From Pills to wires SMEL meeting April 2009 Joseph Macari.
47
From Pills to wires SMEL meeting April 2009 Joseph Macari
-
date post
22-Dec-2015 -
Category
Documents
-
view
217 -
download
2
Transcript of From Pills to wires SMEL meeting April 2009 Joseph Macari.

From Pills to wires
SMEL meeting April 2009Joseph Macari

From Pills to wires…

Road Map
A bit of history of Electrophysiology Different disease needs different therapy Heart Failure the problem and the solution Future

Road Map
A bit of history of Electrophysiology Different disease needs different therapy Heart Failure the problem and the solution Future


Hippocrates (460 – 375 BC)
“Those who suffer from frequent and strong faints without any manifest cause die suddenly.”

Willem Einthoven 1860 - 1927
Electrodes were salt water
Father of Electrocardiography

Einthoven’s Electrocardiograph Machine
An entire lab was dedicated to the ECG (EKG)

Hand-operated “Pacemaker” by Albert Hyman
Hyman AS, Resuscitation of the stopped heart by intracardiac therapy, Arch Int Med 1932; 50: 283-305

Hyman’s Artificial Pacemaker and needles
Hymanotor mfg by Adlanco, a U.S. division of Siemens

1958 to 2008 - Side-by Side comparison

1958 to 2008 - Implant
1958 Open thoracotomy General anesthesia 3 to 4 hours
Weeks in hospital 38 cc, 83 grams
24 cm2, 16 mm thick
2 transistors
Longevity < 1 yr Modes of operation: 1 (preset)
Rates: 1 (preset)
Rate Response: None
Parameter combinations: 1
2008 Leads inserted through vein Local anesthesia / sedation One to two hours Same day discharge 12 cc, 29 grams 19 cm2, 6.0 mm thick 20,000,000+ transistors Up to 20 years, at least 5 yr Modes of operation: Over 20 Rates: 30 to 180 pulses/min Rate Response: Tailored to
patient Parameter combinations:
Trillions
Road Map
A bit of history of Electrophysiology Different disease needs different therapy Heart Failure the problem and the solution Future

Bradycardia and Pace Maker
T / I
*
*Atrial lead
Ventricular Lead
• Pacing in both the atriumand ventricle
• Sensing in both the atrium and ventricle
• Intrinsic P wave and intrinsic QRS can inhibit pacing
• Intrinsic P Wave can “trigger” a paced QRS
I

Ventricular Tachycardia and defibrillator
Ventricular fibrillation
Sinus rhythm
…Degenerate to a lethal rhythm...
unless a shock is delivered to restore sinus rhythm
Heart Failure and cardiac resynchronization therapy

Pulse Generator
BatteryBattery
Pacing/Shocking Pacing/Shocking CircuitCircuit
Sensing CircuitSensing Circuit

Components of an Implantable System Heart
◦Disease state - signal quality◦Therapy requirements
Lead◦Receives signals from the heart◦Carry therapy to heart
Implantable Device (Pace Maker, ICD, CRT)◦Processes signals from lead◦Generates & delivers therapy to the Heart
through the Lead

Who’s at risk?

1.Extremely Common2.Extremely Deadly3.Extremely Expensive4. Solution?
Heart Failure

Testicular Cancer
Mild Heart Failure
Which would you prefer ?

0
20
40
60
80
100
5 year Survival0
20
40
60
80
100
5 year Survival
93%
60%
Testicular Cancer Heart Failure
Survival rate
15 Million People world wide suffer from HF
Which kills the most people ?1. Breast Cancer 2. Car Accidents 3. Lung Cancer4. Heart Failure
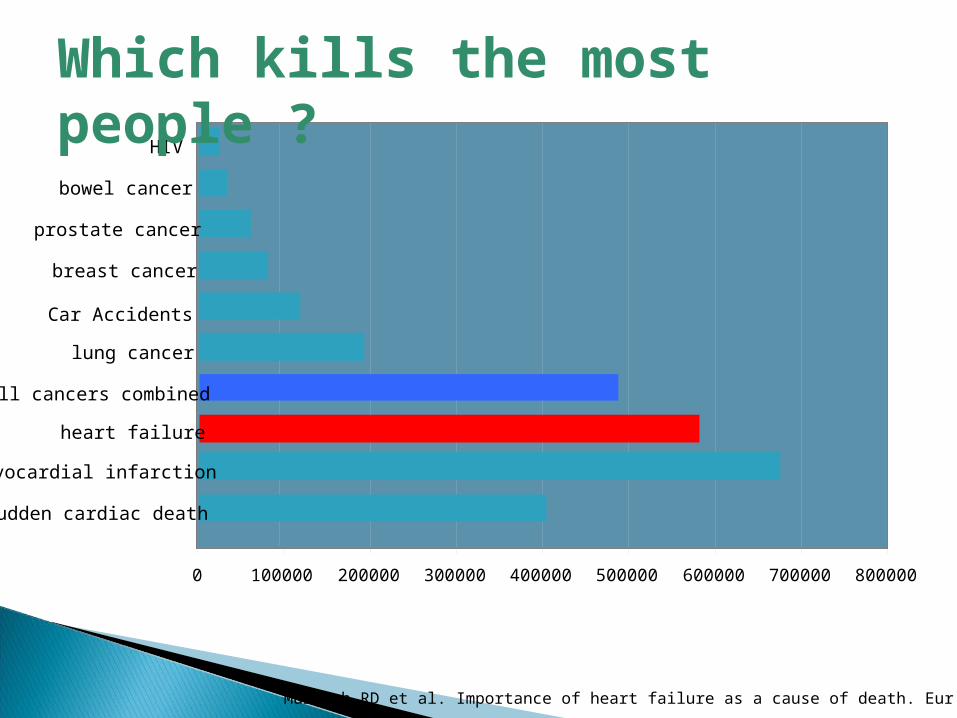
0 100000 200000 300000 400000 500000 600000 700000 800000
heart failure
sudden cardiac death
All cancers combined
lung cancer
breast cancer
prostate cancer
bowel cancer
myocardial infarction
HIV
Car Accidents
Murdoch RD et al. Importance of heart failure as a cause of death. Eur H J 1998;19
Which kills the most people ?
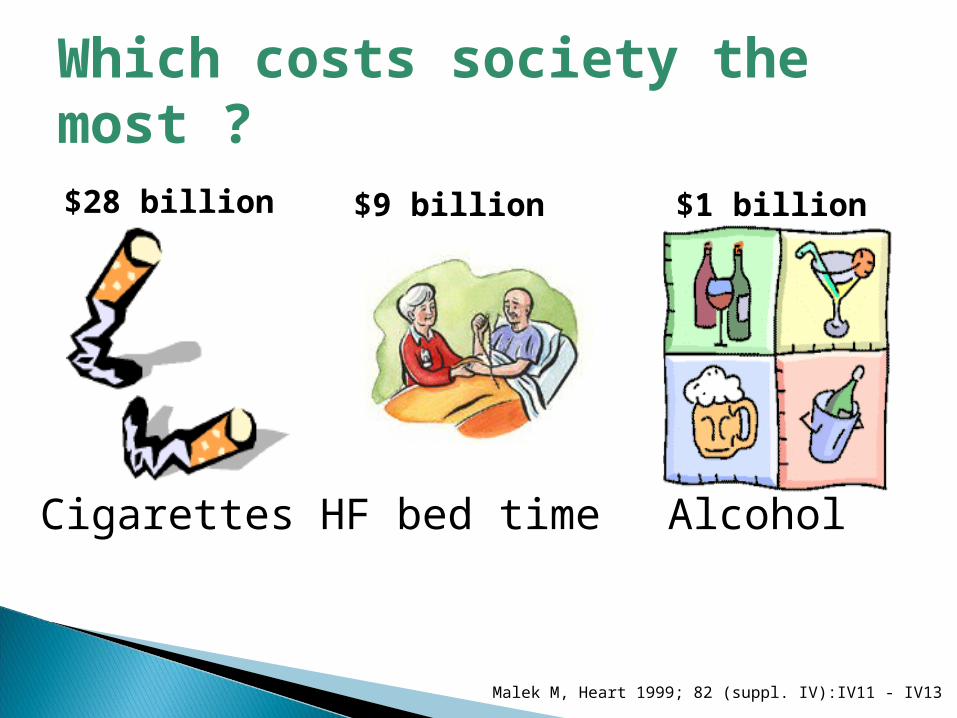
Cigarettes HF bed time Alcohol
$28 billion $9 billion $1 billion
Malek M, Heart 1999; 82 (suppl. IV):IV11 - IV13
Which costs society the most ?

Pump Failure Sudden Cardiac Death
How does Heart Failure Kill you?

Symptoms Of Heart Failure Dyspnea Reduced exercise capacity Fatigue / weakness Nocturia Confusion Pulmonary Oedema
◦ Shortness of breath◦ Congestion◦ Global fatigue◦ Ankle oedema
None

Jessup M, Brozena S. Medical Progress-Heart Failure. N Eng J Med 2003; 348: 2007-2018. Copyright 2002 Massachusetts Medical Society. All rights reserved.
The treatment of heart failureThe treatment of heart failure

The Vicious Cycle of Heart Failure Management
Chronic HF
MD’s Office
Emergency Room
Hospitalization
SOB
Weight
PO LasixIV Lasix or Admit
Diuresis & Home

Therapy
• All measures under stages A,B, and C
• Mechanical assist devices
• Heart transplantation
• Continuous (not intermittent) IV inotropic infusions for palliation
• Hospice care
Treatment Approach for the Patient with HF
Stage A
At high risk, no structural disease
Stage B
Structural heart disease,
asymptomatic
Stage D
Refractory HF requiring
specialized interventions
Therapy
• Treat Hypertension
• Treat lipid disorders
• Encourage regular exercise
• Discourage alcohol intake
• ACE inhibition
Therapy
• All measures under stage A
• ACE inhibitors in appropriate patients
• Beta-blockers in appropriate patients
Therapy
• All measures under stage A
Drugs:
• Diuretics
• ACE inhibitors
• Beta-blockers
• Digitalis
• Dietary salt restriction
Stage C
Structural heart disease with prior/current
symptoms of HF
Hunt, SA, et al ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult, 2001
Heart Failure and the Donkey Analogy

General Measures
Weight reduction
Discontinue smoking
Avoid alcohol and other cardiotoxic substances
Exercise
Treat HTN, hyperlipidemia, diabetes, arrhythmias
Coronary revascularization
Anticoagulation
Immunization
Sodium restriction
Daily weights
Close outpatient monitoring
Lifestyle ModificationsLifestyle Modifications Medical ConsiderationsMedical Considerations

Pharmacologic Management
Used to relieve fluid retention Improve exercise tolerance Facilitate the use of other drugs indicated for heart failure Patients can be taught to adjust their diuretic dose based on
changes in body weight Electrolyte depletion a frequent complication Should never be used alone to treat heart failure Higher doses of diuretics are associated with increased mortality
DiureticsDiuretics

Diuretics, ACE Inhibitors
Reduce the number of sacks on the wagon

Pharmacologic Management
Cardioprotective effects due to blockade of excessive SNS stimulation
In the short-term, beta blocker decreases myocardial contractility; increase in EF after 1-3 months of use
Long-term, placebo-controlled trials have shown symptomatic improvement in patients treated with certain beta-blockers1
When combined with conventional HF therapy, beta-blockers reduce the combined risk of morbidity and mortality, or disease progression1
1Hunt, SA, et al ACC/AHA Guidelines for the Evaluation and Management of Chronic Heart Failure in the Adult, 2001 p. 20.
Beta-BlockersBeta-Blockers

ß-Blockers
Limit the donkey’s speed, thus saving energy

Pharmacologic Management
Enhances inotropy of cardiac muscle
Reduces activation of SNS and RAAS
Controlled trials have shown long-term digoxin therapy:◦ Reduces symptoms◦ Increases exercise tolerance◦ Improves hemodynamics◦ Decreases risk of HF progression◦ Reduces hospitalization rates for decompensated HF◦ Does not improve survival
DigoxinDigoxin

Digitalis Compounds
Like the carrot placed in front of the donkey

Device Therapy save and enhance lives

Cardiac Resynchronization Therapy
Increase the donkey’s (heart) efficiency
Merlin.net Patient Care Network (PCN)
Remote Patient Management

Today Without Remote Care
Patient Waiting Room
Required Programming Changes

1
Merlin.net Server
Housecall 3180-T Transmitter
PhysicianPatient
Patient makes appt. & calls on analog phone line
HC+ 3180-R Receiver
Any PC
Merlin@home RF Transmitter
w/InvisiLink
2
Physician
EMR
Office Visit for reprogramming
PhysicianAny PC
CLINIC
ANYWHERE
+ internet access
Merlin@home EMEAC (Q3 2008)

1
Merlin.net Server
Housecall 3180-T Transmitter
PhysicianPatient
Patient makes appt. & calls on analog phone line
HC+ 3180-R Receiver
Any PC
Physician
+ internet access
Merlin@home RF Transmitter
w/InvisiLink
2
Physician
EMR
Any PC
Office Visit for reprogramming
InvisiLink reprogramming
CLINIC
ANYWHERE
Merlin@home EMEAC (Q2 2009)

Virtual Patient Waiting Room
Tomorrow with Remote Care Model

The stethoscope analogy
Which is the most important part?

Thank you