Full shoulder
80
-
Upload
el-nour-radiolgy-center-in-zagazig -
Category
Education
-
view
630 -
download
1
description
by dr. sameh khodair
Transcript of Full shoulder


Lecturer of radiodiagnosis

































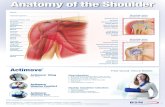
SHOULDER JOINT SHOULDER JOINT DISEASESDISEASES

1 - Rotator cuff disease 1 - Rotator cuff disease
2 – Instability and Labral lesions, 2 – Instability and Labral lesions,
3- Biceps disorders, 3- Biceps disorders,
4-Truma4-Truma
5-Tumors5-Tumors
6-Arthritis.6-Arthritis.
7-Refered pain as radiculopathy, and thoracic outlet syndrome. 7-Refered pain as radiculopathy, and thoracic outlet syndrome.

Tendinosis
The earliest stage of rotator cuff tendon pathology. The term tendinosis and not tendinitis is probably appropriate to describe such a cuff.
Rotator cuff diseaseRotator cuff disease
Partial-thickness tear
shows no communication between the glenohumeral joint and subacromial bursa.
Bursal side tearArticular side tearIntratendinous tear
Full-thickness tear
It is a discontinuity in the tendon that extends from the articular surface to the bursal surface.

Causes
1 – Impingement syndrome
Rotator cuff diseaseRotator cuff disease
2 – Degenerative
3 - Traumatic

shoulder instability is slipping of the humeral head out shoulder instability is slipping of the humeral head out of the glenoid socket during activities causing symptoms. It is of the glenoid socket during activities causing symptoms. It is referred to a spectrum of disorders that includes dislocation, referred to a spectrum of disorders that includes dislocation, subluxation and laxity.subluxation and laxity.
Shoulder instabilityShoulder instability
Instability is classified according to Instability is classified according to
temporal relationship of antecedent traumatemporal relationship of antecedent trauma (acute first-time (acute first-time versus recurrent)versus recurrent)
degreedegree (subluxation versus dislocation) (subluxation versus dislocation)
directiondirection, , either unidirectional (anteroinferior or posterior) or either unidirectional (anteroinferior or posterior) or multidirectional.multidirectional.

CausesCauses
1 – Laxity1 – Laxity
2 – Labral tear2 – Labral tear
SLAP lesionSLAP lesion
Bankart lesionBankart lesion
Shoulder instabilityShoulder instability

MR imagingMR imaging
Pulse sequences
MR images obtained included axial , oblique coronal and oblique sagittal planes with different pulse sequences as following:
Oblique Coronal T1 weighted images Oblique Coronal T2 weighted images Oblique Coronal T2 weighted fat suppressed images Oblique Coronal Proton Density (PD) weighted images Oblique Sagittal T1 weighted images Axial Gradient weighted images

Technique
Anterior approach for intra-articular injection was done by using a 22 G spinal needle.
Contrast agent
1- 0.5 mL of iodinated contrast agent was injected, guided under fluoroscopy for confirmation of intra-articular position of the needle.
Pulse sequences
T1 – weighted fat suppressed images was performed in axial , oblique coronal and oblique sagittal planes.
Direct MR arthrographyDirect MR arthrography
2- 10 – 12 mL of a diluted solution of a paramagnetic contrast material (( consisted of 1 mL. gadopentetate dimeglumine ( Magnevist ) diluted in 200 mL normal saline 0.9% )) was then injected.

Case 1 Supraspinatus tendinosisSupraspinatus tendinosis
AbAbnormal high signals equal less than normal high signals equal less than fluid signals with intact tendonfluid signals with intact tendon

Case 2 Supraspinatus partial tear ( Bursal side )

Case 2 Supraspinatus partial tear ( Bursal side )

Case 3 Supraspinatus partial tear ( Articular side )

Case 3 Supraspinatus partial tear ( Articular side )

Case 4 Supraspinatus partial tear ( Intratendinous )

Case 4 Supraspinatus partial tear ( Intratendinous )

Case 5 Supraspinatus full thickness tear

Case 5 Supraspinatus full thickness tear

Case 6 Supraspinatus full thickness tear

Case 6 Supraspinatus full thickness tear

Case 7 Supraspinatus full thickness tear

Case 7 Supraspinatus full thickness tear

ROLE OF MRI IN THE ROLE OF MRI IN THE DIAGNOSIS OF DIAGNOSIS OF
GLENOID LABRAL GLENOID LABRAL TEARSTEARS

GGlenoid labrum is a ring of dense lenoid labrum is a ring of dense fibrocartilagenousfibrocartilagenous tissue attached to the bony tissue attached to the bony glenoid cavity, increasing its depth and glenoid cavity, increasing its depth and considered to be a factor for shoulder considered to be a factor for shoulder stabilizationstabilization. .
Glenoid
Cavity

It appearse as a triangular structure at the It appearse as a triangular structure at the margin of the glenoid rim on both axial and margin of the glenoid rim on both axial and coronal planscoronal plans. . It displays low signal intensity on It displays low signal intensity on all pluse sequences.all pluse sequences.
CORONAL T1 WICORONAL T1 WI AXIAL T1 WIAXIAL T1 WI

Labral tears appear in MRI as a high signal Labral tears appear in MRI as a high signal intensity within the substance of the labrum intensity within the substance of the labrum detaching it from the glenoid rim. This is detaching it from the glenoid rim. This is obviously seen in acute stages where obviously seen in acute stages where associated joint effusion is present allowing associated joint effusion is present allowing fluid to inter the site of the tearfluid to inter the site of the tear

HHowever in chronic stages, fibrosis may owever in chronic stages, fibrosis may occur at the site of the tear also with occur at the site of the tear also with resolving of the joint effusion making the resolving of the joint effusion making the detection of the tear by conventional MRI is detection of the tear by conventional MRI is difficult and the labrum appears to be difficult and the labrum appears to be normalnormal..

SSo in this situation direct MR o in this situation direct MR arthrography is indicatedarthrography is indicated

Conventional MRIConventional MRIDirect MR arthrographyDirect MR arthrography
Intra-articular injection of about 10 – 12 mL of a diluted solution of a paramagnetic contrast material (( consisted of 1 mL. gadopentetate dimeglumine ( Magnevist ) diluted in 200 mL normal saline 0.9% )) by using a 22 G spinal needle.

Two mechanisms of truma are Two mechanisms of truma are encountered in the glenoid encountered in the glenoid
labral tearslabral tears

Fall on an outstretchedFall on an outstretched armarm

Superior labral tearSuperior labral tear
Superior labral anterior Superior labral anterior –– to to –– posterior tear posterior tear
SLAPSLAP

Four main types of SLAP LESIONSFour main types of SLAP LESIONS
Type IType I
Just fraying or irregularity of the Just fraying or irregularity of the labrum is demonstrated. This type labrum is demonstrated. This type of lesion is quite common in elderly of lesion is quite common in elderly persons and maypersons and may represent a represent a degenerative tear of the labrum. degenerative tear of the labrum. This type rarely causes symptoms This type rarely causes symptoms and do not require surgical repair.and do not require surgical repair.

SLAP lesion ( type II )SLAP lesion ( type II )
Type II SLAP lesions consist of detachment of the Type II SLAP lesions consist of detachment of the superiorsuperior labral-bicipital complex from the superior labral-bicipital complex from the superior
glenoid rimglenoid rim

SLAP lesion ( type III )SLAP lesion ( type III )
In type III SLAP lesions, the superior portionIn type III SLAP lesions, the superior portion of the of the labrum is detached from both the glenoid and the labrum is detached from both the glenoid and the bicepsbiceps tendon, and may be displaced into the joint tendon, and may be displaced into the joint
spacespace..

SLAP lesion ( type IV )SLAP lesion ( type IV )
Type IVType IV SLAP lesion is similar to type III lesion, with SLAP lesion is similar to type III lesion, with the tearthe tear extending into the biceps tendonextending into the biceps tendon ..

Directed more mediallyDirected more medially
At and anteriot to the biceptal labral At and anteriot to the biceptal labral complexcomplex
Smoothly outlinedSmoothly outlined
TThe biggest difficulty in diagnosing SLAP tears is he biggest difficulty in diagnosing SLAP tears is differentiation of type II tears from the normal differentiation of type II tears from the normal sublabral recess, which can be seen separating the sublabral recess, which can be seen separating the superior labrum from the glenoid as a normal superior labrum from the glenoid as a normal variantvariant

Usually directed laterally
Irregular outlinesExtend posterior to the biceptal labral
complex
SLAP IISLAP II

SHOULDER DISLOCATION

Anterior dislocationAnterior dislocation
BANKART LESIONBANKART LESION
HILL SACHS HILL SACHS FRACTUREFRACTURE

Posterior dislocationPosterior dislocation
REVERSE HILL SACHSREVERSE HILL SACHS

Bankart lesionBankart lesion

Bankart lesionBankart lesion
Hill Sachs fractureHill Sachs fracture

Perthes lesionPerthes lesion
A variant of Bankart lesionA variant of Bankart lesion

ALPSA lesionALPSA lesion
A variant of Bankart lesionA variant of Bankart lesion

MRI is an accurate modality in detection of MRI is an accurate modality in detection of glenoid labral tear specially in acute stagesglenoid labral tear specially in acute stages
Direct MR arthrography may be needed for Direct MR arthrography may be needed for detection of labral tear in chronic stages, detection of labral tear in chronic stages, however it converts the modality from non however it converts the modality from non invasive to an invasive methodinvasive to an invasive method..

Have A Nice Day