
G. B. Migliori WHO Collaborating Centre for TB and Lung Disease, Fondazione S. Maugeri, Care and...
77
G. B. Migliori WHO Collaborating Centre for TB and Lung Disease, Fondazione S. Maugeri, Care and Research Institut Tradate, Italy MDR-/XDR-TB: is the white plague spectrum back?
-
Upload
allen-crawford -
Category
Documents
-
view
214 -
download
0
Transcript of G. B. Migliori WHO Collaborating Centre for TB and Lung Disease, Fondazione S. Maugeri, Care and...
G. B. MiglioriWHO Collaborating Centre for TB and Lung Disease,Fondazione S. Maugeri, Care and Research InstituteTradate, Italy
MDR-/XDR-TB: is the white plague spectrum back?
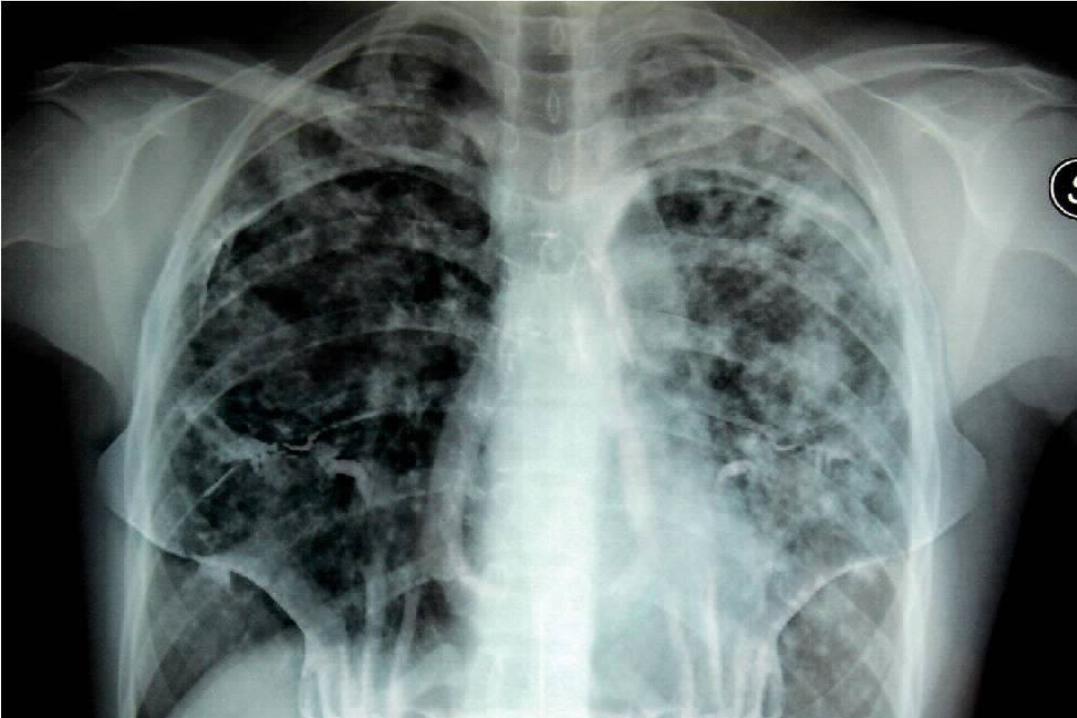
Q1: the 2 previous slides show that
1) M/XDR-TB is dangerous like a wild animal
2) M/XDR-TB is a clinical nightmare
3) M/XDR-TB is a death sentence
4) M/XDR-TB is a problem in Africa
Aims
• Demonstrate that M/XDR-TB is a real (global) threat to TB control, and urgent action is needed
• Call for more research on key priorities
• Advocate for the collaboration of European Chest Physicians

Outline
• Definitions
• Epidemiology
• How does M/XDR-TB develop?
• How is M/XDR-TB diagnosed?
• Can M/XDR-TB be cured?
• What can we do to prevent M/XDR-TB?

Outline
• Definitions
• Epidemiology
• How does M/XDR-TB develop?
• How is M/XDR-TB diagnosed?
• Can M/XDR-TB be cured?
• What can we do to prevent M/XDR-TB?

8
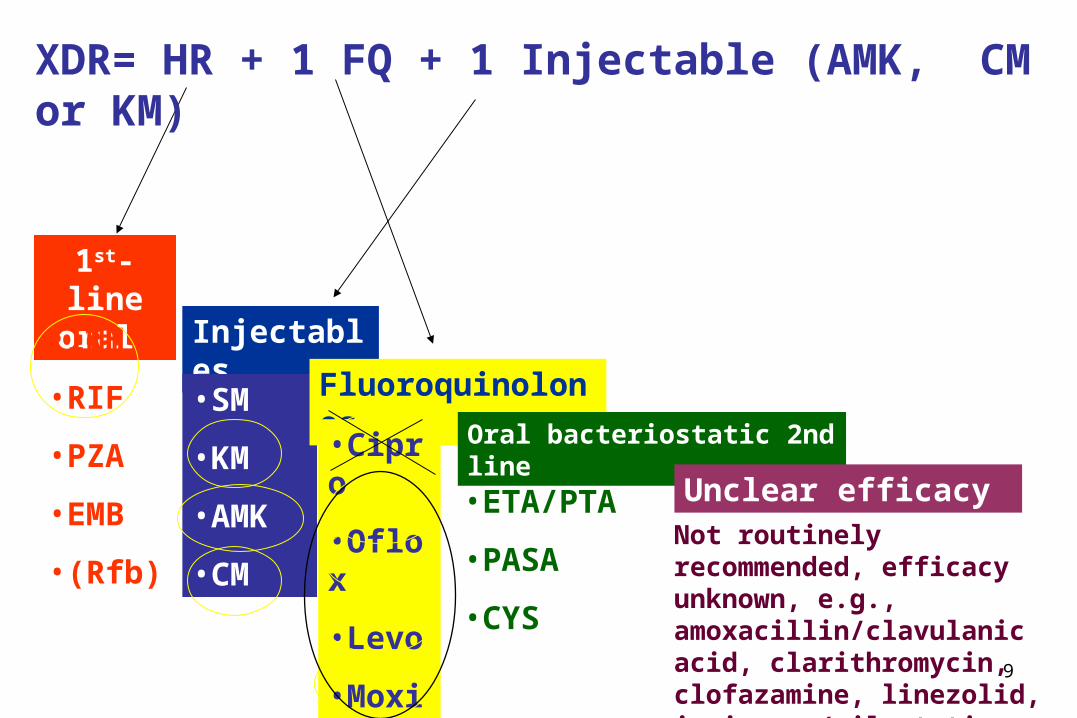
XDR= extensively drug-resistant TB
Definition
Resistance to at least rifampicin and isoniazid, in addition to any fluoroquinolone, and to at least one of the three following injectable drugs used in anti-TB treatment: capreomycin, kanamycin and amikacin.
9
1st-line oral
•INH
•RIF
•PZA
•EMB
•(Rfb)
Injectables
•SM
•KM
•AMK
•CM
Fluoroquinolones
•Cipro
•Oflox
•Levo
•Moxi
•(Gati)
Oral bacteriostatic 2nd line
Unclear efficacy•ETA/PTA
•PASA
•CYS
Not routinely recommended, efficacy unknown, e.g., amoxacillin/clavulanic acid, clarithromycin, clofazamine, linezolid, inmipenem/cilastatin, high dose isonizid
XDR= HR + 1 FQ + 1 Injectable (AMK, CM or KM)
Outline
• Definitions
• Epidemiology
• How does M/XDR-TB develop?
• How is M/XDR-TB diagnosed?
• Can M/XDR-TB be cured?
• What can we do to prevent M/XDR-TB?

Q2: M/XDR is
1) Highly prevalent in specific settings
2) Highly prevalent outside Europe
3) Not affecting Africa
4) Identified whenever somebody looked for it

Countries that had reported at least oneXDR-TB case by end 2010
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. WHO 2010. All rights reserved
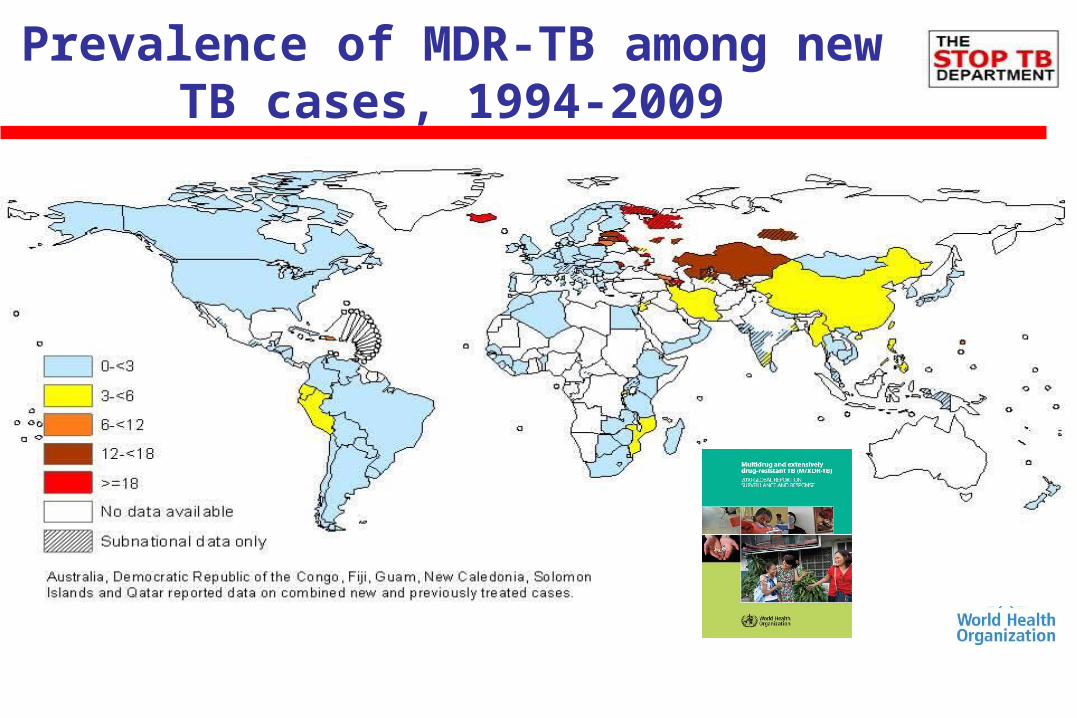
Prevalence of MDR-TB among new TB cases, 1994-2009

Prevalence of MDR-TB, retreatment cases, 1994-2009
15
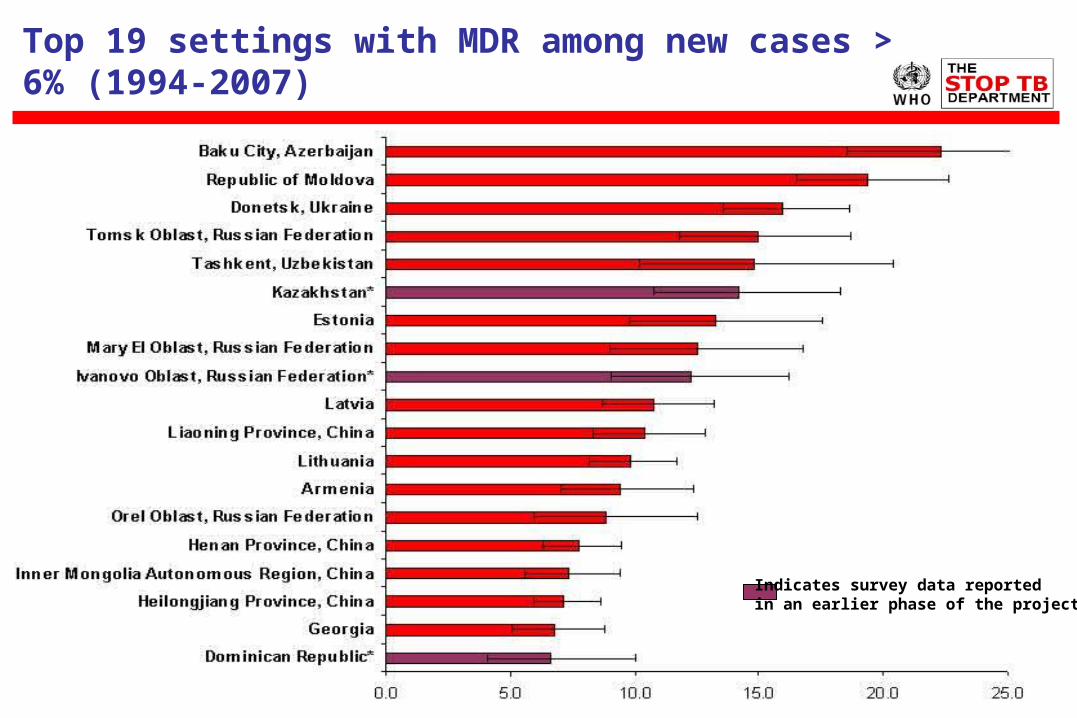
Top 19 settings with MDR among new cases > 6% (1994-2007)
Indicates survey data reported in an earlier phase of the project
M/XDR-TB is becoming, in selected settings, a time-bomb
Outline
• Definitions
• Epidemiology
• How does M/XDR-TB develop?
• How is M/XDR-TB diagnosed?
• Can M/XDR-TB be cured?
• What can we do to prevent M/XDR-TB?
Q3: MDR is
1) Difficult to select
2) Is mainly due to patient’s mistakes
3) Is mainly due to sub-standard drugs
4) Is a multi-factorial man-made phenomenon
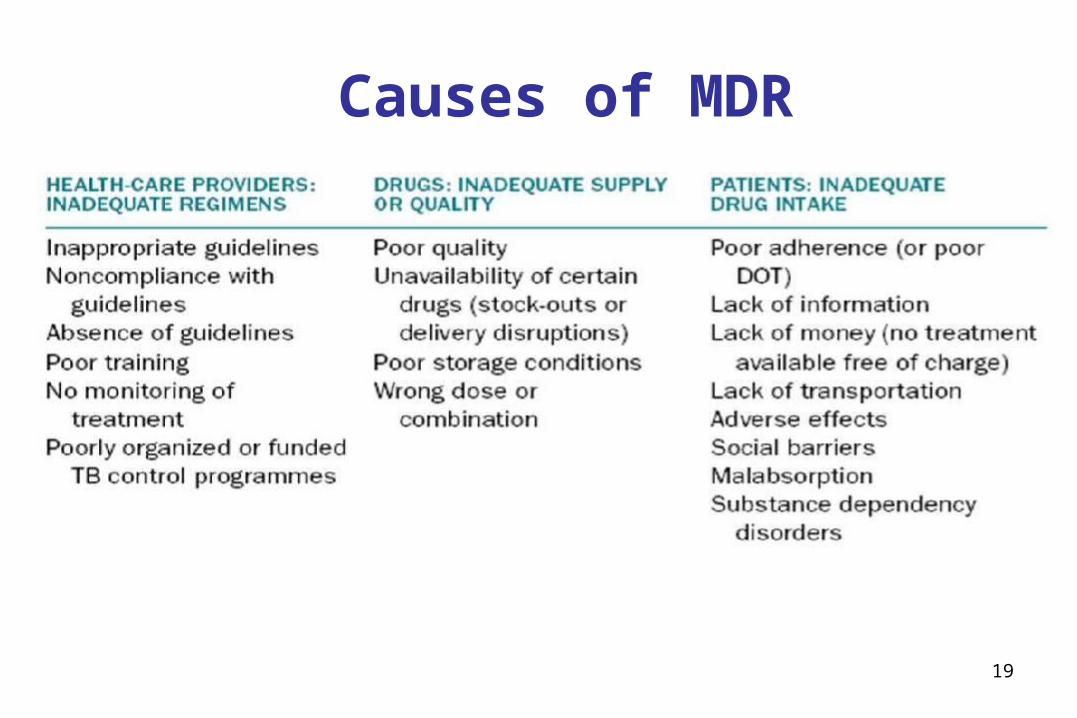
19
Causes of MDR
20
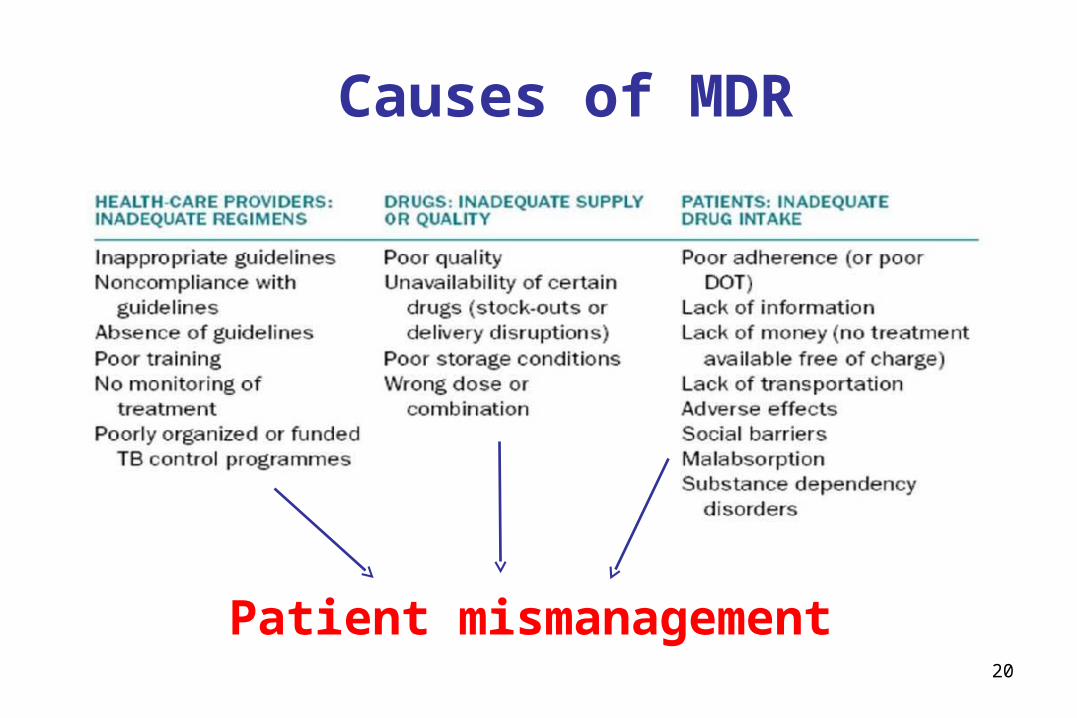
Causes of MDR
Patient mismanagement
21

22
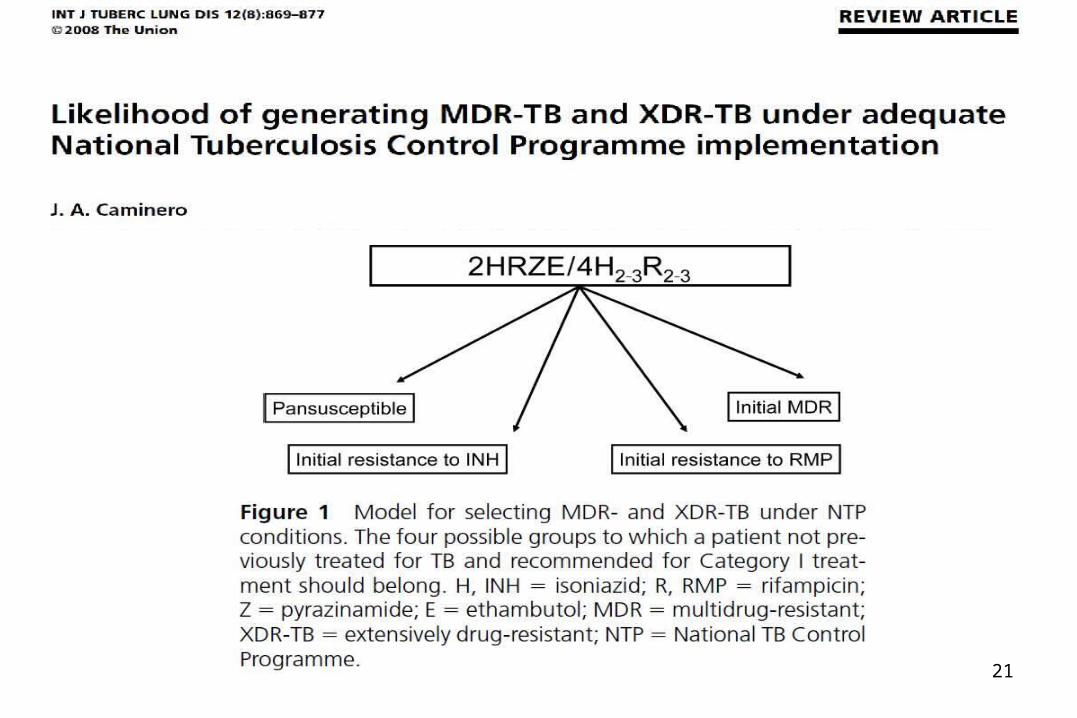
Step 1:Everything OKbut don’t miss the cure

23
Step 2:Single resistance,Danger ahead!
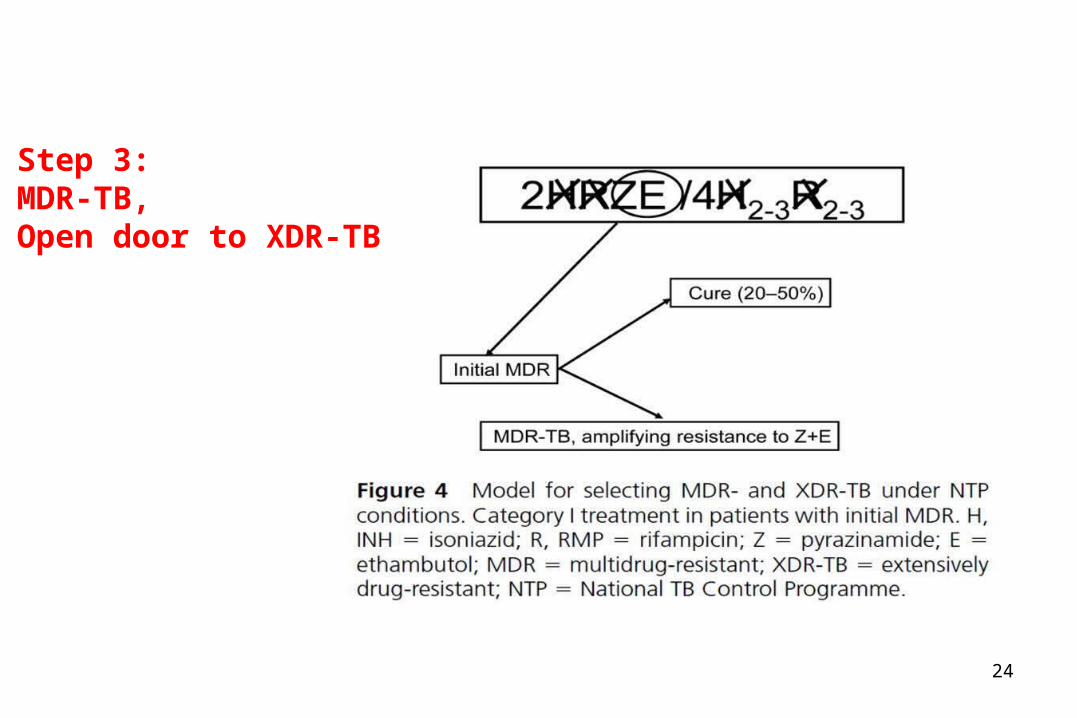
24
Step 3:MDR-TB,Open door to XDR-TB


MDR-/XDR-TB: a manmade product!

27
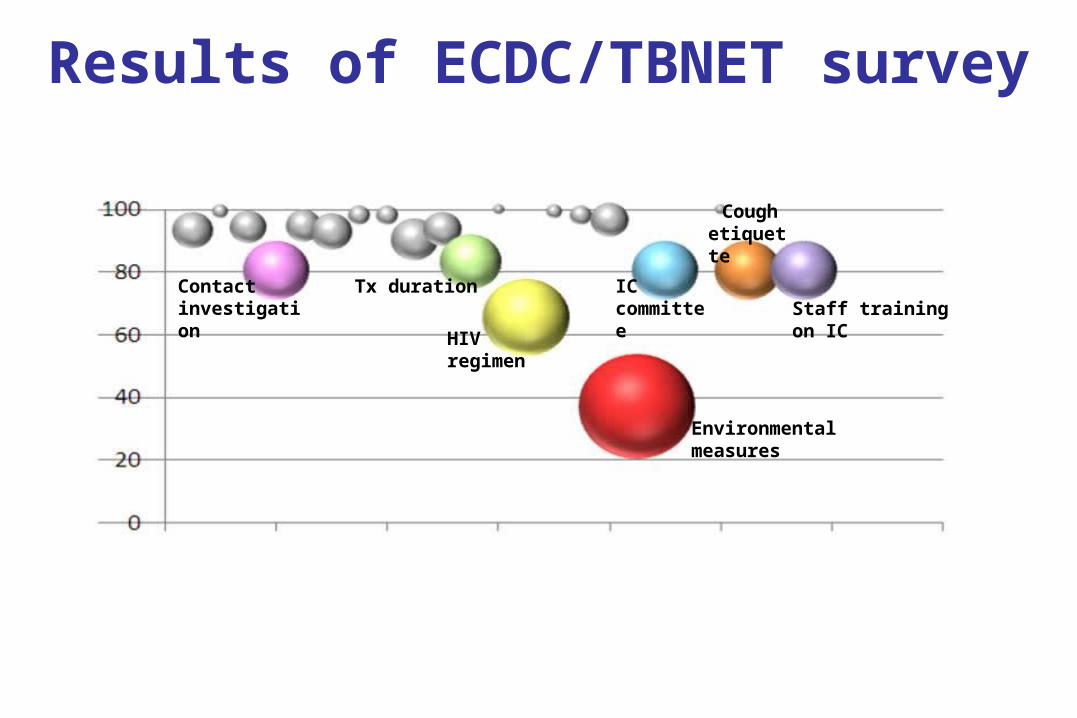
Results of ECDC/TBNET survey
Environmental measures
Contactinvestigation
HIV regimen
Tx duration ICcommittee
Coughetiquette
Staff training on IC

Results of ECDC/TBNET survey
Environmental measures
Contactinvestigation
HIV regimen
Tx duration ICcommittee
Coughetiquette
Staff training on IC

Surgical masks(yes for patients)
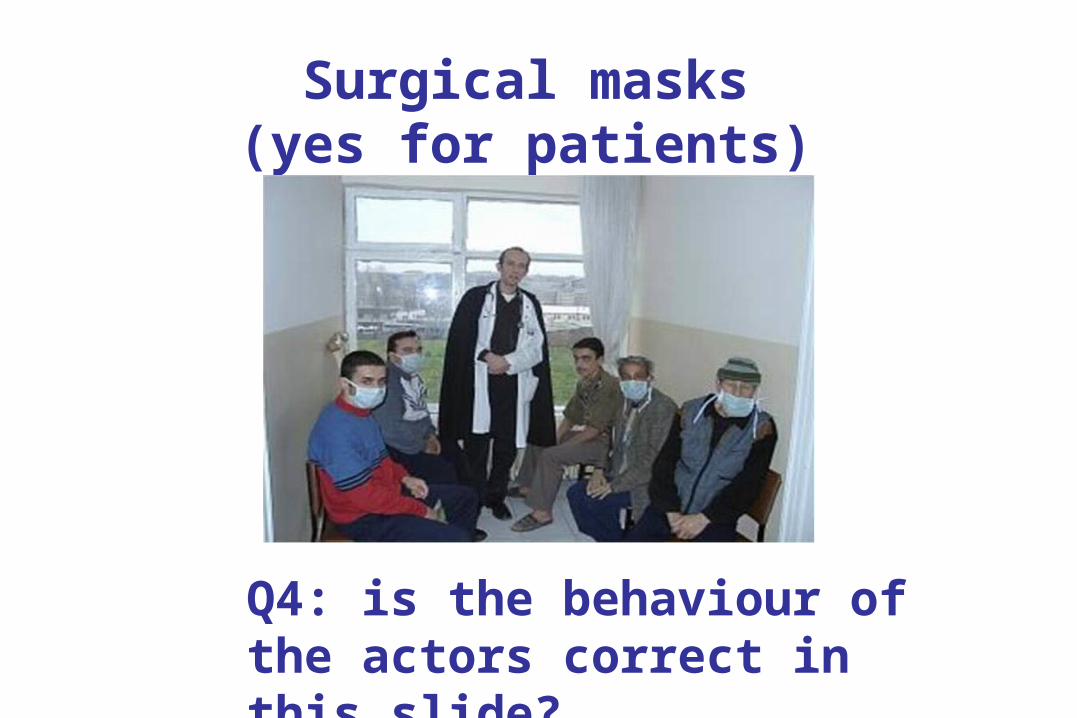
Surgical masks(yes for patients)
Q4: is the behaviour of the actors correct in this slide?

Fit test

Respiratory Fit Testing

WHO Policy on Infection control
1) Managerial activities
2) Administrative controls
3) Environmental controls
4) Personal protection
WHO Policy on Infection control
1) Managerial activities
2) Administrative controls
3) Environmental controls
4) Personal protection

TB Treatment: loopholes identified
Inadequate TB regimen choice (4 active drugs ensured), no. (%)
20/201 (10)
Inadequate dosage, no. (%) 13/201 (6.5)
Inadequate duration, no. (%) 34/201 (17)
Ineffective management adverse events TB treatment, no. (%)
1/201 (0.5)

Outline
• Definitions
• Epidemiology
• How does M/XDR-TB develop?
• How is M/XDR-TB diagnosed?
• Can M/XDR-TB be cured?
• What can we do to prevent M/XDR-TB?

Q5: the main recent advances on TB management were related to
1) Drugs
2) Vaccines
3) Diagnostics
4) Funding opportunities

Diagnosis by smear microscopyEastern Europe
Diagnosis, smear conversion, failure, cure
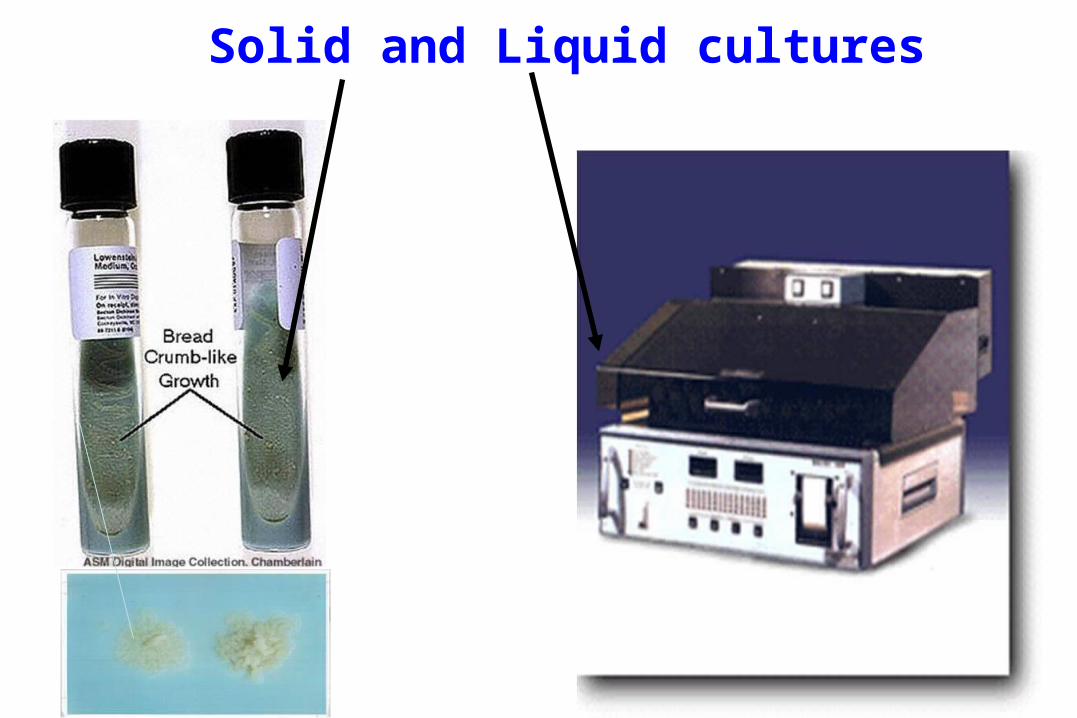
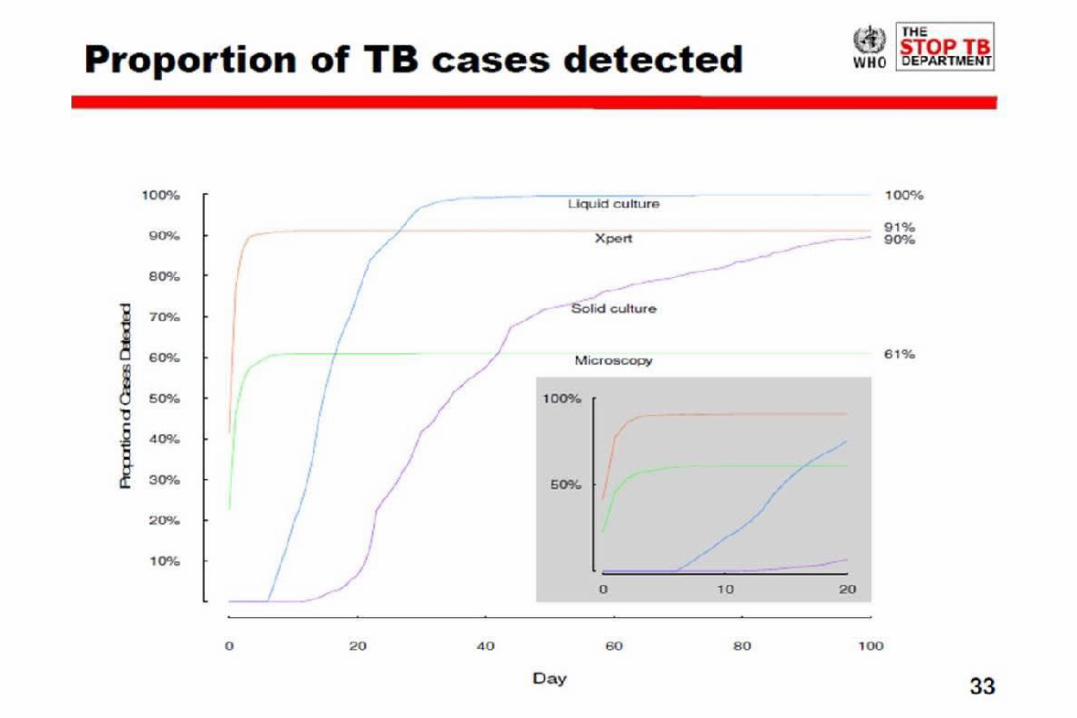
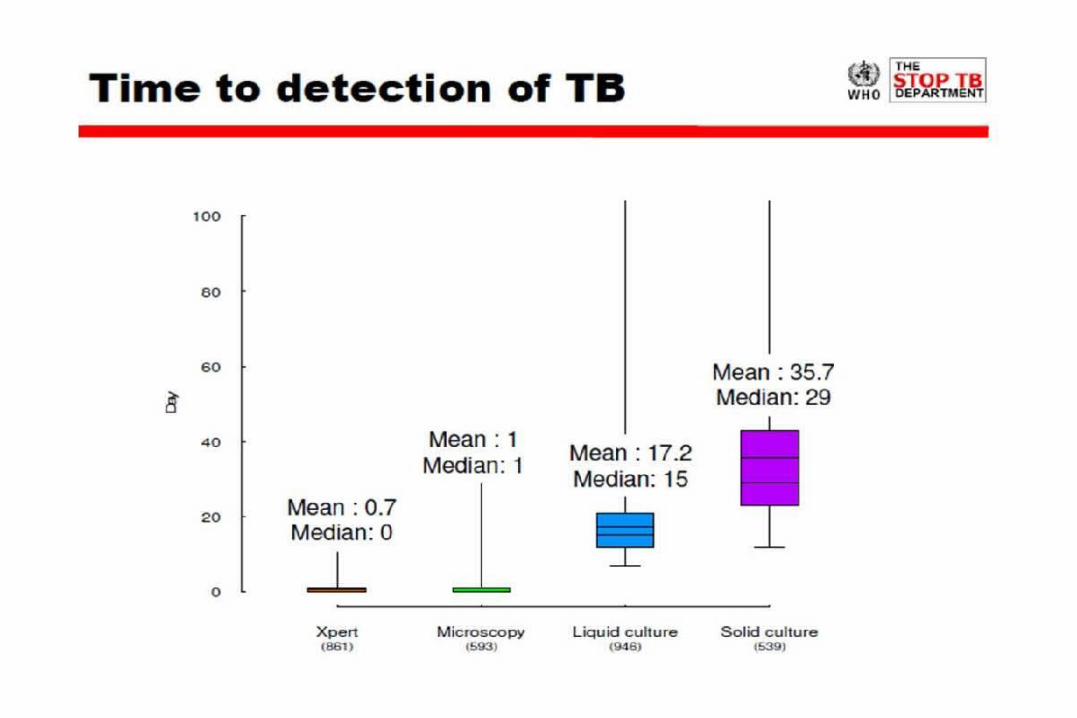
Solid and Liquid cultures
≥1
<1
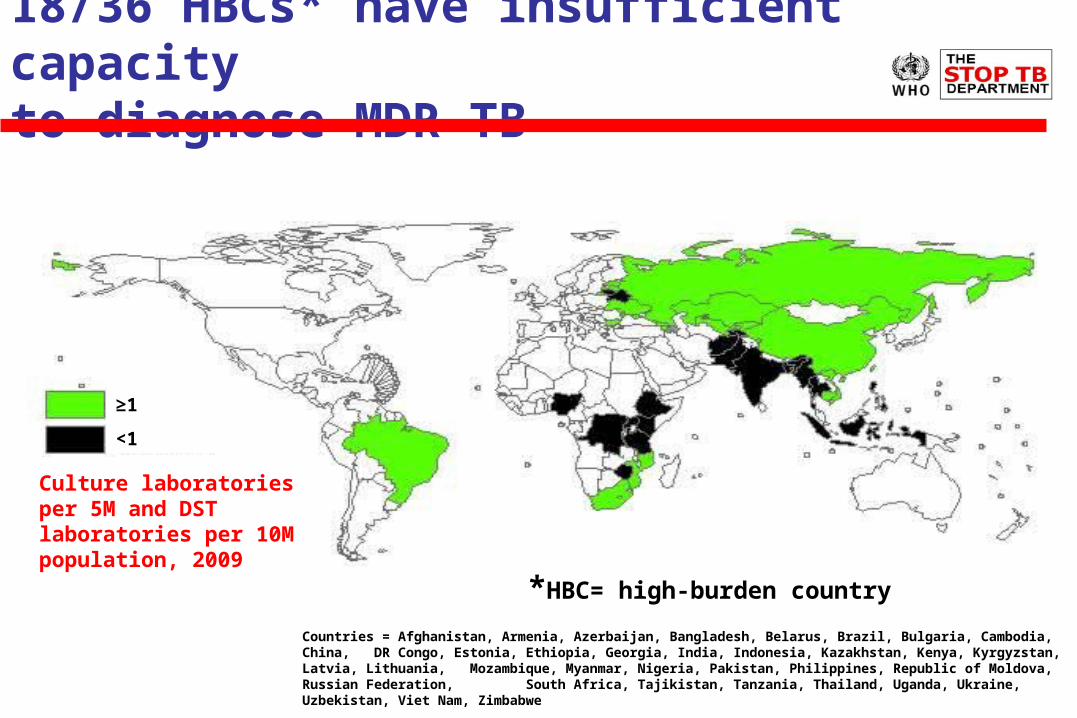
18/36 HBCs* have insufficient capacity to diagnose MDR-TB
*HBC= high-burden country
Countries = Afghanistan, Armenia, Azerbaijan, Bangladesh, Belarus, Brazil, Bulgaria, Cambodia, China, DR Congo, Estonia, Ethiopia, Georgia, India, Indonesia, Kazakhstan, Kenya, Kyrgyzstan, Latvia, Lithuania, Mozambique, Myanmar, Nigeria, Pakistan, Philippines, Republic of Moldova, Russian Federation, South Africa, Tajikistan, Tanzania, Thailand, Uganda, Ukraine, Uzbekistan, Viet Nam, Zimbabwe
Culture laboratories per 5M and DST laboratories per 10M population, 2009
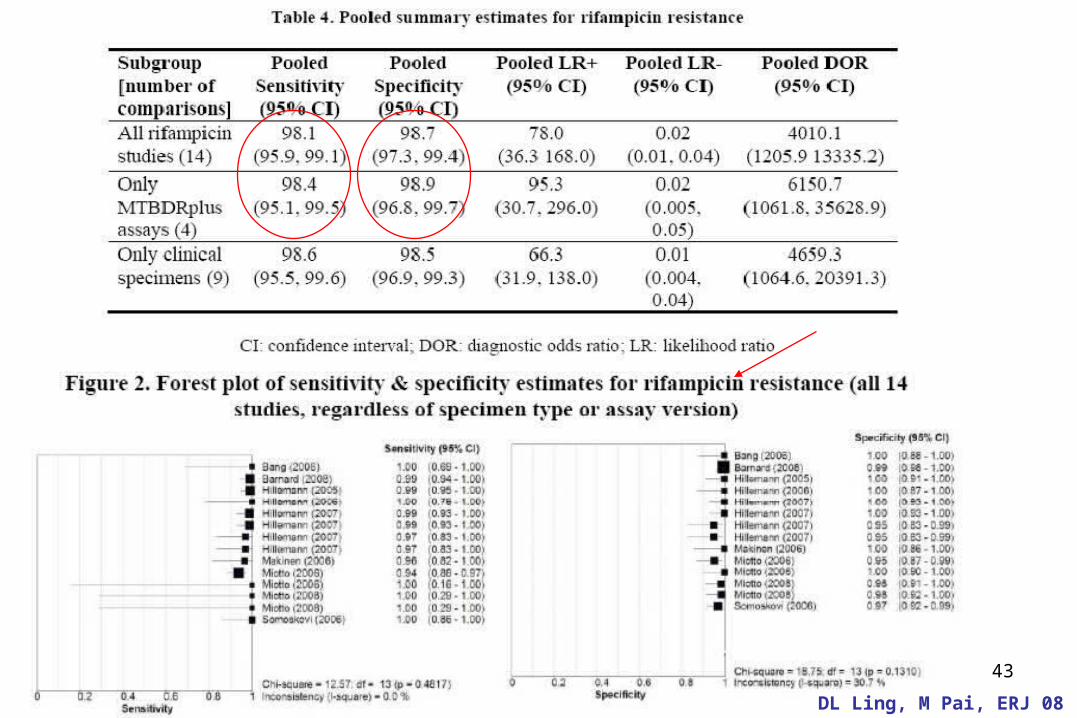
43
DL Ling, M Pai, ERJ 08

44
DL Ling, M Pai, ERJ 08

Examples of implications of introduction of Genotype MTBDRplus
Uzbekistan: 17% MDR among new cases, 45% among PT cases, 23% PT among all SS+ cases
• Before Hain: culture, 1st line DST for all SS+patients n= 6600, then 2nd line DST for R resistant cases n=1700
• After Hain: Hain test for all 6600 patients, followed by culture+ 1st+2nd line DST for H and/or R res cases n= 3400
• Advantages: – Early diagnosis and MDR treatment for R resistant cases (1700)– Early diagnosis and adequate treatment for H resistant cases (1700)– 50 % reduction of laboratory workload for culture/DST– Reduction in time to diagnosis of XDR TB
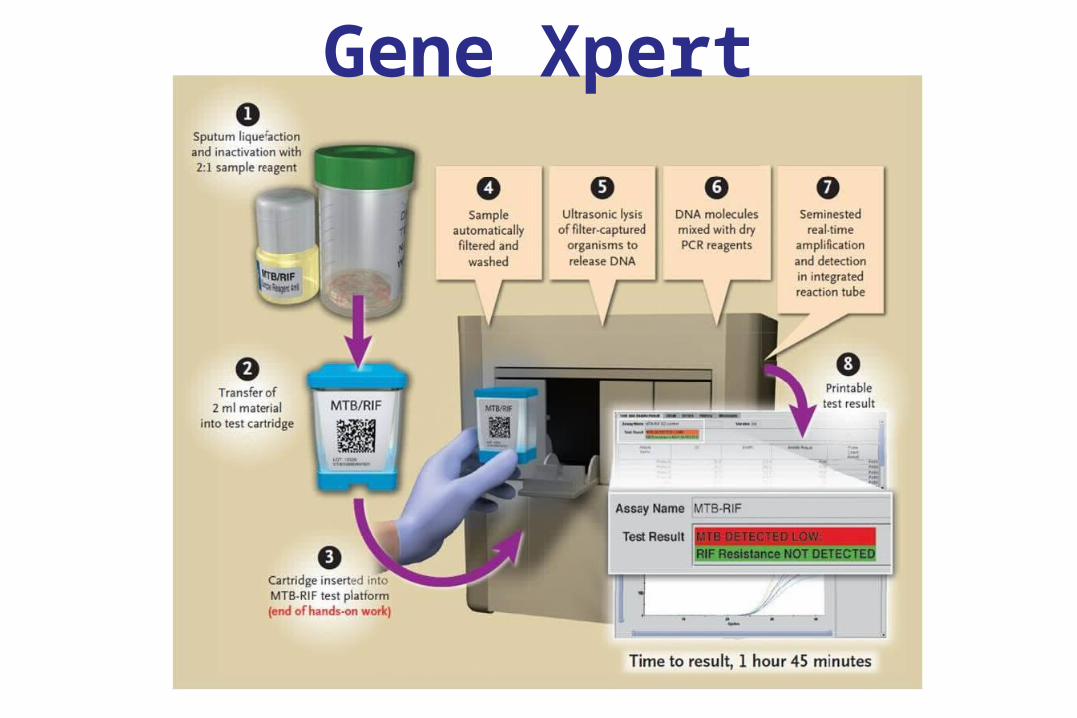
Gene Xpert
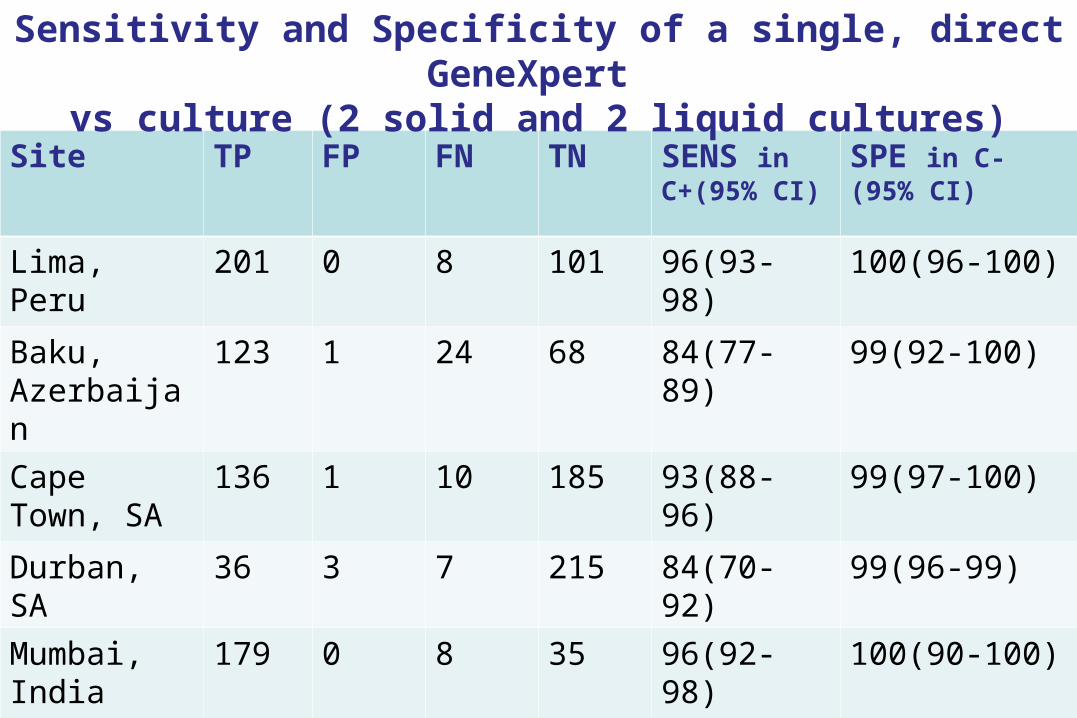
Site TP FP FN TN SENS in C+(95% CI)
SPE in C- (95% CI)
Lima, Peru 201 0 8 101 96(93-98) 100(96-100)
Baku, Azerbaijan
123 1 24 68 84(77-89) 99(92-100)
Cape Town, SA
136 1 10 185 93(88-96) 99(97-100)
Durban, SA 36 3 7 215 84(70-92) 99(96-99)
Mumbai, India
179 0 8 35 96(92-98) 100(90-100)
Total 675 5 57 604 92(90-94) 99(98-100)
Sensitivity and Specificity of a single, direct GeneXpert vs culture (2 solid and 2 liquid cultures)

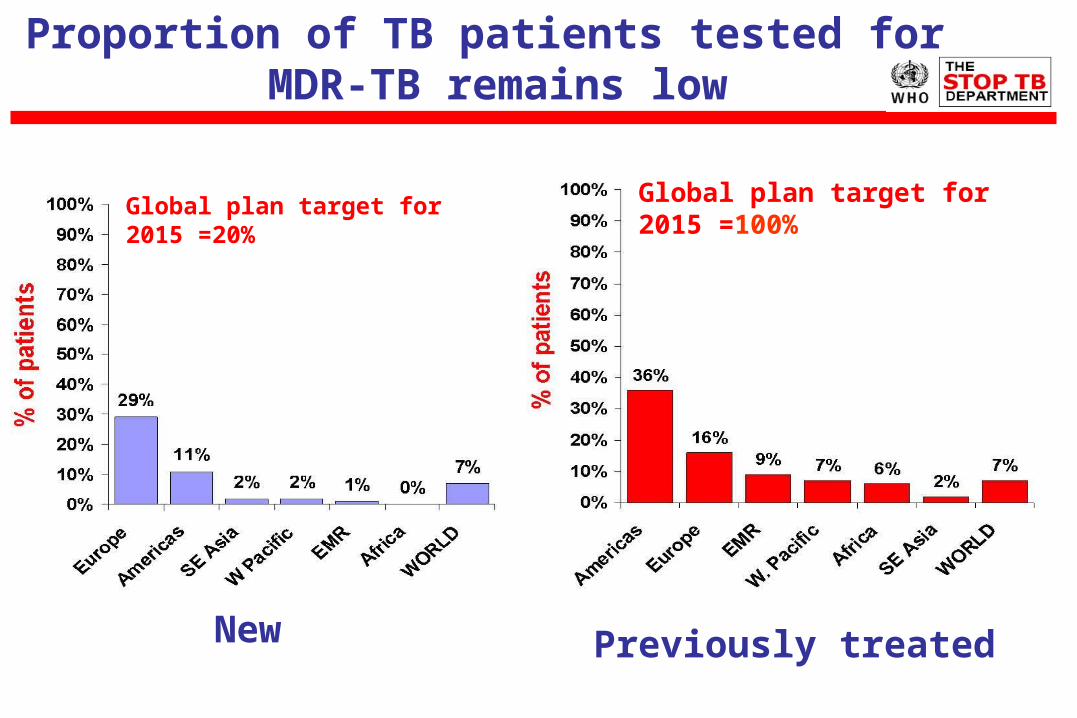
Proportion of TB patients tested for MDR-TB remains low
New
Global plan target for 2015 =20%
Previously treated
Global plan target for 2015 =100%
Outline
• Definitions
• Epidemiology
• How does M/XDR-TB develop?
• How is M/XDR-TB diagnosed?
• Can M/XDR-TB be cured?
• What can we do to prevent M/XDR-TB?
54
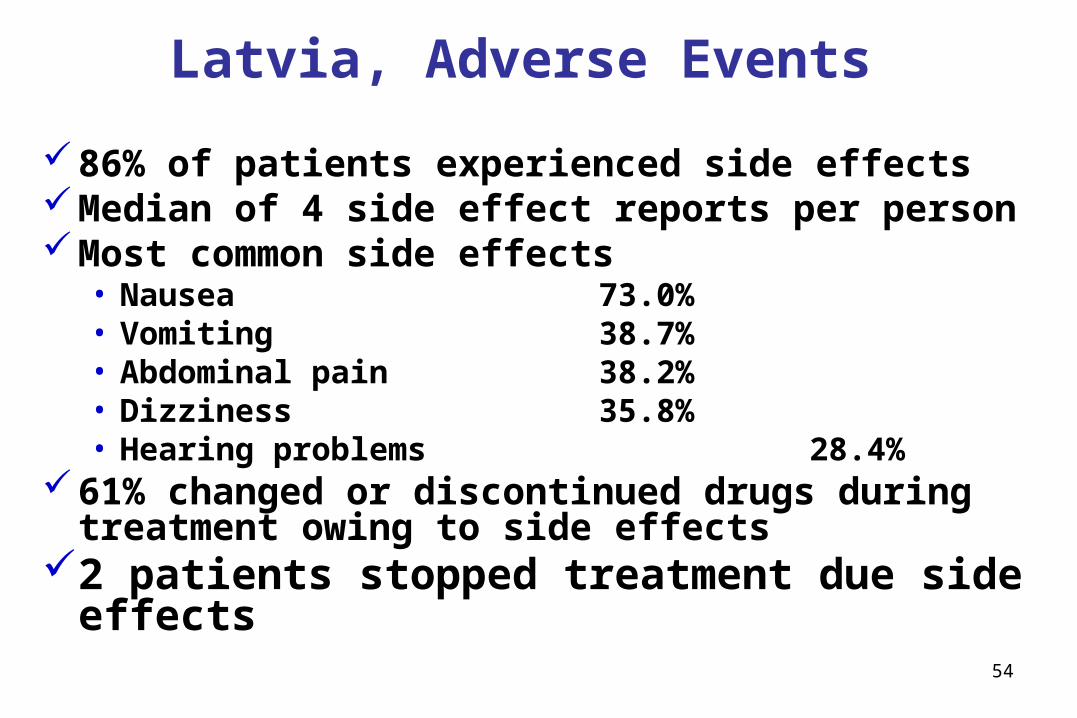
Latvia, Adverse Events
86% of patients experienced side effectsMedian of 4 side effect reports per personMost common side effects
• Nausea 73.0%• Vomiting 38.7%• Abdominal pain 38.2%• Dizziness 35.8%• Hearing problems 28.4%
61% changed or discontinued drugs during treatment owing to side effects
2 patients stopped treatment due side effects
55
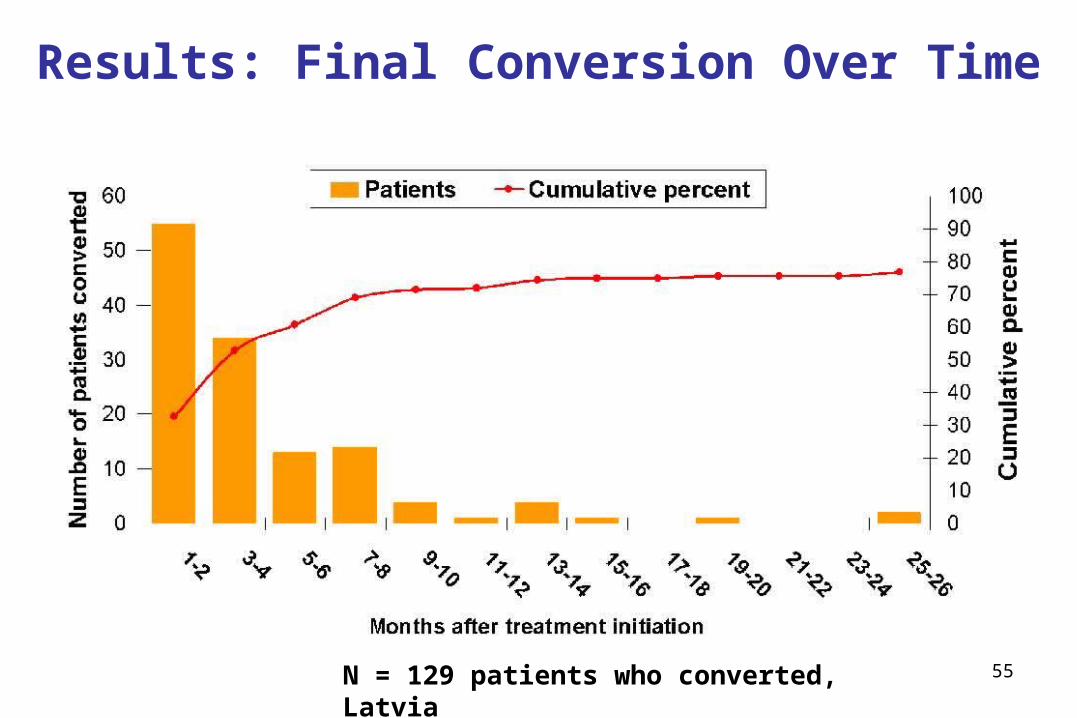
Results: Final Conversion Over Time
N = 129 patients who converted, Latvia

56
Consilium for MDR-TB case and programme management

57
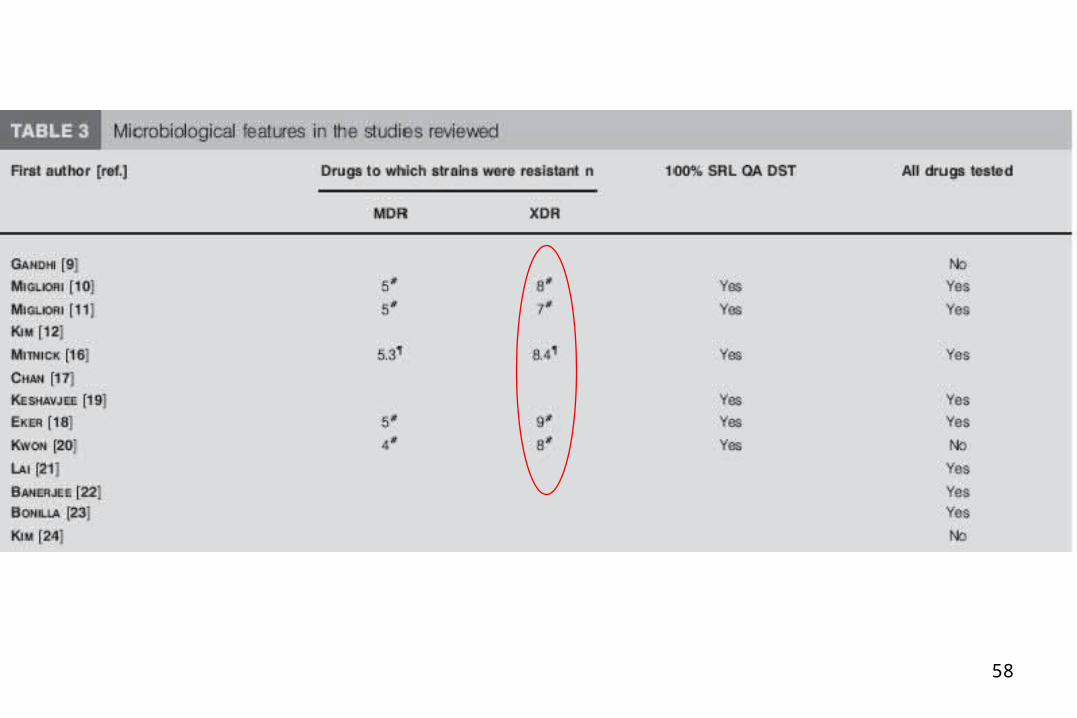
58

59
60
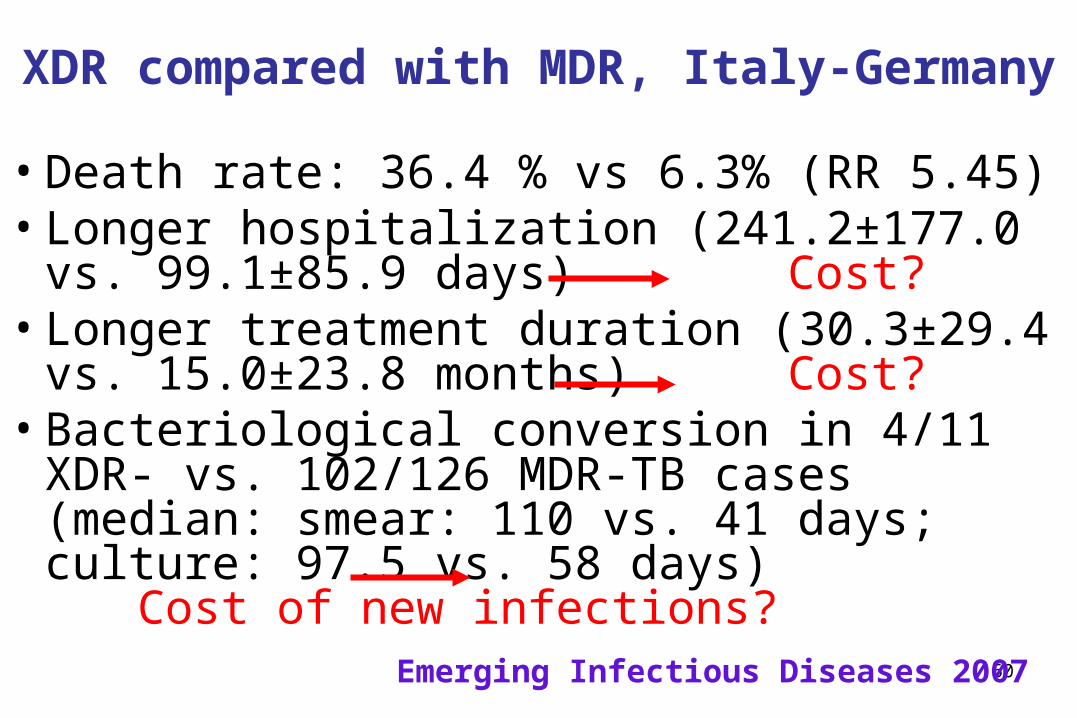
XDR compared with MDR, Italy-Germany
• Death rate: 36.4 % vs 6.3% (RR 5.45)• Longer hospitalization (241.2±177.0 vs.
99.1±85.9 days) Cost?• Longer treatment duration (30.3±29.4 vs.
15.0±23.8 months) Cost? • Bacteriological conversion in 4/11 XDR- vs.
102/126 MDR-TB cases (median: smear: 110 vs. 41 days; culture: 97.5 vs. 58 days)
Cost of new infections?
Emerging Infectious Diseases 2007
61
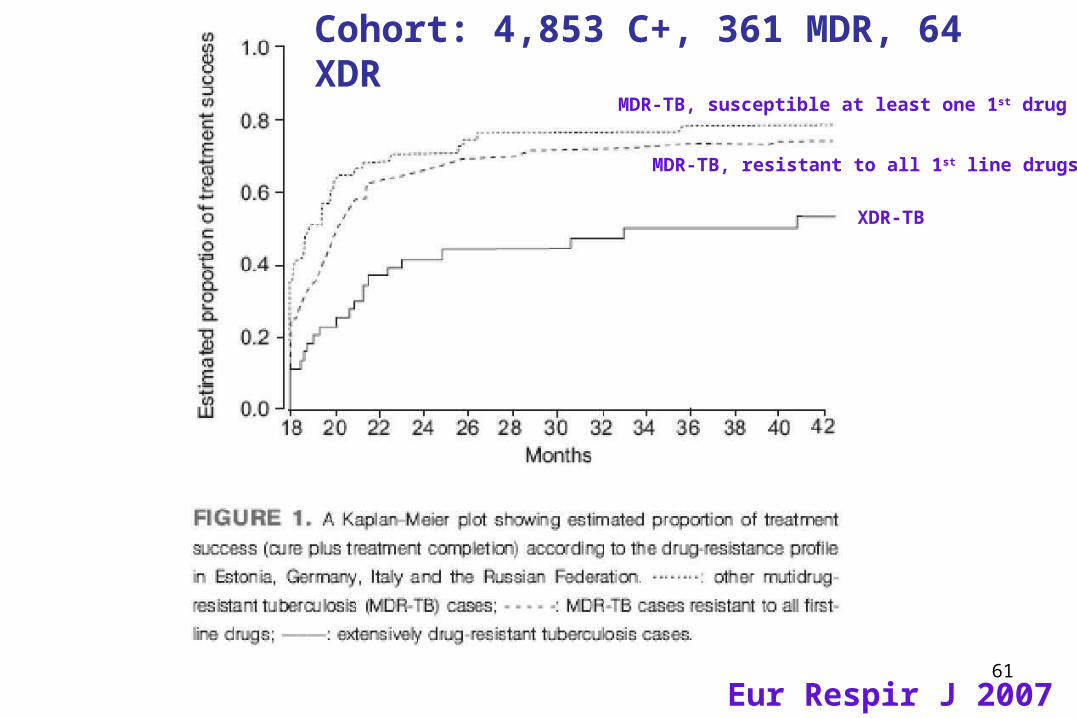
XDR-TB
MDR-TB, resistant to all 1st line drugs
MDR-TB, susceptible at least one 1st drug
Eur Respir J 2007
Cohort: 4,853 C+, 361 MDR, 64 XDR

62
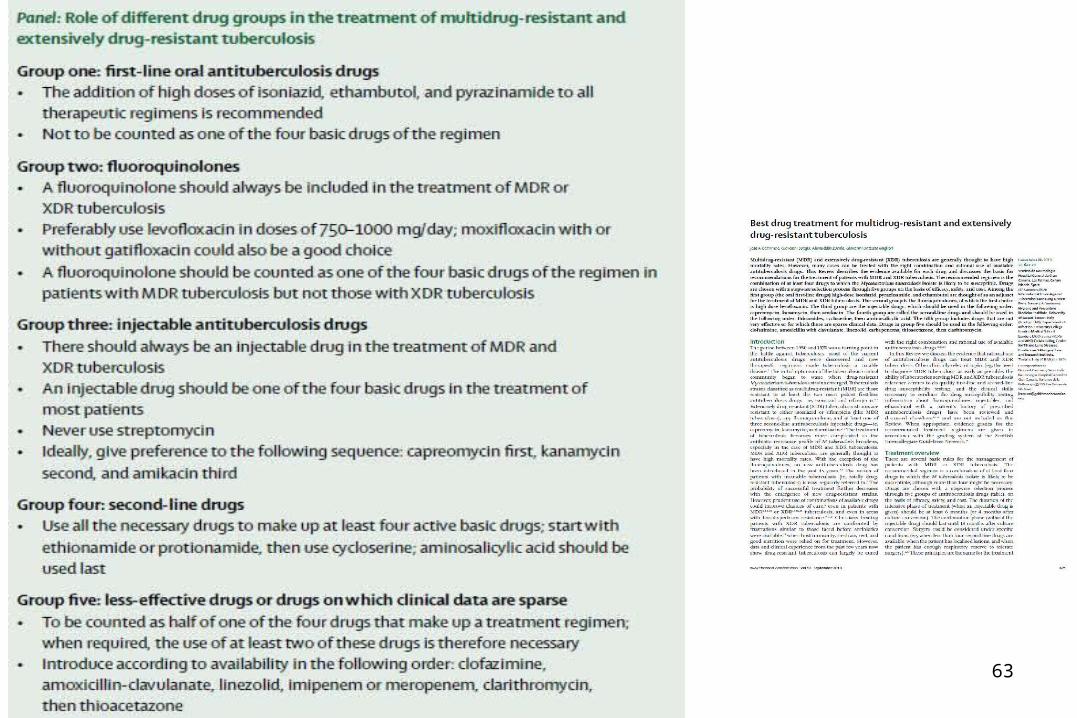
How to design a MDR-TB regimen
63

64

65

66
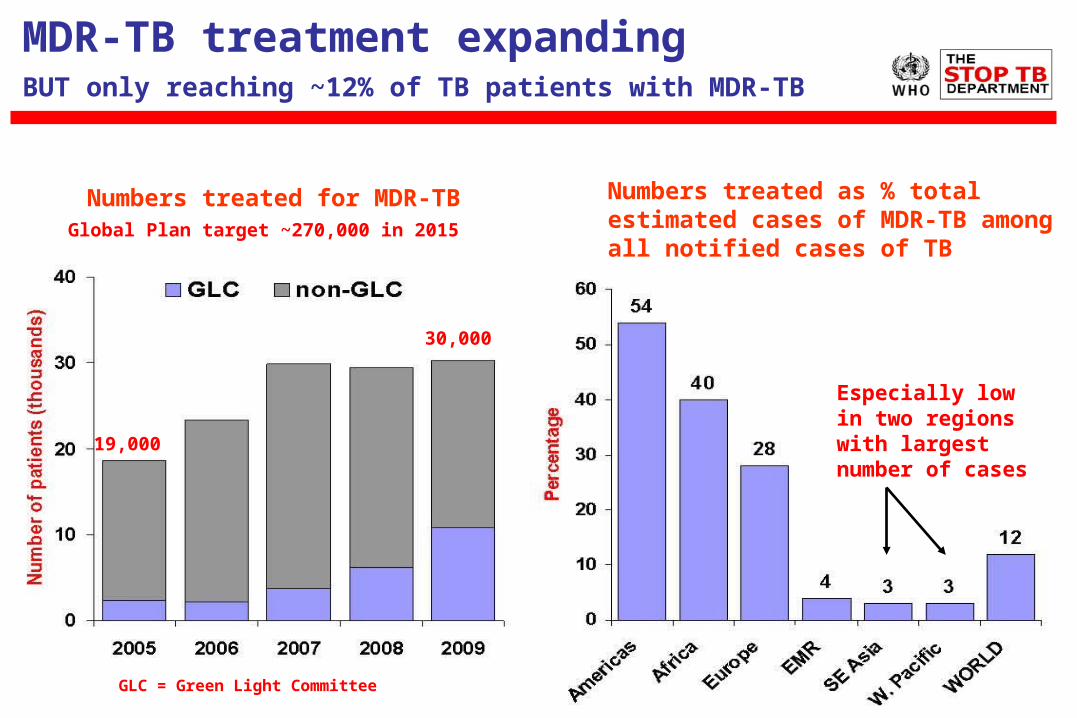
MDR-TB treatment expandingBUT only reaching ~12% of TB patients with MDR-TB
Numbers treated for MDR-TB Numbers treated as % total estimated cases of MDR-TB among all notified cases of TB
GLC = Green Light Committee
Global Plan target ~270,000 in 2015
30,000
19,000
Especially low in two regions with largest number of cases

Outline
• Definitions
• Epidemiology
• How does M/XDR-TB develop?
• How is M/XDR-TB diagnosed?
• Can M/XDR-TB be cured?
• What can we do to prevent M/XDR-TB?

69
Global Policy: MDR-TB and XDR-TB
1. Strengthen basic TB control, to prevent M/XDR-TB
2. Scale-up programmatic management and care of MDR-TB and XDR-TB
3. Strengthen laboratory services for adequate and timely diagnosis of MDR-TB and XDR-TB
4. Ensure availability of quality drugs and their rational use5. Expand MDR-TB and XDR-TB surveillance 6. Introduce infection control, especially in high HIV
prevalence settings7. Mobilize urgently resources domestically and
internationally8. Promote research and development into new diagnostics,
drugs and vaccines
70
Global Policy: MDR-TB and XDR-TB
1. Strengthen basic TB control, to prevent M/XDR-TB2. Scale-up programmatic management and care of MDR-TB
and XDR-TB
3. Strengthen laboratory services for adequate and timely diagnosis of MDR-TB and XDR-TB
4. Ensure availability of quality drugs and their rational use5. Expand MDR-TB and XDR-TB surveillance 6. Introduce infection control, especially in high HIV
prevalence settings7. Mobilize urgently resources domestically and
internationally8. Promote research and development into new diagnostics,
drugs and vaccines
71
Global Policy: MDR-TB and XDR-TB
1. Strengthen basic TB control, to prevent M/XDR-TB2. Scale-up programmatic management and care of MDR-TB
and XDR-TB 3. Strengthen laboratory services for adequate and timely
diagnosis of MDR-TB and XDR-TB
4. Ensure availability of quality drugs and their rational use
5. Expand MDR-TB and XDR-TB surveillance 6. Introduce infection control, especially in high HIV
prevalence settings7. Mobilize urgently resources domestically and
internationally8. Promote research and development into new diagnostics,
drugs and vaccines
72
Global Policy: MDR-TB and XDR-TB
1. Strengthen basic TB control, to prevent M/XDR-TB2. Scale-up programmatic management and care of MDR-TB
and XDR-TB 3. Strengthen laboratory services for adequate and timely
diagnosis of MDR-TB and XDR-TB4. Ensure availability of quality drugs and their rational use5. Expand MDR-TB and XDR-TB surveillance
6. Introduce infection control, especially in high HIV prevalence settings
7. Mobilize urgently resources domestically and internationally
8. Promote research and development into new diagnostics, drugs and vaccines
73
Global Policy: MDR-TB and XDR-TB
1. Strengthen basic TB control, to prevent M/XDR-TB2. Scale-up programmatic management and care of MDR-TB
and XDR-TB 3. Strengthen laboratory services for adequate and timely
diagnosis of MDR-TB and XDR-TB4. Ensure availability of quality drugs and their rational use5. Expand MDR-TB and XDR-TB surveillance 6. Introduce infection control, especially in high HIV
prevalence settings7. Mobilize urgently resources domestically and
internationally
8. Promote research and development into new diagnostics, drugs and vaccines
The STOP TB Strategy – 2010
1. Pursue high-quality DOTS expansion and enhancementa. Secure political commitment, with adequate and sustained financing b. Ensure early case detection, and diagnosis through quality-assured bacteriologyc. Provide standardised treatment with supervision, and patient supportd. Ensure effective drug supply and management e. Monitor and evaluate performance and impact
2. Address TB-HIV, MDR-TB, and the needs of poor and vulnerable populationsa. Scale–up collaborative TB/HIV activitiesb. Scale-up prevention and management of multidrug-resistant TB (MDR-TB)c. Address the needs of TB contacts, and poor and vulnerable populations
3. Contribute to health system strengthening based on primary health care a. Help improve health policies, human resources development, financing, supplies, service delivery and informationb. Strengthen infection control in health services, other congregate settings and householdsc. Upgrade laboratory networks, and implement the Practical Approach to Lung Health (PAL) d. Adapt approaches from other fields and sectors, and foster action on the social determinants of health
4. Engage all care providersa. Involve all public, voluntary, corporate and private providers through Public-Private Mix (PPM) approachesb. Promote use of the International Standards for Tuberculosis Care (ISTC)
5. Empower people with TB, and communities through partnershipa. Pursue advocacy, communication and social mobilizationb. Foster community participation in TB care, prevention and health promotionc. Promote use of the Patients' Charter for Tuberculosis Care
6. Enable and promote researcha. Conduct programme-based operational research, and introduce new tools into practiceb. Advocate for and participate in research to develop new diagnostics, drugs and vaccines
The STOP TB Strategy – 2010
1. Pursue high-quality DOTS expansion and enhancementa. Secure political commitment, with adequate and sustained financing b. Ensure early case detection, and diagnosis through quality-assured bacteriologyc. Provide standardised treatment with supervision, and patient supportd. Ensure effective drug supply and management e. Monitor and evaluate performance and impact
2. Address TB-HIV, MDR-TB, and the needs of poor and vulnerable populationsa. Scale–up collaborative TB/HIV activitiesb. Scale-up prevention and management of multidrug-resistant TB (MDR-TB)c. Address the needs of TB contacts, and poor and vulnerable populations
3. Contribute to health system strengthening based on primary health care a. Help improve health policies, human resources development, financing, supplies, service delivery and informationb. Strengthen infection control in health services, other congregate settings and householdsc. Upgrade laboratory networks, and implement the Practical Approach to Lung Health (PAL) d. Adapt approaches from other fields and sectors, and foster action on the social determinants of health
4. Engage all care providersa. Involve all public, voluntary, corporate and private providers through Public-Private Mix (PPM) approachesb. Promote use of the International Standards for Tuberculosis Care (ISTC)
5. Empower people with TB, and communities through partnershipa. Pursue advocacy, communication and social mobilizationb. Foster community participation in TB care, prevention and health promotionc. Promote use of the Patients' Charter for Tuberculosis Care
6. Enable and promote researcha. Conduct programme-based operational research, and introduce new tools into practiceb. Advocate for and participate in research to develop new diagnostics, drugs and vaccines
Conclusions
• M/XDR-TB is ubiquitous• In some settings its prevalence is high enough to compromise TB control in absence of prompt action• Recent advances in new diagnostics needs to be complemented by parallel development of new drugs and vaccines• Chest physicians have a key role in ensuring prevention of development of further MDR-TB by ensuring early diagnosis and effective treatment of newly diagnosed, pan-susceptible, TB cases


















