FSPHP Annual Meeting 2010 - Chicago, IL Resources for the Distressed Physician William Swiggart, MS,...
86
FSPHP Annual Meeting 2010 - Chicago, IL FSPHP Annual Meeting 2010 - Chicago, IL Resources for the Distressed Physician Resources for the Distressed Physician William Swiggart, MS, William Swiggart, MS, LPC/MHSP LPC/MHSP Associate in Medicine Associate in Medicine Co-Director Co-Director Vanderbilt Center for Vanderbilt Center for Professional Health Professional Health Betsy White Williams, Ph.D., M.P.H Betsy White Williams, Ph.D., M.P.H. Rush University Medical School Rush University Medical School Professional Renewal Center Professional Renewal Center eid Finlayson, MD eid Finlayson, MD ssistant Professor of Psychiatry ssistant Professor of Psychiatry irector irector anderbilt Comprehensive anderbilt Comprehensive ssessment Program ssessment Program Martha E. Brown, MD Martha E. Brown, MD Assoc. Dean Faculty Assoc. Dean Faculty Development Development Associate Professor of Associate Professor of Psychiatry Psychiatry USF College of Medicine USF College of Medicine
-
Upload
virgil-lloyd -
Category
Documents
-
view
222 -
download
0
Transcript of FSPHP Annual Meeting 2010 - Chicago, IL Resources for the Distressed Physician William Swiggart, MS,...

FSPHP Annual Meeting 2010 - Chicago, ILFSPHP Annual Meeting 2010 - Chicago, ILResources for the Distressed PhysicianResources for the Distressed Physician
William Swiggart, MS, LPC/MHSPWilliam Swiggart, MS, LPC/MHSPAssociate in MedicineAssociate in MedicineCo-DirectorCo-DirectorVanderbilt Center for Vanderbilt Center for Professional HealthProfessional Health
Betsy White Williams, Ph.D., M.P.H.Betsy White Williams, Ph.D., M.P.H.Rush University Medical SchoolRush University Medical SchoolProfessional Renewal CenterProfessional Renewal Center
Reid Finlayson, MDReid Finlayson, MDAssistant Professor of PsychiatryAssistant Professor of PsychiatryDirectorDirectorVanderbilt Comprehensive Vanderbilt Comprehensive Assessment ProgramAssessment Program
Martha E. Brown, MDMartha E. Brown, MDAssoc. Dean Faculty DevelopmentAssoc. Dean Faculty DevelopmentAssociate Professor of PsychiatryAssociate Professor of PsychiatryUSF College of Medicine USF College of Medicine

William Swiggart, MS, LPC/MHSPWilliam Swiggart, MS, LPC/MHSPAssociate in MedicineAssociate in Medicine
Co-DirectorCo-DirectorVanderbilt Center for Professional Vanderbilt Center for Professional
HealthHealth
www.mc.vanderbilt.edu/cph

Disruptive / DistressedDisruptive / DistressedPhysiciansPhysicians

44
When “a little chat” doesn't When “a little chat” doesn't workwork
Mr. Bangsiding felt (and wrongly so) that a littlechat would be enough to stop Bob’s disruptive behavior.

2004 AAMC Council of 2004 AAMC Council of DeansDeans
“Physicians are often poorly socialized and enter medical school with inadequate social skills for practice.”
“There is a growing body of literature documenting residency programs do notprepare resident physicians adequately for the practice of medicine.”

Why bother dealing Why bother dealing with disruptive with disruptive
behavior?behavior?

Reported PrevalenceReported PrevalenceState/State/
CountryCountryPrevalencPrevalenc
eeSourceSource
AlabamaAlabama 12%12% ReferralsReferrals
IndianaIndiana 8%8%
1%1%ReferralsReferrals
StatewideStatewide
KentuckyKentucky 20%20%
0.4%0.4%ReferralsReferrals
StatewideStatewide
TennesseeTennessee 30%30% ReferralsReferrals
WisconsinWisconsin 30%30% ReferralsReferrals
AustraliaAustralia 36%36% ReferralsReferrals
EnglandEngland 6%6% DisciplinarDisciplinaryy
Multiple References Available

Failure to Address Failure to Address Disruptive Conduct Leads Disruptive Conduct Leads
ToTo Team members may adopt disruptive Team members may adopt disruptive
person’s negative mood/angerperson’s negative mood/anger (Dimberg & (Dimberg & Ohman, 1996)Ohman, 1996)
Lessened trust among team members Lessened trust among team members can lead to lessened task performance can lead to lessened task performance (always monitoring disruptive (always monitoring disruptive person)...person)... effects quality and pt safety effects quality and pt safety (Lewicki & Bunker, 1995; Wageman, 2000)(Lewicki & Bunker, 1995; Wageman, 2000)
Felps, W et al. 2006. How, when, and why bad apples spoil the barrel: negative group members and dysfunctional groups. Research and Organizational Behavior, Volume 27, 175-222.

Disruptive Behavior Leads to Disruptive Behavior Leads to Communication Problems…Communication Problems…
Communication Problems Lead To Communication Problems Lead To Adverse EventsAdverse Events11
Communication breakdown factored in OR errors 50% Communication breakdown factored in OR errors 50%
of the timeof the time22
Communication mishaps were associated with 30% of Communication mishaps were associated with 30% of
adverse events in OBGYNadverse events in OBGYN33
Communication failures contributed to 91% of adverse Communication failures contributed to 91% of adverse
events involving residentsevents involving residents44
Gerald B. Hickson, MDJames W. Pichert, PhD
Center for Patient & Professional AdvocacyVanderbilt University School of Medicine
1. Dayton et al, J Qual & Patient Saf 2007; 33:34-44. 3. White et al, Obstet Gynecol 2005; 105(5 Pt1):1031-1038.
2. Gewande et al, Surgery 2003; 133: 614-621. 4. Lingard et al, Qual Saf Health Care 2004; 13: 330-334

Disruptive Behavior Disruptive Behavior CreatesCreates
fearfear confusion or uncertaintyconfusion or uncertainty vengeance vs. those who vengeance vs. those who
oppose/oppress themoppose/oppress them hurt ego/pridehurt ego/pride grief (denial, anger, grief (denial, anger,
bargaining)bargaining) apathyapathy burnoutburnout unhealthy peer pressuresunhealthy peer pressures
ignorance ignorance (expectations, behav. (expectations, behav. standards, rules, standards, rules, protocols, chain of protocols, chain of command, standards of command, standards of care)care)
distrust of leadersdistrust of leaders dropout: early dropout: early
retirement or relocation retirement or relocation errorserrors disruptive behavior disruptive behavior
begets disruptive begets disruptive behaviorbehavior
Vanderbilt University and Medical Center Policy #HR-027

AggressiveAggressive
Anger Outbursts
Profane/Disrespectful Language
Throwing Objects
Demeaning Behavior
Physical Aggression
Sexual Comments or Harassment
Racial/Ethnic Jokes
PassivePassiveAggressiveAggressive
Derogatory comments about institution, hospital, group, etc.
Refusing to do tasks
PassivePassive
Chronically late
Not responding to call
Inappropriate or inadequate chart notes
Spectrum of Disruptive Behaviors

“The Perfect Storm”
PhysicianHospital/Clinic
The external system The internal system
Two systems interact Two systems interact
Good skills
Poor skills
Functional & nurturing
Dysfunctional

13
©CPPA, 2008
Why are we so Why are we so hesitant to act?hesitant to act?

The Balance BeamThe Balance Beam
1414
Do nothing Do something
Staff satisfaction and retention
Reputation
Patient safety, clinical outcomes
Liability, risk mgmt costsFear of antagonizing
Leaders “blink”
Not sure how lack tools, training
Competing priorities
“Can’t change…”
June 2009, Unprofessional Behavior in Healthcare Study, Studer Group and Vanderbilt Center for Patient and Professional Advocacy; Hickson GB, Pichert JW. Disclosure and Apology. National Patient Safety Foundation Stand Up for Patient Safety Resource Guide, 2008; Pichert JW, Hickson GB, Vincent C: “Communicating About Unexpected Outcomes and Errors.” In Carayon P (Ed.). Handbook of Human Factors and Ergonomics in Healthcare and Patient Safety, 2007

15
©CPPA, 2008
Why Might a Medical Why Might a Medical Professional Behave in Ways Professional Behave in Ways
that are Disruptive?that are Disruptive?
1. Substance abuse, psych issues1. Substance abuse, psych issues
2. Narcissism, perfectionism2. Narcissism, perfectionism
3. Spillover of family/home problems3. Spillover of family/home problems
4. Poorly controlled anger4. Poorly controlled anger//Snaps under Snaps under heightened stress, perhaps due to:heightened stress, perhaps due to:a. Poor clinical/administrative/systems supporta. Poor clinical/administrative/systems support
b. Poor mgmt skills, dept out of controlb. Poor mgmt skills, dept out of control
c. Back biters create poor practice c. Back biters create poor practice environmentsenvironments

16
©CPPA, 2008
Why Might a Medical Why Might a Medical Professional Behave in Ways Professional Behave in Ways
that are Disruptive?that are Disruptive?
5. Well, it seems to work pretty well5. Well, it seems to work pretty well
6. No one addressed it earlier (why? See #5)6. No one addressed it earlier (why? See #5)
7. 7. Family of origin issues—guilt and shameFamily of origin issues—guilt and shame
8.8.
9.9.

EtiologiesEtiologies Individual FactorsIndividual Factors
Predisposing Psychological FactorsPredisposing Psychological Factors11
Alcohol and Drug Family HistoryAlcohol and Drug Family History Trauma HistoryTrauma History Religious FundamentalismReligious Fundamentalism Familial High AchievementFamilial High Achievement
Personality TraitsPersonality Traits22
NarcissismNarcissism Obsessive/CompulsiveObsessive/Compulsive
Physician BurnoutPhysician Burnout33
Clinical Skills Satisfactory or Above AverageClinical Skills Satisfactory or Above Average44
1. Valliant, 1972 2. Gabbard, 19853. Spickard and Gabbe, 2002 4. Papadakis, 2004, 2005

EtiologiesEtiologies
Institutional FactorsInstitutional Factors11
ScapegoatsScapegoats System Reinforces BehaviorSystem Reinforces Behavior Individual Pathology may over-shadow Individual Pathology may over-shadow
institutional pathologyinstitutional pathology
Williams and Williams, 2004

19
©CPPA, 2008
What controls What controls behavior?behavior?
Thomas Krause, PhDPresentation at the National Patient Safety Foundation Board of Governors Meeting June, 2007

20
©CPPA, 2008
ConsequencesConsequences Consequences control behaviorConsequences control behavior Antecedents influence behavior only Antecedents influence behavior only
to the extent that they predict to the extent that they predict consequences…consequences…
Timing, consistency and significance Timing, consistency and significance of consequences affect their impactof consequences affect their impact
Thomas Krause, PhDPresentation at the National Patient Safety Foundation Board of Governors Meeting June, 2007

ConsequencesConsequences disharmony and poor moraledisharmony and poor morale11, , staff turnoverstaff turnover22, , incomplete and dysfunctional communicationincomplete and dysfunctional communication11, , heightened financial risk and litigationheightened financial risk and litigation33, , reduced self-esteem among staffreduced self-esteem among staff11, , reduced public image of hospitalreduced public image of hospital11, , financial costfinancial cost11, , unhealthy and dysfunctional work environmentunhealthy and dysfunctional work environment11, ,
andand potentially poor quality of carepotentially poor quality of care1,2,31,2,31. Piper, 20002. Rosenstein, 20023. Hickson, 2002

Characteristics and Characteristics and Behavioral Change in the Behavioral Change in the
First 39 Disruptive First 39 Disruptive PhysiciansPhysicians
Samenow CP, Swiggart W, Blackford J, Fishel T, Dodd D, Neufeld R, Spickard A. A CME Course Aimed at Addressing Disruptive Behavior. Physician Executive; 34 (1) Jan/Feb 2008: 32-40.

2323
General TrendsGeneral Trends At 3 months, significant improvements in At 3 months, significant improvements in
20 of the 22 physicians20 of the 22 physicians Increased motivating behaviors and Increased motivating behaviors and
motivating impactmotivating impact Decreased disruptive behaviors and Decreased disruptive behaviors and
disruptive impactdisruptive impact Changes in behavior reported by “others”Changes in behavior reported by “others”
Samenow CP, Swiggart W, Blackford J, Fishel T, Dodd D, Neufeld R, Spickard A. A CME Course Aimed at Addressing Disruptive Behavior. Physician Executive; 34 (1) Jan/Feb 2008: 32-40.

DemographicsDemographics Total Physicians Studied = 39Total Physicians Studied = 39 Mean Age: 49.7 (compare to CPH mean age Mean Age: 49.7 (compare to CPH mean age
49)49) Age Range: 27 - 64Age Range: 27 - 64 Predominantly Male (84%) and Caucasian Predominantly Male (84%) and Caucasian
(87%)(87%) 49% Married, 10% Divorced, 26% Multiple, 49% Married, 10% Divorced, 26% Multiple,
10% Single10% Single Group Practice/Partnership (41%), Hospital Group Practice/Partnership (41%), Hospital
Based (21%), Solo (10%), Trainee (3%)Based (21%), Solo (10%), Trainee (3%)Samenow CP, Swiggart W, Blackford J, Fishel T, Dodd D, Neufeld R, Spickard A. A CME Course Aimed at Addressing Disruptive Behavior. Physician Executive; 34 (1) Jan/Feb 2008: 32-40.

Specialty TypesSpecialty Types
5 (13%)5 (13%)OtherOther 1 (3%)1 (3%)DentistDentist 2 (5%)2 (5%)Emergency MedEmergency Med
4 (10%)4 (10%)General SurgeryGeneral Surgery 5 (13%)5 (13%)Ob/GynOb/Gyn 5 (13%)5 (13%)Specialty SurgerySpecialty Surgery
5 (13%)5 (13%)General General Med/Family Med/Family PracticePractice
5 (13%)5 (13%)AnesthesiaAnesthesia
7 (18%)7 (18%)Specialty MedicineSpecialty Medicine
Samenow CP, Swiggart W, Blackford J, Fishel T, Dodd D, Neufeld R, Spickard A. A CME Course Aimed at Addressing Disruptive Behavior. Physician Executive; 34 (1) Jan/Feb 2008: 32-40.

Infrastructure for Addressing Infrastructure for Addressing Unprofessional BehaviorUnprofessional Behavior
Leadership commitmentLeadership commitment Model to guide graduated interventionsModel to guide graduated interventions Supportive institutional policiesSupportive institutional policies Surveillance tools to capture pt/staff Surveillance tools to capture pt/staff
allegationsallegations Processes for reviewing allegationsProcesses for reviewing allegations Multi-level professional/leader trainingMulti-level professional/leader training Resources to help disruptive colleaguesResources to help disruptive colleagues Resources to help disrupted staff and patientsResources to help disrupted staff and patients
Hickson GB, Pichert JW, Webb LE, Gabbe SG. A Complementary Approach to Promoting Professionalism: Identifying, Measuring and Addressing Unprofessional Behaviors. Academic Medicine. November, 2007.

2727
Potential Resources for Healthy Potential Resources for Healthy CopingCoping
CoursesCourses Coaches, Coaches,
counselorscounselors Comprehensive Comprehensive
EvaluationEvaluation 360360° Evaluations° Evaluations Risk ManagersRisk Managers Physician WellnessPhysician Wellness Treatment CentersTreatment Centers
Office of General Office of General Counsel Counsel
State BMEState BME Professional SocietiesProfessional Societies QI OfficersQI Officers EAPEAP OthersOthers State Physician Health State Physician Health
ProgramProgram

Reid Finlayson, MDReid Finlayson, MDDirector, Vanderbilt Comprehensive Assessment ProgramDirector, Vanderbilt Comprehensive Assessment ProgramAssociate Professor of PsychiatryAssociate Professor of Psychiatry
www.mc.vanderbilt.edu/root/vcap

““Disruptive” Disruptive” Health Care Health Care
ProfessionalsProfessionals1)1) Literature reviewLiterature review2)2) Fitness-for-duty evaluationsFitness-for-duty evaluations3)3) Future researchFuture research

““More than 20% of caregivers have More than 20% of caregivers have witnessed actual harm come to patients as a witnessed actual harm come to patients as a
result of condescending, insulting or rude result of condescending, insulting or rude behavior by professionals.”behavior by professionals.”

SEVEN ZONES OF SILENCE: SEVEN ZONES OF SILENCE: Broken rules, Mistakes, Lack of support, Broken rules, Mistakes, Lack of support,
Incompetence, Poor teamwork, Incompetence, Poor teamwork, Disrespect, MicromanagementDisrespect, Micromanagement



N=4530 RN=2846 MD=944
Rosenstein and O’Daniel, 2008

Rebecca Saxton et al 2009

Rebecca Saxton et al 2009

Comprehensive Comprehensive EvaluationEvaluation
APA guidelines for Fitness for Duty APA guidelines for Fitness for Duty EvaluationsEvaluations
Multidisciplinary: 1-5 days Multidisciplinary: 1-5 days MedicalMedical Psychiatric evaluationPsychiatric evaluation Psychological testingPsychological testing Psychosocial including genogramPsychosocial including genogram Addiction screeningAddiction screening Collateral informationCollateral information
Comprehensive report with Comprehensive report with recommendationsrecommendations

Disruptive Data, Axis I Disruptive Data, Axis I diagnosisdiagnosis
n = 118n = 118
No DiagnosisNo Diagnosis 5252 Dysthymic D/ODysthymic D/O 1616 Adj. D/OAdj. D/O 1313 SIMD/PTSD/MDDSIMD/PTSD/MDD 1717 Substance Abuse/DepSubstance Abuse/Dep 1616 Int. Explosive D/OInt. Explosive D/O 4 4 Other (Other (psychosis, cognitive d/o, bipolarpsychosis, cognitive d/o, bipolar))
1212

Disruptive Data, Axis II Disruptive Data, Axis II diagnosisdiagnosis
n = 118n = 118
Narcissistic TraitsNarcissistic Traits 4141 Personality D/O, NOSPersonality D/O, NOS 3535 Compulsive TraitsCompulsive Traits 2626 Defer/NoneDefer/None 2525 Other traitsOther traits 1313 Other Pers. D/OOther Pers. D/O 7 7

Disruptive Data: Axis IIIDisruptive Data: Axis IIIn=118n=118
None – 29None – 29 Occular-3Occular-3 ENT/allergy-9ENT/allergy-9 CNS - brain lesions -7; seizures-1; migraine-3CNS - brain lesions -7; seizures-1; migraine-3 Cardiac - CAD-2; HTN-19; arrhythmia-5; Cardiac - CAD-2; HTN-19; arrhythmia-5;
dyslipidemia-9dyslipidemia-9 Diabetes – type I – 3; type II - 4Diabetes – type I – 3; type II - 4 Hypothyroid - 7Hypothyroid - 7 Respiratory asthma/bronchitis- 6; sleep apnea- 5Respiratory asthma/bronchitis- 6; sleep apnea- 5 GI - obesity -10; bariatric surgery-1; GERD or GI - obesity -10; bariatric surgery-1; GERD or
ulcer-12; IBS-3; const-1; Liver-3ulcer-12; IBS-3; const-1; Liver-3 Cancers - 4Cancers - 4 Arthritic back- 9; other joint-13Arthritic back- 9; other joint-13

Case presentation – history Case presentation – history (1)(1)
Dr A is a 40 year old general surgeon referred Dr A is a 40 year old general surgeon referred for evaluation following several angry for evaluation following several angry outbursts in his hospital’s OR. The most outbursts in his hospital’s OR. The most egregious (and final) outburst involved his egregious (and final) outburst involved his threatening to shoot one of his OR staff. threatening to shoot one of his OR staff. Although he reportedly immediately told staff Although he reportedly immediately told staff that he wasn’t serious about the threat, a that he wasn’t serious about the threat, a complaint was filed because he was complaint was filed because he was commonly known to have an extensive gun commonly known to have an extensive gun collection at his home, and this staff member collection at his home, and this staff member lived in the same neighborhood. lived in the same neighborhood.

Rebecca Saxton et al, 2009
Rebecca Saxton 2009

The Disruptive Physician: A Conceptual The Disruptive Physician: A Conceptual OrganizationOrganization
Williams and Williams, 2008Williams and Williams, 2008

Problematic PhysiciansProblematic PhysiciansMMPI -2 Profile PAI MMPI -2 Profile PAI
CategoriesCategories
0
20
40
60
Ds Ch Nl nV
Disrupt
Sexual
Other 020406080
D I AS N
Disrupt
Sexual
Other
A - Disruptive n=39A - Disruptive n=39B – Sexual n=25B – Sexual n=25C – Other n=24C – Other n=24
Category AnalysisCategory Analysis
MMPI-2MMPI-2: Ds=distress, Ch=character, Nl=normal, nV=invalid: Ds=distress, Ch=character, Nl=normal, nV=invalidPAIPAI: D=distress, I-interpersonal, AS=antisocial, N=normal: D=distress, I-interpersonal, AS=antisocial, N=normal
*Roback, Howard et al, Canadian Journal of Psychiatry Vol 52, No 5, May 2007

Problematic Physicians A (Disruptive)
Valid profiles, open, high interpersonal dysfunction, admit and rationalize anger
B (Sexual) – FEWEST NORMAL PROFILES - MOST CHARACTER PATHOLOGY
Impulsive, selfish, low empathy, irresponsible Exaggerated positive light = Therapeutic
Challenge C (Other)
*Roback, Howard et al, Canadian Journal of Psychiatry Vol 52, No 5, May 2007

Systems and Monitoring
Betsy White Williams, Ph.D., M.P.H.Rush University Medical School
Professional Renewal Center

Background
• I have been asked to speak to:– The relationship between disruption and systems;– Monitoring and measurement of behavior.
• These may seem like unrelated issues, but in my view they are very closely intertwined.
4747BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Organization of the discussion
• I have taken the liberty of employing a few illustrative quotations to provide an organization for these thoughts.
• In the area of systems, this presentation focuses on three:– Social systems;– Institutional systems; and,– Personal systems.
BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010 48

Social Systems
• "All mankind is of one author, and is one volume;....No man is an island, entire of itself…, because I am involved in mankind; and therefore never send to know for whom the bell tolls; it tolls for thee.”
• John Donne: Meditation XVll
49BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Institutional Systems
• "Every system is perfectly designed to get the results it gets.”
• Batalden 2006, attributed variously, perhaps W. Edward Deming
50BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Personal Systems
• 'Cause, remember: no matter where you go... there you are.’
• Buckaroo Banzai In the Fourth Dimension
51BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Systems
• Systems nest like Russian dolls:Social SystemSocial System
Institutional SystemInstitutional System
Personal System
Personal System
52BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive Behavior – Personal Systems
• “… no matter where you go... there you are.’
• Can be based on a lack of social competence.• Can be based on a lack of behavioral
regulation.
Poor social competence Poor regulatory competence
53BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive Behavior – Personal Systems
• Can be aimed at diffuse and ill defined goals.
• Can be aimed at specific and well defined outcomes.W
ell d
efine
d ob
jecti
veIll
defi
ned
goal
54BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive Behavior – Personal Systems
Poor social competence Poor regulatory competence
Wel
l defi
ned
obje
ctive
Ill d
efine
d go
al
Demanding
Frustrated Angry
Manipulative
55BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive Behavior and Institutional Functioning
• "Every system is perfectly designed to get the results it gets.”
Social SystemSocial System
Angry
ManipulativeDemanding
Frustrated
Institutional SystemInstitutional System
Personal System
Personal System
56BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive Behavior and Institutional Functioning
• Disruptive behavior affects both the – Connotative elements
• Emotional well being,• Affiliation, as well as the
– Denotative elements of healthcare institutional functioning, including
• Role clarity,• Protocol implementation and duties, and,• Communications.
57BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

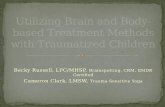
Disruptive Behavior and Institutional Functioning
• Emotional wellbeing is negatively affected:– A significant increase in
departments with identified physicians in:
• Depression, and• Anxiety
Mood Data
30.00
35.00
40.00
45.00
50.00
55.00
60.00
65.00
70.00
T ension Depr ession Anxiety Vigor Fatigue Conf usion
Mood
T-S
core
Physicians Nurses/Techs
Increased anxiety
Increased control and
fatigue
58BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive Behavior and Institutional Functioning
• Disruptive behavior decreases staff’s sense of affiliation with the healthcare institution.– A significant decrease in
staff’s reported sense of affiliation;
– A comparison of staff in a department with an identified disruptive member as compared to a matched department in the same institution.
-1.00 -0.75 -0.50 -0.25 0.00 0.25 0.50 0.75 1.00
Obligation
Affilliation
Loyalty
Index Comparison
59BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive Behavior and Institutional Functioning
• Disruptive behavior decreases staff’s understanding of their role.– A significant decrease in
staff’s reported understanding of their role;
– A comparison of staff in a department with an identified disruptive member as compared to a matched department in the same institution.
-1.00 -0.75 -0.50 -0.25 0.00 0.25 0.50 0.75 1.00
Clear Goals
Clear Clients
Unnecessary Tasks
Clear Tasks
Index Comparison
60BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive Behavior and Institutional Functioning
• Depending on the nature of the disruptive behavior it can engender:– Deviation from accepted institutional protocols;
and,– Support staff providing services out-of-scope.
61BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive Behavior and Institutional Functioning
• Disruptive behavior’s hallmark is a decrease in communication:– Such decreases are typically
marked by a decrease between the disruptive physician and others;
– Other patterns include decreased communications between micro-systems or even entire departments.
Team Cohesion Index Physician vs. Department
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Frequency Importance Comfort
62BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive Behavior and Institutional Functioning
• The presence of the system disruption ultimately results in breakdown:– Communications;– Affiliation;– Roles; and,– Protocols and duties.
63BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive behavior – Social systems
• ”… never send to know for whom the bell tolls; it tolls for thee.”
Social SystemSocial System
Institutional SystemInstitutional System
Angry
ManipulativeDemanding
Frustrated
Personal System
Personal System
64BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive behavior – Social systems
• The disruptive physician is referred to treatment, administrative procedure or both.
Social SystemSocial System
Institutional SystemInstitutional System
Personal System
Personal System
BoardBoard
PHPPHP
TreaterTreater
65BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive behavior – Social systems
• If the physician is returned to the institution to practice, it is necessary to ensure that the behavior does not recur,– There is a significant level of recidivism,– As high as 20% among “severe offenders” (Grant
and Alfred 2007)
• Prior behavioral issues are a significant risk factor for later disruption (Papadakis and collegues, see for example, Papadakis, Arnold et al. 2008)
66BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive behavior – Social systems
• A monitoring system that is under development measures these issues using a 360◦ survey.
• Early data show the survey to be well tolerated and demonstrates face validity.
• The survey was developed to facilitate integration with institutional systems.
67BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive behavior – Social systems
• Preliminary results suggest that disruptive physicians may not differ significantly from normal physicians in mean performance but may differ significantly in skew.
68BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010

Disruptive behavior – Social systems
• It seems likely that over time as the disruptive behavior is extinguished the pattern of data will modify.
• Early results suggest the proportion of extreme reports falls and moderate to good reports increase.
69B.W.WILLIAMS TO ACCOMPANY A TALK
DELIVERED AT THE FSPHP SPRING MEETING 2010

A Quick SummaryIssue Result
'Cause, remember: no matter where you go... there you are.’
The disruptive physician carries the behavioral consequences of their problem to all systems in which they function.
"Every system is perfectly designed to get the results it gets.”
A system in which a disruptive physician is functioning is a system in which a disruptive physician can function and perhaps prosper.
"All mankind is of one author, and is one volume;....No man is an island, entire of itself…, because I am involved in mankind; and therefore never send to know for whom the bell tolls; it tolls for thee.”
The disruptive physician can be treated, but if they are treated as an “island”, they are likely to return to the behaviors that had “worked” for them in the past.
BWWilliams to accompany a talk delivered at the FSPHP Spring Meeting 2010 70

Approaches To The Approaches To The Disruptive ProfessionalDisruptive Professional
Martha E. Brown, MDMartha E. Brown, MDAssociate Dean for Faculty Associate Dean for Faculty
DevelopmentDevelopment
Associate Professor of PsychiatryAssociate Professor of Psychiatry
USF College of MedicineUSF College of Medicine

Remembering this is treatable Remembering this is treatable is hardis hard
When the professional who is taking a When the professional who is taking a CME course on the issue, cusses out and CME course on the issue, cusses out and files complaints against your assistant files complaints against your assistant and the CME officeand the CME office
When the professional punches a hole in When the professional punches a hole in your wallyour wall
When the professional is arrested for When the professional is arrested for hiring people to injury and kill those who hiring people to injury and kill those who have made them madhave made them mad

The Solution Many ConsiderThe Solution Many Consider
Could be the most cost savingCould be the most cost saving Certainly efficientCertainly efficient Saves timeSaves time SimpleSimple Great fantasyGreat fantasy However, not real practical… However, not real practical…


Institutional Barriers To Institutional Barriers To Dealing With The ProblemDealing With The Problem
Medical Center and hospital leaders not Medical Center and hospital leaders not committed to addressing the problem committed to addressing the problem daily and want the PHP to do it alldaily and want the PHP to do it all
Directives do not come from the top downDirectives do not come from the top down Lack of funding for implementation of an Lack of funding for implementation of an
internal program in the organization internal program in the organization (selling point is that programs can save (selling point is that programs can save the organization $5.00 to $16.00 for the organization $5.00 to $16.00 for every dollar invested as well as decrease every dollar invested as well as decrease and prevent malpractice suits)and prevent malpractice suits)

Institutional Barriers To Institutional Barriers To Dealing With The ProblemDealing With The Problem
Behaviors not extensively Behaviors not extensively documenteddocumented
Hospitals do not want to “anger” Hospitals do not want to “anger” their top producerstheir top producers
No one likes lawyersNo one likes lawyers Lack of in-depth policies in the Lack of in-depth policies in the
hospital or practicehospital or practice


HAVING LESS AUTHORITY HAVING LESS AUTHORITY WITH DISRUPTIONWITH DISRUPTION
But Others See You As The But Others See You As The SolutionSolution

DETERMINING YOUR DETERMINING YOUR APPROACHAPPROACH
Do you want to monitor disruption?Do you want to monitor disruption? What legal support do you have?What legal support do you have? What is the level of your tolerance for What is the level of your tolerance for
dealing with the behavior?dealing with the behavior? What is the tolerance level of your staff for What is the tolerance level of your staff for
dealing with the behavior and do they need dealing with the behavior and do they need additional training?additional training?
Determine if you can accept delayed Determine if you can accept delayed gratificationgratification

STARTING AT THE TOPSTARTING AT THE TOP Talk with the referral source about what Talk with the referral source about what
policies they have in placepolicies they have in place Ask what the hospital or medical group is Ask what the hospital or medical group is
willing to do about the problemwilling to do about the problem Seek information from collateral sourcesSeek information from collateral sources Assess the level of the problemAssess the level of the problem
Inpatient evaluationInpatient evaluation Outpatient evaluationOutpatient evaluation 360 workplace evaluation360 workplace evaluation

STARTING AT THE TOPSTARTING AT THE TOP Can start with a comprehensive outpatient Can start with a comprehensive outpatient
evaluation with psychological testing evaluation with psychological testing Many outpatient evaluations SHOULD lead Many outpatient evaluations SHOULD lead
to a five to seven day inpatient evaluationto a five to seven day inpatient evaluation Determine what category the professional Determine what category the professional
falls within:falls within: Needs long-term inpatient treatment and has a Needs long-term inpatient treatment and has a
treatable disorder or an Axis II Disordertreatable disorder or an Axis II Disorder Determine can do well outpatient, can keep working, Determine can do well outpatient, can keep working,
needs information, therapy, monitoring, and/or CMEneeds information, therapy, monitoring, and/or CME Needs to find a paper hat jobNeeds to find a paper hat job

WHAT WE HAVE LEARNEDWHAT WE HAVE LEARNED
Medical student and resident training Medical student and resident training cultivates many of the disruptive cultivates many of the disruptive behaviors as they learn from their behaviors as they learn from their mentor’s behaviors mentor’s behaviors
It is important that the Federation It is important that the Federation start to work with medical schools to start to work with medical schools to ensure information on disruption is ensure information on disruption is included in the training programsincluded in the training programs

WHAT WE HAVE LEARNEDWHAT WE HAVE LEARNED
There is a need to develop standard, There is a need to develop standard, model policies for hospitals model policies for hospitals
Information needs to be widely Information needs to be widely distributed to hospitals and medical distributed to hospitals and medical practices that this is treatable, saves practices that this is treatable, saves money, prevents malpractice suits, money, prevents malpractice suits, and that early intervention is bestand that early intervention is best

WHAT WE HAVE LEARNEDWHAT WE HAVE LEARNED
Monitoring contracts need to be Monitoring contracts need to be flexibleflexible
360 evaluations are imperative for 360 evaluations are imperative for monitoring and to see how the monitoring and to see how the professional is progressingprofessional is progressing
Not all can be helped or savedNot all can be helped or saved Intensive small group CME with Intensive small group CME with
monitoring works for manymonitoring works for many

Summary Disruptive behavior is a patient safety
issue State PHPs can be an extremely
valuable resource for both physicians and institutions
An objective, comprehensive assessment is invaluable
It is important to understand the system’s issues related to an individual’s behavior