Number of peaks 10 Sample number 21 F % 22 Elution time for A0 peak 23 A2 %

48
• Go to MENU • UTILIY • FLAG • Select an empty field • Type in the code and level eg: 01<500 1 • Press ENTER • Press on MSG EDIT • Give in the appropriate message eg. Area too low • Press ENTER • The flag is programmed and will be printed off on the chromatogram when a sample is analysed which
meets the flag. Flag Levels • Level 0: The assay values are displayed/printed or transmitted when flag criteria is met. • Level 1: “---” is displayed or printed in the space of the assay result when flag criteria are met. A blank or
“0” is transmitted to the host computer when flag criteria are met.
01 < 700 0 AREA LOW 01 > 3000 0 AREA HIGH 01 < 500 1 AREA TOO LOW 01 > 4000 1 AREA TOO HIGH
10. Programming the Timer
• Go to MENU, and press key. • When the timer is selected and programmed, the analyser does the initialisation completely automatic
and goes in the STAND-BY mode afterwards. • Give in the correct year, date, time and start up time. • Select the dates of the week where analyser must be switched on automatically.
Figure 9: Weekly Timer
1234

49
Instrument Care
1. Daily Care
• Check buffer one, two and three and replace if necessary. • Check HW and replace if necessary. • Check column counter and replace when necessary. • Check filter counter and replace when counter hits 200 injections. • Discard waste if necessary. • Check printer paper and replace when necessary. 2. Half yearly Care
• Replace suction filters in buffers. • Check sampling needle and replace when bent or broken. • Replace sample loop and rotor seal.
3. Annual Maintenance
• Annual maintenance is always done by Tosoh service personnel.

50
Specifications • Normal values: HbF (<2%) HbA2 (2.0-3.5%) • Pressure: 10-12MPa • Total area: 2000-7000 acceptable with 2200-6000 recommended • TP>250 • Filter injections: change at 200 • Column injections: 750
Retention times F: 0.50-0.90 A0: 2.05-2.65 A2: 2.60-3.40 D+: 3.80-4.20 S+: 4.20-4.80 C+: 4.70-5.30

51
Performance 1. Linearity / Dilution
Two specimens, which have different concentration for F and A2, are mixed.
2. Correlation
The correlation between the HbF and HbA2 values for the G8 and HLC-723G7 analysers are shown in the graph below.
HbF G7 in function of HbF G8 HbA2 G7 in function of HbA2 G8
3. Intra- Precision Patient samples (n=20) HbF HbA2
Sample 1 Sample 2 Sample 1 Sample 2 Mean 0.52 1.93 3.69 3.35 SD 0.04 0.04 0.07 0.05
CV % 7.1 2.3 1.8 1.5
y = 1.0831x - 0.483r=0.99n=32
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
0.0 1.0 2.0 3.0 4.0 5.0 6.0 7.0 8.0G7
G8

52
4. Inter- Precision Patient samples (n=20) HbF HbA2
Mean 0.52 3.65 SD 0.04 0.07
CV % 7.9 1.9
5. Interferences
Glucose • Differences are less than 0.3Hb% • Less than 1000 mg/dL of Glucose may not interfere with the assay Sodium cyanate • Sodium cyanate decreases A2 (%) • Be careful to interpret results of nephritis
Glucose
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
0 200 400 600 800 1000 1200
Concetration(mg / dL)
Hb(
%)
HbF
A2%
Sodium Cyanate
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
0 5 10 15 20 25 30
Concetration(mg / dL)
Hb(
%)
HbF
A2%

53
0.00
0.40
0.80
1.20
1.60
2.00
0 5 10 15 20 25 30
Time (HR)
HbF
(%)
EDTA
Heparin
Citrate
0.00
0.40
0.80
1.20
1.60
2.00
0 2 4 6 8 10 12
Days
HbF
(%)
EDTA
Heparin
Citrate
Acetaldehyde • Acetaldehyde decreases A2 (%) and increases F (%) • Be careful to interpret results of Alcoholics
Stability of samples The primary blood samples with anticoagulants are stable at 25°C for 24 hours. HbF HbA2
The primary blood samples with anticoagulants are stable at 4°C for 10 days. HbF HbA2
Acet aldehyde
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
0 5 10 15 20 25 30
Concetration(mg / dL)
Hb(
%)
HbF
A2%
2.00
2.40
2.80
3.20
3.60
4.00
0 5 10 15 20 25 30
Time (HR)
HbA
2(%
)
EDTA
Heparin
Citrate
2.00
2.40
2.80
3.20
3.60
4.00
0 2 4 6 8 10 12
Days
HbF
(%)
EDTA
Heparin
Citrate

54
Reagent Information Reagent Stability when closed Stability after opening Storage temperature Buffer Till expiration date 3 months 4-25°C Column No expiration date - 4-15°C Calibrator Till expiration date 5 days 2-8°C Control Till expiration date 5 days 2-8°C Haemolysis Wash Solution
Till expiration date 3 months 4-25°C
G8 β-Thal Diluting Solution
Till expiration date 3 months 4-25°C
Venous whole blood or capillary blood samples are required for the assay. Venous blood collected aseptically into primary tubes, which contain EDTA, Heparin and Citric acid may be stored at 25 °C for 24 hours prior to analysis, or at 4 °C for 10 days. No special preparation is necessary. Capillary blood (5�l) may be immediately diluted into the G8 β-Thalassemia Diluting Solution and analysed directly on the G8.
The following components are available for the G8 β-Thalassemia mode Catalogue number
Description Packaging
021560 G8 Automated HPLC analyser 1 021561 90 Sample Loader 1 021562 290 Sample loader 1 021932 G8 Hemoglobin F&A2 Calibrator 4x0.2ml 021933 G8 Hemoglobin F&A2 Control Set 2x2x0.2ml 021929 TSKgel G8 β-Thal. 1 021930 G8 β-Thalassemia Elution Buffer Kit 11x 800ml 18431L Haemolysis and Wash Solution (L) 5 x 2000ml 021600 Filter element 5/bag 018581L Sample cups Hitachi 1000/bag 019563 Thermal printer paper 10 rolls/box 018723 Suction Line filters for Buffer lines 1 019791 Side hole needle 1 020101 Sample cup adapter for Tosoh sample racks 10/box 021931 G8 β-Thalassemia Diluting Dilution (S) 1x 800ml

55
References • Adrain Stephens; Haemoglobinopathies; The Biomedical Scientist; 2004, July, 1-4 • Anita J. Catlin; Thalassemia: The facts and the controversies; Pediatric Nursing, November-December
2003, 29 (6), 447-451 • Barbara J. Bain; Haemoglobinopathy Diagnosis; 2001 Blackwell Science Ltd. • Nancy F. Olivieri; The β-thalassemias; The New England Journal of Medicine, 1999, July 8, 341 (2), 99-
109 • P.C.Giordano, M.Herruer, W.Huisman, J.G.J.Pouwels, J.Smit, N.Verhoef, P.Wijermans; Rapport van de
werkgroep hemoglobinopathieën van de vereniging hematologische laboratoriumonderzoek. Enquêteresultaten en aanbevelingen t.b.v. dragerschapdiagnostiek en preventie van de hemobglobinopathieën. Uitgegeven door de leden van het landelijk werkgroep hemoglobinopathieën van de vereniging van hematologische laboratoria.
• The laboratory diagnosis of haemoglobinopathies; British Journal of Haematology, 1998, 101, 783-792 A lot of information was obtained from the following Internet websites: • www.hbpinfo.com/en/ • www.thalassemia.org/ • www.thalassaemia.org.cy/ • www.thalassemia.com/ • www.ukts.org/ • www.urmc.rochester.edu/genetics/hemobroc.htm • www.uq.edu.au/vdu/HDUHaemoglobinopathies.htm • globin.cse.psu.edu/globin/hbvar/ • sickle.bwh.harvard.edu/

56
Glossary Acidosis = An abnormal increase in the acidity of the body's fluids, caused either by accumulation of acids or by depletion of bicarbonates Aggregate = To gather into a mass, sum, or whole Amniocentesis = A procedure in which a small sample of amniotic fluid is drawn out of the uterus through a needle inserted in the abdomen. The fluid is then analyzed to detect genetic abnormalities in the foetus or to determine the sex of the foetus Anaemia = is a lack of red blood cells and/or Haemoglobin. This results in a reduced ability of blood to transfer oxygen to the tissues. Haemoglobin has to be present to ensure adequate oxygenation of all body tissues. Anaemia is the most common disorder of the blood. There are several kinds of anaemia, produced by a variety of underlying causes. Anaemia is classified by the size of the red blood cell: decreased (microcytic), normal (normocytic) or enlarged (macrocytic or megaloblastic). Atrophy = A wasting or decrease in size of a body organ, tissue, or part owing to disease, injury, or lack of use Autosome = A chromosome that is not a sex chromosome Cholelithiasis = gallstones = these are crystalline bodies formed within the body by accretion or concretion of normal or abnormal bile components Chorionic villus = One of the minute vascular projections of the foetal chorion that combines with maternal uterine tissue to form the placenta Chromosome = A threadlike linear strand of DNA and associated proteins in the nucleus of eukaryotic cells that carries the genes and functions in the transmission of hereditary information Codon = A sequence of three adjacent nucleotides constituting the genetic code that determines the insertion of a specific amino acid in a polypeptide chain during protein synthesis or the signal to stop protein synthesis Cortical bone = Cortical bone represents nearly 80% of the skeletal mass. It is also called compact bone, because it forms a protective outer shell around every bone in the body Erythrocytes = Red blood cells are the most common type of blood cell and are the vertebrate body's principal means of delivering oxygen to body tissues via the blood. Red blood cells are also known as erythrocytes, from Greek erythros for "red" and kytos for "hollow", nowadays translated as "cell". = RBCs Erythrocytosis = Temporary increase in the number of red blood cells Erythroid = relating to erythrocytes Erythropoeisis = The formation or production of red blood cells Extramedullary = outside the bone marrow Genotype = The genetic makeup, as distinguished from the physical appearance, of an organism or a group of organisms Haematopoietic = pertaining to the formation of blood or blood cells; "haemopoietic stem cells in bone marrow" Haematuria = the presence of blood in the urine; often a symptom of urinary tract disease Haemolysis = lysis of erythrocytes with the release of haemoglobin Haemolytic anaemia = anaemia resulting from destruction of erythrocytes Haemopoietic = pertaining to the formation of blood or blood cells; "haemopoietic stem cells in bone marrow" Haemorrhage = It is usually used to describe internal bleeding

57
Haemosiderin = a granular brown substance composed of ferric oxide; left from the breakdown of haemoglobin; can be a sign of disturbed iron metabolism Haemosiderosis = abnormal deposit of haemosiderin; often a symptom of thalassaemia or haemochromatosis Hepatomegaly = Abnormal enlargement of the liver Hypersplenism = spleen and a decrease in one or more types of blood cells; associated with many disorders Hypertrophy = is the increase of the size of an organ Hypochromic = abnormal decrease in the haemoglobin content of the erythrocytes Hypoglycaemia = is a medical term referring to a pathologic state produced and usually defined by a lower than normal amount of sugar (glucose) in the blood Hyposthenuria = A condition characterized by inability to form urine of high specific gravity Hypoxia = lack of oxygen in tissues Hypoxic = Hypoxia is the lack of oxygen in tissues In Utero = in the uterus Inclusion = any small intracellular body found within another (characteristic of certain diseases); "an inclusion in the cytoplasm of the cell" Intrauterine = Occurring or situated within the uterus Ischaemia = local anaemia in a given body part sometimes resulting from vasoconstriction or thrombosis or embolism Jaundice = Yellowish discoloration of the whites of the eyes, skin, and mucous membranes caused by deposition of bile salts in these tissues. It occurs as a symptom of various diseases, such as hepatitis, that affect the processing of bile. Also called icterus Malaria Tropica = An infectious disease characterized by cycles of chills, fever, and sweating, caused by a protozoan of the genus Plasmodium in red blood cells, which is transmitted to humans by the bite of an infected female anopheles mosquito Microcytic = abnormally small RBCs Microcytosis = a blood disorder characterized by the presence of microcytes (abnormally small red blood cells) in the blood; often associated with anaemia Microvasculature = The portion of the circulatory system composed of the smallest vessels, such as the capillaries, arterioles, and venules Neonatal = Of or relating to newborn infants or an infant Normochromic = having a normal haemoglobin content Normocytic = RBCs with a normal size Osmotic fragility = Osmotic fragility is a test to detect abnormal fragility of red blood cells Phagocytosis = process in which phagocytes engulf and digest micro organisms and cellular debris; an important defence against infection Phenocopy = An environmentally induced, nonhereditary variation in an organism, closely resembling a genetically determined trait Phenotype = The observable physical or biochemical characteristics of an organism, as determined by both genetic makeup and environmental influences Plasmodium falciparum = tropica parasite = cause of malaria tropica Polypeptide = A peptide, such as a small protein, containing many molecules of amino acids, typically between 10 and 100

58
Postpartum = this is the period beginning immediately after the birth of a child and extending for about six weeks. The period is also known as postnatal (Latin for 'after birth') and, less commonly, puerperium Protoporphyrin = A metal-free porphyrin, C32H32N4(COOH)2, that combines with ferrous iron to form the haem group in haemoglobin and myoglobin, and with ferric iron to form the haemin group in catalase and some cytochromes RBC = Red Blood Cell Sequelae = A pathological condition resulting from a disease Sequestration = the action of forming a chelate or other stable compound with an ion or atom or molecule so that it is no longer available for reactions Splenectomy = Surgical removal of the spleen Splenomegaly = Enlargement of the spleen Target cells = periphery and central zone of the RBC are rich in haemoglobin whereas an intermediate rim is devoid of colour (looks like a target) Thrombosis = the formation or presence of a thrombus (a clot of coagulated blood attached at the site of its formation) in a blood vessel Toxaemia = Pre-eclampsia (previously called toxaemia) is a hypertensive disorder of pregnancy. It is said to exist when a pregnant woman with gestational hypertension develops proteinuria. Originally, oedema was considered part of the syndrome of pre-eclampsia, but presently the former two symptoms are sufficient for a diagnosis of pre-eclampsia. Transcription = The process by which messenger RNA is synthesized from a DNA template resulting in the transfer of genetic information from the DNA molecule to the messenger RNA Translation = The process by which messenger RNA directs the amino acid sequence of a growing polypeptide during protein synthesis Vaso-occlusive = blocking of the blood vessels


















