Functional Dyspepsia: Recent Advances In Pathophysiology
5
UPDATE ARTICLE Functional Dyspepsia: Recent Advances In Pathophysiology W H C Hu,* MBBS, MRCP, FHKAM(Med), FHKCP S K Lam, MD, FRCP, FHKCP Department of Medicine The University of Hong Kong Summary Functional (non-ulcer) dyspepsia is a common disease. With effective treatment now available for peptic ulcer; functional dyspepsia remains a major therapeutic challenge in gastrointestinal medicine. Despite advances in technology and diagnostic methods, the "true" underlying pathogenic abnormality in this disease remains elusive. It is likely that functional dyspepsia is a heterogeneous disorder with multiple aetiological factors. In this article various pathophysiological abnormalities in functional dyspepsia are discussed, and possible aetiological mechanisms proposed. (HK Pract 1998;20:327-334) Introduction The discovery of Helicobacter pylori and effective treatments for peptic ulcer disease has resulted in a focusing of research activity into functional dyspepsia, a common condition with limited therapeutic options. Functional (non-ulcer) dyspepsia is a term generally applied to patients who have chronic dyspepsia where oesophagogas- troduodenoscopy, considered the gold standard test, has excluded peptic ulceration, reflux oesophagitis and malignancy. 1,2 Patients with non- erosive gastritis and duodenitis, by convention, are not excluded. The currently accepted "Rome definition of dyspepsia", based on the consensus opinion of an international panel of clinical investigators, is persistent or recurrent pain or discomfort centered in the upper abdomen' (Table 1). Discomfort, in this context, may be characterised by symptoms such as early satiety, postprandial discomfort or fullness, bloating or nausea. On the other hand, symptoms referable to the oesophagus alone, such as heartburn or acid regurgitation, are no longer considered to constitute part of the definition; although patients with dyspepsia may concurrently have typical reflux-like symptoms. 12 * Address for correspondence: Dr Wayne Hu. Senior Medical Officer, Department of Medicine, Queen Mary Hospital, Pokfulam Road, Hong Kong. 327
Transcript of Functional Dyspepsia: Recent Advances In Pathophysiology
UPDATE ARTICLE
Functional Dyspepsia:Recent Advances In Pathophysiology
W H C Hu,* MBBS, MRCP, FHKAM(Med), FHKCP
S K Lam, MD, FRCP, FHKCPDepartment of Medicine
The University of Hong Kong
Summary
Functional (non-ulcer) dyspepsia is a common disease. With effective treatment now available for peptic ulcer;
functional dyspepsia remains a major therapeutic challenge in gastrointestinal medicine. Despite advances intechnology and diagnostic methods, the "true" underlying pathogenic abnormality in this disease remains elusive.
It is likely that functional dyspepsia is a heterogeneous disorder with multiple aetiological factors. In this articlevarious pathophysiological abnormalities in functional dyspepsia are discussed, and possible aetiological mechanisms
proposed. (HK Pract 1998;20:327-334)
Introduction
The discovery of Helicobacter
pylori and effective treatments for
peptic ulcer disease has resulted in a
focusing of research activity into
f u n c t i o n a l dyspepsia, a common
condition with l imited therapeutic
opt ions . Func t iona l (non-ulcer)
dyspepsia is a term generally applied
to p a t i e n t s who h a v e c h r o n i c
dyspepsia where oesophagogas-troduodenoscopy, considered the goldstandard test, has excluded pepticulceration, reflux oesophagitis andmalignancy.1 , 2 Patients with non-erosive gastritis and duodenitis, byconvention, are not excluded. Thecurrently accepted "Rome definitionof dyspepsia", based on the consensusopinion of an international panel ofclinical investigators, is persistent orrecurrent pain or discomfort centered
in the upper abdomen' (Table 1).Discomfort, in this context, may becharacterised by symptoms such asearly satiety, postprandial discomfortor fullness, bloating or nausea. On theother hand, symptoms referable to theoesophagus alone, such as heartburnor acid regurgitation, are no longerconsidered to constitute part of thedef in i t ion ; although patients withdyspepsia may concurrent ly havetypical reflux-like symptoms.12
* Address for correspondence: Dr Wayne Hu. Senior Medical Officer, Department of Medicine, Queen Mary Hospital, Pokfulam Road, Hong Kong.
327
Pathophysiology of Functional Dyspepsia
UPDATE ARTICLE
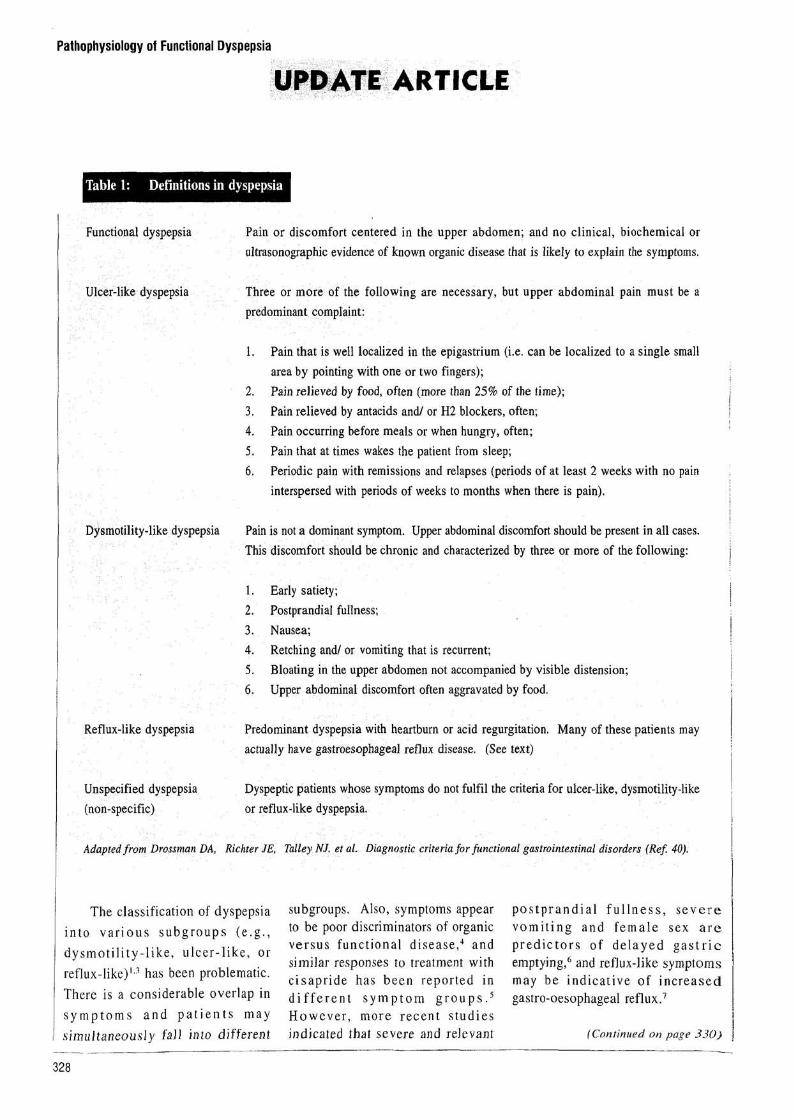
Table 1: Definitions in dyspepsia
Functional dyspepsia
Ulcer-like dyspepsia
Dysmotility-like dyspepsia
Reflux-like dyspepsia
Unspecified dyspepsia(non-specific)
Pain or discomfort centered in the upper abdomen; and no clinical, biochemical orultrasonographic evidence of known organic disease that is likely to explain the symptoms.
Three or more of the following are necessary, but upper abdominal pain must be apredominant complaint:
1. Pain that is well localized in the epigastrium (i.e. can be localized to a single smallarea by pointing with one or two fingers);
2. Pain relieved by food, often (more than 25% of the time);3. Pain relieved by antacids and/ or H2 blockers, often;4. Pain occurring before meals or when hungry, often;5. Pain that at times wakes the patient from sleep;6. Periodic pain with remissions and relapses (periods of at least 2 weeks with no pain
interspersed with periods of weeks to months when there is pain).
Pain is not a dominant symptom. Upper abdominal discomfort should be present in all cases.This discomfort should be chronic and characterized by three or more of the following:
1. Early satiety;2. Postprandial fullness;3. Nausea;4. Retching and/ or vomiting that is recurrent;5. Bloating in the upper abdomen not accompanied by visible distension;6. Upper abdominal discomfort often aggravated by food.
Predominant dyspepsia with heartburn or acid regurgitation. Many of these patients mayactually have gastroesophageal reflux disease. (See text)
Dyspeptic patients whose symptoms do not fulfil the criteria for ulcer-like, dysmotility-likeor reflux-like dyspepsia.
Adapted from Drossman DA, Richter JE, Talley NJ. et al. Diagnostic criteria for functional gastrointestinal disorders (Ref. 40).
The classification of dyspepsiai n t o v a r i o u s s u b g r o u p s ( e . g . ,d y s m o t i l i t y - l i k e , u l ce r - l ike , orreflux-like)1-3 has been problematic.There is a considerable overlap ins y m p t o m s a n d p a t i e n t s m a ysimultaneously fall into different
subgroups. Also, symptoms appearto be poor discriminators of organicversus f u n c t i o n a l disease,4 andsimilar responses to treatment withc i sapr ide has been reported ind i f f e r e n t s y m p t o m g r o u p s . 5
H o w e v e r , more recent s tud ie sindicated that severe and relevant
p o s t p r a n d i a l f u l l n e s s , severev o m i t i n g and f e m a l e sex a rep r e d i c t o r s of de layed g a s t r i cemptying,6 and reflux-like symptomsmay be ind ica t ive of increasedgastro-oesophageal reflux.7
(Continued on page 330)
328

Pathophysiology of Functional Dyspepsia
UPDATE ARTICLE
Pathophysiology of func-tional dyspepsia
Helicobacter pylori, gastritis andduodenitis
A p o p u l a t i o n based s tudyexamined H. pylori positivity indyspeptics with normal endoscopicf i n d i n g s and no rma l con t ro l s .A l though there was a trend fordyspeptics to have a higher infectionrate, the d i f f e r e n c e s were notstatistically significant.8 In a Dutchs tudy , the apparent associa t ionbetween H. pylori and dyspepsia wasdue to subjects with a past ulcerhistory.9 From another perspective,most studies have failed to demon-strate any significant difference inthe symptom pattern in patients withand without the infection.10, 11 Also,H. pylori infection does not affectgastric sensitivity,12 antro-duodenalmot i l i ty 1 3 or gastric emptying1 4 indyspeptic patients. Thus, althoughhistological gastritis (usually causedby H. pylori) is found in between30% to 70% of p a t i e n t s w i t hfunctional dyspepsia,15, 16 it is unlikelyto be a s i g n i f i c a n t c ause fordyspeptic symptoms.
Several studies have attemptedto study the effects of Helicobactereradication, but in many the designsare f l a w e d . 1 7 There are severalreports tha t H. pylori p o s i t i v edyspep t ics r ece iv ing succes s fu le r a d i c a t i o n t h e r a p y h a d l e s ss y m p t o m s t h a n n o n - e r a d i c a t e dcontrols after 6 to 12 months,al though short term response rateswere similar in both groups.18-20 Onthe other hand, another double-blind6-month s tudy us ing a v a l i d a t e d
symptom questionnaire showed nodifference in dyspeptic symptomsafter Helicobacter eradication.21 Atthe present state of knowledge, node f in i t e l i nk between H. pylorigastritis and functional dyspepsia canbe established.
Gastric acid
A recent s tudy us ing gastrinreleasing peptide as a secretogogueto s imula te meal-s t imulated acido u t p u t suggested tha t H. pyloriposi t ive dyspeptics have a higheracid o u t p u t t h a n a s y m p t o m a t i cinfected volunteers.22 However, moststudies have found normal basal andgastrin-stimulated peak acid outputin f u n c t i o n a l dyspep t i c s , whencompared to healthy controls.23
Various studies have attemptedto reproduce pain with intragastricacid p e r f u s i o n . A l t h o u g h somepat ients may experience a typica ldiscomfort, similar symptoms mayoccur af ter pe r fu s ion of normalsaline.2 4 Moreover, while patientswith functional dyspepsia are morel i k e l y to exper ience p a i n a f te rpentagastrin injection, blocking ofacid secretion did not reduce pain.25
Acid p r o b a b l y does not p l a y asignificant role in the pathogenesis offunc t iona l dyspepsia but may bemore re levant in the subgroup ofdyspeptic patients with ref lux- l ikesymptoms.7
Dysmotility
Delayed gastric emptying26 andant ra l h y p o m o t i l i t y 2 7 have beend e m o n s t r a t e d in up to 50% of
patients with functional dyspepsia.However, the correlation betweendyspeptic symptoms and the gastrice m p t y i n g rate is poor.2 8 Morerecently, abnormal distribution ofsolids in the stomach has beendemonst ra ted in pat ients 2 9 wi thincreased postprandial accumulationin the distal stomach. Also, a studyhas reported a lower number ofduodenal migrating motor complexeswith an increased proportion of timein phase II of the cycle dur ingsleep.30 However, in most patientsstudied, there was poor temporalcorrelation between episodes of painand abnormal motor activity.
Altered sensory function
Recent s tudies have focusedmore on abnorma l perception infunctional gastrointestinal disorders.Decreased perception thresholds toi n t r a l u m i n a l d i s t e n s i o n in the 'gastric fundus 3 1 - 3 3 and duodenum34
has b e e n d e m o n s t r a t e d in ap r o p o r t i o n of p a t i e n t s ; and adecreased gastric relaxatory responseto duodenal d i s t ens ion has alsobeen observed." It is possible thatabnormal fundal tone and gastricrelaxation may act synergisticallywith lowered visceral pain thresholdsto produce postprandial pain andbloating in patients.
Increased visceral sensi t ivi tyappears to be a generalised phenom-enon in the gastrointestinal tract.Dyspeptic patients also have loweredsensory thresholds in the oesophagusand rectum.35 Interestingly, despitethe widespread nature of visceralh y p e r s e n s i t i v i t y , somat ic p a i nt h r e s h o l d s are not a f f ec t ed in
330
Hong Kong Practitioner 20 (6) June 1998
UPDATE ARTICLE
ey messages
1. Functional dyspepsia is a common disease with heterogeneous pathophysiology.
2. Although firmly implicated in peptic ulcer disease, the role of Helicobacter pylori in functional dyspepsia is less
clear. Only some studies have shown a long-term benefit in dyspeptic symptoms after H. pylori eradication.
3. Gastric acid is probably not related to dyspeptic symptoms.
4. Dyspeptic patients may have disordered gastrointestinal motility and abnormal fundal tone.
5. Patients may have abnormal visceral hypersensitivity.
6. Increased anxiety and depression are present in dyspeptic patients attending medical clinics.
f u n c t i o n a l dyspepsia . The painthreshold to transcutaneous nervestimulation remains normal, despite alower pain th re sho ld to bal loondistension in the stomach.33
Psychosocial factors
Several studies have shown ah i g h e r l e v e l o f a n x i e t y a n ddepression in patients with functionaldyspeps i a , when compared tohealthy controls.36-38 However, theirlevel of anxiety may not be differentf rom p a t i e n t s w i t h n o n l i f e -t h r e a t e n i n g o r g a n i c b o w e ldiseases.36,39 Co-existing depressionand anxiety may act as a catalyst fora patient to seek medical care, ratherthan being the cause of symptoms.
Conclusions
Much advance has been made inthe unders tanding of func t iona ldyspepsia. It is probably hetero-
geneous in nature and the lack ofdiagnostic markers restrict precisestudy. It remains to be determinedwhether the various physiologicalabnormalities observed are markerso f t he c o n d i t i o n o r m e r e l yepiphenomena . Truly e f fec t ivemanagement strategies can only beformulated when the true underlyingaetiology has been made clear. •
References
1. Talley NJ, Colin-Jones D, Koch KL, et al.Functional dyspepsia: a classification withguidelines for diagnosis and management.Gastroenterology Intl 199l;4:145-160.
2. Talley NJ, Phillips SF. Non-ulcer dyspepsia:potential causes and pathophysiology. AnnIntern Med 1988;108(6):865-879.
3. Talley NJ, Zinsmeister AR, Schleck CD, etal. Dyspepsia and dyspepsia subgroups: apopulation-based study. Gastroenterology1992;102:1259-1268.
4. Talley NJ, Weaver AL, Tesmer DL, et al.Lack of d iscr iminant v a l u e of dyspepsiasubgroups in pa t ients referred for upperendoscopy. Gastroenterology 1993;105(5):1378-1386.
12.
Heading RC, Dyspepsia s tudy group. Uppergastrointestinal symptoms in general practice:a mu l t i c en t r e UK s tudy . J Drug Dev ClinPract 1995;7:109-117.Stanghe l l in i V, Tosetti C, Paternico A, et al.Risk indicators of delayed gastric emptyingo f s o l i d s i n p a t i e n t s w i t h f u n c t i o n a ldyspepsia. Gastroenterology 1996;110:1036-1042.Small PK, Loudon MA, Waldron B, et al.Importance of reflux symptoms in functionaldyspepsia. Cut 1995;36(2):189-192.Bernersen B, Johnsen R, Bostad L, et al. IsHelicobacter pylori the cause of dyspepsia?BMJ 1992;304(6837): 1276-1279.S c h l e m p e r R J , v a n d e r W e r f S D ,Vandenbroucke JP, et al. Nonulcer dyspepsiain a D u t c h w o r k i n g p o p u l a t i o n andHelicobacter pylori. Ulcer history as anexplanation of an apparent association. ArchIntern Med 1995;155(1):82-87.Holtmann G, Goebell H, Holtmann M, el al.Dyspepsia in healthy blood donors: pattern ofsymptoms and association with Helicobacterpylori. Dig Dis Sci 1994;39(5):1090-1098.Agreus L, Engstrand L, Svardsudd K, et al.Helicobacter pylori seroposit ivity amongSwedish adults with and without abdominals y m p t o m s . A p o p u l a t i o n - b a s e depidemiologic study. Scand J Gastroenterol1995;30(8):752-757.Mearin F, de Ribot X, Balboa A, et al. DoesHelicobacter pylori infection increase gastricsensitivity in functional dyspepsia? Gut 1995;37:47-51.
(Continued on page 334)
331

Pathophysiology of Functional Dyspepsia
UPDATE ARTICLE
13. Pieramico O. Di t schunc i t H. MalfertheinerP. Gastrointestinal moti l i ty in patients w i t hnon-u lcer dyspepsia: a role for Helicobacterpylori i n f ec t ion? Am J Gastroenterol 1993;88(3):364-368.
14. Minocha A. Mokshagundam S, Gal lo SH, eta l . A l t e r a t i o n s in upper g a s t r o i n t e s t i n a lm o t i l i t y in Helicobacter p y l o r i - p o s i t i v en o n u l c e r dyspepsia . Am J Gastroenterol1994:89(10): 1797-1800.
15. Loffeld RJ, Potters HV, Arends JW, et al.Campylobacter associated gastritis in patientsw i t h n o n - u l c e r d y s p e p s i a . J Clin Pathol1988:41(l) :85-88.
16. Greenberg RE, Bank S. The prevalence ofHelicobacter pylori in nonu lce r dyspepsia .Importance of s t ra t i f ica t ion according to age.Arch Intern Med 1990;150(l0):2053-3055.
17. Talley NJ. A c r i t i q u e of therapeutic t r i a l s inH e l i c o b a c t e r p y l o r i - p o s i t i v e f u n c t i o n a ldyspepsia . Gastroenterology 1994:106(5):1174-1183 .
18. McCarthy C, Patchett S, Col l ins RM, et al.Long-term prospective study of Helicnbacterpylori in n o n u l c e r dyspepsia . Dig Dis SciI995 ;40 (1 ) : I14 - I19 .
19. Lazzaroni M, Bargiggia S, Sangaletti O, etal. Eradication of Helicobacter pylori andlong-term outcome of f u n c t i o n a l dyspepsia.A c l i n i c a l cndoscopic s tudy. Dig Dis SciI996;4I (8) : I589-I594 .
20. Sheu BS, Lin CY, Lin XZ. et al. Long-termoutcome of t r i p l e therapy in Helicobacterpylori- r e l a t ed n o n u l c e r d y s p e p s i a : aprospect ive con t ro l l ed assessment. Am JGastroenterol !996;91(3):441-447.
21. Ve ldhuyzen van Zanten S, M a l a t j a l i a n D,Tanton R, et al. The effect of eradication ofHelicobacter pylori (Hp) on symptoms ofnon-ulcer dyspepsia (NUD): A randomizedd o u b l e - b l i n d p l acebo c o n t r o l l e d t r i a l .[Abstract ] Gastroenterology 1995;108:(4)A250.
22. El-Omar E, Penman I, Ardi l l JES, et al. Asubstantial proportion of non-ulcer dyspepsia
pat ien ts have the same abnormal i ty of acidsecre t ion as duodena l ulcer patients. Gut1995:36:534-538.
23. Collen MJ, Loebenberg MJ. Basal gastrie-acid secretion in nonulcer dyspepsia w i t h orw i t h o u t duodeni t i s . Dig Dis Sci 1989;34(2):246-250.
24. George AA, Tsuchiyose M, Dooley CP.S e n s i t i v i t y of the gastric mucosa to acid andduodenal contents in pa t ien t s with n o n u l c e rdyspepsia. Gastroenterology 1 9 9 1 : 1 0 1 ( 1 ):3-6.
25. Bates S, Sjoden PO, F e l l e n i u s J. et al.Blocked and nonblocked acid secret ion andreported p a i n in u l ce r , nonu lce r dyspeps ia ,a n d n o r m a l s u b j e c t s . G a s t r o e n t e r o l o g y1989;97(2):376-383.
26. Waldron B, Cu l l en PT. K u m a r R, et al.E v i d e n c e f o r h y p o m o t i l i t y i n n o n - u l c e rdyspepsia: a prospective mul t i fac tor ia l s tudy.Gut 1991;32(3):246-251.
27. Malagelada JR, S t a n g h e l l i n i V. Manometricevaluat ion of functional upper gut symptoms.Gastroenterology 1985:88:1223-1231.
28. Talley NJ. Shuter B, McCrudden G. et al.Lack of association between gastric empty ingo f s o l i d s a n d s y m p t o m s i n n o n u l c e rdyspepsia. J Clin Gastroenterol 1989; 11(6):625-630.
29. Troncon LE, Bennett RJ, A h l u w a l i a NK, etal. Abnormal intragastric distribution of foodd u r i n g g a s t r i c e m p t y i n g i n f u n c t i o n a ldyspepsia patients. Gut 1994;35(3):327-332.
30. David D, Mertz H. Fefer L, et al. Sleep andduodena l motor ac t iv i ty in pa t i en t s w i t hsevere non-ulcer dyspepsia. Gut I994;35(7):916-925.
31. Mearin F, Cucala M, Azpiroz F, et al. Theorigin of symptoms on the brain-gut axis inf u n c t i o n a l dyspeps i a . GastroenterologyI99I;101(4):999-1006.
32. Lemann M, Dederding JP, Flourie B, et al.
A b n o r m a l percept ion of visceral pa in inresponse to gastric d i s t ens ion in ch ron ic
idiopathic dyspepsia. The irr i table stomachsyndrome. Dig Dis Sci 1991 ;36(9): 1249-1254.
33. Coff in B. Azpiroz F. G u a r n c r F, et al.Se lec t ive gastric h y p e r s e n s i t i v i t y and reflexh y p o r e a c t i v i t y i n f u n c t i o n a l d y s p e p s i a .Gastroenterology 1994; 107(5): 1345-1351.
34. H o l t m a n n G, G o e b e l l H, T a l l e y NJ .Impai red smal l i n t e s t i na l peristalt ic reflexesand s e n s o r y t h r e s h o l d s a r e i n d e p e n d e n tf u n c t i o n a l d i s t u r b a n c e s i n p a t i e n t s w i t hc h r o n i c u n e x p l a i n e d d y s p e p s i a . Am JGastroentewl 1996;91 (3):485-491.
35. T r i m b l e KC, Farouk R, Pryde A, et al.Heigh tened visceral s ensa t ion in f u n c t i o n a lg a s t r o i n t e s t i n a l d isease is not site specif ic:ev idence for a genera l i zed d i sorder of guts e n s i t i v i t y . Dig Dis Sci 1995:40(8): 1607-1 6 1 3 .
36. Ta l ley NJ. Fung LH, G i l l i g a n IJ, et al .A s s o c i a t i o n o f a n x i e t y , n e u r o t i c i s m , anddepression with dyspepsia of unknown cause.A ca se -con t ro l s t u d y . Gastroenterology1986;90(4):886-892.
37. Tal ley NJ, P h i l l i p s SF. Bruce B, et al.Relation among personality and symptoms inn o n u l c e r dyspepsia and the i r r i table bowelsyndrome. Gas t roen t e ro logy 1990;99(2):327-333.
3 8 . T a l l e y N J , J o n e s M , P i p e r D W .P s y c h o s o c i a l a n d c h i l d h o o d f a c t o r s i nessent ia l dyspeps ia . A case-control s tudy.Scand J Gastroentewl 1988;23(3):341-346.
39. Langeluddecke P, Goulston K, Tennant C.P s y c h o l o g i c a l f ac to r s i n d y s p e p s i a o fu n k n o w n cause: a comparison wi th pepticulcer disease. J Psychosom Res 1990;34(2):215-222.
40. Drossman DA, Richter JE, Talley NJ, et al.D i a g n o s t i c c r i t e r i a f o r f u n c t i o n a lgas t ro in tes t ina l orders. In: The functionalgastrointestinal disorders. Bos ton /NewYork/Toronto/London: Little, Brown and Co,1994,p.331-337.
334