G. Edrosolo CNL Poster2
1
RESEARCH POSTER PRESENTATION DESIGN © 2012 www.PosterPresentations.com • Operationalize the role of the Clinical Nurse Leader (CNL) in the intensive care unit (ICU) through implementation of the Clinical Nurse Partner (CNP). • Improve patient outcomes in the ICU by decreasing healthcare acquired conditions. • Provide additional resource for bedside clinicians for consultation. • Provide assistance to the multi-disciplinary team in navigating through systems issues. • Ensure consistency of care in the ICU by assisting in the coordination of care, communication among providers regarding institutional policies, and implementation of evidence-based practice through education at the point of care. Objec4ves Clinical Microsystem Definition: The administrative team chose to call this role a Clinical Nurse Partner (CNP) versus a Clinical Nurse Leader (CNL) to maintain professional integrity because the team envisioned the role to be filled by staff nurses who currently work in the microsystem. At the time this role was proposed, none of the staff members had completed a formal CNL education program. Additionally, this role was a pilot project and continuation was contingent on the successful implementation and evaluation of the CNP. The CNP was modeled after the assumptions, roles, and competencies outlined in the American Association of Colleges of Nursing CNL White Paper. Methods • Eight-hour shifts, five days a week (40 hours a week divided among three nurses) • Daily rounding on at least 16 of the 32 patients in the ICU • New admissions and patients with the highest acuity seen first • Those with high risk therapy or procedures prioritized (i.e. CRRT) • Each patient’s orders reviewed and any discrepancies addressed • CNP conducts an assessment at each bedside and delivers education, conducts intervention(s), or assists with resolving systems issues if needed • Clinical focus every two weeks for staff education The CNP Opera4onalized Project Timeline Table 2: Projected Cost Savings from 10% Decrease of HACs *Shannon et al., 2006 **Stone, Braccia, & Larson, 2005 ***Rello et al., 2002 **** Coussement et al., 2008; Stevens, Corso, & Miller, 2006 ^ Amlung, Miller, & Bosley, 2001; Clever, Smith, Bowser, & Monroe, 2002 ^^Amlung et al., 2001; Clever et al., 2002 Preliminary Results Projected Results Giancarlo Fortunato Edrosolo MSN, RN, CNL, CCRNCMC, CPhT Design, Implementa/on, and Evalua/on of the Clinical Nurse Leader in the Intensive Care Unit The Clinical Nurse Partner: Assessment conducted. Business plan proposed to ICU administration team. Project timeline established. Manager approved and made edits. Frequency of staff meetings (non- productive hours) reduced to make way for the CNP role. ICU Manager proposed this plan as a quality improvement and pilot project to Associate Chief Nursing Officer. Project approved. Role introduced to unit leadership team and staff during monthly meeting. Job posting announced to ICU employees. Three staff nurses hired into role. Meetings conducted with administrative team and clinical nurse specialist to define the role of the CNP. CNP implemented in the unit. A unit champion was identified. The admin team, champion, and CNS were available to the CNPs for consultation with clinical issues, hospital policy clarification, and any other needs. Informal weekly touch- base meetings conducted by the unit champion. Additionally, a formal meeting with administrative team was scheduled every eight weeks. Unit outcomes tracked per protocol. Evaluation at the following phases of the implementation time line (three, six, and nine months from implementation date) to assess the effectiveness of the intervention, determine clinical focus, discuss barriers, evaluate quality data and strategize on the next intervention(s) moving forward. Root Cause Analysis 32-bed ICU in California 20 primary services that can admit patients into the ICU 19 Unlicensed Assistive Personnel 1 CNS 15 Nurse Practitioners 1 Social Worker 31 critical care Attendings, 16 Fellows, 2-4 Residents rotating every week from various services 149 Nurses
-
Upload
giancarlo-lyle-edrosolo -
Category
Documents
-
view
122 -
download
0
Transcript of G. Edrosolo CNL Poster2

RESEARCH POSTER PRESENTATION DESIGN © 2012
www.PosterPresentations.com
QUICK DESIGN GUIDE (--THIS SECTION DOES NOT PRINT--)
This PowerPoint 2007 template produces a 36x48 inch professional poster. You can use it to create your research poster and save valuable time placing titles, subtitles, text, and graphics. We provide a series of online tutorials that will guide you through the poster design process and answer your poster production questions. To view our template tutorials, go online to PosterPresentations.com and click on HELP DESK. When you are ready to print your poster, go online to PosterPresentations.com. Need Assistance? Call us at 1.866.649.3004
Object Placeholders
Using the placeholders To add text, click inside a placeholder on the poster and type or paste your text. To move a placeholder, click it once (to select it). Place your cursor on its frame, and your cursor will change to this symbol Click once and drag it to a new location where you can resize it. Section Header placeholder Click and drag this preformatted section header placeholder to the poster area to add another section header. Use section headers to separate topics or concepts within your presentation. Text placeholder Move this preformatted text placeholder to the poster to add a new body of text. Picture placeholder Move this graphic placeholder onto your poster, size it first, and then click it to add a picture to the poster.
Student discounts are available on our Facebook page. Go to PosterPresentations.com and click on the FB icon.
QUICK TIPS (--THIS SECTION DOES NOT PRINT--)
This PowerPoint template requires basic PowerPoint (version 2007 or newer) skills. Below is a list of commonly asked questions specific to this template. If you are using an older version of PowerPoint some template features may not work properly.
Template FAQs
Verifying the quality of your graphics Go to the VIEW menu and click on ZOOM to set your preferred magnification. This template is at 100% the size of the final poster. All text and graphics will be printed at 100% their size. To see what your poster will look like when printed, set the zoom to 100% and evaluate the quality of all your graphics before you submit your poster for printing. Modifying the layout This template has four different column layouts. Right-click your mouse on the background and click on LAYOUT to see the layout options. The columns in the provided layouts are fixed and cannot be moved but advanced users can modify any layout by going to VIEW and then SLIDE MASTER. Importing text and graphics from external sources TEXT: Paste or type your text into a pre-existing placeholder or drag in a new placeholder from the left side of the template. Move it anywhere as needed. PHOTOS: Drag in a picture placeholder, size it first, click in it and insert a photo from the menu. TABLES: You can copy and paste a table from an external document onto this poster template. To adjust the way the text fits within the cells of a table that has been pasted, right-click on the table, click FORMAT SHAPE then click on TEXT BOX and change the INTERNAL MARGIN values to 0.25. Modifying the color scheme To change the color scheme of this template go to the DESIGN menu and click on COLORS. You can choose from the provided color combinations or create your own.
© 2013 PosterPresenta/ons.com 2117 Fourth Street , Unit C Berkeley CA 94710 [email protected]
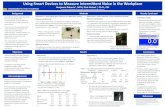
• Operationalize the role of the Clinical Nurse Leader (CNL) in the intensive care unit (ICU) through implementation of the Clinical Nurse Partner (CNP).
• Improve patient outcomes in the ICU by decreasing healthcare acquired conditions.
• Provide additional resource for bedside clinicians for consultation. • Provide assistance to the multi-disciplinary team in navigating through
systems issues. • Ensure consistency of care in the ICU by assisting in the coordination of care,
communication among providers regarding institutional policies, and implementation of evidence-based practice through education at the point of care.
Objec4ves
Clinical Microsystem
Definition: The administrative team chose to call this role a Clinical Nurse Partner (CNP) versus a Clinical Nurse Leader (CNL) to maintain professional integrity because the team envisioned the role to be filled by staff nurses who currently work in the microsystem. At the time this role was proposed, none of the staff members had completed a formal CNL education program. Additionally, this role was a pilot project and continuation was contingent on the successful implementation and evaluation of the CNP. The CNP was modeled after the assumptions, roles, and competencies outlined in the American Association of Colleges of Nursing CNL White Paper.
Methods
• Eight-hour shifts, five days a week (40 hours a week divided among three nurses)
• Daily rounding on at least 16 of the 32 patients in the ICU • New admissions and patients with the highest acuity seen first • Those with high risk therapy or procedures prioritized (i.e. CRRT) • Each patient’s orders reviewed and any discrepancies addressed • CNP conducts an assessment at each bedside and delivers
education, conducts intervention(s), or assists with resolving systems issues if needed
• Clinical focus every two weeks for staff education
The CNP Opera4onalized
Project Timeline
Table 2: Projected Cost Savings from 10% Decrease of HACs *Shannon et al., 2006 **Stone, Braccia, & Larson, 2005 ***Rello et al., 2002 **** Coussement et al., 2008; Stevens, Corso, & Miller, 2006 ^ Amlung, Miller, & Bosley, 2001; Clever, Smith, Bowser, & Monroe, 2002 ^^Amlung et al., 2001; Clever et al., 2002
Preliminary Results
Projected Results
Giancarlo Fortunato Edrosolo MSN, RN, CNL, CCRN-‐CMC, CPhT
Design, Implementa/on, and Evalua/on of the Clinical Nurse Leader in the Intensive Care Unit The Clinical Nurse Partner:
Assessment conducted. Business plan proposed to ICU administration team. Project timeline established. Manager approved and made edits. Frequency of staff meetings (non-productive hours) reduced to make way for the CNP role. ICU Manager proposed this plan as a quality improvement and pilot project to Associate Chief Nursing Officer. Project approved.
Role introduced to unit leadership team and staff during monthly meeting. Job posting announced to ICU employees. Three staff nurses hired into role. Meetings conducted with administrative team and clinical nurse specialist to define the role of the CNP. CNP implemented in the unit. A unit champion was identified.
The admin team, champion, and CNS were available to the CNPs for consultation with clinical issues, hospital policy clarification, and any other needs. Informal weekly touch-base meetings conducted by the unit champion. Additionally, a formal meeting with administrative team was scheduled every eight weeks. Unit outcomes tracked per protocol.
Evaluation at the following phases of the implementation time line (three, six, and nine months from implementation date) to assess the effectiveness of the intervention, determine clinical focus, discuss barriers, evaluate quality data and strategize on the next intervention(s) moving forward.
Root Cause Analysis
32-bed ICU in
California
20 primary services that can admit
patients into the ICU
19 Unlicensed Assistive Personnel
1 CNS
15 Nurse Practitioners 1 Social Worker
31 critical care Attendings, 16 Fellows, 2-4
Residents rotating every week from various services
149 Nurses