
Fr.tibia Dan Fibula_irham
34
Irham Khairi C 111 10 820 Advisor: dr. M. Luthfi Muammar dr. Andika Supervisor: dr. Muhammad Sakti, Sp.OT Department of Orthopedic and Traumatology Faculty of Medicine Hasanuddin University Makassar 2015 CASE REPORT OPEN COMMINUTIVE FRACTURE OF THE RIGHT TIBIA AND SEGMENTAL FRACTURE OF THE FIBULA GRADE IIIA
-
Upload
jefrizal-mat-zain -
Category
Documents
-
view
3 -
download
1
description
orthopedi
Transcript of Fr.tibia Dan Fibula_irham

Irham KhairiC 111 10 820
Advisor:dr. M. Luthfi Muammar
dr. AndikaSupervisor:
dr. Muhammad Sakti, Sp.OT
Department of Orthopedic and TraumatologyFaculty of Medicine Hasanuddin University
Makassar 2015
CASE REPORT
OPEN COMMINUTIVE FRACTURE OF THE RIGHT TIBIA AND SEGMENTAL FRACTURE OF THE FIBULA
GRADE IIIA

Name : BAge / Sex : 50 years old/ male Address : Emmy Saelan MakassarAdmission : January 8th, 2015MR : 479019
PATIENT IDENTITY

Chief complain : Wound at the right leg Anamnesis : Suffered since 15 minutes before
admitted to the hospital due to traffic accident Mechanism of trauma : The patient was cross the
street then got hit by a motorcycle from the right side.
History of unconsciousness (-), nausea (-), vomited (-).
HISTORY TAKING

A : PatentB : RR = 20 x/min, spontan, thoracoabdominal type.C : BP = 120/80 mmHg, RR = 7 x/min, regular, strong palpable. D : GCS 15 (E4M6V5), pupil isochors, Ø : 2.5 mm /2.5 mm , light reflex +/+E : T = 36.5o C (axillar temp)
Primary Survey

Right Leg RegionI : Lacerated wound at middle side from anterior aspect
extend to medial aspect, sized 10 x 5 x 2 cm, deformity (+), swelling (+), hematoma (+), muscle exposed (+), bone exposed (+).
P : Tenderness (+)ROM : active and passive motion at knee and ankle joint are
limited due to painNVD : sensibility is good, the pulse of dorsalis pedis artery is
palpable, capillary refill time < 2”
Secondary Survey

WBC 14,72 x 103 /uL RBC 4,02 x 106 /uL HGB 12,4 gm/dL HCT 36,3 % PLT 223 x 103 /uL CT 7’ 00’’ BT 2’30’’
LABORATORY FINDINGS

CLINICAL PICTURES

Radiologic findings

Open comminutive fracture of the right tibia grade III A
Open segmental fracture of the right fibula grade III A
Diagnosis

IVFD RL Antibiotic Anti tetanus Analgesic Debridement Immobilize fracture with long leg back slab
Planning :1. Plan for ORIF
MANAGEMENT

Male 50 years old, admitted to the hospital with chief complain of wound at right leg region due to traffic accident.
On physical Examination lacerated wound sized 10cm x 5cm x 2 cm at at anterior aspect extend to medial aspect, deformity (+), swelling (+), hematoma (+), muscle exposed (+), bone exposed (+).
ROM of knee joint and ankle joint was limited due to pain.
NVD: within normal limited On radiologic examination, there are comminutive
fracture at the right tibia and segmental fracture at the right fibula
SUMMARY

DISCUSSION
FRACTURE OF TIBIA AND FIBULA
Open fracture means that bone penetrated skin resulting in open wound and exposed to external environment.
Tibia is the major weight bearing of the leg (85% of the whole load), while fibula responsible for 6% -17% of weight bearing load.
INTRODUCTION

Anatomy

COMPARTMENTS OF THE LOWER LEG

Anterior Compartement
Thompson,JD. Netter's concise atlas of orthopedic anatomy.2004.

Lateral Compartement
Thompson,JD. Netter's concise atlas of orthopedic anatomy.2004.

Superficial Posterior Compartement
Thompson,JD. Netter's concise atlas of orthopedic anatomy.2004.

Deep Posterior Compartement
Thompson,JD. Netter's concise atlas of orthopedic anatomy.2004.
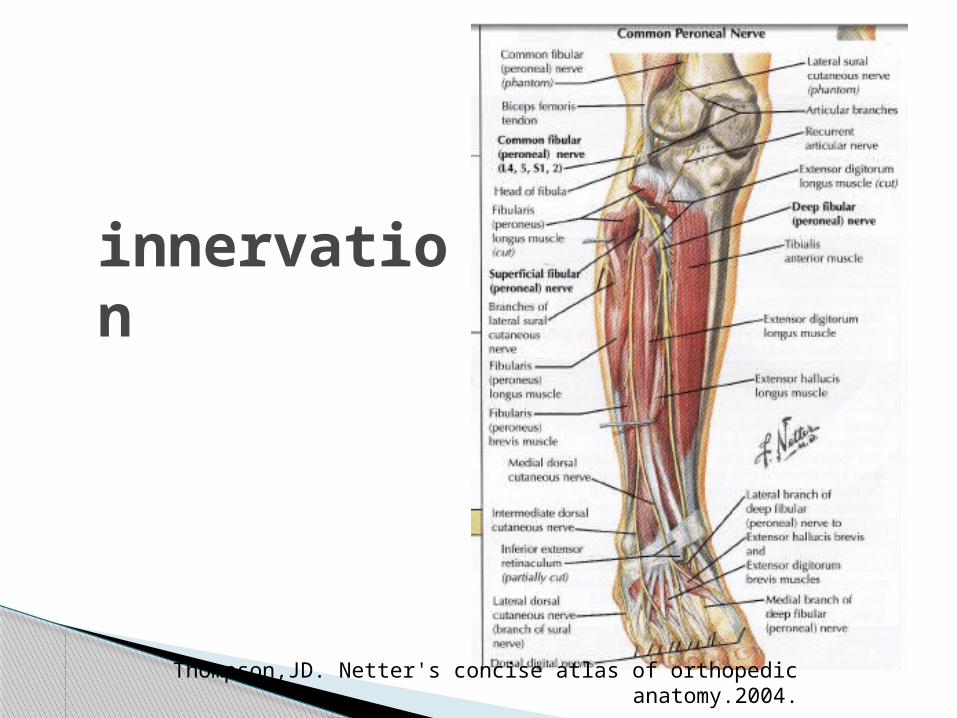
innervation
Thompson,JD. Netter's concise atlas of orthopedic anatomy.2004.

Vascularitation
Thompson,JD. Netter's concise atlas of orthopedic anatomy.2004.

Muller’s Classification
Solomon L, Warwick D, Nayagam S. Injuries of the knee&leg. In: Apley’s system of orthopaedic and fractures. 8th edition. New York: Oxford University
Press Inc; 2001.
PROXIMAL
DISTAL

MECHANISM OF INJURY
Indirect • Low energy• Spiral or long oblique• Bone fragment may pierce the
skin from within
Direct • High energy• Crushes or splits the skin• Usual open
Solomon L, Warwick D, Nayagam S. Injuries of the knee&leg. In: Apley’s system of orthopaedic and fractures. 8th edition. New York: Oxford University
Press Inc; 2001.

Gustilo and Anderson Classification for open fracture
Type Wound Level of contamination Soft tissue injury Bone injury
I < 1 cm long
Clean Minimal Simple, minimal comminution
II > 1 cm long
Moderate Moderate, some muscle damage
Moderate comminution
IIIA Usually > 10 cm
High Severe with crushing Usually comminuted; soft tissue coverage of bone possible
IIIB Usually > 10 cm
High Very severe loss of coverage; usually require soft tissue reconstruction surgery
Bone coverage poor; variable may be moderate to severe comminution
IIIC Usually > 10 cm
High Vascular injury requiring repair
Kenneth Koval, et al. Handbook of fractures third edition. 2006. Lippincott Williams and wilkins. USA
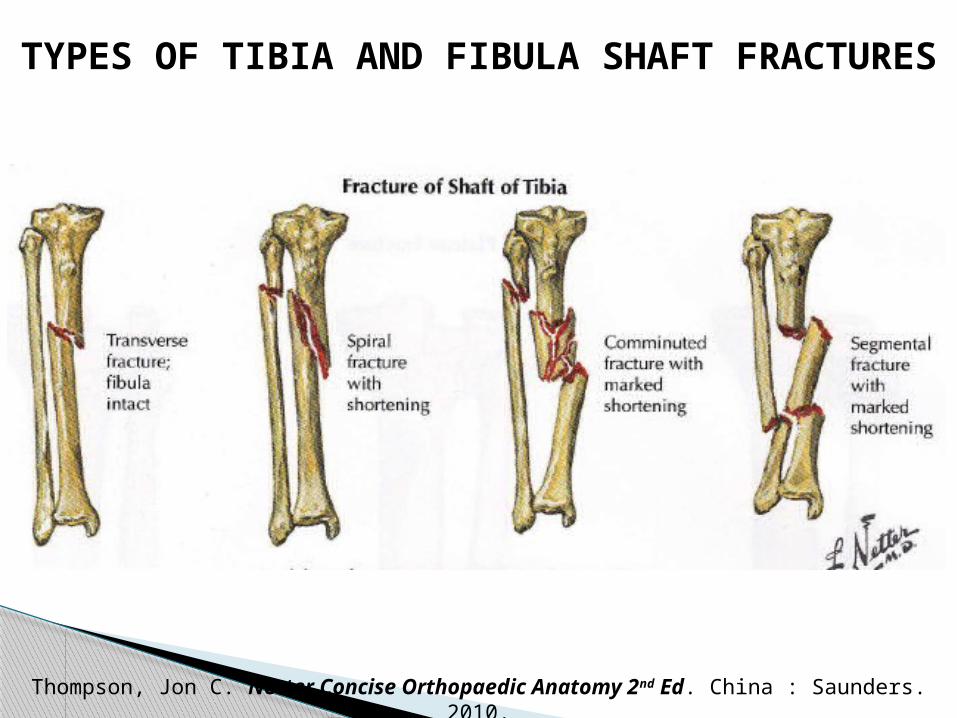
TYPES OF TIBIA AND FIBULA SHAFT FRACTURES
Thompson, Jon C. Netter Concise Orthopaedic Anatomy 2nd Ed. China : Saunders. 2010.

Clinical features Soft tissue damage :
bruise severe swelling crushing or tenting of skin open wound circulatory changes weak or absent pulses diminution or loss of sensation and ability to move the
toes Deformity Alert for impending compartment syndrome
Solomon L, Warwick D, Nayagam S. Injuries of the knee&leg. In: Apley’s system of orthopaedic and fractures. 8th edition. New York: Oxford University
Press Inc; 2001.

Diagnosis
History Taking : History of illness, Mechanism of trauma
Physical examination: LOOK, FEEL, MOVE (examine the good limb the
bad limb) X- ray, with rule of ‘2’:
2 view, 2 limb, 2 joint, 2 occasion, 2 injuries Laboratory examination

Goals of fracture management
• Fracture site, types of fractureRecognize
• For adequate apposition and normal alignment of boneReduction
• Immobilize promote soft tissue healingRetention
• As early as possible by active and passive exercise (restore function)
Rehabilitation

Management

Low energy fracture
Non operative: CastingSplint
Bracing
Operative : Intramedullary nailing
Plates fixation External fixation
Solomon L, Warwick D, Nayagam S. Injuries of the knee&leg. In: Apley’s system of orthopaedic and fractures. 8th edition. New York: Oxford University
Press Inc; 2001.
High energy fracture
- Transverse fracture : surgical- Comminuted & segmental fracture : surgical
stabilization- Open fracture : external fixation
- Closed fracture : external fixation & closed nailing
Solomon L, Warwick D, Nayagam S. Injuries of the knee&leg. In: Apley’s system of orthopaedic and fractures. 8th edition. New York: Oxford University Press Inc; 2001.

Complication
Early complications Compartment syndrome Vascular injury Infection
Late complications Malunion Delayed union Non union Joint stiffness
Solomon L, Warwick D, Nayagam S. Injuries of the knee&leg. In: Apley’s system of orthopaedic and fractures. 8th edition. New York: Oxford University Press Inc; 2001.

THANK YOU


















