Future directions for CKD anaemia Iain C Macdougall BSc, MD, FRCP Consultant Nephrologist and...
41
Future directions for CKD anaemia Iain C Macdougall BSc, MD, FRCP Consultant Nephrologist and Honorary Senior Lecturer Renal Unit, King’s College Hospital, London, UK
-
Upload
madelyn-ellett -
Category
Documents
-
view
221 -
download
7
Transcript of Future directions for CKD anaemia Iain C Macdougall BSc, MD, FRCP Consultant Nephrologist and...

Future directions for CKD anaemia
Iain C Macdougall BSc, MD, FRCP
Consultant Nephrologist and Honorary Senior Lecturer
Renal Unit, King’s College Hospital, London, UK

Honoraria, lecture fees, grants from:-
Disclosure
Amgen
Ortho Biotech
Roche
Affymax
Shire


Lancet, 9th September 2006

Overview of erythropoiesis in CKD in 2007
Cellular and molecular mechanisms relevant to anaemia
Future therapies for stimulating erythropoiesis
Future developments in the management of CKD anaemia
Outline of presentation

Overview of erythropoiesis in CKD in 2007
Cellular and molecular mechanisms relevant to anaemia
Future therapies for stimulating erythropoiesis
Future developments in the management of CKD anaemia
Outline of presentation


Papayannopoulou T, et al. In: Hoffman R, et al., ed. Hematology: Basic Principles and Practice. 4th ed. 2005;267-288.
SCF, GM-CSF, IL-3
SCF, IL-1, IL-3, IL-6, IL-11
PluripotentStem Cell
Burst-Forming Unit-Erythroid Cells (BFU-E)
Colony-FormingUnit-ErythroidCells (CFU-E)
Reticulocytes RBCsErythro-blasts
Proerythro-blasts
About 8 Days
Iron
Erythropoietin
Erythropoiesis in CKD

Pro-inflammatory cytokines (IL-1, TNFα, IL-6, IFNγ)
EPO production
EPO
+ +
Iron
Fas Ag
Apoptosis
─
hepcidin Fe absorption Fe transport Fe availability(EPO-R, Tf, TfR, Ferriportin, DMT-1)
─
Erythropoiesis in CKD

Overview of erythropoiesis in CKD in 2007
Cellular and molecular mechanisms relevant to anaemia
Future therapies for stimulating erythropoiesis
Future developments in the management of CKD anaemia
Outline of presentation

rHuEPO stimulates erythropoiesis by activating EPO receptors
membrane
Activation
EPO Receptor
rHuEPO
Signal Transduction
Growth and Differentiation

Activation of EPO receptors results in initiation of intracellular signalling pathways
Conformational change
Phosphorylation of JAK2,
a tyrosine kinase
Phosphorylation of EPO receptor
Initiation of intracellularsignalling pathways
membrane
Jak2Jak2
P
Jak2Jak2Jak2 Jak2
P P
P P
rHuEPO
Jak2Jak2P P
P PP

EPO receptor activation leads to activation of genes that promote erythropoiesis
membrane
nucleus
Jak2Jak2P
Survival, differentiation, proliferation, and maturation of RBC progenitors and precursors
Gene Activation
P
P
P
ST
AT
5
P

Survival, differentiation, proliferation, and maturation of RBC progenitors and precursors
ST
AT
5
Gene Activation
P
PI-3-Kinase
Jak2Jak2P
SCH
MAPK
SOS
GRB
P
P
P
membrane
nucleus
EPO receptor activation leads to activation of genes that promote erythropoiesis

Jak2Jak2P P
P P
EPO,rHuEPO
EPO dimer EPO mimetic peptide
Darbepoetinalfa
membrane
C.E.R.A.Peg-rHuEPO
Signal Transduction
Survival, differentiation, proliferation, and maturation of RBC progenitors and precursors
Gene Activation
Jak2Jak2P P
P P
Jak2Jak2P P
P P
Jak2Jak2P P
P P
Jak2Jak2P P
P P
Investigational
All ESAs have the same signalling pathway

Termination of EPO-receptor signalling
JAK 2JAK 2
S S
P P
P
P
EPO
P
Haemopoietic cell phosphatase
Internalisation and degradation

All ESAs have the same mechanism of action
Activation of the EPO receptor is the common mechanism by which all ESAs stimulate erythropoiesis
However, ESAs may differ from one another in:– Biophysical characteristics (e.g. molecular weight)– EPO receptor binding affinity– Pharmacokinetic properties (e.g. serum half-life,
clearance)

Weiss & Goodnough, NEJM, March 2005


Overview of erythropoiesis in CKD in 2007
Cellular and molecular mechanisms relevant to anaemia
Future therapies for stimulating erythropoiesis
Future developments in the management of CKD anaemia
Outline of presentation

Lancet 9th September 2006

I. EPO-receptor agonists
Protein-based ESA therapy
Epoetin (alfa, beta, delta, omega)
Biosimilar EPOs (epoetin zeta)
Darbepoetin alfa
C.E.R.A. (methoxy polyethylene glycol epoetin beta)
Synthetic erythropoiesis protein (SEP)
EPO fusion proteins
~ EPO–EPO
~ GM–CSF–EPO
~ Fc–EPO
~ CTNO 528
Small molecule ESAs
Peptide-based (e.g. Hematide)
Non-peptide based

II. Other mechanisms
Prolyl hydroxylase inhibitors (HIF stabilisers)
GATA inhibitors
Haemopoietic cell phosphatase (HCP) inhibitors
EPO gene therapy

I. EPO-receptor agonists
Protein-based ESA therapy
Epoetin (alfa, beta, delta, omega)
Biosimilar EPOs (epoetin alfa, epoetin zeta)
Darbepoetin alfa
C.E.R.A. (methoxy polyethylene glycol epoetin beta)
Synthetic erythropoiesis protein (SEP)
EPO fusion proteins
~ EPO–EPO
~ GM–CSF–EPO
~ Fc–EPO
~ CTNO 528
Small molecule ESAs
Peptide-based (e.g. Hematide)
Non-peptide based

II. Other mechanisms
Prolyl hydroxylase inhibitors (HIF stabilisers)
GATA inhibitors
Haemopoietic cell phosphatase (HCP) inhibitors
EPO gene therapy

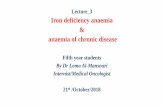
Multiple generic epoetin alfas are being marketed worldwide
– variable quality– variable biological activity– inaccurate labelling– ? immunogenicity
PERU
China

LaneLoad
(Units)
1 60
2 60
3 60
4 60
5 60
6 60
7 60
8 60
9 60
10 60
11 60
12 60
13 60
14 60
EPO F.P. STD
HEMAX / INDIA / HSA
EPO P.B. STD
EPO F.P. STD
WEPOX / INDIA / HSA FREE
Condition/TimePoint
NINGHONGXIN / CHINA / HSA
EMCURE / CHINA / HSA
ESPOGEN / KOREA / HSA
ZYROP / ARGENTINA / HSA
HEMAX / ARGENTINA / HSA
Candidate EPO Ph. Eur. BRP Batch 2 (BRP2)
EPO Ph. Eur. BRP Batch 1 (BRP 1)
EPO P.B. STD
ISOFORM 6
The “generic” epoetin alfas differ from approved epoetin alfas
Isoelectric Focusing*
The first biosimilar epoetin alfa was approved in Europe in June 2007 (Sandoz) – others pending

C.E.R.A.
Continuous Erythropoietin Receptor Activator Methoxy polyethylene glycol epoetin beta
long-acting ESA IV half-life = SC half-life = 130 hrs ?once–monthly dosing
C.E.R.A. EPO


EPO mimetic peptides
Family of peptides discovered with erythropoietin-mimetic activity Amino acid sequences completely unrelated to native EPO Same functional / biological properties as EPO First one described was EMP-1 A similar EMP pegylated and dimerised to produce HematideTM
HematideTM is about to begin Phase III of clinical development– stable at room temperature– antibodies do not cross-react with EPO, x1/month, ?cheaper

Injection 1 Injection 2 Injection 3 Injection 4 Injection 5 Injection 6
(Targ
et H
b R
an
ge: 1
1 – 1
3 g
/dL
)
-0.5
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
0 4 8 12 16 20 24Week
Me
an
Hb
Ch
an
ge
Fro
m B
as
eli
ne
(g
/dL
)
Starting Dose:
Hematide in pre-dialysis CKD patients (Phase 2)
0.025 mg/kg SC0.050 mg/kg SC0.075 mg/kg SC0.050 mg/kg IV
Macdougall et al., ASN, San Diego, Nov. 2006.

0
20
40
60
80
100
-3 -2 -1 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 Months
Pe
rce
nt
Pa
tie
nts
Re
ce
ivin
g R
BC
Tra
ns
fus
ion
s
Du
rin
g E
ac
h S
tud
y M
on
th
6
7
8
9
10
11
12
13
14
He
mo
glo
bin
co
nc
en
tratio
n (g
/dL
)
0
0 0 0 0 0 0 0 0 0 0 0
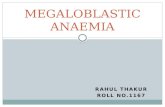
Hematide™ Injections
0
n= 9 9 9 10 10 10 9* 9 8 6** 5*** 5 5 5 5 5 5 5 4 3 2
*Subject 39-003, **Subject 39-004, and ***Subject 14-032 were censored due to kidney transplantation.
10 CKD patients with Ab+PRCA (Germany, France, UK) Treated with once-monthly SC Hematide 0.05mg/kg End-point – Hb > 11 g/dL without RBC transfusions

O2
OHproteasomaldegradation
OH
HRE
HIF-1
HIF-2
HIF
HIF-2 HIF-1
PHD
1
3
2
HIF target genes- EPO, etc.
HIF stabilizers (Prolyl hydroxylase inhibitors)
Macdougall & Eckardt, Lancet, 2006

HIF stabilizers
FDA has suspended further development of FG-2216 following the death of a female patient from fulminant hepatic necrosis
BUT
FG-2216 was in phase II of its clinical trial programme
Orally-active inhibitors of HIF prolyl hydroxylase have been synthesized (FG-2216; FG-4592 - FibroGen)
They cause an increase in EPO levels, even in CKD patients
Urquilla P et al.: J Am Soc Nephrol 2004; 15: 546A.
-1.5
-1.0
-0.5
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Day 0 Day 7 Day 14 Day 21 Day 28 Day 35 Day 42
Day
Ch
ang
e fr
om
Bas
elin
e -
Hem
og
lob
in (
gm
/dL
)
-1.5
-1.0
-0.5
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Day 0 Day 7 Day 14 Day 21 Day 28 Day 35 Day 42
Day
FG-2216 Patients Placebo Patients
Wiecek A. et al. XLII ERA-EDTA Congress, Istanbul 2005.
FG-2216 Patients Placebo Patients

Overview of erythropoiesis in CKD in 2007
Cellular and molecular mechanisms relevant to anaemia
Future therapies for stimulating erythropoiesis
Future developments in the management of CKD anaemia
Outline of presentation

New iron preparations – ferrumoxytol, Ferrinject, etc.
New trials
Further initiatives

Study design
Study pop. n
Follow-up
Goals End-points
RCT-db Type 2 DM
CKD 4000 4 years Hb 13
vs 9 CVS
RCT-sb > 70 yrs
CKD260 88 wks Hb 13
vs 9.5QoL
SF36 vit
EXTEND Observ. CKD pts 4000 q2wk vs q4wk DA
PREFERENCE Prospective
cohortCKD pts Several
hundred
Compare diff.mode of admin.
ESA mode of admin.
MIRCERA in Renal Tx
Open-label
Renal Tx Several hundred
1 year Hb QoL
New trials

TREAT1
CHOIR2
CREATE3
Besarab4
1000 2000 3000 4000
Number of patients
3896*
* IVRS 12 October 2007

TREAT vs. CHOIR
No. of centres
Median (pt-mths)
Total follow-up (pt-yrs)
Events (n)
CHOIR 130 14 1900 222

TREAT vs. CHOIR
No. of centres
Median (pt-mths)
Total follow-up (pt-yrs)
Events (n)
CHOIR 130 14 1900 222
TREAT 700 16 (already) 5182.9 (already)
> double that of CHOIR

Questions we don’t have answers to
Are high doses of EPO bad or is it just that “being hyporesponsive” is bad?
Is giving EPO to “hyporesponsive” patients bad?
Is a Hb of 11–12 g/dl appropriate for all CKD patients?
Does Hb variability/instability/cycling impact on mortality/morbidity, or is it just a marker of outcome?