From Apgar to Z-plasty
80
From Apgar to Z-plasty Pediatric Medical Terms
description
From Apgar to Z-plasty. Pediatric Medical Terms. But first…. ABG – Arterial blood gases Blood test using blood from an artery (usually radial artery) Used to determine gas exchange levels in the blood related to lung (respiratory) function Tests pH, and CO2 and O2 levels. One more…. - PowerPoint PPT Presentation
Transcript of From Apgar to Z-plasty

From Apgar to Z-plasty
Pediatric Medical Terms

But first….
• ABG – Arterial blood gases– Blood test using blood from an artery (usually
radial artery)– Used to determine gas exchange levels in the
blood related to lung (respiratory) function– Tests pH, and CO2 and O2 levels

One more….
• ABP – Arterial blood pressure– Blood pressure (force exerted by circulating blood
on walls of blood vessels) measured through an arterial line
– Often used in ICU

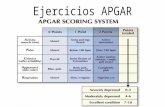
Apgar Score
• Virginia Apgar, U.S. anesthesiologist, 1909-1974)– System of scoring infant’s physical condition one
minute and five minutes after birth. – Heart rate, respiration, muscle tone, response to
stimuli and color– Each rated 0, 1, or 2 with maximum score of ’10’– Low scores = immediate attention– A low score at one minute is a sign of asphyxia– A low score at five minutes is an index of the
possibility of death

Apgar Score
Score
Sign 0 1 2
Heart Rate Absent Slow (less than 100) Greater than 100
Respiratory Effort Absent Slow, irregular Good; crying
Muscle tone Limp Some flexion of extremities
Active motion
Reflex irritability No response Grimace Cough or sneeze
Color Blue, pale Body pink; extremities blue
Completely pink

Atrial Septal Defect (ASD)• In developing fetus, the interatrial septum
develops to eventually separate the left and right atria
• ASD is a congenital heart defect involving the interatrial septum that enables blood to flow between the left and right atria
• Results in improper mixing of low oxygen venous blood (right side)with high oxygen arterial blood (left side)

ASD• This mixture of blood is called a ‘shunt.’ A
‘right to left’ shunt typically poses more danger for the patient.
• Results in cyanosis, pulmonary hypertension, right-sided heart failure, stroke

Patent Foramen Ovale
• The foramen ovale (foraymen ovalee) also remains open during fetal development but after birth it should close completely
• In approximately 25% of people, the foramen ovale does not entirely seal. Elevation in the pulmonary circulatory system (i.e., pulmonary hypertension -- chronic or transient,like when you cough) can cause the foramen ovale to remain open.

Patent foramen ovale
• This is a PFO – It is a small channel with little hemodynamic consequence. Clinically, it is linked to decompression sickness, paradoxical embolism and migraine. Investigation is underway about the role of PFO in stroke and TIAs in the absence of other problems.

Bronchopulmonary Dysplasia
• BPD• <34 weeks’ gestation and <4.5 pounds• Associated with infant respiratory distress
syndrome (IRDS)• Damage to lung tissuedue to prolonged mechanical ventilation

BPD
• Often a high amount of pressure and a higher oxygen concentration are necessary due to stiff, underdeveloped lungs
• Over time, pressure from the ventilator and excess oxygen intake can injure the lungs leading to IRDS.
• If IRDS persists, then dx of BPD is given if baby needs oxygen after 28 days or past 36 weeks’ postconceptual age.

BPD
• Also caused by trauma, pneumonia and other infections
• Associated with inflamation and scarring of lung tissues
• Tx with bronchodilators (albuterol) and diuretics to reduce buildup of fluid in lungs
• Severe cases – steroids (see Cushingoid faces)

Congenital Diaphragmatic Hernia
• CDH
• Applied to a variety of congenital birth defects that involve abnormal development of the diaphragm

CDH

CDH• Three major defects: – Failure of diaphragm to close– Herniation of abdominal contents into the chest– Pulmonary hypoplasia (decreased lung volume)
• Majority occur on left side, some on right side, small fraction bilateral
• Leads to severe, life-threatening respiratory distress
• Treatment is often……

Extracorporeal Membrane Oxygenation

ECMO
• Provides both cardiac and respiratory support when heart and lungs can no longer serve their function
• ~75% effective in saving a newborn’s life• Cannot be <4.5 pounds so rules out most
premature and/or small BW (birth weight) infants

ECMO machine

ECMO Machine

ECMO
• Time limit is usually around 21 days• Tubes are placed via a large vein at the base
of the neck (right side) with a cannula leading to the right atrium of the heart
• Another cannula is placed in a large artery (carotid)
• Cannulas are connected to tubing of the ECMO machine

Infant in ICU on ECMO

ECMO
• Blood drains from right side of neck through tubing
• Blood is oxygenated, rewarmed and returned to the body through the arterial cannula
• As heart/lungs improve, amount of blood flow through the circuit can be decreased

Free and Appropriate Public Education
• FAPE• Mandated by IDEA• Defines the rights of students with disabilities• Looks different for each child• Driven by the IEP process

Least Restrictive Environment
• LRE– The location in which FAPE is provided– Can vary based on severity of disability– We are required to evaluate what type of services
a child needs and create an environment that meets those needs

Apnea and Bradycardia
• ABC– Apnea is a pause in breathing with one or more of
the following characteristics:• > 15-20 sec• Associated with color change (pale, purplish or blue)• Associated with bradycardia
– Bradycardia• Slowing of the heart rate, usually <80 bpm• May be due to reflex (e.g., NGT or stooling)

ABC
• Common causes:– Prematurity, low blood sugar, infection, sz, PDA,
BI, high or low body temp, insufficient oxygen
• Common treatment:– Caffeine, CPAP, mechanical ventilation, periodic
stimulation

Clostridium difficile
• C. diff– Most serious cause of antibiotic associated
diarrhea (AAD) and can lead to colitis, a severe infection of the colon, often resulting from eradication of the normal gut flora by abx (antibiotics)
– Bacteria naturally residing in the body becomes overgrown, bacterium release toxins causing bloating, constipation, diarrhea with abdominal pain

C. diff• Human transmission by the fecal-oral route• Residence in hospital or nursing home is a risk
factor• Rate of acquisition is estimated to be 13% in
patients with hospital stays of up to 2 weeks and 50% in those longer than 4 weeks
• Vancomycin is treatment of choice• Wear gloves!! Wash with soap and water;
alcohol-based hand rubs are ineffective!!

CHARGE syndrome
• A recognizable (genetic) pattern of birth defects
• 1:9-10,000 births


• CHARGE (was a way to refer to the cluster of features seen)– Coloboma of the eye (a ‘cleft’ of the iris, retina,
choroid, macula or disc)– Heart defects– Atresia of the choanae– Retardation of growth and/or development– Genital and/or urinary abnormalities– Ear abnormalities and deafness

CHARGE
• These features are no longer used in making a dx of CHARGE syndrome, but the name stays
• Clinical dx is made using a combination of Major and Minor features– Coloboma, choanal atresia, CN abnormality, outer,
middle and/or inner ear, heart defects, cleft lip/palate, TE fistula, kidney abnormalities, genital abnormalities, growth deficiences, “typical face,” palm crease, behavior, limb/skeletal, etc.

Necrotizing enterocolitis
• NEC• Typically seen in preemies• Timing of onset is generally inversely
proportional to gestational age at birth (e.g., the earlier a child is born, the later the signs of NEC are seen)
• Portions of the bowel undergo necrosis (tissue death)

NEC

NEC
• Tx includes providing bowel rest by stopping enteral feeds, gastric decompression with intermittent suction, fluid replacement, support for BP, parenteral nutrition, and abx therapy
• Emergency surgery resection of necrotic bowel may be required
• Colostomy may be required (reversed later)

NEC
•Warning – Picture of resection is next

NEC

NEC
• Almost never seen before oral feedings are introduced
• Formula feeding increases risk of NEC by tenfold compared to infants who are breastfed alone.
• Breastmilk (even expressed BM) – antiinfective effect, immunoglobulin agents, rapid digestion

Methicillin-resistant Staphylococcus aureus
• MRSA• A strain of staph that is resistant to broad
spectrum antibiotics• Can be fatal• Most MRSA infections occur in hospitals or
other health care settings (HA-MRSA = health care associated MRSA)

MRSA
• Recently another type has been found among otherwise healthy individuals in the community (CA-MRSA = Community associated MRSA)– Serious skin and soft tissue infections – Serious form of pneumonia

MRSA
• Staph bacteria normally found on skin and in nose of about 1/3 of the population
• If you have staph on your skin or in your nose and aren’t sick, you are said to be ‘colonized’ but not infected.
• You can pass the bacteria on to others, though.

MRSA
• MRSA infections start out as small red bumps that can quickly turn into painful abscesses

Kate…don’t look

MRSA• Staph are generally harmless unless they
enter the body through a cut or other wound• Risk factors:– Young age (not fully developed immune system)– Contact sports– Sharing towels or athletic equipment– Weakened immune system– Crowed, unsanitary living conditions– Health care

Kate…don’t look, again

MRSA• Prevention– Wash you hands/use alcohol sanitizer– Wash you hands often– Don’t share personal items– Shower after games/practices– Sit out games/practices if you have an infection– Sanitize linens (towels, sheets, etc.)– Get tested– Use antibiotics appropriately

Tracheoesophageal Fistula
• TEF• Abnormal connection (fistula) between the
esophagus and trachea.• Common congenital abnormality• In adults, usually sequela of surgical
procedure such a laryngectomy

TEF

Congenital TEF
• Type A – proximal and distal esophageal buds (esophageal agenesis = EA)
• Type B – Proximal esophageal termination in the lower trachea with distal esophageal bud (EA + TEF)
• Type C – Proximal esophageal atresia (esophagus ending in a blind loop) with distal esophagus arising from the lower trachea or carina. (EA + TEF) 90% of cases

Congenital TEF
• Type D – Proximal esophageal termination on the lower trach or carina with distal esoph arising from carina (EA + TEF)
• Type E (or Type H) – Variant of type D; if the two segments of esoph communicate, has a resemblance to the letter ‘H.’ (TEF without EA)

Congenital TEF

Congenital TEF
• Failed fusion of the tracheoesophageal ridges during the third week of embryological development
• Unable to feed safely• Prompt surgery is required• May develop feeding difficulties and chest
problems post-operatively

Congenital TEF
• Clinical presentation– Copious salivation– Choking, coughing, cyanosis with the onset of
feeding
• Treatment – Resection of fistula and anastomosis of
discontinuous segments– Complications• Structure, leak at point of anastomosis, recurrence

Congenital TEF
• Some babies with TEF also have other abnormalities
• Most commonly associated with VACTERL association

VACTERL or VATER Association
• Acronym used to describe a series of characteristics– V – vertebrae– A – imperforate anus or anal atresia– C – cardiac anomalies– TE – TEF– R – Renal or kidney anomalies– L – limb anomalies (radial agenesis)

VACTERL Association

VACTERL
• There is a wide range of manifestation so the exact incidence is unknown
• Babies usually have at least three or more individual anomalies
• 75% have heart disease (VSD, ASD, TOF)

Human respiratory syncytial virus• RSV– The major cause of lower respiratory tract
infection and hospital visits during infancy and childhood
– In US, 60% of infants infected during their first RSV season (usually winter months)
– Nearly all children have been infected by age 2-3 – Severe RSV infections have been increasingly
found among elderly patients

RSV
• Produces only mild symptoms in most people• Causes bronchiolitis leading to severe
respiratory illness requiring hospitalization and sometimes death (rare)
• Predisposes children to asthma/RAD

RSV

RSV• No known immunization• Infection does not induce protective immunity
so you can get it again• Synagis (palivizumab) – a moderately effective
prophylactic drug used for high risk infants (preemies, immuno suppressed, etc.)

Patent Ductus Arteriosus
• PDA• Before birth the two major arteries (aorta and
pulmonary artery) are connected by a blood vessel called the DA
• This vessel is an essential part of fetal blood circulation.
• DA mostly closes within 12-24 hours after birth and is completely sealed after three weeks

PDA
• If DA stays open (patent), it allows oxygen-rich blood from aorta to mix with oxygen-poor blood from the pulmonary artery.
• If uncorrected it may lead to congestive heart failure
•

PDA

PDA
• Typically found in preemies, congenital rubella syndrome and chromosomal abnormalities such as Down Syndrome
• Relatively common in US ~8:1000 births (preemies)
• In full-term (~2:1000 births)• Twice as common in girls

PDA
• Symptoms– Increased WOB, poor weight gain
• Treatment– Ligation – DA manually tied shut, plugs or coils– Indomethacin (inhibitor of prostaglandin)• Usually used with preemies

Ventricular Septal Defect
• VSD• Defect in the ventricular septum, the wall
dividing the left and right ventricles of the heart; a “hole” in the heart
• Causes a murmur that is audible to auscultation

VSD
• A large amount of oxygen-rich blood from heart’s left side is forced through the defect in to the right side. Then it’s pumped back to the lungs, even though it’s already been refreshed with oxygen.
• The already over-oxygenated blood displaces blood that needs oxygen. So the heart must pump more blood and may enlarge from all the work.

VSD

VSD
• Causes volume overload on the left ventricle leading to hypertension
• Usually manifests a few weeks after birth• Often closes on its own as heart grows
(childhood and adolescence)• Symptoms:– Breathlessness– Poor feeding– FTT

VSD
• If the opening is large, closing the hole in the first two years of life (patch or sewn together) is recommended to prevent serious problems later.
• Collectively, the most common congenital heart defect (2-6:100,000 births)
• 30-60% of all NB with a congenital heart defect

Tetralogy of Fallot
• TOF• Four key features– Pulmonary stenosis – Overriding aorta– VSD– Right ventricular hypertrophy
• An ASD or PFO is called a pentalogy of Fallot

TOF

TOF
• 400 per million live births• Males > females• ‘Tet spells’ – Sudden marked increase in cyanosis followed by
syncope; may result in hypoxic brain injury and death
– Older children squat, which cuts off circulation to the legs and improves blood flow to brain and vital organs

TOF
• Emergency management of tet spells– Beta blockers (propanolol)– Morphine – Ephinephrine
• Palliative surgery (shunt) then total surgical repair when older as required

TOF
• 90% of patients with total repair as infant develop progressively leaky pulm valve as heart grows to adult size but valve does not
• At risk for sudden cardiac death or heart failure.

Z-plasty
• Plastic surgery technique • Improves functional and cosmetic appearance
of scars• Can elongate a contracted scar or rotate the
scar tension line• Used in repair of cleft lip, palate and
ankyloglossia

Z-plasty

Z-plasty

That’s all folks!