FUNGAL INFECTIONS and ANTIFUNGAL AGENTS. AIMS & OBJECTIVES To provide an overview of the medically...
59
FUNGAL INFECTIONS and ANTIFUNGAL AGENTS
-
Upload
spencer-tucker -
Category
Documents
-
view
235 -
download
2
Transcript of FUNGAL INFECTIONS and ANTIFUNGAL AGENTS. AIMS & OBJECTIVES To provide an overview of the medically...

FUNGAL INFECTIONS and ANTIFUNGAL AGENTS

AIMS & OBJECTIVES
• To provide an overview of the medically important fungal infections
• List and classify Antifungal drug classes with their modes of action
• Make some key learning points through illustrated cases

The Fungal Kingdom
• Diverse groups of eukaryotic organisms that find nourishment from living or dead organic matter
• Their classification is based on their structural appearance
• During evolution relied on both sexual and asexual reproduction
• Both forms important for identification

FUNGI
• Saccharomyces cerevisiae is the model organism for studying yeast genetics
• Many seen as harmless environmental organisms
• Of the 50-250,000 fungal species less than 200 cause human disease and only a dozen or so on a regular basis

Fungi of medical importance:Classification
• Based on the colony morphology, vegetative hyphae that produce a mycelium and specialised aerial hyphae that bear spores (conidia)
• Yeasts: unicellular fungi reproduce by budding
• Moulds (filamentous): produce hyphae and mycelium
• Dimorphic: grow as moulds (environment) or yeasts (in human host)

YEAST:Blastospore; hyphae;
pseudohyphae
MOULD:Mycelium; hyphae
Some examples
• Yeast: Candida albicans, Cryptococcus neoformans
• Mould: Aspergillus, Penicillium, Fusarium, Dermatophytes
• Dimorphic: Histoplasma capsulatum

Types of diseases caused by human fungal pathogens
• Mycotoxicosis: due to ingestion of the toxic metabolites of mould fungi eg, poisonous toadstools

Mycotoxins
• Aspergillus flavus
• A ochraceus
• Fusarium moniliforme
• F graminearum
• Aflatoxin(hepatic ca)
• Ochratoxin (renal tox)
• Fumonisins (oesophageal ca)
• Deoxynivalenol (gastrointestinal toxicity)

Allergic lung disease
• Due to inhalation of fungal spores
• eg, A fumigatus, causing a type I or type III hypersensitivity reaction
• A clinical example is called allergic bronchopulmonary aspergillosis
• Farmers lung is another example
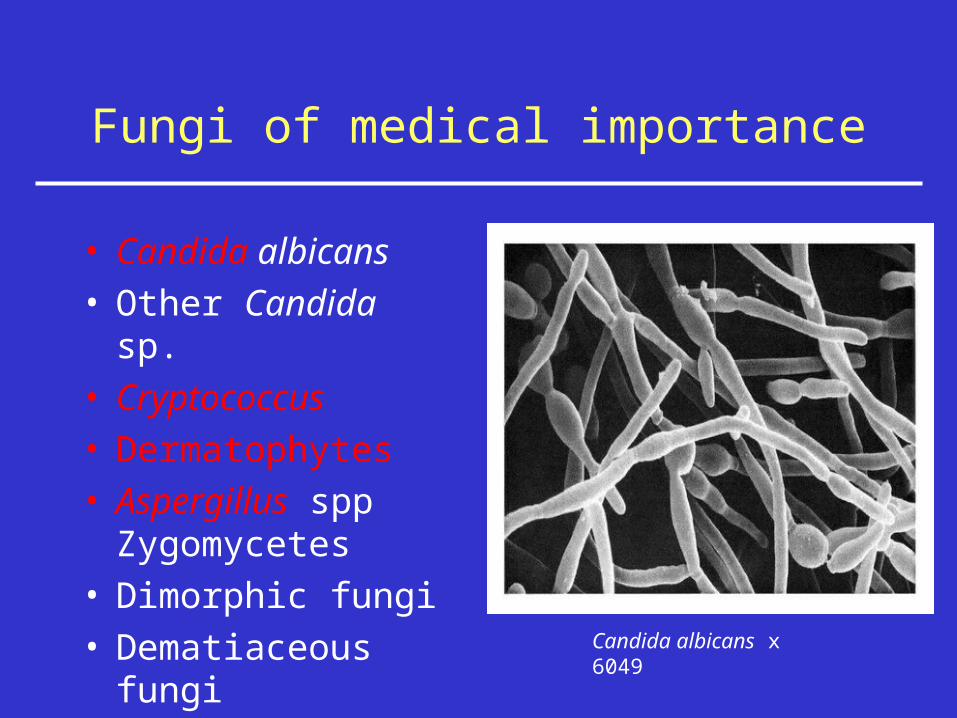
Fungi of medical importance
• Candida albicans• Other Candida sp.• Cryptococcus• Dermatophytes• Aspergillus spp
Zygomycetes• Dimorphic fungi• Dematiaceous fungi
Candida albicans x 6049

Classification of human fungal infections
• Superficial: ringworm (dermatophytes) , thrush (Candida species), dandruff (Pityrosporum)
• Subcutaneous: involve the dermis of the skin, deep tissues or bone. Usually found in tropics/sub-tropics where caught walking barefoot eg, mycetoma
• Systemic: due to pathogenic (Histoplasma) or opportunistic (Aspergillus) fungi

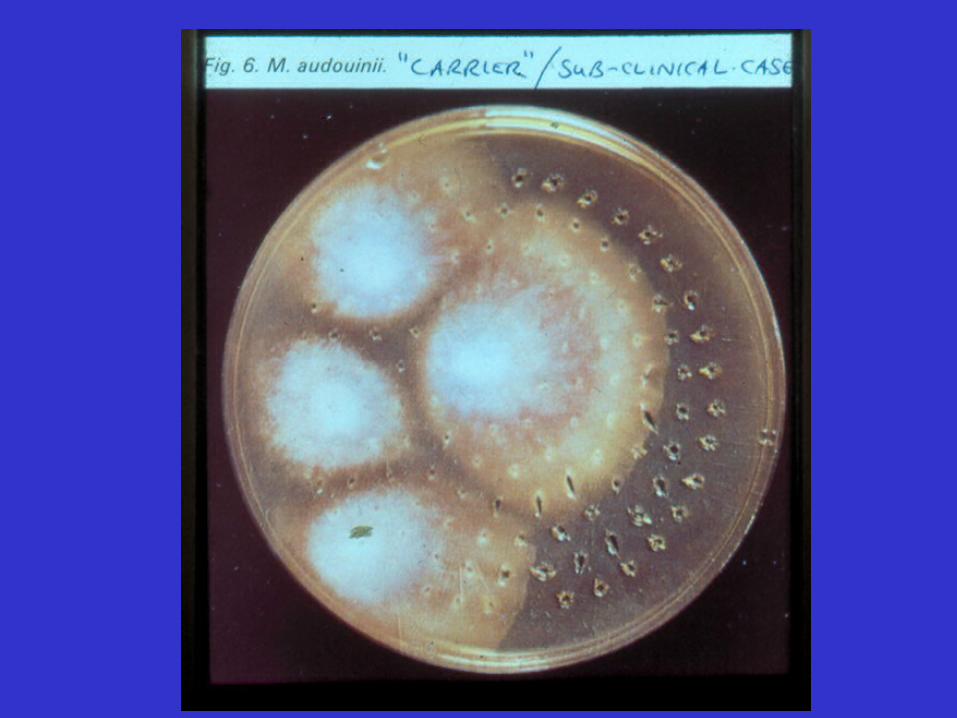
Dermatophytes (the cause of RINGWORM)
• Infection of scalp (Tinea capitis), trunk (Tinea corporis) or nails (Tinea unguium)
• Causative fungi are Trichophyton, Epidermophyton, Microsporum
• Geophilic, zoophylic, anthropophylic• Clinically red patches on skin, or scalp, scaly,
hair loss• Athletes foot an example

Some other skin fungal infections
• Seborrhoeic dermatitis (Pitysporum)
• Pityriasis versicolor (Pitysporum)
• Candidiasis (Candida albicans)



Vaginal Candidiasis (Thrush)
Common in women of child bearing years
Symptoms are itchy vaginal discharge
Diagnosed by vaginal examination (white plaques) and microscopy/culture
Treat: topical pessary
Or Fluconazole

SYSTEMIC (DEEP/INVASIVE) FUNGAL INFECTIONS:
MAJOR EXAMPLES
• Candidiasis • Aspergillosis• Cryptococcosis• Other mould infections• Endemic mycoses• Emerging fungal infections

ILLUSTRATION OF SOME CASES

CANDIDIASIS: CASE 1
• A 70-year old man has colonic surgery for carcinoma of colon
• Recovery is in the ITU
• He develops high fevers which don’t respond to antibiotics
• An organism is grown from blood cultures which is seen on gram stain

Candida blastospores (yeast)
In blood

Candidaemia

GERM TUBE
CANDIDIASIS:CASE 1………..• Candida albicans is identified• He is treated with a systemic antifungal
drug called amphotericin B intravenously• He develops rigors each time the drug is
given and after 7 days treatment although he is improving kidney failure develops and he requires haemofiltration
• Treatment is changed to fluconazole
SYSTEMIC (invasive) CANDIDIASIS
• Increasing in incidence
• Risk factors are prior colonisation of mucosal surfaces, antibiotics, major surgery, leukaemia, vascular catheters
• Main pathogenic species is Candida albicans (others are C tropicalis, C glabrata, C krusei)
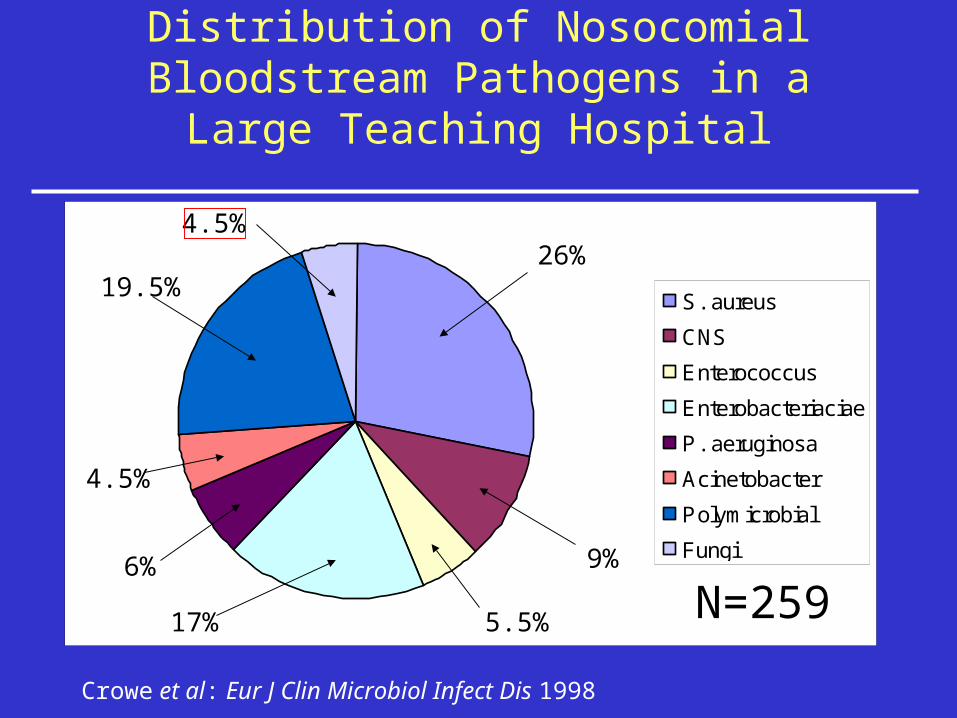
Distribution of Nosocomial Bloodstream Pathogens in a Large Teaching Hospital
Crowe et al: Eur J Clin Microbiol Infect Dis 1998
S. aureus
CNS
Enterococcus
Enterobacteriaciae
P. aeruginosa
Acinetobacter
Polymicrobial
Fungi
N=259
26%
9%
5.5%17%
6%
4.5%
19.5%
4.5%

Distribution of candidaemia by species(Hammersmith Hospital 1997-2000)
C. albicans
C. glabrata
C. parapsilosis
C. tropicalis
C. lusitaniae
other
mixed
44%
24%
14%
8%
6%2%
N=50

General patterns of susceptibility of Candida species
Pappas et al CID 2004; 38: 161-189
Candida species Fluco Itraco Vorico Flucy AmB Candins
C. albicans S S S S S S
C. tropicalis S S S S S S
C. parapsilosis S S S S S S (- I?)
C. glabrata SDD - R SDD - R S - I S S – I S
C. krusei R SDD - R S – I I - R S – I S
C. lusitaniae S S S S S - R S

Interpretive breakpoints for isolates of Candida species
Pappas et al CID 2004; 38: 161-189
MIC range (g/ml)
Drug SusceptibleIntermediately
susceptible Resistant
Fluconazole ≤8 16-32 (SDD) >32
Itraconazole ≤0.125 0.25-0.5 (SDD) > 0.5
Flucytosine ≤4 8.16 >16

Candida biofilms (on vascular catheter): a source of candidaemia
Courtesy of Dr J Douglas

Clinical manifestations of candidaemia/invasive candidiasis
• Infective endocarditis (heart valve surgery, IVDAs)
• Endophthalmitis
• Embolic skin lesions (petechial rash)
• Hepatic, renal, cerebral, meningeal infection

ANOTHER CASE……….
• Case no 2: a man who is HIV antibody positive
• He complains of difficulty with swallowing and retrosternal burning
• Endoscopy reveals white plaques on the oesophageal mucosa typical of Candida (thrush)
FINALLY: SOME LEARNING POINTS ABOUT CANDIDIASIS
• In immunocompromised relapses often occur unless underlying problem is removed
• Candida endocarditis often requires surgery• Fluconazole resistance has been reported in
AIDS cases because of the high fungal load• Disseminated candidiasis is difficult to
diagnose

Antifungal Drugs Currently licensed for systemic therapy
• POLYENES: examples: amphotericin B, nystatin:
Including 3 lipid formulations of amB (Ambisome)
• AZOLES:– Imidazoles: miconazole, ketoconazole– Triazoles: fluconazole, itraconazole, voriconazole
• FLUORINATED PYRIMIDINE: flucytosine• ALLYLAMINE: terbinafine• CANDINS: new antifungal class

CELL WALL SYNTHESISCaspofungin
AnidualfunginMicafungin
MEMBRANE FUNCTIONAmphotericin B
Nyststin
NUCLEIC ACID SYNTHESIS5-Flucytosine
ERGOSTEROL SYNTHESISAzoles:
Fluconazole, itraconazole, voriconazole
ALLYLAMINE:Terbinafine
Targets of action of antifungal drugs


AMPHOTERICIN B vs FLUCONAZOLE
• Polyene antifungal• Inhibits cell
membrane• Broad spectrum• Not absorbed• Causes rigors• Causes kidney
damage• Resistance rare
• Azole antifungal• Inhibits cytochrome
p450 ( ergosterol)• Broad spectrum• Orally absorbed• Few side effects• No kidney damage• Resistance occurs

Caspofungin
• New class• Fungicidal • Broad spectrum
– not Cryptococcus
• Few side effects• o.d. regimen• No cross resistance with azoles & polyenes

Phospholipid bilayerof the fungal cell
membrane
Fungalcell wall
-(1,3)-glucan
-(1,6)-glucan
-(1,3)-glucan synthase Ergosterol
Mechanism of Action
CANDINS

Antifungal drug resistance
• Rare in Candida albicans except in AIDS patients
• Some fungi are inherently resistant to antifungal: aspergillus and fluconazole
• Others acquire resistance following exposure eg, C albicans in oropharyngeal infection in an AIDS patient
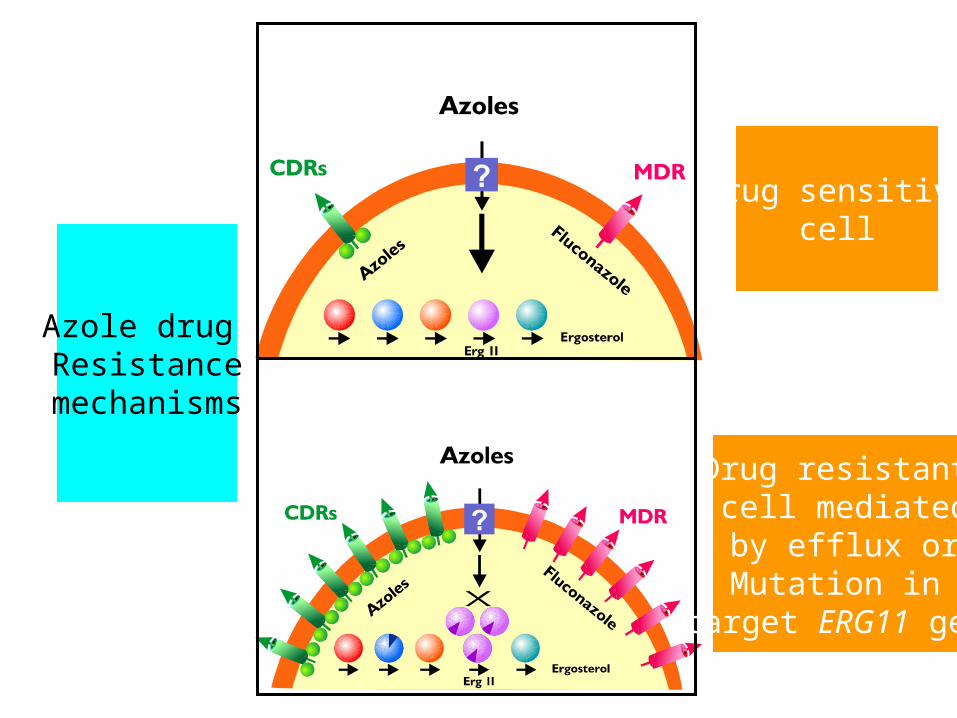
Azole drug Resistance
mechanisms
Drug sensitivecell
Drug resistant cell mediated by efflux orMutation in
target ERG11 gene

Acquired Resistance to Fluconazole in HIV-associated Oropharyngeal Candidiasis
Fluconazole quickly became established as the drug of choice
Effective doses have ranged between 50mg and 400mg
Since the late 1980’s there have been many reports of clinical failure

ASPERGILLOSIS
• Saprophytic (aspergilloma), allergic (ABPA) and invasive forms of this infection
• Environmental fungus Aspergillus is the pathogen
• Acquired by inhalation• Pulmonary disease is main feature• Difficult to diagnose & high mortality
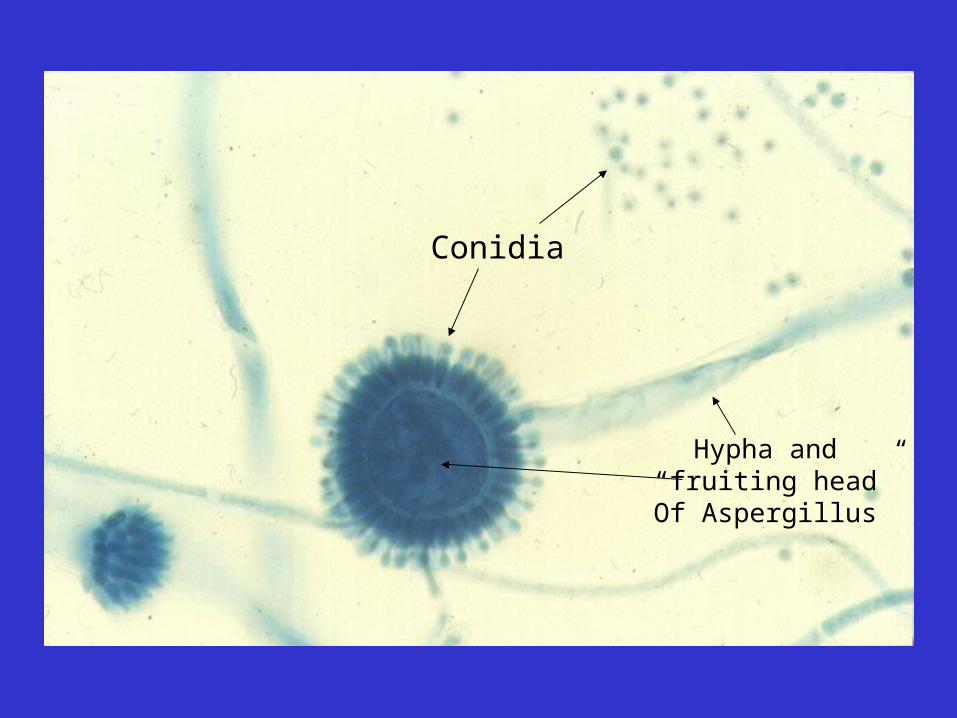
Hypha and “fruiting head”Of Aspergillus
Conidia

Airborne conidia
Alveolar macrophage
How Aspergillus infection is acquired


ASPERGILLOSIS: CASE STUDY
• A 23-year old man suffering from acute myeloid leukaemia undergoes a therapeutic bone marrow transplant
• There follows a long period of neutropenia
• He complains of pleuritic chest pain, breathlessness and has a fever
• Antibiotics make no difference

ASPERGILLOSIS CASE
CONT’D……...• Chest x ray is performed: infiltrates
• This is followed by a CT scan
• He also undergoes bronchoscopy which reveals some white plaques
• The patient dies despite amphotericin B therapy (there was no recovery of his bone marrow)

Risk groups for Invasive Aspergillosis
• Syndromes/treatments with severe neutropenia
• Haematological malignancy• Chronic immunosuppression• Solid organ transplantation• AIDS• Chronic granulomatous disease• Chronic lung diseases: sarcoidosis
Another mould infection: Zygomycosis
• Patients with Haematological malignancy at risk
• Diabetic patients also susceptible• Rhinocerebral infection a feature• Eye swelling and cellulitis also seen• Antifungal therapy not effective• Due to several related mould fungi eg,
Rhizopus

ANOTHER SYTEMIC FUNGAL
INFECTION: CRYPTOCOCCOSIS • A man who had a kidney transplant is
receiving immunosuppression with prednisone and azathioprine
• He develops headache over several days, followed be photophobia and neck stiffness
• Spinal fluid is obtained which reveals a high count of lymphocytes

CASE CONT’D………..
• A special stain called India ink reveals the presence of round cells surrounded by haloes as illustrated
• These haloes are the capsule of the yeast Cryptococcus neoformans
• A silver stain of a skin biopsy also shows many yeast cells

Cryptococcosis (India ink stain)

CRYPTOCOCCOSIS
• A major opportunistic infection in AIDS• Also occurs in chronically immunosuppressed
patients eg, organ transplant• Causes insidious meningitis with lymphocytes
in spinal fluid• Treatment is amphotericin B + flucytosine (as
in IDSA treatment guidelines)

ENDEMIC MYCOSES
• Histoplasmosis (H capsulatum, H duboisii)• Blastomycosis (B dermatitidis)• Coccidioidomycosis (C immitis)• Paracoccidioidomycosis

HISTOPLASMOSIS
• Has a specific geographical distribution• For example it is endemic in some mid west
states in USA• Evidence of endemicity is from skin testing of
healthy population• May cause a self-limiting flu-like illness in
immunocompetent• Severe pneumonia in immunocompromised

Emerging fungal pathogens
• Increasingly being seen in severely immunocompromised
• Susceptibility to antifungals unpredictable• Often these are environmental organisms• Fusarium is reported to be the 4th most
common opportunist fungus in some US centres
SUMMARY POINTS
• Superficial fungal infections are a not uncommon presenting complaint in primary care
• Invasive fungal infections are associated with compromised patients and are seen in hospital practice
• Limited antifungal therapies make them more difficult to treat than bacterial infection