Functional Weakness - Case Control Study€¦ · Web viewFor example in one study. ... The next...
36
ARTICLE for Neurologic Clinics - Case Studies Functional Disorders in Neurology: Case Studies Jon Stone 1 , Ingrid Hoeritzauer 1 , Jeannette Gelauff 2 , Alex Lehn 3,4 , Paula Gardiner 1 , Anne van Gils 5 , Alan Carson 1,6 1 Dept Clinical Neurosciences, University of Edinburgh, Western General Hospital, Crewe Rd, Edinburgh EH4 2XU. Tel 0131 537 1137 Fax 0131 537 1132 2 University Medical Center Groningen, Department of Neurology, University of Groningen, Netherlands 3 Department of Neurology, Princess Alexandra Hospital, Brisbane, Australia 4 School of Medicine, University of Queensland, Brisbane, Australia 5 University Medical Center Groningen, Department of Psychiatry, University of Groningen, Netherlands 6 Department of Psychological Medicine, Western General Hospital, Edinburgh, United Kingdom
Transcript of Functional Weakness - Case Control Study€¦ · Web viewFor example in one study. ... The next...

ARTICLE for Neurologic Clinics - Case Studies
Functional Disorders in Neurology: Case Studies
Jon Stone1 , Ingrid Hoeritzauer1, Jeannette Gelauff2, Alex Lehn3,4, Paula Gardiner1, Anne van Gils5, Alan Carson1,6
1Dept Clinical Neurosciences, University of Edinburgh, Western General Hospital, Crewe Rd, Edinburgh EH4 2XU. Tel 0131 537 1137 Fax 0131 537 1132
2University Medical Center Groningen, Department of Neurology, University of Groningen,
Netherlands3Department of Neurology, Princess Alexandra Hospital, Brisbane, Australia4School of Medicine, University of Queensland, Brisbane, Australia5University Medical Center Groningen, Department of Psychiatry, University of Groningen,
Netherlands6Department of Psychological Medicine, Western General Hospital, Edinburgh, United Kingdom
Correspondence to: Dr Jon Stone, Dept Clinical Neurosciences, University of Edinburgh, Western General Hospital, Edinburgh EH4 2XU. Email: [email protected] Tel 0131 537 1137
Keywords: Functional; Psychogenic; Conversion Disorder; Non-epileptic seizures; Movement
Disorder; Dizziness; Physiotherapy; Psychotherapy
Abstract
Functional, often called psychogenic, disorders are common in neurological practice. We
illustrate clinical issues and highlight some recent research findings using six case studies of
functional neurological disorders. We discuss dizziness as a functional disorder, describing the
relatively new consensus term Persistent Posturo-Perceptual Dizziness (PPPD), axial
jerking/myoclonus as a functional movement disorder, functional speech symptoms, post-
concussion disorder with functional cognitive symptoms and finally advances in treatment of
dissociative seizures and functional motor disorders.
Key Points
Functional Disorders in Neurology should be diagnosed on the basis of positive clinical
features, not the absence of disease or normal investigations
Functional dizziness has now been conceptualised around the term Persistent Postural
Perceptual Dizziness and can be recognised on the basis of typical features in the
history.
Axial jerking, sometimes labelled propriospinal myoclonus, is a functional movement
disorder in most patients.
Dissociative (non-epileptic) seizures are commonly preceded by prodromal autonomic
and fear symptoms which are a good target for evidence based treatment.
Functional Movement Disorders may respond well to physiotherapy designed to reverse
states of abnormally focused attention and abnormal movement habits.

Introduction
Functional disorders, which within neurological practice can also be described as psychogenic,
non-organic or conversion disorders are one of the commonest reasons for referral to a clinical
neurologist. Their frequency, around 1 in 6 to 1 in 3 new neurology patients in ambulatory care,
is not matched by their representations in textbooks and training for neurologists. In the last 15
years, research in the field has slowly emerged which allows a neurologist to approach the
diagnosis and management of their patients with functional disorders in a structured and logical
way. The unique format of Neurologic Clinics Case Studies gives an opportunity to discuss some
of the many challenges but also rewarding treatment opportunities that can be found in
working constructively with patients who have functional symptoms and disorders.
This selection of case studies of functional disorders was written to complement those already
found in a previous edition of Neurologic Clinics: Case Studies published in 20061. Although the
field has seen many advances since that time2,3, the fundamental principles of diagnosis and
treatment for functional limb weakness, dissociative (non-epileptic) seizures and movement
disorders remain the same.
We have therefore taken the opportunity in this new article highlight advances with respect to
the field in different symptoms of functional disorders (such as dizziness, impaired cognition
and myoclonus) and treatment. For a more comprehensive review of the field the reader is
directed elsewhere2,34.
We use the term functional disorder throughout this article not because we insist others do the
same, there are valid arguments for other terms5,6, but because we find it more useful
mechanistic term to use with our patients, which does not presuppose aetiology and fits best
with a biopsychosocial approach to these often complex presentations.

Case 1. Jerky body movements after an unpleasant anaesthetic
A man in his mid 50s presents with frequent episodes of axial jerking which started after an
inguinal hernia repair but which was characterised by unusually long recovery time after
anaesthetic with some symptoms of dissociation. His jerks occur as frequently during sitting as
when he is supine. Recently he has started having vocalisations during his jerks. Examination
shows arrhythmic flexor axial jerking. He has associated bilateral jerking of his arms and legs and
facial spasm. His partner notices that social situations or talking about his symptoms worsens
them. When you begin to talk about his vocalisations he develops a brief grunt each time he jerks.
On further questioning the patient describes a feeling of "fizzing" in his legs which builds up and is
released when he jerks. He can postpone the jerks for a few seconds but is left with a very
unpleasant feeling. Despite the frequency of jerks when seated he has never had one when riding
his motorbike. His partner says they are not present during sleep. A normal MRI of his whole
spine has already been carried out when he attends your clinic. . The patient is distressed by his
symptoms and fearful of leaving the house or having visitors.
What Is the Diagnosis and How Are You Going to Confirm It?
The history and examination is in keeping with what has traditionally been termed idiopathic
propriospinal myoclonus. Propriospinal myoclonus describes arrhythmical flexor jerking of the
trunk, hips and knees which increases when supine. Propriospinal myoclonus (PSM) can be
secondary to a structural spinal lesion, , or be idiopathic. Until recently idiopathic PSM was
thought usually to be an organic movement disorder. However, a large combined retrospective
case series from London and the Netherlands (n=176, n=76) suggests that around two thirds of
idiopathic PSM is a functional movement disorder based on multiple clinical features and
especially the demonstration of a Bereitschaftspotential (BP) in many cases. (Table 1)7–9.
Functional propriospinal myoclonus, also called psychogenic axial myoclonus, occurs as
frequently in males as it does in females. Onset is later than other functional movement
disorders, occurring usually in the 40s. A common trigger is a surgical or medical illness, often
with physiological triggers for myoclonus such as sepsis or hypoxia combined with a health
anxiety inducing situation.
TABLE 1 here
Some of the usual criteria for a functional movement disorders such as acute onset and rapid
progression are unhelpful in differentiating PSM secondary due to a spinal cause from
functional PSM. From the history the main differentiating characteristics are variability over
time, and presence of alleviating or exacerbating factors8,9. Multifocal onset of jerks,

predominant lower limb involvement or unilateral limb involvement and prolonged muscle
contraction following jerks suggest a diagnosis of functional PSM8,9. Signs of a disorder outside
of the spinal cord such as co-existing facial involvement, vocalisations or evidence of other
functional movement disorders reinforce a likely functional aetiology. Most patients with
secondary PSM will have evidence of a myelopathy on careful history and clinical examination.
Investigation
An MRI of whole spine is usually required to exclude a spinal lesion. The diagnosis of functional
PSM should ideally be made with the assistance of electrophysiological testing. Polymyography
in 'structural' PSM will show slow conduction velocity (>15m/s), EMG burst duration of
<1000ms, a constant pattern of muscle activation without involvement of facial muscles10. An
EEG-EMG multichannel recording with jerk-locked back-averaging will often show a
Bereitschaftspotential (BP), a pre-movement potential seen in voluntary movement. The
absence of a BP does not exclude functional propriospinal myoclonus as BP can be affected by
the level of attention, motivation and task complexity as well as technical difficulties during
testing. Clinical suspicion of functional PSM is best verified by an incongruent EMG pattern for
PSM (as described above) and/or a BP.
Treatment
Treatment for functional propriospinal myoclonus is uncertain. Medication such clonazepam or
botulinum toxin can be tried but in many cases a symptomatic response may be related to
placebo. For example in one study. 17 patients achieved complete resolution of their symptoms
after a one off botulinum toxin injection (n=17/39)8
Case 2. Persistent and disabling dizziness in a young woman
A 19 year old woman presents with a history of persistent dizziness for the previous two years. She
had an initial illness consistent with a viral labyrinthitis with intense rotatory vertigo and nausea
rendering her bedbound for a week. She was found to have rotatory nystagmus at the time but this
settled. As she recovered her complaint of dizziness changed to a more non-specific feeling of
disequilibrium, light headedness with swaying and a feeling of motion present mainly on standing
and walking but also noticeable when lying in bed at night. Intermittently she felt 'spaced out' as if
she was floating and people seemed far away which she found frightening. She also complained of
sensitivity to objects moving in her environment when she was still, difficulty using a computer or
being in busy environments such as shops with a fear of falling. Symptoms of fatigue, poor
concentration and anxiety about going outside were prominent and she had stopped working as a
consequence. She had occasional migraine. Detailed vestibular testing and neuroimaging, whilst
very uncomfortable for the patient, were all normal.
What is the diagnosis?
This is a typical history for a patient with dizziness presenting as part of a functional disorder.
Commonly used terminology for this symptom cluster is chronic subjective dizziness, phobic
postural vertigo, visual vertigo, space and motion discomfort and most recently persistent
postural-perceptual dizziness (PPPD or 'Triple PD') .
Neurologists and Otologists working in balance clinics have long been aware that a significant
proportion of patients referred with dizziness do not have one of the common vestibular
disorders (eg vestibular migraine, benign paroxysmal positional vertigo (BPPV), canal
dehiscence syndromes). For example in a study of 547 patients from the balance clinic in
Munich, 19% had a 'non-organic' final diagnosis11.
In the 1980s Thomas Brandt and Marianne Dieterich proposed the concept of 'Phobic Postural
Vertigo'12, subsequently revised by Jeff Staab who proposed the term 'Chronic Subjective
Dizziness'13 to describe a symptom complex of dizziness that importantly they recognised
wasn't a diagnosis of exclusion and was clinically recognisable in their patient group. PPPD is
the latest term agreed to bring together these diagnostic entities and to encourage more
positive diagnosis. This is now described in the beta draft of ICD-11 (World Health
Organisation) as:
"Persistent non-vertiginous dizziness, unsteadiness, or both lasting three months or more.
Symptoms are present most days, often increasing throughout the day, but may wax and
wane. Momentary flares may occur spontaneously or with sudden movement. Affected
individuals feel worst when upright, exposed to moving or complex visual stimuli, and during
active or passive head motion. These situations may not be equally provocative. Typically,
the disorder follows occurrences of acute or episodic vestibular or balance-related problems.
"
The dizziness seen in PPPD / Functional Dizziness is not really vertigo. Although the patient as
in this case, may complain of swaying they typically also describe the feeling as lightheadedness
or heaviness of the head. Dissociative symptoms of derealisation and depersonalisation may
also occur as in this case. Clinically, a useful clue is improvement during more complex balance
tasks such as cycling or after alcohol. Fear of falling, worsening or 'attacks' of dizziness in
crowded places or places with a lot of sensory stimulation (movement, visual or auditory) can
lead to a picture similar or overlapping with panic with agoraphobia.. Onset after an identifiable
vestibular trigger such as migraine, labyrnthitis, BPPV or minor head injury is typical whereas
the rates of life events and stress before onset is not substantially different between 'functional'
and 'organic' groups14. Obsessional personality traits or psychiatric disorder may or may not be
present. Anxiety disorders, especially phobic disorders, occur in up to half of patients with
'organic' vestibular disorders11. They are therefore not diagnostic in themselves although tend
to worsen disability and distress associated with them.
Investigations
Vestibular studies and neuroimaging (MRI brain) should be normal in PPPD although co-
existence with other neurological, vestibular or psychiatric disorders may occur.
Posturographic studies may demonstrate improved performance during distraction. Clinically,
asking a patient to guess numbers written on their back or play a mobile phone game while
standing can be helpful when there is visible sway15.
Treatment
This new conception of functional dizziness or PPPD allows the clinical neurologist to make a
positive diagnosis in the same way that they would for functional movement disorder or
dissociative non-epileptic attacks, on the basis of the characteristic nature of the symptoms
themselves and not the presence or absence of psychopathology. This in itself is a major step
forward for patients, their families and for anyone attempting therapy.
PPPD can be explained to patients as a problem with the "software" of the nervous system
which has arisen usually as a result of an earlier vestibular problem or dizzy experience.
Normally feelings of dizziness and imbalance settle after such episodes but in PPPD the
"sensitivity settings" have become reset at an abnormal way such that the patient experiences
sensation of movement and imbalance that are normally "filtered out" by the brain. The longer
it goes on the more firmly this "sensitivity" gets stuck at these abnormal levels. If the person
takes steps to avoid activities situations which provoke dizziness this only serves to make them
more sensitive when they are exposed.
This kind of discussion can lead in to discussion about superimposed anxiety and panic when
present, as well as dissociation, a frightening symptom which patients often relieved to discover
is a common experience and not a sign of 'going crazy'16.
It is not hard to see the role here for physiotherapy to help expose and desensitise patients to
feared or avoided stimuli using exercise17 and also for cognitive behavioural therapy to help
overcome unhelpful thoughts and fears18. There may also be a role for medication such as an
SSRI in some patients13.
Case 3. New onset stuttering in an adult.
A 43 year old man presents with new onset stuttering for three weeks. He had previously been well,
but earlier in the month has been clipped by a car while riding his bike. He was wearing a helmet ,
there was no loss of consciousness or post traumatic amnesia On the way to hospital he recovered
quickly (but was left with a severe headache) with no focal neurological deficit including normal
speech. CT head scan was normal and he was kept overnight for observation because he felt
unwell. The next morning nursing staff initially noticed some word finding difficulties, which
rapidly deteriorated to a severe stutter. Apart from the speech disorder no other neurological
deficit was found on re-examination and an MRI scan of the patient’s head was entirely normal.
Over the last three weeks the stutter has been worsening, although the patient’s partner reports
significant variability in its severity.
What is the diagnosis?
The history is in keeping with a functional speech disorder (FSD) and there are several typical
features of functional stutter. Functional speech disorders commonly occur in the setting of
other functional disorders, particularly functional movement disorders19, but can also occur in
isolation. After functional dysphonia, stuttering is the second most common functional speech
abnormality, followed by articulation deficits and prosodic abnormalities (including foreign
accent syndrome). The combination of different abnormalities is also seen frequently20. The
diagnosis of functional speech disorder can be difficult as the clinical features of functional and
organic speech deficits are sometimes similar and they can occur together.

Several features in history and on examination can be helpful in diagnosis (also see table 2): the
development of significant speech deficits after a minor ictus such as mild traumatic brain
injury, especially with delayed onset, makes an organic cause unlikely21. Sudden onset and rapid
progression of a deficit in the absence of other associated deficits makes a functional disorder
more likely. The severity of functional speech symptoms typically varies across different
examination activities and some patients with FSD show significant distractibility and/or
suggestibility in their deficit (whereas organic speech disorders are usually consistent during
examination and don’t fluctuate). Also some patients with functional stutter show marked
effortful physical struggle of face, head as well as torso and limbs, which can be a helpful clue22.
Speech may be more effortful and problematic when there is discussion of the speech
symptoms. Stutter is a rare consequence of brain disease and in itself should be a red flag for a
functional disorder. Lastly the presence of reversibility is a strong marker towards FSDs. While
organic speech disorders can improve with speech therapy, the improvement is rarely dramatic.
With FSDs on the other hand some patients show rapid improvements even after just one or
two therapy sessions22.
TABLE 2 ABOUT HERE
Investigations and Workup
MRI brain scans are normal in patients with pure FSDs, but as mentioned above the co-
occurrence of organic and functional disturbances are not rare. An experienced speech therapist
will often be able to define the organic and functional components through clinical assessment.
Treatment
Treatment of FSDs follows the same principles applicable to other functional disorders. The
patient needs a clear positive diagnosis, preferably with transparency about the clinical features
of inconsistency that allow the diagnosis to be made and indication that it is being taken as
seriously as any other speech disorder. Speech therapy works on the principal of reducing
abnormally focused attention and re-learning normal movements/speech production20. In
practice this may mean: identifying abnormal speech characteristics, which are often due to
excessive and/or abnormal muscle activation patterns; asking the patient to imitate sounds that
will approximate a normal response (e.g. grunts, single syllables, simple words) and then
normalising the speech back to more natural speech sounds. Explain to the patient that these
abnormal speech features are a barrier to speaking normally (“You are working so hard to talk
that you are unable to speak naturally”). No randomised-controlled trial data is available, but
experience suggest that symptomatic speech therapy can be helpful in a large proportion of
cases20.
Case 4. Fatigue, headache and cognitive symptoms after a minor traumatic brain injury
A 22 year old student presented with fatigue, headache and cognitive symptoms. The symptoms
started three months earlier after he had been hit on the head by a ball while playing a game of
hockey. He had been unconscious for five minutes and describes feeling ‘as if he were in a bubble’
and having a severe headache afterwards. He was taken to the emergency department, where
physical examination and a CT scan were normal. In the weeks following the accident he
experienced extreme tiredness, general weakness, dizziness, and headaches. He spent most of his
time in bed, at home with his parents. He was unable to read or watch TV, because he had difficulty
concentrating. His parents noticed that at times he was struggling to find the rights words and
that he had become rather irritable. The patient was worried that the accident might have caused
permanent damage to his brain and he feared he would not be able to finish his studies.
What is the Diagnosis?
This diffuse collection of physical, emotional, behavioural, and cognitive symptoms in the
aftermath of a mild traumatic brain injury (mTBI), when it lasts longer than you would expect
from the nature of the injury, is often referred to as ‘post concussion syndrome’ (PCS). More
recent guidance23 has cautioned against this term as the available evidence does not support a
unique association with concussion and similar symptoms follow non- neurological trauma.
Typical symptoms after a mTBI include headache, dizziness, fatigue, irritability poor
concentration, hypersomnia, photosensitivity and hyperacusis. They routinely settle down
within weeks to 3 months24. However, in a minority of patients the reverse happens and the
symptoms progressively increase in intensity, the reverse pattern from more severe brain
injury where improvement occurs. In the UK this affects approximately 15% of patients25 but
the rates vary considerably internationally. There is disagreement on the aetiological
mechanisms underlying PCS. Some authors believe PCS results from diffuse axonal injury with
micro-trauma to axons, while most consider PCS to be the result of an interaction between
biological, psychological and social factors25. This might explain why similar symptoms are
described after other types of injuries as well24. Risk factors for developing PCS are: negative
illness perceptions (believing symptoms will last a long time and will have a negative impact on
your life), "all-or-nothing" behaviour, and litigation and/or compensation issues24–26
Treatment
The first step in the treatment is to explain to the patient what is wrong. The patient’s primary
concern is almost always, the not unreasonable, belief that these symptoms indicate brain
damage and that (s)he will not recover. We start treatment with a review of the injury severity,
checking that the Glasgow coma scale was 13 or above at time of admission to hospital, the
duration of total loss of consciousness was less than15 minutes and the duration of post
traumatic amnesia was less than 24 hours. When necessary we will supplement this with
reference to national clinical guidelines such as SIGN 13023 for additional reassurance. We will
then explain that although head injury commonly triggers such symptoms they are just as
common after severe injuries to legs or arms and their presence doesn’t indicate brain damage.
We will explain that recovery is the norm but the complicated course experienced is far from
unusual and can also fully recover. We review analgesic use with a view to stopping opiate
drugs and avoiding medication overuse headaches and if analgesia is required for headache or
photosensitivity using a tricyclic antidepressant. We use the principles of cognitive therapy, and
indeed sometimes formal CBT27, to structure a programme of graded exposure to tackle
avoidance and return to normal activity stressing the need to avoid ‘boom and bust’ cycles of
excessive activity and then collapse. We find a definite programme, albeit arbitrary- ie read for
15 minutes on day 1-3 then 30mins day 4-6- works better than vague advice. We challenge
fearful cognitions. A common example would be ‘my memory is not working, I have damaged
my brain’ which usually relates to anxiety interfering with normal retrieval mechanisms.
Memory symptoms can often be identified as functional in nature, for example using the fact
that they can recount the memory problem in some detail, that memory performance is highly
variable 28(see Table 3 for other features). We can also work on recognising how often memory
does actually work and have the patient challenging their anxious thoughts by talking these
ideas through to themselves when they arise. In more intractable cases, particularly when there
is considerable premorbid psychopathology, formal therapy can be required but for most cases,
such as the exemplar above, these principles can be utilised within the confines of a neurology
clinic appointment and we usually find resolution within a couple of months is the norm. We
have developed these principles in to a free-to-access patient self help website
www.headinjurysymptoms.org.
Table 3 about here
Case 5. Treatment of Dissociative (non-epileptic) attacks/ seizures
A 28 year old lady presents with a two year history of blackouts occurring up to 5 times a day but
sometimes with periods of two weeks with no episodes. The description given was of sudden
motionless unresponsiveness lasting 5-10 minutes during which her eyes are usually closed. The

patient initially said she had no warning symptoms when asked. However, when pressed she
admitted she did often get brief symptoms lasting 10-20 seconds of light-headedness and a
'horrible' feeling of ‘not really being there and floating’ which she was reluctant to describe. She
also described sweating and altered breathing pattern with a rising sense of fear. The patient
admitted that although she felt "wiped out" and upset after the seizure, she was relieved that the
unbearable feelings preceding it had gone. Many of the ‘seizures’ had happened outside which
cause embarrassment and a reluctance to go out.
What is the diagnosis?
The diagnosis is clearly that of a dissociative (non-epileptic) seizures (DS) or attack. In fact this
kind of episode, which represents around 20% of all DS presentations, looks like syncope not a
seizure. The term dissociative seizure or attack, as used in ICD-10, is therefore potentially more
inclusive. Recent studies of these patients indicates that they are more common than previously
thought and often present to cardiology services more than neurology29. Sudden motionless,
long duration episodes (more than 2 minutes) like this, especially with eyes closed are usually
diagnostic of DS. Further testing may be required to establish whether the patient also has
cardiac or autonomic comorbidities.
Increasing, evidence supports a hypothesis that in many patients, DS is a dissociative response
to a state of arousal similar to panic (1, 2). Several studies have highlighted how common
symptoms of panic and dissociation are in the prodromal state prior to a seizure303132. As in this
case, patients will typically be reluctant to admit they have warning symptoms33, partly because
they dont like to think about them in case it brings an attack on, and partly because they are
hard to describe and sound, in the case of dissociation, a bit 'crazy'. Not all patients do have
prodromal symptoms, sometimes because they have lost them, and sometimes because the
patient is amnestic for the prodromal stage which others may report as 'looking glazed' or 'they
were staring through me'. Patients may sometimes report mixed feelings of relief (that the
prodromal symptoms have gone) combined with anxiety and distress at the blackout itself34.
This helps clinicians to understand how the process becomes 'conditioned' and keeps repeating.
What can we learn from treatment
The patient was given a clear diagnosis backed up with written material (eg as found on
www.codestrial.org). They were referred to a cognitive behavioural therapist with expertise in
seeing patients with DS. Over a period of 12 sessions the events stopped completely. Additional
problems with past trauma arose and were approached with further therapy.
Increasing awareness of the arousal/dissociation mechanism, in many patients with DS has led
to advances in evidenced based treatment. This has developed from cognitive behavioural
therapy (CBT) approaches to panic disorder and other functional disorders. Two pilot RCTs of
CBT for dissociative seizures3536 produced promising data and a large multicentre trial is
ongoing37.
CBT involves formulating an understanding of seizure development and agreeing the reasons as
to why the seizures may be happening. This understanding is often enough to reduce or stop
seizures in some patients, probably through reducing fear. However most patients need help
overcoming learnt cognitions and avoidant behaviours that perpetuate their seizure.
Understanding mechanism is only part of the picture. A multifactorial aetiological model can be
used to understand that no single contributing factor has been identified sufficient to explain DS
in all patients but in each individual, different factors will be relevant (Figure 1).
Figure 1 here
In this patient, predisposing factors included post traumatic stress disorder after being raped at
gun point and only telling one close friend about it. There was also a history of bullying at school
and perfectionistric traits. Precipitating factors identified included relationship breakdown,
reports in media about rape and a friend being attacked.Perpetuating factors included
flashbacks and inducing feelings of anxiety and the need to avoid the thoughts or memories. She
had also been upset by feeling that health professionals didnt know what was wrong and had
avoidance of socialising, going outside and travelling alone because of seizures. All these
contributed to form a vicious cirle that could be addressed with treatment.
The first step of treatment was to help the patient understanding the diagnosis, its mechanism
and aetiology. Secondly, we worked to reduce seizure frequency by recognising the prodromal
sensations and use distraction technigues and exposure technigues to reduce anxiety over time
to prodromal symptoms. Technigues to deal with the anxiety sensations such as breathing
techniques, imagery and mindfulness allowed her to start going outside and face some of the
fears she has. In this patient dealing with the past trauma was also necessary and therefore
exposure to imagery of the rape and being able to talk about it was helpful. Therapy also used
thought and behaviour diaries to find alternate thought for her abnormal cognitions around self
esteem and gradually challenge avoidant behaviour. This patients seizures ceased with
treatment.

Case 6. Treatment of Fixed Dystonia
A 20-year-old woman with a history of chronic abdominal pain presented with pain and a fixed
posture of her left leg and foot. Symptoms had started after she sprained her left ankle on a
trampoline 3 years before. Persistent ankle pain and swelling in the presence of an inconclusive
ankle MRI was treated with a cast for several weeks. When the cast came off, the foot looked
different. It was swollen, more purple and felt colder to the touch than the other side. In the
following days to weeks, the ankle progressively inverted, to the point that the posture was mostly
fixed. She complained of weakness in the whole leg and the pain persisted. Many specialists were
consulted and she received diagnosis of Complex Regional Pain Syndrome (CRPS), muscle
dystrophy, dystonia and a functional disorder, depending on the specialty of the physician.
Neurological investigation showed a fixed inversion of the left ankle, with only small active
movements of the toes and passively some movement of the ankle. The patient said ‘my whole foot
feels as if it’s not there’.
What is the diagnosis
For a patient presents with fixed abnormal posture of a limb with pain and sensory
abnormalities, the diagnostic label depends partly on the preference and specialty of the
physician. Functional dystonia, often called fixed dystonia, is characterised by the onset in an
adult of an inverted ankle or clenched fist (Figure 2 and Video 1), although other types of
functional dystonia including at the shoulder are also recognised38. It may occur in the absence
of pain, but it is recognised that onset after injury and chronic pain are common and there is a
large overlap with Complex Regional Pain Syndrome (CRPS).
Figure 2 here
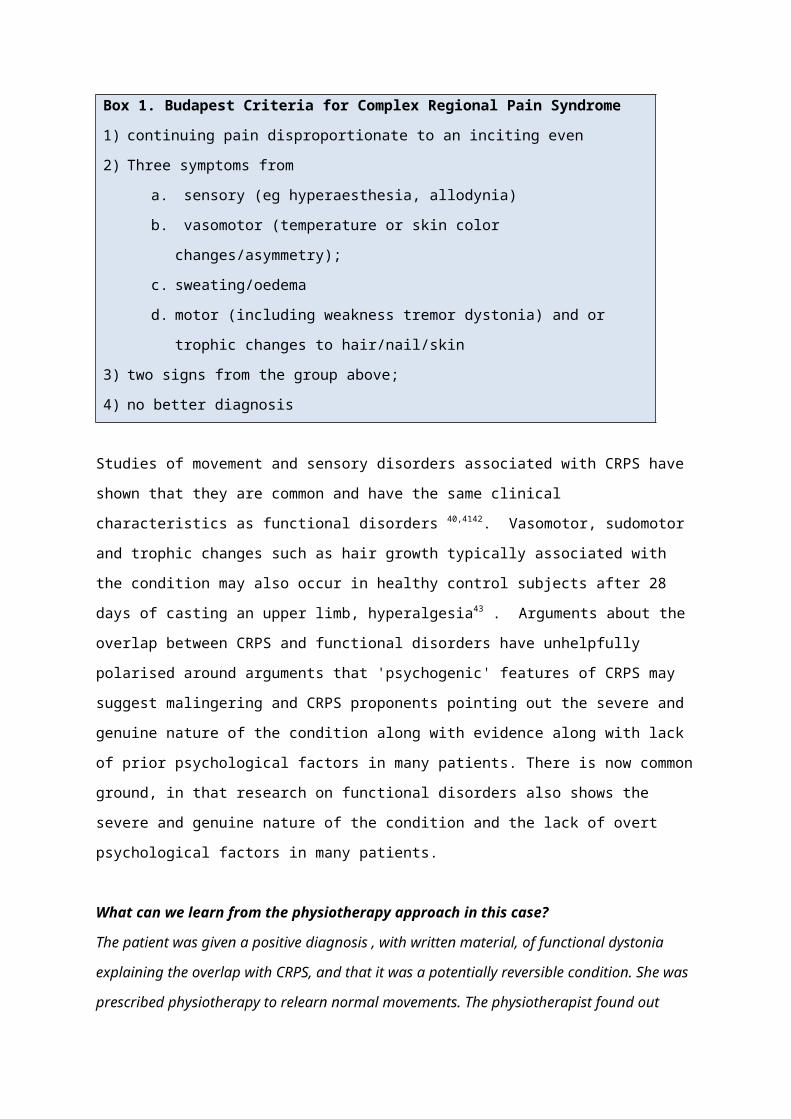
CRPS , is now most commonly diagnosed using the Budapest Criteria39 (Box 1):
Box 1. Budapest Criteria for Complex Regional Pain Syndrome
1) continuing pain disproportionate to an inciting even
2) Three symptoms from
a. sensory (eg hyperaesthesia, allodynia)
b. vasomotor (temperature or skin color changes/asymmetry);
c. sweating/oedema
d. motor (including weakness tremor dystonia) and or trophic changes to
hair/nail/skin
3) two signs from the group above;
4) no better diagnosis
Studies of movement and sensory disorders associated with CRPS have shown that they are
common and have the same clinical characteristics as functional disorders 40,4142. Vasomotor,
sudomotor and trophic changes such as hair growth typically associated with the condition may
also occur in healthy control subjects after 28 days of casting an upper limb, hyperalgesia43 .
Arguments about the overlap between CRPS and functional disorders have unhelpfully
polarised around arguments that 'psychogenic' features of CRPS may suggest malingering and
CRPS proponents pointing out the severe and genuine nature of the condition along with
evidence along with lack of prior psychological factors in many patients. There is now common
ground, in that research on functional disorders also shows the severe and genuine nature of
the condition and the lack of overt psychological factors in many patients.
What can we learn from the physiotherapy approach in this case?
The patient was given a positive diagnosis , with written material, of functional dystonia
explaining the overlap with CRPS, and that it was a potentially reversible condition. She was
prescribed physiotherapy to relearn normal movements. The physiotherapist found out normal
posture could be evoked by exercises the patient used to do at her gymnastics practice. This was
used to gain function and improve walking and posture.
Physiotherapy has been shown recently in a systematic review44 case series4546 and a
randomised controlled trial47 to be potentially highly effective in functional motor disorders.
Consensus recommendations exist which highlight that physiotherapy for these disorders
departs in many significant ways from that used in other neurological disorders48. For example
distraction techniques are used to enhance diagnostic confidence and regain 'automatic
movement', preferably collaboratively and creatively with the patient as in this case. This may
involve asking the patient to walk backwards or go on a treadmill even if they can barely walk.
Treatment is more about movement retraining and can be explained as a way of altering
abnormal movement 'habits' that have developed as a consequence of pain, injury or
dissociation.
Nielsen et al. studied 47 patients with a mean duration of symptoms of 5.5 years who completed
an intensive 5 day physiotherapy program45. A good outcome (defined as ‘‘very much improved’’
or ‘‘much improved’’ on the 7 point Clinical Global Impression scale) was seen in 64 % of
patients at the end of treatment, and in 55% of patients after a mean follow-up of 95 days. The
physiotherapy approach was based on a combination of education, retraining of normal
movement and self-management. Such treatment is also commonly advocated in CRPS49.
Arguably it is better to approach this clinical syndrome as fixed abnormal posturing that is most
commonly functional in origin40. Helping the patient to understand that the potential for
reversibility and the origin of the problem in the nervous system rather than the affected limb
appear to be key components of treatment that this approach fosters.
Table 1. Clinical clues to help differentiate Functional Axial Myoclonus from Secondary
and other 'organic' causes, taken from 7–9
Functional Axial Myoclonus Secondary /'Structural' /'organic'
Axial Myoclonus
Bereitschaftspotential present Bereitschaftspotential absent
Incongruous and variable
neurophysiology
Slow conduction velocity (5-15m/s),
EMG burst less than 1000ms, Constant
pattern of activation
Distractible and variable Structural cause seen on spinal MRI
Premonitory sensation Present during sleep
Facial involvement or vocalisation Other clinical evidence of spinal lesion
Prolonged muscle contraction with
jerks
Neck involvement
Temporary suppressibility Rhythmic
Jerks internally inconsistent
Immediate response to Botulinum
Toxin

Table 2: Clues to the presence of a functional speech disorder: adapted from Duffy 201320
History Development of severe speech deficit after uncomplicated mild
traumatic brain injury
Severe speech disorder in absence of other associated deficits
Other functional neurological symptoms may be present
Other features of functional speech disturbance e.g. baby speech,
telegraphic speech
Variability of deficit with significant fluctuations of speech disorder
Examination Speech characteristics do not fit known patterns of organic speech
disorders
Inconsistencies between speech and cranial nerve/oral mechanism
examination
Variability of deficit during examination (e.g. during conversation vs.
formal exam)
Susceptibility to suggestion and/or distraction
Paradoxical fatigability with deterioration of speech during examination
due to increased muscle activity (e.g. strained voice)
Rapid improvement in speech with symptomatic therapy
Table 3: Clues to the presence of functional cognitive symptoms either with or without
preceding minor head injury: adapted from Stone et al28
Functional Neurological Diseases
Young Older
Attends alone Attends with someone
Patient more aware of the problem than
others
Others more aware of the problem than
patient
Able to detail list of drugs, previous
interactions with doctors
Less able
Watches TV dramas Stops following drama
Marked variability Less variability
Types of memory symptom are usually
within most people's normal experience
Types of memory symptom are often
outwith normal experiences
‘I used to have a brilliant memory’ Does not highlight previous ‘brilliant
memory’
Figure 1: A range of potential factors involved in the mechanism and aetiology of Dissociative Seizures adapted from Reuber et al50
Figure 2. Fixed ankle inversion is a typical feature of functional dystonia

References
1 Stone J, Sharpe M. Functional symptoms in neurology: case studies. Neurol Clin
2006;24:385–403.
2 Carson AJ, Brown R, David AS, et al. Functional (conversion) neurological
symptoms: research since the millennium. J Neurol Neurosurg Psychiatry
2012;83:842–50.
3 Lehn A, Gelauff J, Hoeritzauer I, et al. Functional neurological disorders:
mechanisms and treatment. J Neurol 2015;:10.1007/s00415–015 – 7893–2.
4 Stone J, Carson A. Functional Neurologic Disorders. Continuum (N Y)
2015;21:818–37.
5 Edwards MJ, Stone J, Lang AE. From psychogenic movement disorder to
functional movement disorder: it’s time to change the name. Mov Disord
2014;29:849–52.
6 Fahn S, Olanow CW. ‘Psychogenic Movement Disorders’: They Are What They Are.
Mov Disord 2014;29:853–6.
7 van der Salm SMA, Koelman JHTM, Henneke S, et al. Axial jerks: a clinical
spectrum ranging from propriospinal to psychogenic myoclonus. J Neurol
2010;257:1349–55.
8 Erro R, Edwards MJ, Bhatia KP, et al. Psychogenic axial myoclonus: Clinical
features and long-term outcome. Parkinsonism Relat Disord 2014;20:596–9.
9 van der Salm SM a, Erro R, Cordivari C, et al. Propriospinal myoclonus: clinical
reappraisal and review of literature. Neurology 2014;83:1862–70.
10 Erro R, Bhatia KP, Edwards MJ, et al. Clinical diagnosis of propriospinal
myoclonus is unreliable: an electrophysiologic study. Mov Disord 2013;28:1868–
73.
11 Lahmann C, Henningsen P, Brandt T, et al. Psychiatric comorbidity and
psychosocial impairment among patients with vertigo and dizziness. J Neurol
Neurosurg Psychiatry 2015;86:302–8.
12 Brandt T, Dieterich M. Phobischer Attacken Schwankschwindel, ein neues
Syndrom? Munch Med Wschr 1986;28:247–50.
13 Staab JP. Chronic subjective dizziness. Continuum (Minneap Minn) 2012;18:1118–
41.
14 Radziej K, Schmid G, Dinkel A, et al. Psychological traumatisation and adverse life
events in patients with organic and functional vestibular symptoms. J Psychosom
Res 2015;79:123–9.
15 Wolfsegger T, Pischinger B, Topakian R. Objectification of psychogenic postural
instability by trunk sway analysis. J Neurol Sci 2013;334:14–7.
16 Tschan R, Wiltink J, Adler J, et al. Depersonalization experiences are strongly
associated with dizziness and vertigo symptoms leading to increased health care
consumption in the German general population. J Nerv Ment Dis 2013;201:629–
35.
17 Thompson KJ, Goetting JC, Staab JP, et al. Retrospective review and telephone
follow-up to evaluate a physical therapy protocol for treating persistent postural-
perceptual dizziness: A pilot study. J Vestib Res 2015;25:97–104.
18 Schmid G, Henningsen P, Dieterich M, et al. Psychotherapy in dizziness: a
systematic review. J Neurol Neurosurg Psychiatry 2011;82:601–6.
19 Baizabal-Carvallo JF, Jankovic J. Speech and voice disorders in patients with
psychogenic movement disorders. J Neurol 2015;:DOI: 10.1007/s00415–015 –
7856–7.
20 Duffy JR. Motor Speech Disorders: : Substrates, Differential Diagnosis, and
Management. 3rd ed. St Louis: : Elsevier Health Sciences 2013.
21 Binder LM, Spector J, Youngjohn JR. Psychogenic Stuttering and Other Acquired
Nonorganic Speech and Language Abnormalities. Arch Clin Neuropsychol
2012;27:557–68.
22 Duffy JR, Baumgartner J. Psychogenic stuttering in adults with and without
neurologic disease. J Med Speech Lang Pathol 1997;5:75–95.
23 Scottish Intercollegiate Guidelines Network (SIGN). Brain injury rehabilitation in
adults. Edinburgh: : SIGN 2013.
24 Carroll L, Cassidy JD, Peloso P, et al. Prognosis for mild traumatic brain injury:
results of the who collaborating centre task force on mild traumatic brain injury. J
Rehabil Med 2004;36:84–105.
25 Reuben A, Sampson P, Harris AR, et al. Postconcussion syndrome (PCS) in the
emergency department: predicting and pre-empting persistent symptoms
following a mild traumatic brain injury. Emerg Med J 2014;31:72–7.
26 Hou R, Moss-Morris R, Peveler R, et al. When a minor head injury results in
enduring symptoms: a prospective investigation of risk factors for
postconcussional syndrome after mild traumatic brain injury.
JNeurolNeurosurgPsychiatry 2012;83:217–23.
27 Al Sayegh A, Sandford D, Carson AJ. Psychological approaches to treatment of
postconcussion syndrome: a systematic review. J Neurol Neurosurg Psychiatry
2010;81:1128–34.
28 Stone J, Pal S, Blackburn D, et al. Functional (Psychogenic) Cognitive Disorders: A
Perspective from the Neurology Clinic. J Alzheimer’s Dis 2015;48:S5–17.
29 Blad H, Lamberts RJ, Gert van Dijk J, et al. Tilt-induced vasovagal syncope and
psychogenic pseudosyncope: Overlapping clinical entities. Neurology
2015;85:2006–10.
30 Hendrickson R, Popescu A, Dixit R, et al. Panic attack symptoms differentiate
patients with epilepsy from those with psychogenic nonepileptic spells (PNES).
Epilepsy Behav 2014;37:210–4.
31 Goldstein LH, Mellers JDC. Ictal symptoms of anxiety, avoidance behaviour, and
dissociation in patients with dissociative seizures. J Neurol Neurosurg Psychiatry
2006;77:616–21.
32 Reuber M, Jamnadas-Khoda J, Broadhurst M, et al. Psychogenic nonepileptic
seizure manifestations reported by patients and witnesses. Epilepsia
2011;52:2028–35.
33 Reuber M, Monzoni C, Sharrack B, et al. Using interactional and linguistic analysis
to distinguish between epileptic and psychogenic nonepileptic seizures: a
prospective, blinded multirater study. Epilepsy Behav 2009;16:139–44.
34 Stone J, Carson AJ. The unbearable lightheadedness of seizing: wilful submission
to dissociative (non-epileptic) seizures. J Neurol Neurosurg Psychiatry
2013;84:822–4.
35 Goldstein LH, Chalder T, Chigwedere C, et al. Cognitive-behavioral therapy for
psychogenic nonepileptic seizures: A pilot RCT. Neurology 2010;74:1986–94.
36 LaFrance WC, Baird GL, Barry JJ, et al. Multicenter pilot treatment trial for
psychogenic nonepileptic seizures: a randomized clinical trial. JAMA psychiatry
2014;71:997–1005.
37 Goldstein LH, Mellers JDC, Landau S, et al. COgnitive behavioural therapy vs
standardised medical care for adults with Dissociative non-Epileptic Seizures
(CODES): a multicentre randomised controlled trial protocol. BMC Neurol
2015;15:98.
38 Sa DS, Mailis-Gagnon A, Nicholson K, et al. Posttraumatic painful torticollis. Mov
Disord 2003;18:1482–91.
39 Harden RN, Bruehl S, Stanton-Hicks M, et al. Proposed new diagnostic criteria for
complex regional pain syndrome. Pain Med 2009;8:326–31.
40 Hawley JS, Weiner WJ. Psychogenic dystonia and peripheral trauma. Neurology
2011;77:496–502.
41 Schrag a, Trimble M, Quinn N, et al. The syndrome of fixed dystonia: an

evaluation of 103 patients. Brain A J Neurol 2004;127:2360–72.
42 Verdugo R, Ochoa J. Abnormal movements in complex regional pain syndrome:
assessment of their nature. Muscle Nerve 2000;:198–205.
43 Terkelsen AJ, Bach FW, Jensen TS. Experimental forearm immobilization in
humans induces cold and mechanical hyperalgesia. Anesthesiology
2008;109:297–307.
44 Nielsen G, Stone J, Edwards MJ. Physiotherapy for functional (psychogenic) motor
symptoms: A systematic review. J Psychosom Res 2013;75:93–102.
45 Nielsen G, Ricciardi L, Demartini B, et al. Outcomes of a 5-day physiotherapy
programme for functional (psychogenic) motor disorders. J Neurol
2015;262:674–81.
46 Czarnecki K, Thompson JM, Seime R, et al. Functional movement disorders:
Successful treatment with a physical therapy rehabilitation protocol. Park Relat
Disord 2012;18:247–51.
47 Jordbru AA, Smedstad LM, Klungsøyr O, et al. Psychogenic gait disorder: A
randomized controlled trial of physical rehabilitation with one-year follow-up. J
Rehabil Med 2014;46:181–7.
48 Nielsen G, Stone J, Matthews A, et al. Physiotherapy for functional motor
disorders: a consensus recommendation. J Neurol Neurosurg Psychiatry
2015;86:1113–9.
49 Harden RN, Oaklander AL, Burton AW, et al. Complex regional pain syndrome:
practical diagnostic and treatment guidelines, 4th edition. Pain Med
2013;14:180–229.
50 Reuber M. The etiology of psychogenic non-epileptic seizures: toward a
biopsychosocial model. NeurolClin 2009;27:909–24.