Frequency of TPR-MET rearrangement in patients with gastric carcinoma and in first-degree relatives
6
Frequency of TPR-MET Rearrangement in Patients with Gastric Carcinoma and in First-Degree Relatives Jun Yu, M.D. 1,2 Stephan Miehlke, M.D. 1 Matthias P. A. Ebert, M.D. 2 Juliane Hoffmann, Ph.D. 2 Matthias Breidert, M.D. 1 Birgit Alpen, M.D. 1 Teresa Starzynska, M.D. 3 Manfred Stolte, Prof., M.D. 4 Peter Malfertheiner, Prof., M.D. 2 Ekkehard Bayerdo ¨ rffer, Prof., M.D. 1 1 Medical Department I, Gastroenterology, Hema- tology and Oncology, Technical University Hospital, Dresden, Germany. 2 Department of Gastroenterology, Hepatology, and Infectious Diseases, Otto-von Guericke University, Magdeburg, Germany. 3 Department of Gastroenterology, Pomeranian Medical Academy, Szczecin, Poland. 4 Institute for Pathology, Klinikum Bayreuth, Bay- reuth, Germany. Presented in part at the Meeting of the American Gastroenterology Association, Orlando, Florida, May 1999. Supported by the Deutsche Forschungsgemein- schaft (Eb 187/1-2) and Land Sachsen-Anhalt (2775A/0087H) (M.E.), and by an unrestricted re- search grant from Astra GmbH, Wedel, Germany (S.M.). Address for reprints: Stephan Miehlke, M.D., Med- ical Department I, Technical University Hospital, Fetscherstrasse 74, D-01307 Dresden, Germany. Received August 30, 1999; revision received De- cember 7, 1999; accepted December 7, 1999. BACKGROUND. The activation of the c-met protooncogene through a rearrange- ment has been detected previously in gastric carcinoma tissue and precancerous lesions. In the current study the authors analyzed the rearrangement of TPR-MET in gastric carcinoma patients and in first-degree relatives to evaluate the potential role and timepoint of this genetic alteration in the process of gastric carcinogenesis and its potential value in identifying those individuals with an increased risk of developing gastric carcinoma. METHODS. The presence of TPR-MET mRNA was determined in gastric tissue from 19 patients with gastric carcinoma and in the gastric mucosa of 18 first-degree relatives without gastric carcinoma and in the gastric mucosa of 18 first-degree relatives without gastric carcinoma using a nested reverse transcriptase-poly- merase chain reaction (RT-PCR) and Southern blot analysis. A 205-base pair (bp) cDNA fragment and a 70-bp cDNA fragment spanning the breakpoint were am- plified by nested PCR. Amplification products were hybridized with an oligonu- cleotide labeled at the 39-end with DIG-11-dUTP spanning the breakpoint using Southern blot analysis. The MNNG-HOS cell line served as a positive control. RESULTS. TPR-MET mRNA was detected in nine gastric carcinoma patients (47%). Among these patients, TPR-MET mRNA was present in the both tumor and tumor free tissues in 5 patients (26%), in the tumor tissue only in 2 patients (11%), and in the tumor free gastric mucosa only in 2 patients (11%). It is interesting to note that TPR-MET rearrangement also was detected in the gastric corpus mucosa of 1 first-degree relative (6%), but in none of the control subjects. CONCLUSIONS. The data from the current study indicate that TPR-MET activation may be an early event in gastric carcinogenesis and may be useful for the identi- fication of individuals with an increased risk of developing gastric carcinoma. Cancer 2000;88:1801– 6. © 2000 American Cancer Society. KEYWORDS: TPR-MET rearrangement, gastric carcinoma, Helicobacter pylori, c-met, gastritis. G astric carcinoma is one of most frequent cancers worldwide and the second most common cause of cancer-related death. From a clinical point of view, there is a need to elucidate the molecular mechanisms of gastric carcinogenesis to improve early detection, develop treatment, and, finally, predict prognosis. 1,2 Recent analysis has established a number of genetic alterations that take place in the process of gastric carcinogenesis. Alteration of oncogenes, such as the activation of the c-met protooncogene and the amplification of k-sam, are frequently found in gastric carcinoma. Furthermore, inactivation of the tumor suppressor gene p53 and the inactivation of mismatch repair genes, along with the presence of microsatellite instability, have been demonstrated. 3,4 Approximately 10% of gastric carcinoma patients show familial 1801 © 2000 American Cancer Society
Transcript of Frequency of TPR-MET rearrangement in patients with gastric carcinoma and in first-degree relatives

Frequency of TPR-MET Rearrangement in Patientswith Gastric Carcinoma and in First-Degree Relatives
Jun Yu, M.D.1,2
Stephan Miehlke, M.D.1
Matthias P. A. Ebert, M.D.2
Juliane Hoffmann, Ph.D.2
Matthias Breidert, M.D.1
Birgit Alpen, M.D.1
Teresa Starzynska, M.D.3
Manfred Stolte, Prof., M.D.4
Peter Malfertheiner, Prof., M.D.2
Ekkehard Bayerdorffer, Prof., M.D.1
1 Medical Department I, Gastroenterology, Hema-tology and Oncology, Technical University Hospital,Dresden, Germany.
2 Department of Gastroenterology, Hepatology, andInfectious Diseases, Otto-von Guericke University,Magdeburg, Germany.
3 Department of Gastroenterology, PomeranianMedical Academy, Szczecin, Poland.
4 Institute for Pathology, Klinikum Bayreuth, Bay-reuth, Germany.
Presented in part at the Meeting of the AmericanGastroenterology Association, Orlando, Florida,May 1999.
Supported by the Deutsche Forschungsgemein-schaft (Eb 187/1-2) and Land Sachsen-Anhalt(2775A/0087H) (M.E.), and by an unrestricted re-search grant from Astra GmbH, Wedel, Germany(S.M.).
Address for reprints: Stephan Miehlke, M.D., Med-ical Department I, Technical University Hospital,Fetscherstrasse 74, D-01307 Dresden, Germany.
Received August 30, 1999; revision received De-cember 7, 1999; accepted December 7, 1999.
BACKGROUND. The activation of the c-met protooncogene through a rearrange-
ment has been detected previously in gastric carcinoma tissue and precancerous
lesions. In the current study the authors analyzed the rearrangement of TPR-MET
in gastric carcinoma patients and in first-degree relatives to evaluate the potential
role and timepoint of this genetic alteration in the process of gastric carcinogenesis
and its potential value in identifying those individuals with an increased risk of
developing gastric carcinoma.
METHODS. The presence of TPR-MET mRNA was determined in gastric tissue from
19 patients with gastric carcinoma and in the gastric mucosa of 18 first-degree
relatives without gastric carcinoma and in the gastric mucosa of 18 first-degree
relatives without gastric carcinoma using a nested reverse transcriptase-poly-
merase chain reaction (RT-PCR) and Southern blot analysis. A 205-base pair (bp)
cDNA fragment and a 70-bp cDNA fragment spanning the breakpoint were am-
plified by nested PCR. Amplification products were hybridized with an oligonu-
cleotide labeled at the 39-end with DIG-11-dUTP spanning the breakpoint using
Southern blot analysis. The MNNG-HOS cell line served as a positive control.
RESULTS. TPR-MET mRNA was detected in nine gastric carcinoma patients (47%).
Among these patients, TPR-MET mRNA was present in the both tumor and tumor
free tissues in 5 patients (26%), in the tumor tissue only in 2 patients (11%), and in
the tumor free gastric mucosa only in 2 patients (11%). It is interesting to note that
TPR-MET rearrangement also was detected in the gastric corpus mucosa of 1
first-degree relative (6%), but in none of the control subjects.
CONCLUSIONS. The data from the current study indicate that TPR-MET activation
may be an early event in gastric carcinogenesis and may be useful for the identi-
fication of individuals with an increased risk of developing gastric carcinoma.
Cancer 2000;88:1801– 6. © 2000 American Cancer Society.
KEYWORDS: TPR-MET rearrangement, gastric carcinoma, Helicobacter pylori, c-met,gastritis.
Gastric carcinoma is one of most frequent cancers worldwide andthe second most common cause of cancer-related death. From a
clinical point of view, there is a need to elucidate the molecularmechanisms of gastric carcinogenesis to improve early detection,develop treatment, and, finally, predict prognosis.1,2 Recent analysishas established a number of genetic alterations that take place in theprocess of gastric carcinogenesis. Alteration of oncogenes, such as theactivation of the c-met protooncogene and the amplification of k-sam,are frequently found in gastric carcinoma. Furthermore, inactivationof the tumor suppressor gene p53 and the inactivation of mismatchrepair genes, along with the presence of microsatellite instability,have been demonstrated.3,4
Approximately 10% of gastric carcinoma patients show familial
1801
© 2000 American Cancer Society

clustering.5,6 One study reported a high prevalence ofintestinal metaplasia in patients with pernicious ane-mia and in first-degree relatives of patients with gas-tric carcinoma.7 Furthermore, in first-degree relativesof patients with gastric carcinoma, an increased rate ofcell proliferation of the gastric mucosa has been re-ported.8 However, little is known regarding geneticalterations in the stomach of first-degree relatives ofpatients with gastric carcinoma. Recently, Soman et al.found that a fusion product of TPR-MET is expressedin the human gastric mucosa in gastritis, intestinalmetaplasia, and gastric carcinoma.9 TPR-MET rear-rangement is caused by a fusion of a TPR (translocatedpromoter region) locus on chromosome 1 to the 59region of sequences derived from the MET locus onchromosome 7.10 The activated TPR-MET oncogeneencodes a 65-kilodalton (kD) fusion protein. In thecurrent study, we analyzed the rearrangement of theTPR-MET oncogene in gastric carcinoma patients andfirst-degree relatives as well as normal subjects toassess the role of this genetic alteration in the multi-step process of gastric carcinogenesis and its potentialrole as a marker for the identification of individualswith an increased risk of developing gastric carci-noma.
MATERIALS AND METHODSPatients and Tissue SamplesNineteen gastric carcinoma patients (10 males and 9females) with a mean age of 62 years (range, 35–73years), 18 first-degree relatives of gastric carcinomapatients without clinically relevant disease (4 malesand 14 females) with a mean age of 47 years (range,27– 65 years), and 8 healthy control subjects (5 malesand 4 females) with a mean age 45 years (range, 25– 61years) without a family history of gastric carcinomawere enrolled in this study. The first-degree relativesand control subjects were recruited during the Preven-tive Intervention Study on Neoplastic Changes of theStomach (PRISMA).11 In 9 of 19 gastric carcinomapatients, multiple tumor biopsies were obtained en-doscopically for histologic and molecular examina-tion. In addition, endoscopic biopsies (two from theantrum and two from the corpus mucosa) were takenas distant from the tumor as possible to ensure thetaking of tumor free tissue. In the 18 first-degree rel-atives and in the control subjects, biopsies for histol-ogy and molecular analysis were obtained from de-fined locations of the corpus and antral mucosaduring endoscopy.12 All endoscopic biopsies for his-tology and molecular analysis from each respectivesite were taken within direct vicinity to each other. In10 patients undergoing surgery for gastric carcinoma,surgical tissues were taken from the tumor itself and
the tumor free area located at least 8 cm from themargins of the tumor. All individual specimens formolecular analysis were placed in separate tubes andwere frozen immediately in liquid nitrogen for storageat 280 °C until use. Gastric carcinoma types wereclassified histologically as intestinal-type (n 5 9) anddiffuse-type (n 5 9) according to the Lauren system.13
Grading of gastritis and Helicobacter pylori coloniza-tion of the nontumouros gastric mucosa was per-formed according to the updated Sydney system.12
Detection of H. pylori infection was performed histo-logically by Warthin-Starry stain.
The study was approved by the Ethics Committeeof the Technical University Hospital of Dresden andinformed consent to participate in the study was ob-tained from all patients.
RNA IsolationTissue specimens were stored at 280 °C and homog-enized with an ultrasound homogenizer (Ultra-TurraxT25; Janke and Kunkel GmbH, Wedel, Germany) in thepresence of RNAzolB (CINNA/MRC, Cincinnati, OH)containing RNase inhibitors. Total RNA was extractedfrom frozen tissues by the acid-guanidinium/phenol-chloroform extraction method and was quantitated bymeasuring the optical density at A260 and separatedby gel electrophoresis.
Reverse Transcriptase-Polymerase Chain ReactionAnalysisOne microgram of total RNA was reverse transcribedusing dNTPs (1 mM), DTT (5 mM), reverse-transcrip-tion buffer (50 mM Tris-HCl [pH 8.3], 75 mM KCl, 3mM MgCl2, and 1 mM DTT), 20 u of RNasin, and 6 uof Superscript plus, which were added to a total vol-ume of 20 mL. After incubation at 37 °C for 1 hour, thereaction was terminated by incubating the mixture at95 °C for 10 minutes. Polymerase chain reaction (PCR)amplification of the cDNA was performed using prim-ers as previously published9: Ta (24-mer), 59-GAAC-CAATGAG-AGACTATCTCAAG-39; Mb (20-mer), 59-CC-GTTCTGAGATGAATTAGG-39; T2 (30-mer), 59-GCTC-AGGATCGCAATATTGCCATTCAGAGC-39; and M2 (30-mer), 59-TAGTTAGGA-TGGGGGACATGTCTGTCAG-AG-39. Primers Ta and T2 are complementary to se-quences of the (2) strand of TPR cDNA and primersMb and M2 are complementary to the (1) strand ofMet cDNA. Primer T2 and M2 were designed to am-plify a 205-base pair (bp) region of the TPR-MET cDNAcarrying the breakpoint, whereas primers Ta and Mbdelineate a short stretch of a 70-bp cDNA region span-ning the breakpoint. First, the cDNA was amplifiedusing primers T2 and M2, and a nested PCR reactionthen was performed using nested primers Ta and Mb.
1802 CANCER April 15, 2000 / Volume 88 / Number 8

The reaction mixture contained 100 ng of cDNA, 1 uTaq polymerase, 20 mM dNTPs, 50 mM MgCl, and 10pmol of each primer in 50 mL of PCR buffer (50 mMTris-HCl and 50 mM KCl [pH 8.4]). The reaction mix-ture was incubated for 6 minutes at 95 °C. The sampleswere denatured at 94 °C for 1 minute, annealed at60 °C for 1 minute, and then extended at 72 °C for 1.5minutes. Each cycle was repeated 40 times and wasextended at 72 °C for 7 minutes to allow annealing ofthe products and stored at 4 °C. Nested PCR wasperformed with internal primers Ta and Mb in a 50-mLreaction solution. Thirty-five reaction cycles at 94 °C (1minute), 42 °C (1 minute), and 72 °C (1.5 minutes)were performed, at the end of which the mixture wasincubated at 72 °C for an additional 7 minutes andthen stored at 4 °C. For the negative controls, all PCRreagents were included except cDNA. An MNNG-treated osteosarcoma cell line (MNNG HOS) served asthe positive control.14 All necessary precautions weretaken to avoid cross-contamination between samples.Processing of samples before and after the PCR pro-cedure was performed in separate rooms. Every PCRprocedure was performed in duplicate.
Southern Blot AnalysisThe PCR products were separated on 1.25% agarosegel. Gels were stained with ethidium bromide. TheDNA was denatured by soaking the gels in 0.4 N NaOHfor 20 minutes and then transferred for 24 hours to aHybond N1 nylon membrane using 0.4N NaOH as thetransfer medium. The membranes then were neutral-ized in 1 M 5 3 standard saline citrate, allowed toair-dry for 6 hours, and baked for 20 minutes at 80 °C.
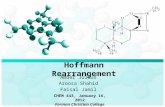
An oligonucleotide (59-GAACTTATGAATTGTCTAGT-39) spanning the breakpoint was labeled at the 39-endwith digoxigenin-ddUTP according to the manufac-turers’ recommendations (Boehringer MannheimGmbH, Indianapolis, IN). Hybridization for 24 hoursat 56 °C and washing conditions were performed ac-cording to the manufacturers’ recommendations. Theblots were exposed to Kodak films, (Eastman Kodak,Rochester, NY) at room temperature for 1.5 hours, 2hours, and 12 hours (Fig. 1).
Statistical AnalysisThe chi-square test was used to determine statisticaldifference, with P , 0.05 taken as the level of signifi-cance.15
RESULTSTPR-MET mRNA was detected in 9 of 19 gastric carci-noma patients (47%) (Table 1). Among these 19 pa-tients the fusion product of TPR-MET was present inthe tumor tissues of 7 patients (37%) and in the tumorfree gastric mucosa of 2 patients with intestinal-typegastric carcinoma (11%). In 5 of 19 gastric carcinomapatients (26%) TPR-MET rearrangement was observedin both tumor and tumor free gastric tissue. Amongthe nine patients with TPR-MET rearrangement in thetumor tissue, five had adenocarcinoma of intestinal-type and four had carcinoma of diffuse-type (Table 1).
One tumor exhibiting TPR-MET mRNA was clas-sified histologically as undifferentiated carcinoma. Nosignificant difference was found between diffuse andintestinal types of gastric carcinoma (P . 0.05). Threeof the 19 patients had signet ring cell carcinoma that
FIGURE 1. (Upper panel) Ethidium
bromide staining of the TPR-MET cDNA
fragments obtained by polymerase chain
reaction (PCR) analysis. PCR products
were obtained from mRNA extracted
from gastric tissue specimens using Ta
and Mb primers. The presence of the
rearrangement was confirmed by South-
ern blot analysis (lower panel). An inter-
nal probe spanning the breakpoint was
end-labeled with digoxigenin and used
for Southern blot analysis. The autora-
diogram was developed after 2 hours of
exposure at room temperature. Lane C:
corpus mucosa; Lane A: antrum mu-
cosa; Lane T: tumor; 1: positive control
(MNNG-HOS cDNA); 2: negative control.
C5, A5, T5: Patient 5; C6, A6, T6: Patient
6; C7, A7, T7: Patient 7; C8: Relative 8.
TPR-MET Rearrangement in Gastric Carcinoma/Yu et al. 1803

showed TPR-MET rearrangement in the tumor tissue.In one of these three patients TPR-MET also was ex-pressed in the tumor free gastric mucosa.
Twelve of 19 gastric carcinoma patients were his-tologically H. pylori positive (63%). Among these, fivegastric carcinoma patients showed TPR-MET rear-rangement, three in both tumor and tumor free tissue,one in tumor tissue only, and one in tumor free tissueonly. Seven gastric carcinoma patients were H. pylorinegative (37%). Among these, four patients had TPR-MET rearrangement either in tumor or tumor freetissue. Thus, no statistically significant association be-tween TPR-MET rearrangement and H. pylori infec-tion was observed.
It is interesting to note that the rearrangement ofTPR-MET was detected in the corpus mucosa of 1 of18 first-degree relatives of patients with gastric carci-noma (5.6%), but in none of the control subjects (Fig.1). Eleven of 18 first-degree relatives had H. pylorigastritis. Among those, 6 individuals showed gastritisof the gastric carcinoma phenotype (55%) (i.e., gradeand activity of gastritis in the corpus equal to or higherthan that in the antrum). One of these 6 first-degreerelatives with gastric carcinoma phenotype gastritisshowed TPR-MET rearrangement in the corpus mu-cosa (17%). Seven individuals were H. pylori negative,five of whom had minimal to mild, chronic, but non-active gastritis, and two of whom had moderate gas-tritis with only mild activity without any history of
nonsteroidal antiinflammatory drug use nor any directproof of H. pylori infection.
DISCUSSIONThe TPR-MET oncogene originally was identified as anoncogene rearranged after treatment of an osteosar-coma cell line (HOS) with N-methy-N9-nitro-N-ni-trosoguanidine (MNNG).10,16 –18 This activation is theconsequence of a chromosomal rearrangement inwhich the region of the c-met gene encoding the ex-tracellular and transmembrane domains is replacedby the 59 region of an unrelated gene designatedTPR.19,20 The c-met protooncogene encodes a 190-kDprotein belonging to the family of tyrosine kinase re-ceptors. Hepatocyte growth factor (HGF) is the ligandof the c-met receptor and HGF/c-met plays an impor-tant role in the regulation of cell growth, shape, andcell migration. TPR-MET, the fusion molecule (65 kD),contains the tyrosine kinase domain of the c-met pro-tooncogene, and the TPR sequence is comprised ofthe constitutive promoter and an open reading frame,leading to the transformation of NIH 3T3 cells to aconstitutively expressed tyrosine kinase.16
Several observations suggest that c-met may play arole in gastric carcinogenesis. First, amplification withconcomitant overexpression of c-met has been de-scribed in a human gastric carcinoma cell line.21–24
Second, amplification and overexpression of c-met hasbeen reported to occur in up to 50% of gastric carci-
TABLE 1TPR-MET Rearrangement, Histologic Diagnosis, and Helicobacter Pylori Status in Gastric Carcinoma Patients
Patient no. Age (yrs) Gender Hp
TPR-MET rearrangement
Histology Lauren typeNontumor Tumor
1 65 F 1 2 2 Adenoca Diffuse2 69 M 1 2 2 Adenoca Diffuse3 71 M 1 2 2 Adenoca Intestinal4 55 M 1 1 1 Signet ring Diffuse5 69 M 1 1 1 Adenoca Diffuse6 62 F 2 1 1 Adenoca Intestinal7 73 M 2 1 1 Undifferentiated8 60 F 1 2 2 Signet ring Diffuse9 69 F 1 2 2 Adenoca Diffuse10 37 M 2 2 2 Adenoca Intestinal11 63 M 2 2 2 Adenoca Intestinal12 63 M 1 1 1 Adenoca Intestinal13 69 M 2 1 2 Adenoca Intestinal14 66 F 2 2 2 Signet ring Diffuse15 35 M 1 2 2 Signet ring Diffuse16 57 F 1 2 1 Signet ring Diffuse17 64 F 1 2 2 Adenoca Intestinal18 54 F 1 1 2 Adenoca Intestinal19 63 F 2 2 1 Signet ring Diffuse
Hp: Helicobacter pylori status; F: female; 1: positive; 2: negative; Adenoca: adenocarcinoma; M: male.
1804 CANCER April 15, 2000 / Volume 88 / Number 8

nomas,25–27 and the amplification of c-met also wasdetected in the adjacent normal gastric tissues.28
Third, the TPR-MET oncogenic rearrangement alsohas been found in intestinal metaplasia.9 In the cur-rent analysis seven patients exhibited TPR-MET in thegastric tumor. This is in keeping with previous studiesdemonstrating the presence of TPR-MET in gastriccarcinoma. In five of these seven gastric tumors TPR-MET mRNA also was present in the tumor free gastricmucosa, raising the possibility that this genetic alter-ation occurs at an early stage of gastric carcinogenesis.However, in two cases the rearrangement was de-tected only in the tumor free gastric mucosa, not inthe tumor itself. This may indicate that these tumors,which both were of the intestinal type, may havearisen from a sequence of different genetic alterationsthat did not include the TPR-MET rearrangement. Insummary, the rearrangement of the TPR-MET gene inthe tumor free mucosa of gastric carcinoma patientssuggests a possible role of this oncogene during theinitial stages of gastric carcinogenesis. This observa-tion is consistent with previous findings that TPR-MET mRNA is expressed in biopsy samples of humangastric mucosa in patients with both gastritis and in-testinal metaplasia.9
Recent studies have reported an increased risk fordeveloping gastric carcinoma in first-degree relativesof gastric carcinoma patients. Harper reported athreefold increased relative risk for first-degree rela-tives of gastric carcinoma patients.29 Furthermore, afamily history of gastric carcinoma has been reportedto occur in approximately 10 –15% of gastric carci-noma patients.7 In addition, potential precancerouslesions, such as intestinal metaplasia of the gastricmucosa, have been reported to be detected in 52% offirst-degree relatives of gastric carcinoma patients.30
In comparison with control patients, first-degree rel-atives of gastric carcinoma patients also exhibit in-creased mucosal proliferation.8 Therefore, first-degreerelatives of gastric carcinoma patients exhibit histo-morphologic changes in the gastric mucosa that maycarry an increased risk of developing the disease. Inthe current study, the TPR-MET rearrangement wasfound in 1 of 18 first-degree relatives of gastric carci-noma patients. It is interesting to note that, this rela-tive also showed gastritis of the gastric carcinomaphenotype.31,32 This may suggest that patients with astrong family history of gastric carcinoma may harborgenetic alterations in the gastric mucosa that mayprecede the development of gastric tumors. Becausethe TPR-MET rearrangement is present in a large pro-portion of patients with gastric carcinoma and absentin healthy volunteers, the presence of this geneticalteration may point to an increased cancer risk for the
individual with this mutation. Therefore, a close fol-low-up of these individuals may be recommended toexclude a possible malignant transformation of thegastric mucosa and to confirm the value of this rear-rangement as a marker for gastric carcinoma.
REFERENCES1. Fuchs CS, Mayer RJ. Gastric carcinoma. N Engl J Med 1995;
333:32– 41.2. Delchier JC, Ebert M, Malfertheiner P. Helicobacter pylori in
gastric lymphoma and carcinoma. Curr Opin Gastroenterol1998;14:41–5.
3. Tahara E, Semba M, Tahara H. Molecular biological obser-vations in gastric cancer. Semin Oncol 1996;23:307–15.
4. Wright PA, Quirke P, Attanoos R, Williams GT. Molecularpathology of gastric carcinoma: progress and prospects.Hum Pathol 1992;23:848 –59.
5. La Vecchia C, Negri E, Franceschi S, Gentile A. Family his-tory and the risk of stomach and colorectal cancer. Cancer1992;70:50 –5.
6. Zanghieri G, Di Gregorio C, Sacchetti C, Fante R, Sassatelli R,Cannizzo G, et al. Familial occurrence of gastric cancer inthe 2-year experience of a population-based registry. Cancer1990;66:2047–51.
7. Sipponen P, Seppala K, Varis K, Hjelt L, Ihamaki T, Kekki M,et al. Intestinal metaplasia with colonic-type sulphomucinsin the gastric mucosa: its association with gastric carcinoma.Acta Pathol Microbiol Scand 1980;88:217–24.
8. Meining A, Hackelsberger A, Daenecke C, Stolte M, Bayer-dorffer E, Ochsenkuhn T. Increased cell proliferation of thegastric mucosa in first-degree relatives of gastric carcinomapatients. Cancer 1998;83:876 – 81.
9. Soman NR, Correa P, Ruiz BA, Wogan GN. The TPR-METoncogenic rearrangement is present and expressed in hu-man gastric carcinoma and precursor lesions. Proc NatlAcad Sci USA 1991;88:4892– 6.
10. Park M, Dean M, Cooper CS, Schmidt M, O’Brien SJ, BlairDG, et al. Mechanism of met oncogene activation. Cell 1986;45:895–904.
11. Forman D. Lessons from ongoing intervention studies. In:Hunt RH, Tytgat GNJ, editors. Helicobacter pylori-basicmechanisms to clinical cure. Dordrecht: Kluwer AcademicPublishers, 1998:354 – 61.
12. Dixon MF, Genta RM, Yardley JH, Correa P. Classificationand grading of gastritis. The updated Sydney system. Inter-national Workshop on the Histopathology of Gastritis,Houston 1994. Am J Surg Pathol 1996;20:1161– 81.
13. Lauren P. The two histological main types of gastric carci-noma. An attempt at a histo-clinical classification. ActaPathol Microbiol Scand 1965;64:31– 49.
14. Michelin S, Daya-Grosjean L, Sureau F, Said S, Sarasin A,Suarez HG. Characterization of a c-met proto-oncogene ac-tivated in human xeroderma pigmentosum cells after treat-ment with N-methyl-N9-nitro-N-nitrosoguanidine (MNNG).Oncogene 1993;8:1983–91.
15. Siegel S. Nonparametric test for behavourial sciences. NewYork: McGraw-Hill, 1956.
16. Cooper CS, Park M, Blair DG, Tainsky MA, Huebner K, CroceCM, et al. Molecular cloning of a new transforming genefrom a chemically transformed human cell line. Nature1984;311:29 –33.
TPR-MET Rearrangement in Gastric Carcinoma/Yu et al. 1805

17. Chan AM, King HW, Tempest P, Deakin EA, Cooper CS,Brookes P. Primary structure of the met protein tyrosinekinase domain. Oncogene 1987;1:229 –33.
18. Park M, Dean M, Kaul K, Braun MJ, Gonda MA, VandeWoude G. Sequence of MET protooncogene cDNA has fea-tures characteristic of the tyrosine kinase family of growth-factor receptors. Proc Natl Acad Sci USA 1987;84:6379 – 83.
19. Dean M, Park M, Le Beau MM, Robins T, Diaz M, Rowley J,et al. The human met oncogene is related to the tyrosinekinase oncogenes. Nature 1985;318:385– 8.
20. Testa JR, Park M, Blair DG, Kalbakji A, Arden K, VandeWoude GF. Analysis by pulsed field gel electrophoresis re-veals complex rearrangements in two MET alleles in achemically-treated human cell line, MNNG-HOS. Oncogene1990;5:1565–71.
21. Giordano S, Ponzetto C, Di Renzo MF, Cooper CS, ComigliPM. Tyrosine kinase receptor indistinguishable from thec-met protein. Nature 1989;339:155– 6.
22. Kuniyasu H, Yasui W, Kitadai Y, Yokozaki H, Ito H, Tahara E.Frequent amplification of the c-met gene in scirrhous typestomach cancer. Biochem Biophys Res Commun 1992;189:227–32.
23. Kuniyasu H, Yasui W, Yokozaki H, Kitadai Y, Tahara E.Aberrant expression of c-met mRNA in human gastric car-cinomas. Int J Cancer 1993;55:72–5.
24. Rege-Cambrin G, Scaravaglio P, Carozzi F, Giordano S,Ponzetto C, Comoglio PM, et al. Karyotypic analysis of gas-tric carcinoma cell lines carrying an amplified c-met onco-gene. Cancer Genet Cytogenet 1992;64:170 –3.
25. Di Renzo MF, Narsimhan RP, Olivero M, Bretti S, GiordanoS, Medico E, et al. Expression of the Met/HGF receptor innormal and neoplastic human tissues. Oncogene 1991;6:1997–2003.
26. Tsugawa K, Yonemura Y, Hirono Y, Fushida S, Kaji M, MiwaK, et al. Amplification of the c-met, c-erB-2 and epidermalgrowth factor receptor gene in human gastric cancers: cor-relation to clinical features. Oncology 1998;55:475– 81.
27. Houldsworth J, Cordon-Cardo C, Ladanyi M, Kelsen DP,Chaganti RS. Gene amplification in gastric and esophagealadenocarcinomas. Cancer Res 1990;50:6417–22.
28. Wu CW, Li AFY, Chi CW, Chung WW, Liu TY, P’eng FK. Hepa-tocyte growth factor and Met/HGF receptors in patients withgastric adenocarcinoma. Oncol Rep 1998;5:817–22.
29. Harper PS. Hereditary and gastrointestinal tumours. ClinGastroenterol 1973;2:675–90.
30. Schuman BM, Salerno-Mele P, Ghironzi G, Jackson CE, MaCK, Spigolon G. Gastric cancer in San Marinese and theirfirst degree relatives in San Marino and the United States.Gastroscopic biopsy as an epidemiological tool. GastrointestEndosc 1987;33:224 – 6.
31. Meining A, Bayerdorffer E, Muller P, Miehlke S, Lehn N,Holzel D, et al. Gastric carcinoma risk index in patientsinfected with Helicobacter pylori. Virchows Arch 1998;432:311– 4.
32. Meining A, Bayerdorffer E, Stolte M. Helicobacter pylorigastritis of the gastric cancer phenotype in relatives of gas-tric carcinoma patients. Eur J Gastroenterol Hepatol 1999;11:717–20.
1806 CANCER April 15, 2000 / Volume 88 / Number 8