Frequent Detection of bcl-2/JH Translocations in Human ... · To verify that the PCR products seen...
8
ICANCER RESEARCH55, 2876-2882, July 1, 19951 ABSTRACT Using an ultrasensitive assay involving the PCR, we have examined the frequency of a follicular lymphoma-assoclated translocation in peripheral blood from 132 individuals, most of whom were healthy blood donors. This translocation occurs between the bcl-2 proto-oncogene and the JH gene region and prolongs the life of lymphocytes. At a level of sensitivity of 1 translocation-bearing cell per 5 x 106cells, almost one-half of healthy human adults had this translocation in the mononuclear fraction of pe ripheral blood. However, the range of frequency of these translocations spanned almost three orders of magnitude among translocatlon-positive individuals. Furthermore, there was a statistically significant increase with age in the percentage of individuals who were translocation positive. Such an age correlation was also seen for the percentage of blood donors with rather high translocation frequencies (20 per Sx 106 peripheral blood mononuclear cells). However, the blood donor who had by far the highest concentration of this translocation was a healthy 35-year-old male containing —900 apparently monoclonal, translocation-bearing cells per 5 x 106 peripheral blood mononuclear cells. Our findings suggest that some individuals who may be at risk for fofficular lymphoma might be able to be identified by this PCR assay on peripheral blood. Also, these data may help explain the age dependence of the occurrence of this cancer. INTRODUCTION Many human cancers are associated with specific chromosomal rearrangements. For example, the t(14;18)(q32;q21) translocation, in which the downstream region of the bc!-2 proto-oncogene is joined to one of six â€oeH sequences in the immunoglobulin gene region, is found in up to 90% of follicular lymphomas and about 30% of diffuse large-cell lymphomas (1—3).The translocation junction in the bc!-2 gene region is most often located within about 150 bp of its untrans lated 3' terminus called the MBR3 (4, 5). The formation of this translocation, which results in overexpression of the rearranged bc!-2 gene region, may be a very early step in oncogenic transformation of lymphoblastoid cells. Constitutive expression of the bcl-2 gene inter feres with apoptosis in cells otherwise programmed to die, and, therefore, it extends the normal lifetime of these cells and increases their resistance to genotoxic agents (6—10).However, although the bcl-2/JH translocation is frequently detected in tumor cells of follic ular lymphomas, the consequent up-regulation of the bcl-2 gene does not suffice to induce tumor formation; rather, subsequent DNA alter ations in other cancer-associated genes seem to be necessary for tumor formation and progression (1 1, 12). Translocation-positive follicular lymphomas contain this chromo somal rearrangement in each cancer cell. At a copy number that was Received 2/7/95; accepted 5/3/95. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. I Supported in part by NIH Grant ES5946, Grant 91016019 from the U.S. Army Medical Research and Development Command, a grant from the Department of Defense through the Center for Bioenvironmental Studies at Tulane University, and developmental funds from the Tulane Cancer Center. 2 To whom requests for reprints should be addressed, at the Department of Biochem istry/SL43, Tulane Medical School, 1430 Tulane Avenue, New Orleans, LA 70112. 3 The abbreviations used are: MBR, major breakpoint region; PBM, peripheral blood mononuclear cells; bcl/J @, bcl-2/JH translocation-positive; CLL, chronic lymphocytic leukemia. orders of magnitude lower, this translocation was detected in a nonquan titative PCR assay on l-@g DNA samples from peripheral blood of almost one-half of patients with follicular lymphoma (13). This type of assay for the bc!-2/JH translocation at the MBR translocation hotspot of the bcl-2 gene uses primers from a @H sequence and from upstream of the MBR of the bc!-2 gene (14—17).Such tests revealed that even follicular lymphoma patients in remission often have PCR-detectable bc!-2IJH translocations in their peripheral blood-derived DNA (13, 18) and that one-third to one-halfofhyperplastic lymph nodes or tonsils of cancer-free individuals contained the bcl-2/JH translocation (19, 20). This percentage of translocation-positive individuals far exceeds the percentage of hu mans afflicted with follicular lymphoma (21). While the present study was under way, Liu et a!. (17) reported that about one-half of 53 hospital-derived blood samples showed evidence by PCR of the MBR-type bcl-2/JH translocation. Their assay allowed detection of a single translocation in DNA from about 10@mononuclear cells in peripheral blood. Although they did not define the medical status of the blood donors, their study indicated that there is an increase in the frequency of ‘@‘@@H translocations with the age of the donor. We report results from an examination of bcl-2/JH translocations in DNA from 132 blood donors, classified according to their health status, age, and gender. Using a directly quantitative PCR assay with a sensitivity of one bc!-2/JH translocation per 35 ,i.g of DNA (DNA from —SX 106 cells), we confirmed the findings of Liu et a!. (17) of an age dependence of the level of this translocation in blood cells and of the common occurrence of these translocations in the adult human population. However, we found that several apparently healthy mdi viduals in their twenties and thirties had very much higher levels of this translocation in their blood cells than most people. MATERIALS AND METHODS DNA Samples. Peripheral blood (2—5 ml) was obtained from 91 healthy blood donors, ages 18—82;8 sickle cell anemia patients, ages 6—16;24 patients, ages 51—89, with various diseases other than cancer; and 9 cancer patients. The latter were a 58-year-old (breast cancer), a 62-year-old (breast cancer), and a 70-year-old (lung cancer), as well as the 6 cancer patients listed in Tables 3 and 4. DNA was isolated from a mononuclear cell fraction of these blood samples (Ref. 22; Histopaque 1077; Sigma Chemical Co.) as well as from autopsy tissues as described previously (23). DNA concentrations were determined spectrophotometrically. Samples were checked for high molecular weight by agarose gel electrophoresis. Autopsy material was obtained during clinically mandated autopsies, and the blood samples were either from discard materials from medically necessary procedures or small leftover specimens from the analysis of the quality of blood donated by healthy individuals at a blood bank, as approved by the Tulane Institutional Review Board. PCR. Seminested PCR (Fig. 1A) was conducted with Taq polymerase as previously described using stringent precautions to prevent chemical contam ination (16). Unless otherwise specified, the primers used were: in the first round of PCR (24 cycles), primers 639, 5'-ACCTGAGGAGACGGTGACC 3', and 667, 5'-AGAAGTGACATCFTCAGCAAATAAAC-3'; and in the second round of PCR (22 cycles after a 1:20 dilution of the first-round product), primer 639 and 32P-labeledprimer 641, 5'-ACATTGATGGAATA ACTCFGTGG-3'. Where indicated, primer 700, 5'-TCCAGmAGAAT CAGCcTrG-3', or primer 781, 5'-TCAATG1TFAATGCFGTGQTTG-3', replaced primer 641. Usually, reactions were conducted in triplicate with two 14-pg aliquots and one 7-pg DNA aliquot per sample. For samples in which 2876 Frequent Detection of bcl-2/JH Translocations in Human Blood and Organ Samples by a Quantitative Polymerase Chain Reaction Assay' Weizhen Ji, Guang-zhi Qu, Peng Ye, Xian-Yang Zhang, Susan Halabi, and Melanie Ehrlich2 Tulane Cancer Center [W. J., X-Y. Z. S. H., M. E.J and Departments of Biochemistry 1W. J., G. Q., P. 1'., X-Y. Z, M. E.J and Biostatistics and Epidemiology [S. H.), Tulane Medical School. New Orleans, Louisiana 70112 Research. on November 14, 2020. © 1995 American Association for Cancer cancerres.aacrjournals.org Downloaded from
Transcript of Frequent Detection of bcl-2/JH Translocations in Human ... · To verify that the PCR products seen...

ICANCER RESEARCH55, 2876-2882, July 1, 19951
ABSTRACT
Using an ultrasensitive assay involving the PCR, we have examined thefrequency of a follicular lymphoma-assoclated translocation in peripheralblood from 132 individuals, most of whom were healthy blood donors.This translocation occurs between the bcl-2 proto-oncogene and the JHgene region and prolongs the life of lymphocytes. At a level of sensitivityof 1 translocation-bearing cell per 5 x 106cells, almost one-half of healthyhuman adults had this translocation in the mononuclear fraction of peripheral blood. However, the range of frequency of these translocationsspanned almost three orders of magnitude among translocatlon-positiveindividuals. Furthermore, there was a statistically significant increasewith age in the percentage of individuals who were translocation positive.Such an age correlation was also seen for the percentage of blood donorswith rather high translocation frequencies (20 per S x 106 peripheralblood mononuclear cells). However, the blood donor who had by far thehighest concentration of this translocation was a healthy 35-year-old malecontaining —900 apparently monoclonal, translocation-bearing cells per5 x 106 peripheral blood mononuclear cells. Our findings suggest thatsome individuals who may be at risk for fofficular lymphoma might beable to be identified by this PCR assay on peripheral blood. Also, thesedata may help explain the age dependence of the occurrence of this cancer.
INTRODUCTION
Many human cancers are associated with specific chromosomalrearrangements. For example, the t(14;18)(q32;q21) translocation, inwhich the downstream region of the bc!-2 proto-oncogene is joined toone of six “Hsequences in the immunoglobulin gene region, is foundin up to 90% of follicular lymphomas and about 30% of diffuselarge-cell lymphomas (1—3).The translocation junction in the bc!-2gene region is most often located within about 150 bp of its untranslated 3' terminus called the MBR3 (4, 5). The formation of thistranslocation, which results in overexpression of the rearranged bc!-2gene region, may be a very early step in oncogenic transformation oflymphoblastoid cells. Constitutive expression of the bcl-2 gene interferes with apoptosis in cells otherwise programmed to die, and,therefore, it extends the normal lifetime of these cells and increasestheir resistance to genotoxic agents (6—10).However, although thebcl-2/JH translocation is frequently detected in tumor cells of follicular lymphomas, the consequent up-regulation of the bcl-2 gene doesnot suffice to induce tumor formation; rather, subsequent DNA alterations in other cancer-associated genes seem to be necessary for tumorformation and progression (1 1, 12).
Translocation-positive follicular lymphomas contain this chromosomal rearrangement in each cancer cell. At a copy number that was
Received 2/7/95; accepted 5/3/95.The costs of publication of this article were defrayed in part by the payment of page
charges. This article must therefore be hereby marked advertisement in accordance with18 U.S.C. Section 1734 solely to indicate this fact.
I Supported in part by NIH Grant ES5946, Grant 91016019 from the U.S. Army
Medical Research and Development Command, a grant from the Department of Defensethrough the Center for Bioenvironmental Studies at Tulane University, and developmentalfunds from the Tulane Cancer Center.
2 To whom requests for reprints should be addressed, at the Department of Biochem
istry/SL43, Tulane Medical School, 1430 Tulane Avenue, New Orleans, LA 70112.3 The abbreviations used are: MBR, major breakpoint region; PBM, peripheral blood
mononuclear cells; bcl/J @,bcl-2/JH translocation-positive; CLL, chronic lymphocyticleukemia.
orders of magnitude lower, this translocation was detected in a nonquantitative PCR assay on l-@g DNA samples from peripheral blood ofalmost one-half of patients with follicular lymphoma (13). This type ofassay for the bc!-2/JH translocation at the MBR translocation hotspot ofthe bcl-2 gene uses primers from a @Hsequence and from upstream of theMBR of the bc!-2 gene (14—17).Such tests revealed that even follicularlymphoma patients in remission often have PCR-detectable bc!-2IJHtranslocations in their peripheral blood-derived DNA (13, 18) and thatone-third to one-halfofhyperplastic lymph nodes or tonsils of cancer-freeindividuals contained the bcl-2/JH translocation (19, 20). This percentageof translocation-positive individuals far exceeds the percentage of humans afflicted with follicular lymphoma (21).
While the present study was under way, Liu et a!. (17) reported thatabout one-half of 53 hospital-derived blood samples showed evidenceby PCR of the MBR-type bcl-2/JH translocation. Their assay alloweddetection of a single translocation in DNA from about 10@mononuclearcells in peripheral blood. Although they did not define the medical statusof the blood donors, their study indicated that there is an increase in thefrequency of ‘@‘@@Htranslocations with the age of the donor.
We report results from an examination of bcl-2/JH translocations inDNA from 132 blood donors, classified according to their healthstatus, age, and gender. Using a directly quantitative PCR assay witha sensitivity of one bc!-2/JH translocation per 35 ,i.g of DNA (DNAfrom —SX 106 cells), we confirmed the findings of Liu et a!. (17) ofan age dependence of the level of this translocation in blood cells andof the common occurrence of these translocations in the adult humanpopulation. However, we found that several apparently healthy mdividuals in their twenties and thirties had very much higher levels ofthis translocation in their blood cells than most people.
MATERIALS AND METHODS
DNA Samples. Peripheral blood (2—5ml) was obtained from 91 healthyblood donors, ages 18—82;8 sickle cell anemia patients, ages 6—16;24patients, ages 51—89, with various diseases other than cancer; and 9 cancer
patients. The latter were a 58-year-old (breast cancer), a 62-year-old (breastcancer), and a 70-year-old (lung cancer), as well as the 6 cancer patients listedin Tables 3 and 4. DNA was isolated from a mononuclear cell fraction of theseblood samples (Ref. 22; Histopaque 1077; Sigma Chemical Co.) as well asfrom autopsy tissues as described previously (23). DNA concentrations weredetermined spectrophotometrically. Samples were checked for high molecularweight by agarose gel electrophoresis. Autopsy material was obtained duringclinically mandated autopsies, and the blood samples were either from discardmaterials from medically necessary procedures or small leftover specimensfrom the analysis of the quality of blood donated by healthy individuals at ablood bank, as approved by the Tulane Institutional Review Board.
PCR. Seminested PCR (Fig. 1A) was conducted with Taq polymerase aspreviously described using stringent precautions to prevent chemical contamination (16). Unless otherwise specified, the primers used were: in the firstround of PCR (24 cycles), primers 639, 5'-ACCTGAGGAGACGGTGACC3', and 667, 5'-AGAAGTGACATCFTCAGCAAATAAAC-3'; and in thesecond round of PCR (22 cycles after a 1:20 dilution of the first-round
product), primer 639 and 32P-labeledprimer 641, 5'-ACATTGATGGAATAACTCFGTGG-3'. Where indicated, primer 700, 5'-TCCAGmAGAATCAGCcTrG-3', or primer 781, 5'-TCAATG1TFAATGCFGTGQTTG-3',replaced primer 641. Usually, reactions were conducted in triplicate with two14-pg aliquots and one 7-pg DNA aliquot per sample. For samples in which
2876
Frequent Detection of bcl-2/JH Translocations in Human Blood and Organ Samplesby a Quantitative Polymerase Chain Reaction Assay'
Weizhen Ji, Guang-zhi Qu, Peng Ye, Xian-Yang Zhang, Susan Halabi, and Melanie Ehrlich2
Tulane Cancer Center [W. J., X-Y. Z. S. H., M. E.J and Departments of Biochemistry 1W. J., G. Q., P. 1'., X-Y. Z, M. E.J and Biostatistics and Epidemiology [S. H.), TulaneMedical School. New Orleans, Louisiana 70112
Research. on November 14, 2020. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from

@;;;Vp/AJIJ2
J3J4J5@a4—639
667700641781L__@@;@-4-4 -9 -9
F@c
bcl-2/J@TRANSLOCATIONS IN BLOOD OF HEALTHY DONORS
AI bcl-2
667700641 781-+ -4 -@ -9 MBR
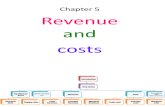
Fig. 1. Detection of @1VJHtranslocations byseminested PCR and analysis of the translocationjunctions in three translocation-positive DNA sampies fromthe bloodof healthyindividuals.A, therelative position of sequences complementary to theprimers (not drawn to scale) used for seminestedPCR to detect translocations between lad and theMBR at the end of the bcl-2 gene. Usually, in thefirst and second rounds of PCR (see “MaterialsandMethods―),primer pairs 667/639 and 641/639 wereused, respectively, with 32P-labeled primer 641 asthe source of radioactivity. Where indicated, primer641 was replaced with primers 700 or 781. In seminestedPCR,thesesetsofprimersyieldlabeledproducts only from the ‘@‘@@Htranslocation-bearingchromosome. Primer 639 is shown annealing to partof the 4,4 sequence, but this @Hconsensus sequenceprimer can anneal to any of the six @Hsequences. B.the DNAsequencesat thejunctionregionof PBMsamples 30 M, 70 M, and 55 F from Table 3. In thecase of the 55 F amplification products, 55 F a and55 F b refer, respectively, to the 880- and 720-bpPCR products that were separately sequenced.
chromosome 18
chromosome 14
t (14;18) chromosome
4,
4-
639
B
PBMSample bcl-2MBR Interveningregion
30M cTGcocTccTrococ
70 M ccTa*MTGDOTOGTOcT
PCCGATATATGGA TfrCTPCTPCGGTA1
CTC.CCCTTA&@TtGTT@GCTTATCTCCT1TCM@CTCTC
55 F a GTOGTATGMGCCGATP8CATAGTCCCTMCTGCG.MJCfrCG.1@M
55F b TODOTGGTGCT1A ATGfr@MCTGGTTtGt@
lGa&cfrcoG1tfrccG1@rcc1t J6
w@cTGGTcftGcmcTcc1t J4
T@GATGTCTGOGO@CMGGG@L3
cA.*ccxT0GTc.@mcTocTcJi
In the present study, most of the 132 blood samples, including allsamples from individuals between the ages of i8 and 50, came fromhealthy blood-bank donors, and the rest were from patients withdiseases other than lymphoma (see “Materials and Methods―). In
seminested PCR (Fig. 1A) on DNA from these blood samples, anyt(14;18) chromosomes whose translocations occurred between theMBR of the bcl-2 gene and one of the six @Hregions should giveamplification products of about 0.6- to 0.8-kb pairs. Even a singletranslocation-containing DNA molecule can be visualized in thisassay (16). Of the tested PBM samples, which contained a total of7—35I_Lgof DNA representing approximately i—SX 106 cells, 47%gave specific PCR products in the expected size range (bcl/J@ DNAsamples; Table 1; Fig. 2). The standard used in all PCR experimentswas DNA from SU-DHL-4, a diffuse histiocytic lymphoma-derivedcell line whose t(i4;i8) chromosome apparently contains a deletion ofseveral hundred bp in the MBR/JH4 junction region (4, i6). Uponseminested PCR, the translocation target sequence gives rise to an
—0.3-kb band instead of 0.6 to 0.8 kb (Fig. 2A, Lanes 9—ii) and,sometimes to a secondary higher-molecular-weight product (Fig. 14,Lane 11). This secondary band is probably due to the consensussequence @Hprimer, sometimes priming at @H5instead of @H4(27).
In all sets of PCR assays, control reactions were performed with ahuman brain DNA sample that contains no detectable bcl-2/JH translocations. These mixtures never gave a band in the 0.2- to 1.0-kbregion (Fig. 14, Lane 8; Fig. 3, Lanes 8, 16, and 24). Similarly, thePBM samples that showed no bands in the expected region fortranslocation products usually had no labeled bands at all (includingno nonspecific-labeled bands) after amplification (Fig. 14, Lanes 1—3,and 6; Fig. 2B, Lanes 7—10).
To verify that the PCR products seen in the bcl/J@ PBM sampleswere derived from the bcl-2/JH junction region, we replaced bcl-2primer 641 (Fig. IA) in the second round of PCR with primers 781 or700, which are —@80bp closer to or 30 bp further from the translocation breakpoints. From the standard SU-DHL-4 DNA, major labeledproducts of approximately 360, 330, and 250 bp were obtained afterthe second round of PCR with primers 700, 641, and 781, respectively(Fig. 3, Lanes 5, 6, 13, 14, 21, and 22). Fig. 3, Lanes 1—4,9—12,and17—20show that analogously amplified PBM DNA samples from fourindividuals had the predicted sizes (Fig. 3). Confirmation that thepositive samples contain in vivo-derived translocations is seen in theheterogeneity in the exact sizes of the specific amplification productsfrom different individuals (Fig. 28). This heterogeneity probably
2877
only limiting amounts of mononuclear blood cells were obtained, less DNAwas amplified as follows: for the 6—20-yeargroup (Table 1), two DNA samples of only 14 @gwere analyzed and one each of 21 and 28 @g;for the21—40-year group, five samples of 28 p@g;for the 41—60-year group, onesample each of 7 and 14 @g,three of 14 ,.@g, and two of 28 @g;for the
over-60-year group (including cancer patients), fourteen samples of 7 gig, four
of 14 g.@g,eight of 21 @g,and three of 28 [email protected] translocation-positivesamples containing less than 35 @.&gof DNA, the translocation frequency per 35I.Lg of DNA was derived by extrapolation. In each experiment, SU-DHL-4
DNA was used as a ‘@‘@@Htranslocation-positivestandard(24) in three reactionmixtures containing an average of 1, 2, or 4 molecules ofthis translocation plus 14,Lg of human brain DNA free of this translocation.To quantitate the bCI-2/JHtranslocation-containing DNA molecules in test samples, the intensity of theirspecific PCR product bands was compared to the intensity of an average of onetranslocationin the SU-DHL-4standard by phosphorimageranalysis A normalization factor was used to correct for the higher efficiency of amplification of the
latter, smaller PCR product (see “Resultsand Discussion―).Sequencing. DNA sequences at the translocation junction region were
determined by standard methods (Sequenase 2.0 kit; U.S. Biochemicals) usingthe following primer from the MBR: 5'-TFAGAGAGTfGClTIACGTGGCCTG-3'. The template DNASfor these reactions were PCR products obtainedwith unlabeled primers and purified on molecular sieve columns (SephacrylS-400; Promega) or, in the case of multiple bands from one sample, they wereseparated by PAGE and isolated by electroelution before sequencing as above.
Statistical Analysis. In assessing the relationship between age and translocation frequency, the Spearman's rank correlation coefficient was computed(25). In addition,@ tests for linearity and for testing the significance of theslope between age and translocation-positive status or between age and hightranslocation frequencies were performed (26).
RESULTS AND DISCUSSION
Detection of Very Low Levels of bcl-2/JH Translocations inHuman Blood. We used a highly sensitive PCR assay (Fig. IA) onDNA from PBM to detect lymphoma-associated translocations between the MBR, the breakage hotspot of the bcl-2 gene on chromosome 18, and the ‘Hregion on chromosome i4. This type of translocation had been shown previously to be present only in theB-lymphocyte fraction of peripheral blood (17), which constitutes—10—20%of PBM. B cells are expected to be the source of bcl-2/JHtranslocations because the DNA sequences (including N-type inserlions) at the junction points of these translocations from PBM, follicular lymphomas, pre-B cell leukemias, and hyperplastic tonsils mdicute that these translocations occur during B-cell differentiation (Refs.5, 6, 17, and 20 and see below).
Research. on November 14, 2020. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from

Table 1 Frequency of &1VJH translocations in differentagegroups'@%
of blood donors with the indicated no.ofNo.
oftranslocations
per 5 X 106 PBMb% of @/J@donorsdisplayingMultiple
@lVJHAge
group (yr)donors
inage groupNone1—19 20-495020
co@ies per bands per5 X 10 PBM 5 X 106PBMC6—20228614
000021—4043583057282841—60323850932060Over-602840―22
18146047Over-60Incl. cancer patients3540―23 20176238Total
md. cancer patients1325330 9835 40
‘@IVJH TRANSLOCATIONS IN BLOOD OF HEALTHY DONORS
a All subjects below the age of 51 were healthy blood-bank donors with the exception of 8 individuals from the ages of 5—16who had sickle cell anemia; the other 14 subjects in
the 6—20age group were healthy blood-bank donors between the ages of 18 and 20. None of the nine cancer patients had neoplasms associated with the bC!-2/JH translocation. Theother blood donors had non-cancer-related diseases (see “Materialsand Methods,―Fig. 5; Tables 3 and 4). bcl-2/J@, translocation-positive.
b The percentages of blood donors with the indicated @l@VJH@ frequencies or with no detectable bCI@2/JH translocations were determined by PCR on DNA from the
mononuclear cell fraction of peripheral blood as described in “Materialsand Methods.―Translocation frequency data for this table are derived from Fig. 5.C These @/J@ samples gave two or more bands of different electrophoretic mobility upon PCR indicative of multiple @1@2/@H translocations within an individual blood sample
(Tables 3 and 4; Fig. 4).d These numbers are probably overestimates because only 5 of 28 samples from the over-60 group excluding cancer patients and one of the 7 cancer patients over the age of 60
had enough DNA for the genomes from 5 X 106 cells to be analyzed (see “Materialsand Methods―).
reflects the position ofthe translocation breakpoint within the MBR atthe bc!-2 gene region, the presence of various N insertions and Dregion sequences at the breakpoint, and the exact @Hsequence at thebreakpoint (5, 20, 28). The DNA sequences at the breakpoint junctionof the PCR products from several PBM samples were determined
81 F 63M 70F 71F 82F 70F 35M StO Sti St2 St4*—‘_
kb
1.61
8:91
0.39
0.32
M 1 2 3 4 5 6 7 8 9 10 11
B
25M 71M 44F 41M 50F 20F 30F 21F 19F 28F 38F
(Fig. 1B). These junctions contained @Hsequences with extra basesthat may represent as yet unidentified D regions as well as N nucleotideadditions (20) that are characteristic of VDJ recombination occurring inpre-B cells (2). These sequences werejoined to MBR sequences from thebc!-2 gene (Fig. 1B). Therefore, we conclude that a large percentage ofnormal individuals have low levels of bcl-2JJH translocations in PBMbecause of abnormalities in immunoglobulin gene rearrangements.
Detection of bcl-2/JH Translocations in Various Organs. If thet(14;18) translocations are due to derangements in lymphocyte maturation, then spleen samples from autopsies would be expected to bean especially good source for this low-level chromosome rearrange
ment. As shown in Table 2, bc!-2/JH translocations were detected inspleen DNA from eight of nine subjects, none of whom had lymphomas. Four ofthese sets of autopsy samples came from individuals withcancer, two with gastric carcinoma, which has not been associatedwith bcl-2/JH translocations, one with breast cancer, and one withCLL. By Southern blot analysis, about 2% of CLL patients werefound to harbor this translocation throughout their tumor cells (29).All of the examined organ DNAS from the CLL autopsy samples
@ contained PCR-detectable bcl-2/JH translocations, a result that is,q'. consistentwiththepathologyfindingsof lymphocyteinfiltrationor
aggregation in these organs. The very low copy number in the nonhematopoietic organs in the autopsy specimens from the 55-year-oldmay be due to PBM contamination. None of the five analyzed placental DNA samples had detectable levels of this translocation. However, the PCR-amplified bc!-2JJH translocation product in the spleen of a2-month-old infant@who died of sudden infant death syndrome, indicatesthat cells with this translocation can be generated very early in life.
Quantitation of the Translocation Products. We previouslystudied, by Poisson and linear regression analyses, PCR productformation from different amounts of the translocation standard DNA,SU-DHL-4 DNA. These analyses showed that this assay has verygood reproducibility and linearity (16). In the present study, thereproducibility of this 46-cycle assay can also be seen by comparingthe intensity of PCR product bands from 14-pg duplicate DNAsamples (Tables 3 and 4). To use the SU-DHL-4 DNA as a quantitation standard for blood and organ DNA samples, we determined anormalization factor, i.e., the ratio of radioactivity in the —0.3-kbPCR product derived from one bcl-2/JH molecule in SU-DHL-4 DNAto that in an —0.7-kb PCR product from one bcl-2/JH molecule in asample DNA. This normalization factor is needed because of thehigher yield of PCR product expected when the target size is smaller.To calculate this factor, we used 10—20replicate PCRs on severaltranslocation-positive DNAS that we previously titrated by limiting
A
M I 2 3 4 5 6 7 8 9 10 11Fig. 2. Characterization of bcl-2JJH translocation-derived PCR products from blood
samples. Fourteen or 7 @gof PBM DNA from 18 individuals were amplified, and the PCRproducts were electrophoresed on a 6% polyacrylamide gel and visualized by autoradiography. The age and sex of each blood donor is indicated. A. Lanes 4. 5. and 7, and B, Lanes1—6,and I 1, translocation-positive (bcl/J@) PBM samples (quantitation of samples 71F,82F, 35M, and 25M is in Table 3). A, Lanes 1—3and 6, and B, Lanes 7—10,translocationnegative PBM samples. A, Lanes 9—11(Si!. St2, and Sf4), aliquots of a bcl/J@@SU-DHL-4 DNA, that should contain an average of 1, 2, or 4 molecules of the bCI@2/JHtranslocation; Lane 8 (StO), 14 p@gof human brain DNA alone, as a negative control,subjected to PCR in parallel to the PBM samples. The amplification experiment in A andthat in B were done with different batches of 32P-labeled primer; therefore, they are notcomparable. M. molecular weight DNA markers.
2878
g@@
Research. on November 14, 2020. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from

M12 3 4 56 7 8 9101112131415161718192021222324Fig. 3. Demonstration of the specificity of PCR products using alternative pairs of primers for amplifying the MBR-type bcl-2/JH translocation. Aliquots of the first-round PCR
products obtained with primers 639 (JH primer) and 667 (bcl-2 primer) from 14 g.@gof PBM DNA from healthy donors 28M, 27M. 35F, and 31F (Lanes 1—4, 9—12, and 17—20) were
amplified with the indicated set ofprimers in the second round of PCR. Lanes 5—8,13—16,and 21—24,the standards described in the legend to Fig. 2 were amplified with the indicatedprimers. That no band was seen in Lanes 7. 15, and 23, which contain the 1-copy bCI-2/JHstandard, reflects stochastic effects in taking the single aliquot of DNA for their commonfirst-round PCR mixture. M. molecular-weight markers; *, the radiolabeled primer used for PCR in the second round.
•0•
liver); and 1.3 (PBM, 35-year-old PBM). The average of 2.1 was used asthe normalization factor with the understanding that stochastic effects canaffect the very-low-copy-number determinations severalfold.
For the quantitation of bc!-2/JH molecules occurring at higherfrequencies, we extended the previous titration of the standard from amaximum of 15 to a maximum of 200 copies of the SU-DHL-4bc!-2/JH translocation per reaction mixture. Above 25 copies, theyield of the specific PCR product began to plateau, although up to 25copies, it was approximately linear (Ref. 16 and data not shown). Thisexplains the underestimated copy number of the 650-bp bc!-2/JHderived amplification product for the 14- and 7-p.g 35-year-old malePBM DNA @Table3). Limiting dilution analysis indicated that about900 copies of the bcl-2/JH translocation are present per 5 X 106 PBMin this individual (Table 3). Therefore, the observed level of translocation-containing molecules in bcl-2/JH translocation-positive PBMvaried from 1 to —900per 5 X 106 PBM, which, as described above,may be localized to the B-cell population and, therefore, this translo
_______________________ cation level in the target cell population may be about 10-fold higher.This can be compared with mean mutant frequencies in the human
Spleen Liver Kidney Lung hypoxanthine phosphoribosyltransferase gene of 25—50per 5 X 106 T
2 0 0 lymphocytes in normal adults, although the frequencies can be up to
0 0 100-fold higher in mutagen-exposed individuals (30). The hypoxan
15 thine phosphoribosyltransferase gene represents a large target for a
C diversesetof mutations,includingdeletionsapparentlymediatedby88 0 aberrant VDJ recombinase activity during embryogenesis (30), while
4 0 the breakpoints for the bcl-2/JH translocations that we are observing
5 with this PCR assay are usually localized within a few hundred bp.
48 0 0 Identification of PBM Samples with Multiple Independent
25 0 1 1 Translocations. In 40% of the bcl/J@ PBM DNA samples, two or
more closely spaced major product bands were seen (e.g., Fig. 4,11 8 30 6 Lanes 1—5). These are likely to be oligoclonal in origin and, thereby,
Placentas― derived from more than one independently arising bc!-2/JH translo
cation-containing cell. These multiple bands can be distinguishedespecially well in our study because of the use of a radiolabeledprimer to visualize the PCR products. Their specificity was confirmedfor nine of the PBM samples (Tables 3 and 4) by demonstrating thatwhen primer 781 was used for the second round of amplificationinstead of primer 641, the DNA fragments obtained were about 80 bpshorter, as expected. These samples were analyzed after treatment withnuclease Si, as well as without such treatment, and the multiple bandspersisted, indicating that they were not single-stranded products of PCR(Fig. 4). Furthermore, the junction points for the bc!-2IJH translocationsin the 720- and 880-bp bands of the 55-year-old female sample (Table 3)
ABCDE00000
bci-2/JH TRANSLOCATIONS IN BLOOD OF HEALThY DONORS
I 639/700• I U- 639/641* 639/781—
28M27M35F31FSt4S12 Sti Sb 28M27M35F31FSt4 St2 Sti StO28M27M35F31FSt4 St2Stl StOkb1.61 @‘
g@@
O@2@
o@e S0.32@
dilution analysis for their translocation frequency. From 75 amplification reactions containing an average of 1 bc!-2/JH chromosome perstarting mixture, we obtained the specific PCR product in 69% of theassays, in close agreement with the Poisson formula, which predicts63% positive reactions if the average target number is one. Theintensity of the radioactive signal in the specific product bandsshowed that the Poisson distribution was followed rather closely evenfor deducing the number of target molecules that were actually presentwithin each starting PCR mixture. From these experiments, we obtainedthe following ratios of intensities of bands amplified from 1 molecule of‘@‘@“Htranslocation in the spleen, liver, or PBM DNA compared to that
from 1 molecule in the SU-DFIL-4 DNA: 1.6, 1.8, 1.9 (spleen, 45-yearold female); 4.5, 2.9 (spleen, 23-year-old male); 0.9 (liver, 57-year-old
Causeof death
Sudden infant death syndrome
Unknown
Trauma
Trauma
Trauma
Gastric carcinoma
Gastric carcinoma
Breast cancer with lymph nodeinvolvement
72 M chronic lymphocytic leukemia
Table 2 PCR analysis oIDNA from various human organs for bcl-2/JH translocations―
No. of translocations per 5 X 106cells from the indicated organ
Organs from autopsy samplesSubject
Age and scx@'
2-month F
iF
23M
25M
41M
45 F
49M
55 F
a .@ translocation frequency was determined on triplicate samples as described in
“Materialsand Methods.―b The age is given in years unless otherwise indicated and the gender as F or M.cr@ sample, as well as the 41 M and 49 M spleen DNAS and the 72 M spleen, liver,
kidney, and lung DNA samples, gave two differently sized bcI-2fJ@-specificamplificationproducts in the 0.7- to 0.8-kb region, indicative of a biclonal origin. The 55 F spleen DNAsample had three bc1-2/J@-specific PCR products of different sizes in the 0.5- to 0.8-kbregion.
@iTranslocation frequencies are given for these DNA samples from five different
full-term human placentas(A-E), which had been rinsed to minimize excess blood beforeDNA isolation.
2879
- a@@
@.@
Research. on November 14, 2020. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from

Table 3 Peripheral blood samples displaying moderately high copy numbers ofbcl-2JJH translocations in PBM (20 bcl-2/JH translocations per 5 x IO@PBM)a
60 M 122 Metastatic renalcell carcinoma
62 F 158 Breast cancer69 M 116 Cardiovascular disease
and 61 M (ID #142)]. That these DNA products were not present ineach replicate reaction mixture is probably due to stochastic effects atvery low target numbers. In Tables 3 and 4 are nine PBM DNA
samples that appear to have three or four independent bcl-2/JH translocations. This sample number is probably an underestimate. Forexample, clonally diverse bcl-2/JH translocations in one DNA samplecould coelectrophorese due to the clustering of translocation breakpoints within the approximately 150-bp MBR at the end of the bcl-2gene (28). Also, we have not counted higher-molecular-weight bandsof lower intensity than the main band with size differentials that donot preclude their arising from alternative use of @Hsequences forprimer annealing during PCR. Furthermore, only MBR-localizedbcl-2/JH translocations are scored in this PCR assay and about 40% ofbcl-2/JH translocations in follicular lymphomas do not occur at thisregion of the bcl-2 gene (32). Despite these caveats, our data suggestthat the prevalence of individuals with multiple types of bcl-2/JHtranslocations may be one source of the higher-than-expected percentages of follicular lymphomas that are biclonal in origin (33).
Table 4 Peripheral blood samples displaying low copy-numbers 0/multiple types of‘@IVJHtranslocations (<20 translocations per 5 x 10°PBM@Age,
sex and Size of Copy nos. fromID no. of major 14, 14, and 7
donor Health status product(s) @sgDNACopy
no.per
5 X 106cells24M
47 Healthy 700 2,1,37805,3,31725
F 131 Healthy 760 2, 0, —8202,2,—833M
55b Healthy 620 1,2,1670 2,2,1720 1,1,18200,1,01341M
46 Healthy 730 0,2,07800,0,244SF
168 Healthy 625 0,0,37200,1,0447
F 132 Healthy 720 1, 1, 17900,1,0450F
77 Healthy 780 6,0,08500,4,01051
F 156 Rectal polyps 640 5, —,2690 0, —,41852
M 45 Healthy 700 6, 0, 17904,0,01154
M 30 Healthy 690 0, 2, 07601,2,3855
M 162 Alcoholic cirrhosis 620 2, 0, —of the liver 750 0, 1,—457
M 62 Healthy 750 3, 5, 010002,0,01061
M 142 Metastatic squamous 715 1, 0, 0carcinoma 750 0, 1,0261
M 1Mb Trauma 550 0, —,3610 1,—,06902,—,11270
F 148 Diverticulitis 730 —1, —,0760 0,—,4800 2,—,0840 0,—,215
Copy no.per
5 X 106cells
9759
22
22
900c
5032
31
30
2029
10014030
802529
37
150
50
4285
‘@‘@HTRANSLOCATIONS IN BLOOD OF HEALTHY DONORS
Age, sex, andID no. of
donor
25M 8129F 66b
Size ofmajor
product(s)
810660780900
700650800
1500
650705630670830
590720880
Copy nos. from14, 14, and 7
;sg DNA
35, 40, 2220, 11, 510, 6, 02, 0, 5
8, 11,34, 0, 40, 4, 06, 4, 0
>60, >60, >6015, —,159, 6, 36, 4, 02, 2, 0
2, 0, —
7, 7, —
3, 6, —
800685700 3,3,2780 10,9,3
685 28, —,20780760 13,5,—670 6,0,—
605 2,0,—670 9,10, —730 4,5,—
730
a In this table are listed all the bclJJ@ PBM samples which contained at least 20 bcl-2JJH
translocations per 5 X 106 cells. The determination of the approximate number of bcl-2J1Htranslocation-containing molecules per sample (copy no.) was performed on PBM fractions as described in “Materialsand Methods.―The copy number is given for each of threeidentically amplied DNA aliquots of 14, 14, and 7 @.tg,respectively, in the fifth columnand for the total 35 @.tgof DNA in the sixth column except where insufficient amounts ofDNA were present for all three determinations. —,not enough DNA was present toperform the indicated replicate determination. In the cases of samples with less than 35 @gof DNA (the amount of DNA from —5X 10'@cells), the approximate copy number for theamount of tested DNA was extrapolated to that expected for 35 @g.
b These samples were tested for the specificity of their PCR products by varying theprimer in the second round of PCR from primer 641 to 781 and by demonstrating theirresistance to SI nuclease as described in the text.
C For this one sample with an unusually high concentration of the translocation-containing
molecules,the copy number was determinedby limitingdilution analysis (see taxi).
were sequenced and were shown, as expected, to be nonidentical, indicating that they arose from independent translocation events (Fig. 1B).
The small size differentials, about 50 to 90 bp for most of the bandsappearing as doublets, precludes their arising by the use of alternative
@Hsequences for annealing to the @Hconsensus primer during PCR
because the number of residues between @Hsequences 1 through 6 inthe human genome is 210, 602, 373, 445, and 605 bp, respectively(31). In somecases,only onebandin thesizerangeexpectedforspecific translocation products was seen in each of duplicate amplification reactions, but the band in each duplicate mixture had aslightly different mobility [Table 4, samples 41 M, 45 F, 50 F, 55 M,
Health status
HealthyHealthy
30 M 33 Healthy34 M 61b Healthy
35 M 69 Healthy44 M 82 Healthy51 F 137 Healthy
55 F 161b Renal disease
700 6,—,—770 6,—,—
630760 11, 10, —830 3,0,—
70F llO@70F 14670M 36
GastritisBreast cancerHealthy
700 3,—,2780 8,—,12910 2, —,3
760 17,—,—
670
71 M 155 Ophthalmic infection71F 118 Lungcancer74 M 117b Atzheimer's disease
77 M 140b Spinal stenosis
77 F 154 Breast cancer and
brain metastasis
78 F 151b Cardiovasculardisease
82 F 1 19 Diabetes
89 F 149 Alzheimer's disease
a This table lists the translocation frequences for bC1/J@ samples which gave multiple
bands indicative of oligoclonality but which had <20 translocations per 5 X i($ PBM.The presence of different MBR-type bC1-2J1Htranslocations in a given PBM sample wasdetermined by looking for distinct-sized PCR products as described in the text. Analysisof the number of copies of the bCl@2/JHtranslocation-bearing DNA molecules andpresentation of the data are as for Table 3.
Th@ samples were tested for the specificity of their PCR products by varying the
primer in the second round of PCR from primer 641 to 781 and by demonstrating theirresistance to 51 nuclease as described in the text.
2880
Research. on November 14, 2020. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from

@a.
@‘2@'JHTRANSLOCATIONS IN BLOOD OF HEALTHY DONORS
55F 25F 47F 70F St4 correlation was not seenunlessthis outlier was excludedfrom theI 1 analysis. In addition to this 35-year-old male, two other healthy blood
kb donorslessthan40yearsof agehadratherhighlevelsof translocation-bearing PBM (Table 3, 25 M and 29 F). Therefore, much higherthan-normal levels of bcl-2/JH translocations in PBM of a smallportion of apparently cancer-free individuals is seen in younger adultsas well as in older adults, despite the general relationship betweentranslocation frequency and age.
1.61@ In addition,a significantcorrelationwasobservedbetweenthosedonors who had multiple-sized bcl-2IJH translocation products and age(Table 1; Spearman rank, r = 032; P < 0.001). That 3 of 43 peoplebetween the ages of 21 and 40 appear to have three or four independently
0 81 generatedbcl/J@PBMpopulationswhilethemajority(58%)ofthisage071 . grouphadnodetectabletranslocations(Tables3 and4)suggeststhat
. some individuals may be es@ally prone to generating or accumulating
multiple independently arising bcl-2IJH translocations. Furthermore,0.52@ individualswhoaremorelikelythannormaltorearrangetheir
bcl-2 and immunoglobulin gene loci might also be more likely togenerate cells with illegitimate recombination products involving
0.39 otherproto-oncogenesandsobealsoatriskforcertaintypesofcancer in addition to those associated with bcl-2/JH translocations.
032@ Withregardtothehealthstatusoftheblooddonors,allofthePBM. samples from individuals between the ages of 18 and 50 were from
volunteer blood donors, prescreened for good health. Most of theelderly blood donors were clinic patients with diseases other than
‘, I) 4 5 6 cancer (Tables 1, 3, and 4). Those cancer patients included in Table 1
M 1@@ andFig.S did nothavetypesof cancerassociatedwithbcl-2/JHtranslocations. The translocation data obtained from PBM of the smallnumber of over-60 nonlymphoma cancer patients (seven) were similarto the data obtained from the other over-60 donors (Table 1). We did
(900)
+. .+ + ++ :@*++ .: s$•+++:4+::.++,+@:.* : ‘:‘@:+@ :. ..++ •
Fig. 4. Examples of multiple PCR product bands obtained upon amplification ofindividual samples of PBM DNA. Lanes 1—5.samples from individuals 5SF, 25F, 47F,and 70F (nos. 161, 131, 132, and 148, respectively, in Table 3 or 4) were subject toseminested PCR under standard conditions, and then one-third of the reaction product wasdigestedwith 10 unitsof Si nucleasein a 35-s.dreactionmixtureat pH 4.5. That thelowestband was seen in one amplifiedaliquotof 5SF DNA(Lane 1) but not in theduplicate PCR reaction (Lane 2) probably reflects stochastic effects. Lane 6. an aliquot ofthe @,4(J@standard, which should have an average of four copies of the SU-DHL-4translocation, was amplified in parallel with the sample DNAS.The bands in this figurewere observed whether or not the samples were treated with SI nuclease. However, insome amplified DNA samples, we did see Si nuclease-sensitive bands, but these bandsalwayshad a lowermobilitythan i-kb DNAfragments,and usuallylowerthan 1.6-kbfragments, and were more diffuse and much less intense than those of the duplextranslocation-derived amplification products (see Fig. 2A, Lane 4).
analyze one sample from a patient with recurrent lymphoma, who wasnot currently showing signs of the disease. This individual had only 7bcl-2/JH translocations per S X 106 PBM and no evidence for multiple, independent translocations.
A higher percentage oftranslocation-positive adults were found amongmales than among females. The percentages of individuals who werebd/J@ in the 21—40,41—60,or over-60 age groups for males (M) versusfemales (F) were: M, 55% versus F, 29%; M, 71% versus F, 56%; and M,73% versus F, 54%, respectively. Furthermore, a similar gender differ
Analysis of the Translocation Frequency with Respect to Age,Gender, and Health Status ofthe Donors. Follicular lymphoma, thecancer most frequently associated with the bcl-2/JH translocation,usually occurs in people over the age of 60 and only rarely in thoseless than 40 (21). In this study, there was a statistically significantlinear trend in the proportion of translocation-positive blood donorswith age. The percentages of translocation-positive individuals in the6—20,21—40,41—60,and 61 age groups (including the nonlymphoma cancer patients) were 14, 42, 62, and 60%, respectively (Table1; x@2= 11.7; P < 0.01). Moreover, we observed a significant steadyincrease with age (x@2 = 14.2; P < 0.001) in the percentage ofindividuals having rather high translocation frequencies, i.e., 20translocations per 5 X 106 PBM (Tables 1 and 3), and this relationshipwas linear. This linear trend was also statistically significant when thenonlymphoma cancer patients or sickle cell patients were excluded.
The correlation between bcl-2/JH translocation frequency and theage of each blood donor (Fig. 5) was analyzed by the Spearman's rankcorrelation test as Liu et a!. (17) did in their study of 53 hospital blooddonors of uncharacterized disease status. We too observed a statistically significant increase with age (r = 0.37; P < 0.001; excluding thesickle cell patients, r = 0.25; P < 0.001). The Spearman rank correlation is not strongly affected by extreme values, such as that from the35-year-old male PBM sample (Table 3). In contrast, when analyzingthe data by Pearson's correlation test, a statistically significant linear
2881
900
150
0.
C0
@ 100C
‘ci
U)C0
@ 50@U0
U)CinC-I-
0 I@@ )@--
6 20 40 60 90
Age (years)
Fig. 5. Number of bcl-2/JH translocations per 5 x i0'@ mononuclear cells fromperipheral blood versus the age of the donor. The number of MBR-type bcl-2JJH translocations per 5 X 10―PBM (35 i.@gof DNA) is plotted versus the age of the blood donor(Table 1). For individuals with multiple types of bcl-2JJHtranslocations or high translocation frequencies, more information can be found in Tables 3 and 4. The off-scaletranslocation frequency of the 35-year-old male is indicated. +, healthy donor or noncancer patient; 0, cancer patient.
Research. on November 14, 2020. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from

@t@'@HTRANSLOCATIONS IN BLOOD OF HEALThY DONORS
6. Korsmeyer, S. J. Bcl-2 initiates a new category of oncogenes: regulators of cell death.Blood, 80: 879—886, 1992.
7. Veis, D. J., Sorenson, C. M., Shutter, J. R., and Korsmeyer, S. J. Bcl-2-deficient micedemonstrate fulminant lymphoid apoptosis, polycystic kidneys, and hypopigmentedhair. Cell, 75: 229—240, 1993.
8. Walton, M. I., Whysong, D., O'Connor, P. M., Hockenbery, D., Korsmeyer, S. J., andKohn, K. W. Constitutive expression of human bcl-2 modulates nitrogen mustard andcamptothecin induced apoptosis. Cancer Res., 53: 1853—1861,1993.
9. Strasser, A., Harris, A. W., Jacks, T., and Cory, S. DNA damage can induce apoptosisin proliferatinglymphoid cells via p53-independent mechanisms inhibitable by Bcl-2.Cell, 79: 329—339,1994.
10. McDonnell, T. J., and Korsmeyer, S. J. Progression from lymphoid hyperplasia tohigh-grade malignant lymphoma in mice transgenic for the t(14;I8). Nature (Land.),349: 254—256,1991.
11. Strasser, A., Harris, A. W., Bath, M. L., and Cory, S. Novel primitive lymphoidtumours induced in transgenic mice by cooperation between myc and bcl-2. Nature(Land.), 348: 331—333,1990.
12. Yano, T., Jaffe, E. S., Longo, D. L., and Raffeld, M. MYC rearrangements inhistologically progressed follicular lymphomas. Blood, 80: 758—767, 1992.
13. Soubeyran, P., Cabanillas, F., and Lee, M. S. Analysis ofthe expression ofthe hybridgene bcl-2/JgH in follicular lymphomas. Blood, 81: 122—127,1993.
14. Stetler-Stevenson, M., Raffeld, M., Cohen, P., and Cossman, J. Detection of occultfollicular lymphoma by specific DNA amplification. Blood, 72: 1822—1825,1988.
15. Lee, M-S., Chang, K-S., Cabanillas, F., Freireich, E. J., Trujillo, J. M., and Stass,S. A. Detection of minimal residual cells carrying the t(14;18) by DNA sequenceamplification. Science (Washington DC), 237: 175—178,1987.
16. Zhang, X-Y., and Ehrlich, M. Detection and quantitation of low numbers of chromosomes containing bcl-2 oncogene translocations using semi-nested PCR. Biotechniques, 16: 502—507,1994.
17. Uu, Y., Hemandez, A. M., Shibata, D., and Cortopassi, G. A. BCL2 translocationfrequencyrises with age in humans.Proc. Nad Acad. Sd. USA, 91: 8910-8914, 1994.
18. Price, C. G. A., Meerabux, J., Murtagh, S., Cotter, F. E., Rohatiner, A. Z. S., Young,B. D., and Lister, T. A. The significance of circulating cells carrying t(14;18) in longremission from follicular lymphoma. J. Clin. Oncol., 9: 1527—1532,1991.
19. Limpens, J., de Jong, D., van Krieken, J. H. J. M., Price, C. G. A., Young, B. D., vanOmmen, G-J. B., and Kluin, P. M. BCI-2/JHrearrangements in benign lymphoidtissues with follicular hyperplasia. Oncogene, 6: 2271—2276,1991.
20. Aster, J. C., Kobayashi, Y., Shiota, M., Mori, S., and Sklar, J. Detection of thet(14;18) at similar frequencies in hyperplastic lymphoid tissues from American andJapanese patients. Am. J. Pathol., 141: 291—299,1992.
21. Greiner, T. C., Medeiros, L 3., and Jaffe, E. S. Non-Hodgkin's lymphoma. Cancer(Phila.), 75 (Suppl. I): 370—380, 1995.
22. Boyum, A. Isolation of mononuclear cells and granulocytes. Scand. J. Gin. Lab.
Invest., 21 (Suppl. 97): 77—89,1968.23. Ehrlich, M., Gama-Sosa, M. A., Huang, L H, Midgett, R. M., Kuo, K. C., McCune,
R. A., and Gehrke, C. Amount and distribution of 5-methylcytosine in human DNAfrom different types of tissues or cells. Nucleic Acids Res., 10: 2709—2721, 1982.
24. Hecht, K-M. B., Epstein, A. L, Berger, C. S., Kaplan, H. S., and Hecht, F. Histiocyticlymphoma cell lines: immunologic and cytogenetic studies. Cancer Genet.Cytogenet., 14: 205—218,1985.
25. Conover, ‘N.J. Practical Nonparametric Statistics, Ed. 2. New York: John Wiley &Sons, 1980.
26. Fleiss, J. L. Statistical Methods for Rates and Proportions, Ed. 2. New York: JohnWiley & Sons, 1981.
27. Negrin, R. S., Kiem, H-P., Schmidt-Wolf, I. G. H., Blume, K. G., and a@, M. LUse of the polymerase chain reaction to monitor the effectiveness of cx vivo tumorcell purging. Blood, 77: 654—660, 1991.
28. Cotter, F. E., Price, C., Meerabux, J., Zucca, E., and Young, B. D. Direct sequenceanalysis of 14q+ and 18q—chromosome junctions at the MBR and MCR revealingclustering within the MBR in follicular lymphoma. Ann. Oncol. 2 (SuppL 2): 93—97,1991.
29. Dyer, M. J. S., Zani, V. J., Lu, W. Z., O'Byrne, A., Mould, S., Chapman, R., Heward,J. M., Kayano, H., Jadayel, D., Matutes, E., Catovsky, D., and Oscier, D. 0. BCL2translocations in leukemias of mature B cells. Blood, 83: 3682—3688,1994.
30. Fuscoe, J. C., Zimmerman, L J., Lippert, M. J., Nicklas, J. A., O'Neill, J. P., andAlbertini, R. J. V(D)J recombinase-like activity mediates hprt gene deletion in humanfetal T-lymphocytes. Cancer Rca., 51: 6001—6005,1991.
31. Ravetch, J. V., Siebenlist, U., Korsmeyer, S., Waldmann, T., and L.eder, P. Structureof the human immunoglobulin@ locus: characterization of embryonic and rearrangedJ and D genes. Cell, 27: 583—591,1981.
32. Cleary, M. L., and Sldar, J. Nucleotide sequence of a t(14;18) chromosomal breakpoint in follicular lymphoma and demonstration of a breakpoint-cluster region near atranscriptionally active locus on chromosome 18. Proc. NatI. Acad. Sci. USA, 82:7439—7443,1985.
33. SkIar, J., Cleary, M. L, Thielemans, K., Gralow, J., Warnke, R., and Levy, R.Biclonal B-cell lymphoma. N. Engi. J. Med., 311: 20—27,1984.
34. Devesa, S. S., and Fears, T. Non-Hodgkin's lymphoma time trends: United States andinternational data. Cancer Res., 52 (SuppL 19): 5432s—5440s,1992.
35. Lipkowitz, S., Garry, V. F., and Kirsch, I. R. Interlocus V-J recombination measuresgenomic instability in agriculture workers at risk for lymphoid malignancies. Proc.NatI. Acad. Sd. USA, 89: 5301—5305, 1992.
36. Bell, D. A., Litt, Y., and Cortopassi, G. A. Occurrence of bcl-2 oncogene translocation with increased frequency in the peripheral blood of heavy smokers. 3. Natl.Cancer Inst., 87: 223—224,1995.
37. Borrebaack, C. A. K. Strategy for the production of human monoclonal antibodiesusing in vitro activated B cells. J. Immunol. Methods, 123: 157—165,1989.
2882
ence was observed for subjects with high translocation frequencies. The
percentages of individuals with 20 translocations per 5 X 10@PBM inthe 21—40,41—60,or over-60 age groups for males versus females wereas follows: M, 18% versus F, 5%; M, 14% versus F, 11%; and M, 46%versusF,33%,respectively.Althoughthenumbersof individualsstudiedhere were insufficient for achieving statistical significance, these resultssuggest that males are more prone to accumulating these translocationsthan females, which might be related to males having a higher rate ofnon-Hodgkin's lymphoma than females (34).
Implications of Our Findings. Follicular lymphomas or diffuselarge-cell lymphomas that progress to high-grade lymphomas areoften associated with bcl-2/JH translocations throughout the tumor (1).These cancers contribute towards the 19,000 deaths per year fromnon-Hodgkin's lymphoma in the U.S. (34). That approximately 43%of healthy blood donors had detectable bcl-2/JH translocations in theirperipheral blood cells indicates that the mere presence of such translocations is not a risk factor for follicular lymphoma. However, thelevel of these translocations in PBM from apparently healthy peoplevaried over almost three orders of magnitude with a general agedependence that may be one of the sources of the strong age dependence of the occurrence of follicular lymphomas.
Furthermore, our finding that 3 of 57 healthy blood donors of lessthan 40 years of age had more than 50 translocations per 5 X 106PBM suggests the existence of a subpopulation of adults at risk forfollicular lymphoma or diffuse large-cell lymphoma later in life.Because these cancers are rare before middle age (21), the possibilitythat these individuals already have occult lymphoma and, hence, ahigh translocation frequency in their PBM can be discounted. Instead,we hypothesize that environmental factors (35) predispose someadults before middle age to accumulating bcl-2/JH translocations inPBM due to aberrant immunoglobulin gene maturation, and this couldlead to cancer if certain other genetic changes occur in these cells.Evidence for heavy smoking being associated with an increase in thebcl-2/JH translocation frequency was reported recently (36). It re
mains to be determined whether those bcl-2/JH translocation-containing cells that we detected at high concentrations in peripheral blood ofsome healthy blood donors may have other cancer-associated DNAchanges. It is also unclear how the extraordinarily large expansion (cf37) of translocation-containing clones that we have noted in severalapparently cancer-free individuals has occurred.
ACKNOWLEDGMENTS
We are very grateful to William Weales of the Blood Center for SoutheastLouisiana; to Drs. John Krause and William Robichaux of the Department ofPathology at Tulane Medical School for generous help in obtaining blood andtissue samples; and to Dr. Roy Weiner of the Tulane Cancer Center and Dr.Kenneth Bost of the Department of Microbiology and Immunology at TulaneMedical School for helpful discussions of this study.
REFERENCES
1. Weiss, L. M., Warnke, R. A., Sklar, J., and Cleary, M. L. Molecular analysis of thet(14;18) chromosomal translocation in malignant lymphomas. N. Engl. J. Med., 317:1185—1189,1987.
2. Tsujimoto, Y., Gorham, J., Cossman, J., Jaffe, E., and Croce, C. M. The t(14;18)
chromosome translocations involved in B-cell neoplasms result from mistakes in VDJjoining. Science (washington DC), 229: 1390—1393, 1985.
3. Risdall, R., Hoppe, R. T., and Warnke, R. Non-Hodgkin's lymphoma: a study of theevolution of the disease based upon 92 autopsied cases. Cancer (Phila.), 44: 529—542,1979.
4. Cleary, M. L., Smith, S. D., and SkIar, J. Cloning and structural analysis of cDNAsfor bcl-2 and a hybrid bcl-2/immunoglobulin transcript resulting from the t(14;18)translocation. Cell, 47: 19—28,1986.
5. Bakhshi, A., Wright, J. J., Graninger, W., Seto, M., Owens, J., Cossman, J., Jensen,J. P., Goldman, P., and Korsmeyer, S. J. Mechanism of the t(14;18) chromosomaltranslocation: structural analysis of both derivative 14 and 18 reciprocal partners.Proc. Natl. Acad. Sci. USA, 84: 2396—2400, 1987.
Research. on November 14, 2020. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from

1995;55:2876-2882. Cancer Res Weizhen Ji, Guang-zhi Qu, Peng Ye, et al. Reaction Assayand Organ Samples by a Quantitative Polymerase Chain
Translocations in Human BloodHbcl-2/JFrequent Detection of
Updated version
http://cancerres.aacrjournals.org/content/55/13/2876
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/55/13/2876To request permission to re-use all or part of this article, use this link
Research. on November 14, 2020. © 1995 American Association for Cancercancerres.aacrjournals.org Downloaded from