
Fungal Infections: Management and Reporting - cibmtr.org€¦ · Fungal Infections: Management and...
22
Fungal Infections: Management and Management and Reporting Marcie Tomblyn, MD, MS Associate Member, Moffitt Cancer Center February 25, 2010 February 25, 2010
Transcript of Fungal Infections: Management and Reporting - cibmtr.org€¦ · Fungal Infections: Management and...

Fungal Infections: Management and Management and
Reporting
Marcie Tomblyn, MD, MSy , ,Associate Member, Moffitt Cancer Center
February 25, 2010February 25, 2010

ObjectivesObjectives
Review common fungal infections in HCT patientsReview current available therapiesDiscuss clinical examples with reporting issues
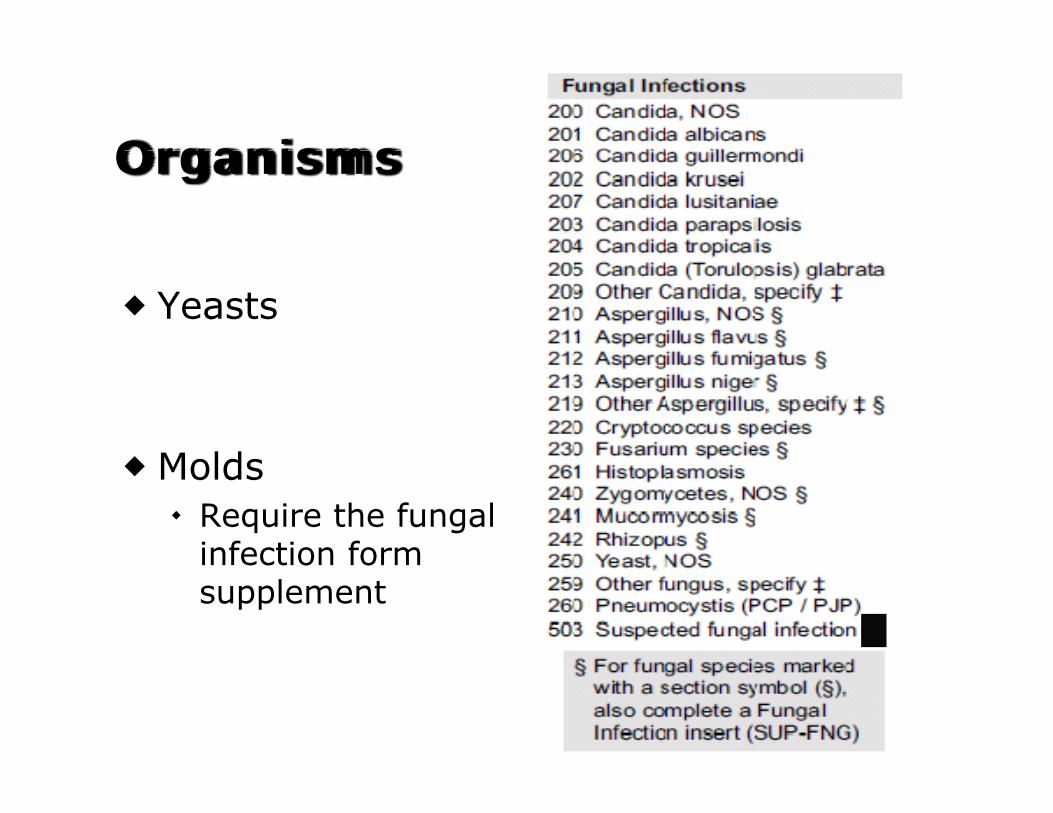
OrganismsOrganisms
Yeasts
M ldMoldsRequire the fungal infection form infection form supplement

MoldsMolds
Mucormycosis AspergillusMucormycosis Aspergillus

Definitions of Fungal InfectionDefinitions of Fungal Infection
ProvenOrganism seen on pathology with associated tissue damageOrganism identified by culture from a sterile procedure from a sterile area with associated clinical/radiologic findings of infection
ProbableRequires 1 host factor + 1 clinical factor + 1 microbiologic factor
PossibleRequires 1 host factor + 1 clinical factorNo microbiologic factor needed
EORTC/MSG Consensus

Host FactorsHost Factors
Recent neutropenia for >10 days Recent neutropenia for >10 days associated with the onset of fungal diseaseReceipt of allogeneic transplantSteroid use of >0.3mg/kg/day for >3 wksTreatment with T-cell immune suppressive meds in prior 90 days
i e Cyclosporine CAMPATH Fludarabinei.e. Cyclosporine, CAMPATH, FludarabineInherited severe immune deficiency
EORTC/MSG Consensus

Clinical FactorsClinical FactorsLower Resp Tract Sinonasal Infection
I i ith i iti CT findings of well-defined nodule, wedge shaped infiltrate, air-crescent or cavity OR
Imaging with sinusitis plus either acute localized pain, nasal ulcer or black eschar, or crescent, or cavity, OR
Nonspecific nodule(s) with pleural rub, pleural pain, or hemoptysis
,extension beyond bony borders
CNSp , p y
TracheobronchitisUlceration nodule
Focal CNS lesionsMeningeal enhancement
Disseminated Ulceration, nodule, pseudomembrane, eschar, or plaque seen on bronch
Disseminated candidiasis
Target lesions in liver and/or spleenand/or spleen
EORTC/MSG Consensus

Microbiologic FactorsMicrobiologic FactorsCytology, Direct Mi C lt
Detection of Antigen, ll ll l i Microscopy, or Culture
Sputum, BAL, or bronchial brush findings with fungal elements by
cell wall, or nucleic acids
Galactomannan: single iti i with fungal elements by
culture or direct observationSinus aspirate with
positive in serum, plasma, pleural fluid, BAL, or CSFBeta-D-glucan: single Sinus aspirate with
findings of fungal elements by culture or direct observation
Beta-D-glucan: single serum sample positivePCR for nucleic acids are NOT considered
Skin ulcerations require both culture and direct observation of fungal elementselements
EORTC/MSG Consensus

Prophylaxis vs TreatmentProphylaxis vs Treatment
Prophylaxis: started about the time of Prophylaxis: started about the time of conditioning to PREVENT infections
Example: Initiation of micafungin at the start f di i i f ll i lof conditioning for allogeneic transplant
Treatment: drugs used for Treatment: drugs used for MANAGEMENT of the infection
Example: Increase of dose of micafungin to p ghigher doses due to clinical findings—likely will add another antifungal as well

Infection Prophylaxis

Fungal Infection TreatmentFungal Infection Treatment
Will have the same drug choicesDoses may be increased to “treatment” dosesdoses
Example: Vori 200mg BID = prophylaxis Vori 200mg BID = prophylaxis Vori 300mg BID = treatment
May have additional antifungal therapiesMay have additional antifungal therapiesDouble therapyTriple therapyTriple therapy

Reporting of Fungal InfectionsReporting of Fungal Infections
Forms for reportingPre-transplant infections
Form 2000Form 2046 (supplement)
Post-transplant infectionsForm 2100F 2146 ( l t)Form 2146 (supplement)Form 2200

Reporting Infectionsp g

What is the same infection? (i e don’t report again)(i.e. don t report again)
Bacteria Virus Fungal
≤7 days• All bacteria (except Clostridium
≤14 days• VZV • HZV
≤14 days• Yeasts
Candida(except Clostridium Difficile)
≤30 days
• HZV• Adenovirus• Enterovirus
CandidaCryptococcus
≤30 days• Clostridium Difficile
• Influenza virus• Parainfluenza• Rhinovirus
≤90 days• Molds
Aspergillus
≤ 365 days•Helicobacter pylori
≤60 days• CMV • HSV
p gFusariumMucor
• HSV• Polyomavirus

Fungal Insert g(Forms 2046, 2146)
To obtain more specific information To obtain more specific information about mold infections
Requests detailed information of DiagnosisDiagnosisProphylaxisThTherapy

Mold Infections of Interest
AspergillusFusariumFusariumMucormycosisRhizopusRhizopusZygomycetes

Key Data ElementsKey Data Elements
Date of infectionSite of infectionDiagnostic testTreatment
F l d t th ti f Fungal drugs at the time of diagnosisTherapy up to 6 months after Therapy up to 6 months after diagnosis

Mold infection Mold infection

Sites of InfectionSites of Infection
**Di i t d i f ti t h th i id tifi d t 3 **Disseminated infections must have the organism identified at 3 or morenon-contiguous sites

Mold Diagnostic Test gOptions
BiopsyCultureCytologyKOH/Calcofluor stainAspergillus galactomannanUnknown

Therapy Data CollectionTherapy Data Collection
*If treatment held for less than 7 consecutive days and then restarted, do not consider as “Therapy Stopped”

Clinical ScenariosClinical Scenarios


















