
Fractures of the proximal end of the humerus caused by convulsive seizures
2
108 Injury (1984) 16, 108-109 Printedin Great Britain Fractures of the proximal end of the humerus caused by convulsive seizures Bjarne Kristiansen and Steen Christensen Hvidovre Hospital Copenhagen, Denmark Summary Fractures due to convulsions are known to occur. The purpose of this study was to find the frequency of convulsive seizures as the cause of fractures of the proximal end of the humerus, which are the most common of these fractures. Of 278 cases admitted to the department, 2 per cent occurred after a seizure without other contributory causes. The manner of injury is discussed, and it is demonstrated that the diagnosis is often delayed. The importance of early reduction in cases with dislocation or displacement of the fracture is emphasized. INTRODUCTION VARIOUSfractures have been noted as a result of convul- sive seizures; they include fractures of the vertebras, pelvis, femoral neck and, most c.ommonly, the proximal end of the humerus (Hamsa and Bennett, 1939; Cumming, 1942; Shaw, 1971; Vastamfiki and Solonen, 1980; Din and Meggit, 1983). Mechanical damage may be the cause in unilateral cases of the latter, but convul- sions such as those occurring in a fit or in electric shock are the single most common cause of bilateral cases (Shaw, 1971; O'Flannagan, 1975). The purpose of the present study was to find the frequency of convulsive seizures as the cause of fractures of the proximal end of the humerus, to present these cases and to discuss how the injury occurs. MATERIALS AND METHODS During the years 1976 to 1983, 276 patients with 278 fractures of the proximal end of the humerus were admitted to the Department of Orthopaedic Surgery, Hvidovre Hospital, Copenhagen. The clinical and radio- logical records have been reviewed in order to classify the fractures as 'little displaced' (all fractures, regardless of the level and number of fracture lines, in which no segment is displaced more than 1.0 cm or is angulated more than 45 °) or 'displaced' (all others) after Neer (1970). In addition the causes, e.g. fall, road traffic accident or convulsion, were sought. RESULTS In all, five fractures (2 per cent) occurred after a convulsion, without suspicion of a fall as a contributory cause. In one of these patients both humeri were broken. Four of the five 'convulsive fractures' were displaced and had a serious prognosis (Neer, 1970) (Table I). CASE REPORTS Case 1 A 57-year-old epileptic man sustained a displaced, four- fragment proximal fracture in conjunction with an epileptic attack. The condition was diagnosed 5 days later and operative reduction and fixation were performed. The patient died from a myocardial infarction 5 months after the operation (Fig. 1). Case 2 A 77-year-old woman received an electric shock through her left hand. She was brought to the local hospital because of severe burns of the hand and the following day was transferred to the District Burns Department. Seven days after the seizure X-ray examination revealed a fracture of the surgical neck of the left humerus, including avulsion of the greater tuberosity. In addition, dislocation of the right shoulder with a fracture of the tuberosity was found. Closed reduction of the right shoulder joint failed and caused a fracture of the proximal part of the humerus. Open repositioning and fixation of the fracture were carried out. The patient had almost normal function of both shoulder joints 7 months after the accident. Table I. Classification and aetiological factors in 278 fractures of the proximal end of the humerus Aetiological factor Trauma Fall on Fall from Road traffic Fracture type same level a height accident Convulsion Little displacement 157 11 31 1 Displaced 26 26 22 4 Total 183 37 53
-
Upload
bjarne-kristiansen -
Category
Documents
-
view
213 -
download
0
Transcript of Fractures of the proximal end of the humerus caused by convulsive seizures

108 Injury (1984) 16, 108-109 Printedin Great Britain
Fractures of the proximal end of the humerus caused by convulsive seizures Bjarne Krist iansen and Steen Chr is tensen
Hvidovre Hosp i ta l Copenhagen, Denmark
Summary Fractures due to convulsions are known to occur. The purpose of this study was to find the frequency of convulsive seizures as the cause of fractures of the proximal end of the humerus, which are the most common of these fractures.
Of 278 cases admitted to the department, 2 per cent occurred after a seizure without other contributory causes. The manner of injury is discussed, and it is demonstrated that the diagnosis is often delayed. The importance of early reduction in cases with dislocation or displacement of the fracture is emphasized.
I N T R O D U C T I O N VARIOUS fractures have been noted as a result of convul- sive seizures; they include fractures of the vertebras, pelvis, femoral neck and, most c.ommonly, the proximal end of the humerus (Hamsa and Bennett, 1939; Cumming, 1942; Shaw, 1971; Vastamfiki and Solonen, 1980; Din and Meggit, 1983). Mechanical damage may be the cause in unilateral cases of the latter, but convul- sions such as those occurring in a fit or in electric shock are the single most common cause of bilateral cases (Shaw, 1971; O'Flannagan, 1975).
The purpose of the present study was to find the frequency of convulsive seizures as the cause of fractures of the proximal end of the humerus, to present these cases and to discuss how the injury occurs.
M A T E R I A L S A N D M E T H O D S During the years 1976 to 1983, 276 patients with 278 fractures of the proximal end of the humerus were admitted to the Department of Orthopaedic Surgery, Hvidovre Hospital, Copenhagen. The clinical and radio- logical records have been reviewed in order to classify the fractures as 'little displaced' (all fractures, regardless of
the level and number of fracture lines, in which no segment is displaced more than 1.0 cm or is angulated more than 45 °) or 'displaced' (all others) after Neer (1970). In addition the causes, e.g. fall, road traffic accident or convulsion, were sought.
R E S U L T S In all, five fractures (2 per cent) occurred after a convulsion, without suspicion of a fall as a contributory cause. In one of these patients both humeri were broken. Four of the five 'convulsive fractures' were displaced and had a serious prognosis (Neer, 1970) (Table I).
C A S E R E P O R T S
Case 1 A 57-year-old epileptic man sustained a displaced, four- fragment proximal fracture in conjunction with an epileptic attack. The condition was diagnosed 5 days later and operative reduction and fixation were performed. The patient died from a myocardial infarction 5 months after the operation (Fig. 1).
Case 2 A 77-year-old woman received an electric shock through her left hand. She was brought to the local hospital because of severe burns of the hand and the following day was transferred to the District Burns Department. Seven days after the seizure X-ray examination revealed a fracture of the surgical neck of the left humerus, including avulsion of the greater tuberosity. In addition, dislocation of the right shoulder with a fracture of the tuberosity was found. Closed reduction of the right shoulder joint failed and caused a fracture of the proximal part of the humerus. Open repositioning and fixation of the fracture were carried out. The patient had almost normal function of both shoulder joints 7 months after the accident.
Table I. Classification and aetiological factors in 278 fractures of the proximal end of the humerus
Aetiological factor
Trauma
Fall on Fall from Road traffic Fracture type same level a height accident Convulsion
Little displacement 157 11 31 1 Displaced 26 26 22 4 Total 183 37 53
Kristiansen and Christensen: Fractures of the proximal humerus
Fig. 1. Four-part displaced proximal fracture of the proximal humerus diagnosed 5 days after an epileptic attack.
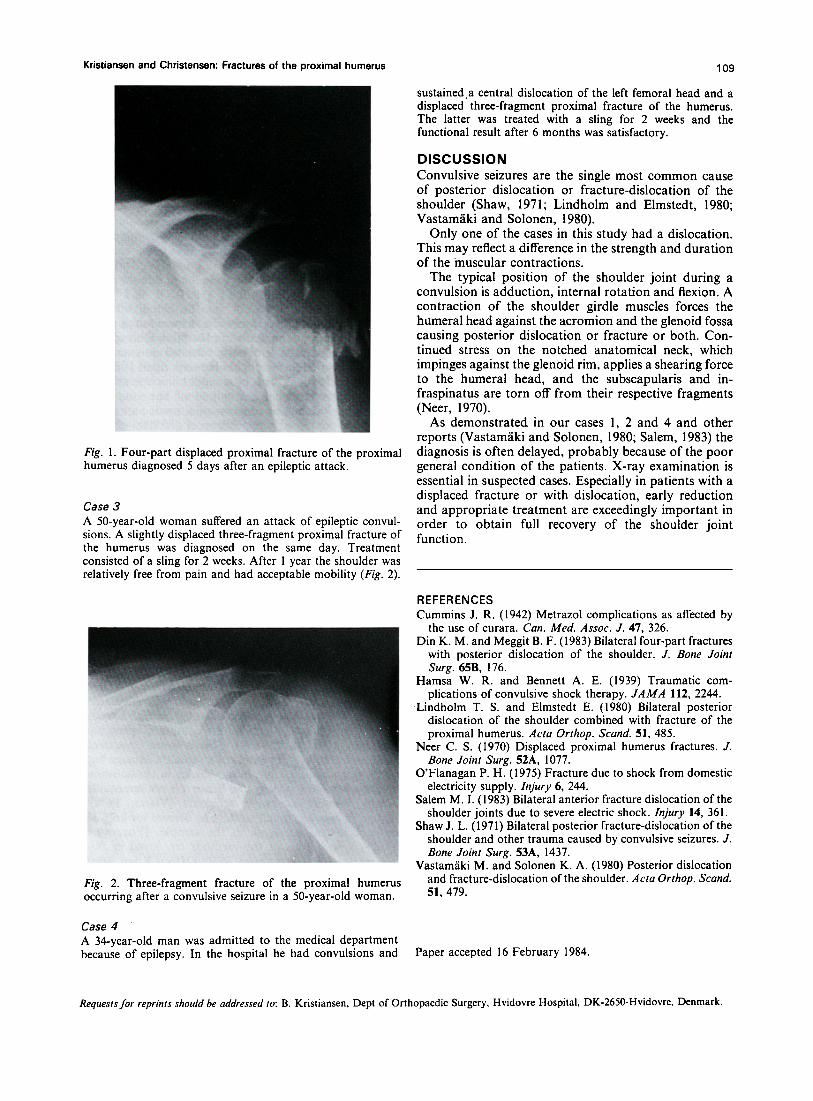
Case 3 A 50-year-old woman suffered an attack of epileptic convul- sions. A slightly displaced three-fragment proximal fracture of the humerus was diagnosed on the same day. Treatment consisted of a sling for 2 weeks. After 1 year the shoulder was relatively free from pain and had acceptable mobility (Fig. 2).
Fig. 2. Three-fragment fracture of the proximal humerus occurring after a convulsive seizure in a 50-year-old woman.
Case 4 A 34-year-old man was admitted to the medical department because of epilepsy. In the hospital he had convulsions and
109
sustained.a central dislocation of the left femoral head and a displaced three-fragment proximal fracture of the humerus. The latter was treated with a sling for 2 weeks and the functional result after 6 months was satisfactory.
DISCUSSION Convulsive seizures are the single most common cause of posterior dislocation or fracture-dislocation of the shoulder (Shaw, 1971; Lindholm and Elmstedt, 1980; Vastam~iki and Solonen, 1980).
Only one of the cases in this study had a dislocation. This may reflect a difference in the strength and duration of the muscular contractions.
The typical position of the shoulder joint during a convulsion is adduction, internal rotation and flexion. A contraction of the shoulder girdle muscles forces the humeral head against the acromion and the glenoid fossa causing posterior dislocation or fracture or both. Con- tinued stress on the notched anatomical neck, which impinges against the glenoid rim, applies a shearing force to the humeral head, and the subscapularis and in- fraspinatus are torn off from their respective fragments (Neer, 1970).
As demonstrated, in our cases 1, 2 and 4 and other reports (Vastam/iki and Solonen, 1980; Salem, 1983) the diagnosis is often delayed, probably because of the poor general condition of the patients. X-ray examination is essential in suspected cases. Especially in patients with a displaced fracture or with dislocation, early reduction and appropriate treatment are exceedingly important in order to obtain full recovery of the shoulder joint function.
REFERENCES Cummins J. R. (1942) Metrazol complications as affected by
the use of curara. Can. Med. Assoc. J. 47, 326. Din K. M. and Meggit B. F. (1983) Bilateral four-part fractures
with posterior dislocation of the shoulder. J. Bone Joint Surg. 65B, 176.
Hamsa W. R. and Bennett A. E. (1939) Traumatic com- plications of convulsive shock therapy. JAMA !12, 2244.
Lindholm T. S. and Elmstedt E. (1980) Bilateral posterior dislocation of the shoulder combined with fracture of the proximal humerus. Acta Orthop. Scand. 51,485.
Neer C. S. (1970) Displaced proximal humerus fractures. J. Bone Joint Surg. 52A, 1077.
O'Flanagan P. H. (1975) Fracture due to shock from domestic electricity supply. Injury 6, 244.
Salem M. I. (1983) Bilateral anterior fracture dislocation of the shoulder joints due to severe electric shock. Injury 14, 361.
Shaw J. L. (1971) Bilateral posterior fracture-dislocation of the shoulder and other trauma caused by convulsive seizures. J. Bone Joint Surg. 53A, 1437.
Vastam~iki M. and Solonen K. A. (1980) Posterior dislocation and fracture-dislocation of the shoulder. Acta Orthop. Scand. 51, 479.
Paper accepted 16 February 1984.
Requests for reprints should be addressed to: B. Kristiansen, Dept of Orthopaedic Surgery, Hvidovre Hospital, DK-2650-Hvidovre, Denmark.






![EPI 2: First-line anti-epileptic medication for management ... · [2015] EPI 2: First-line anti-epileptic medication for management of acute convulsive seizures, when intravenous](https://static.fdocuments.net/doc/165x107/5f23ded294c053128d4015d3/epi-2-first-line-anti-epileptic-medication-for-management-2015-epi-2-first-line.jpg)











