
FQHC Webinar Series Part 1 Telehealth and Chronic Care ......Medicare • CPT code 99453: Remote...
58
Welcome! FQHC Webinar Series Part 1 – Telehealth and Chronic Care Management
Transcript of FQHC Webinar Series Part 1 Telehealth and Chronic Care ......Medicare • CPT code 99453: Remote...

Welcome!FQHC Webinar Series Part 1 – Telehealth and Chronic Care Management

2
www.telehealthresourcecenter.org

▪ Your phone &/or computer microphone has been muted
▪ Time is reserved at the end for Q&A
▪ Q&A function is strictly text and chat formatting
▪ Please fill out the post-webinar survey
▪ Webinar is being recorded
▪ Recordings will be posted to our YouTube Channel:
https://www.youtube.com/c/nctrc
Webinar
Tips &
Notes

FQHC Series
This is only Part 1 of 3 in the NCTRC FQHC Webinar Series. Subscribe to our newsletter for more information.
Upcoming Topics:
• Substance Use Disorder (Date TBD)• Telemental and Behavioral Health (Date TBD)

RICHARD ALBRECHTDirector, Telehealth Network
Health Network HoldingsWallingford, CT
HOWARD CHAPMAN, JR.Director of Programs and
DevelopmentTri-Area Community Health
Laurel Fork, VA
KATHY WIBBERLYDirector
Mid-Atlantic Telehealth Resource Center
Charlottesville, VA
Presenters

Telehealth &
Chronic Care
ManagementServing Delaware, Kentucky, Maryland, New Jersey, North
Carolina, Pennsylvania, Virginia, Washington DC and West Virginia
NCTRC FQHC
Webinar Series
May 1, 2019

Medicare
What Is It?
Care coordination that is outside of the regular
office visit for patients with multiple (two or more)
chronic conditions expected to last at least 12
months or until the death of the patient, and
that place the patient at significant risk of death,
acute exacerbation or decompensation, or
functional decline. It can be delivered to people
with many different types of health conditions.

Medicare
Requirements
Summary Slide Courtesy of Shannon Chambers
Medicare
CPT Codes
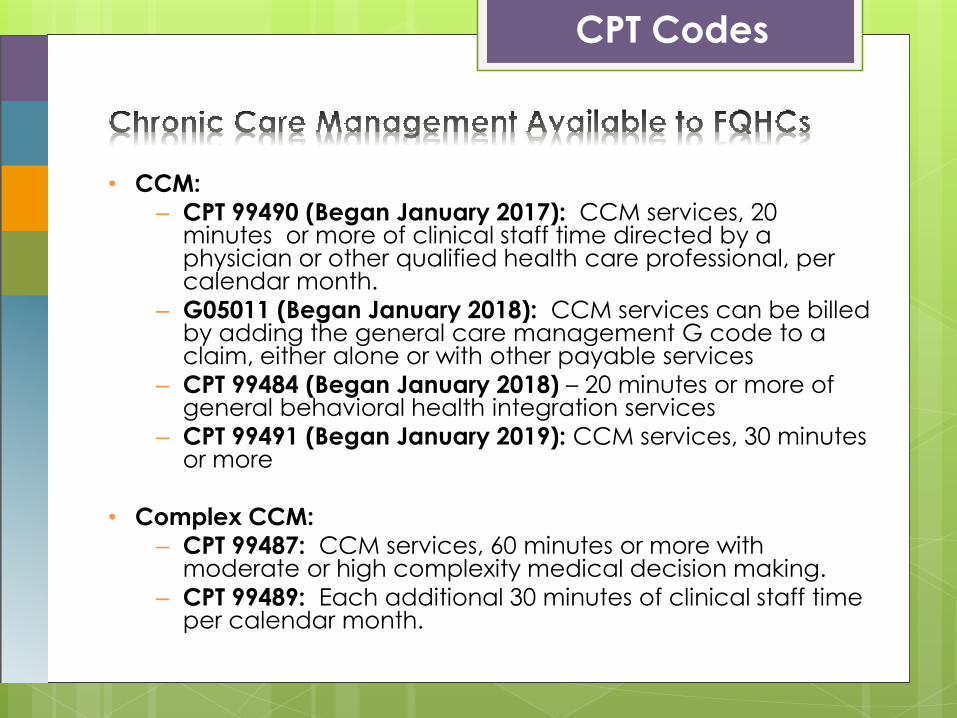
• CCM:
– CPT 99490 (Began January 2017): CCM services, 20 minutes or more of clinical staff time directed by a physician or other qualified health care professional, per calendar month.
– G05011 (Began January 2018): CCM services can be billed by adding the general care management G code to a claim, either alone or with other payable services
– CPT 99484 (Began January 2018) – 20 minutes or more of general behavioral health integration services
– CPT 99491 (Began January 2019): CCM services, 30 minutes or more
• Complex CCM:
– CPT 99487: CCM services, 60 minutes or more with moderate or high complexity medical decision making.
– CPT 99489: Each additional 30 minutes of clinical staff time per calendar month.

CCM

Medicare
• CPT code 99453: Remote monitoring of physiologic parameter(s) (eg, weight, blood pressure, pulse oximetry, respiratory flow rate), initial; set-up and patient education on use of equipment.
• CPT code 99454: Remote monitoring of physiologic parameter(s) (eg, weight, blood pressure, pulse oximetry, respiratory flow rate), initial; device(s) supply with daily recording(s) or programmed alert(s) transmission, each 30 days.
• CPT code 99457: Remote physiologic monitoring treatment management services, 20 minutes or more of clinical staff/physician/other qualified healthcare professional time in a calendar month requiring interactive communication with the patient/caregiver during the month.
– CMS is in the process of writing a technical correction so that the supervision level will be general supervision vs. direct supervision (incident to billing means direct supervision and requires the practitioner and clinical staff to be co-located)
Telehealth & CCM
Medicare
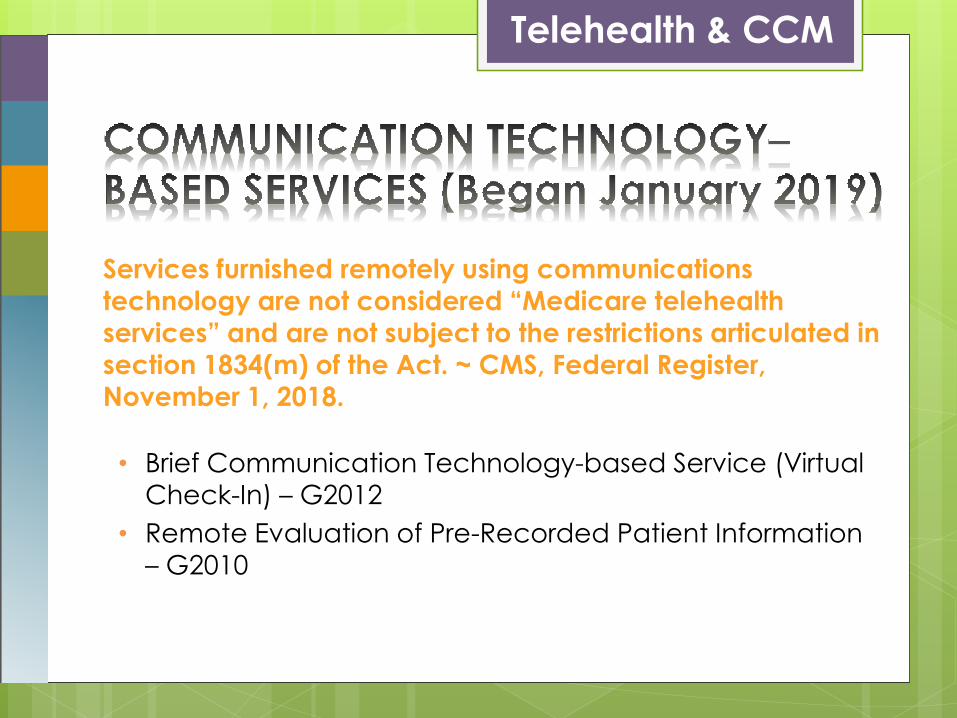
Services furnished remotely using communications
technology are not considered “Medicare telehealth services” and are not subject to the restrictions articulated in
section 1834(m) of the Act. ~ CMS, Federal Register,
November 1, 2018.
• Brief Communication Technology-based Service (Virtual
Check-In) – G2012
• Remote Evaluation of Pre-Recorded Patient Information
– G2010
Telehealth & CCM
Medicare
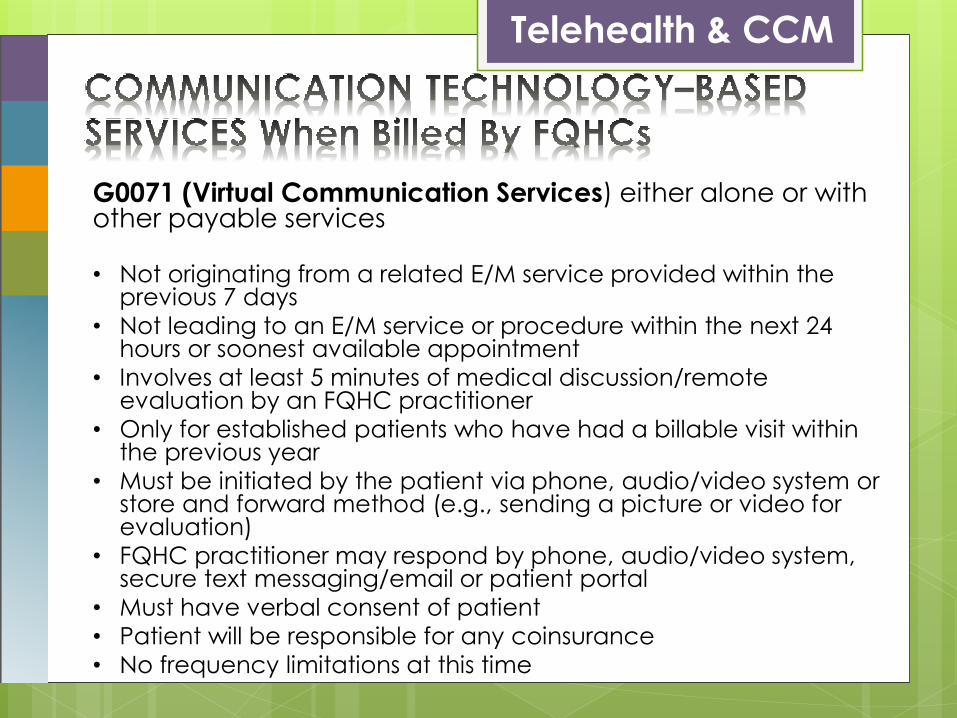
G0071 (Virtual Communication Services) either alone or with other payable services
• Not originating from a related E/M service provided within the previous 7 days
• Not leading to an E/M service or procedure within the next 24 hours or soonest available appointment
• Involves at least 5 minutes of medical discussion/remote evaluation by an FQHC practitioner
• Only for established patients who have had a billable visit within the previous year
• Must be initiated by the patient via phone, audio/video system or store and forward method (e.g., sending a picture or video for evaluation)
• FQHC practitioner may respond by phone, audio/video system, secure text messaging/email or patient portal
• Must have verbal consent of patient
• Patient will be responsible for any coinsurance
• No frequency limitations at this time
Telehealth & CCM
Medicare
Resources
• Connected Care Toolkit: Chronic Care Management
Resources for Health Care Professionals and Communities:
https://tinyurl.com/yxff5pc9
• Medicare Benefit Policy Manual: Chapter 13 – RHC and
FQHC Services Update: https://tinyurl.com/y4bmgvhc
• Care Management Services in RHCs and FQHCs –
Frequently Asked Questions: https://tinyurl.com/y4apcs9p
• Virtual Communication Services in RHCs and FQHCs –
Frequently Asked Questions: https://tinyurl.com/y22q3lm5
• Comparative Effectiveness Review - Telehealth for Acute
and Chronic Care Consultations:
https://tinyurl.com/y35k2rss

Contact
For More Information:
www.facebook.com/MATRC
www.MATRC.org

National Consortium of
Telehealth Resource Centers
Telehealth & Chronic Care
Management
Howard Chapman, Jr.
Director of Programs and Development
May 1, 2019
• Is a small three-site FQHC serving Carroll, Floyd, Franklin, and Patrick Counties in the Blue Ridge Mountains of Southwest of Virginia
• Tri-Area has two full-service retail pharmacies• It is part of the economically depressed Appalachian
Region• We serve around 10,000 patients with around 35,000
patient visits per year• Around 95 employees and 18 medical and behavioral
health providers• Tri-Area is NCQA Level III Recognized as a Patient
Centered Medical Home

Policies and Issues Affecting Telehealth
• Begin using Telemedicine/Telehealth in 2000
• We started with the UVA Office of Telemedicine
Access to 24 separate specialties
As a state supported medical school, UVA
provided services on a Sliding Fee Scale basis
We begin with an “incident to” consult code
(CMS stopped recognizing the code in 2005-2006)
Virginia Telemedicine Regulations
• Parity Law mandates equivalent coverage for telemedicine and in-person services from private payers, Medicaid, and state employee health plans
• State mandates reimbursement only on medical services provided via live video and provide limited coverage for other telehealth applications
• Tri-Area is paid for telemedicine services, even as a Distant Site by Medicaid and most commercial insurance
Issues
• Poor Connectivity and Broadband in rural Southwest Virginia
• Currently 50 mbs Laurel Fork site and 20 mbs at other sites and Corporate Office
• 2 Years ago 10 mbs Laurel Fork site, 6 mbs Floyd site, and 3 mbs Ferrum site and Corporate Office
• Competing with EMR, Practice Management System, email, and internet for bandwidth

Human and Technology Resources Required for Telehealth
• Camera, Monitor, Cart Set-Up Under $12,000 (18 years ago around $75,000)
• Good Connectivity (25 mbs or greater)
• Secure Network to maintain HIPAA Requirements
• Trained Staff (Certification Programs like STAR, UVA has a Certification Program)
• Provider Champion and support from Senior Management

Benefits to Community Health Centers
• Removes rural isolation for physicians and makes it easier to recruit and retain
• Compliance with Patient Centered Medical Home
• Improved Patient access to specialty care
• Improved Patient Compliance with Treatment Plans
• Improved Coordination of Care

Types of Telemedicine/Telehealth Used
Synchronous (live/real-time)
• Access to 24 Specialties through UVA
• UVA has a sliding fee program for our Virginia uninsured patients
• Provider and Staff CME
• Patient Education (Certified Diabetes Education Classes)
• Diabetes Quality Improvement Plan
Asynchronous (Store and Forward)
• X-Ray Interpretation through UVA Transferred electronically
Results the next day
STAT readings in emergencies
• Digital Retinopathy Screening Diabetic Screens for Patients
(40% reported first screening they had)
FDA approval for iPad and smart phone to get results within 20 minutes
• Cardiology
• Dermatology
• Endocrinology
• ENT
• Gastroenterology
• Gerontology
• Gynecology
• Hematology
• Hepatology
• Infectious Disease
• Nephrology
• Neurology
• Ophthalmology
• Orthopedics
• Pain Management
• Pediatrics
• Pediatric Cardiology
• Plastic Surgery
• Psychiatry
• Pulmonology
• Rheumatology
• Surgery
• TCV
• Urology

Diabetes Quality Improvement Program
• Focus on uncontrolled Diabetic Patients HbA1c of 8 or higher
• Endocrinologist follows them for 6 months with telemedicine and on-site at Tri-Area
• Coupled with the Certified Diabetes Education Classes and the Diabetic Retinopathy Screenings
• Uses home monitor to measure blood glucose, dietary intake, physical activity etc.
• Uploaded to smart phone and to a secure cloud server when the patient reaches Wi-Fi signal (not real-time)
• Graphs the data and can be accessed by the endocrinologist, the patient, Tri-Area providers, nurses, and case managers with secure password clearance

Two year data telemedicine diabetes
9.9±1.6 7.7±1.1
N=30
Design Interventions
Intense six month Self-Management component
Use of Project ECHO Educational Programs
Technology Components
Use of meal replacements
Cloud based Telcare meters
Glucomander-outpatient algorithmic insulin
decision making program

Deliverables of Program
• Reduction in glucose levels assessed by HbA1c
• Number of pounds and body weight loss
• Improvement in knowledge regarding diabetes based on pre- and post- testing questionnaire
• Absolute drop in blood pressure
• Improvement in the level of exercise

Problems
• Non-Compliance with number of glucose test requested per day
• Non-Compliance with diet
• Lack of motivation for better control
• Limitation of medications used based on financial situation
• Undercurrent Illness (UTI, URI, etc.)

Solutions
• Telephone Calls from Dr. Santen or the nurses encouraging proper testing (strips and Meter are at no cost to Patient)
• Nutrisystem D meal replacement (3 meals per day at no cost to the patient)
• Behavioral health consults and Diabetes Support Group with family members participation
• Medication Assistance Program, plus 340-B medications
• Prompt treatment by Tri-Area providers for undercurrent illness
Telehealth Resource Centers Thank You!
• Telehealth Resource Centers are an excellent resource for providing education to organizations and individuals interested in telemedicine/telehealth and other health technologies
• They link interested providers, health facilities, and programs to successful programs that are using telemedicine
• They provide technical assistance and arrange trainings to get programs up an running
Thank You! / Questions?
Contact Information:
Howard Chapman, Jr.
Director of Programs and Development Tri-Area Community Health
14168 Danville Pike / P. O. Box 9
Laurel Fork, VA 24352
Telephone: 276-398-2292 ext. 2221
Cell: 276-494-1143
Email: [email protected]
Chronic Care Management for FQHCs(And What We’ve Learned Over the Past 2 Years)
May 1, 2019


Our Agenda Today
• Who We Are
• Why We Were Interested
• Our Decision Process
• How We Implemented
• Lessons and Results
Health Network Holdings Inc. 35

What and Where is “Health Network Holdings”?
Why We Were Interested
Health Network Holdings Inc. 37

How CCM Benefits the Patient
Health Network Holdings Inc. 38
A regular check-in call by theirown care manager to assistwith any needs, provide coaching and support, and who will update the patient’s care team with any changes or concerns.
An up-to-date Care Plan with their current health goals.

How CCM Benefits Health Centers
Health Network Holdings Inc. 39
Clinical teams stay better connected with chronically ill patients.
Centers receive reimbursement for documented non-face-to-face care coordination activities.

Aligned with Our Strategic Goals
• More resources and outreach for patients who most need it
• Positive reimbursement for services already being provided
• Fully aligned with PCMH
Health Network Holdings Inc. 40

Our Decision Process
Health Network Holdings Inc. 41

Assessing the Opportunity / Cost
Health Network Holdings Inc. 42
General Chronic Care Management Financial Projections
2019 G0511 Rate: 67.03$ Actual net reimb.pp/pm $50.00
0.7 0.5 0.75 $67.03 75%
Estimated Number
of Medicare Pts.
Assume 75% of
patients with 2+
chronic
conditions
Assume 50%
Adoption Rate
Assume 75% of
patients meet the
monthly service
requirements
Potential
Monthly
Revenue
Potential Annual
Revenue
Assumed Annual
Cost of providing
CCM @ $50 per
billable patient
1,200 900 450 335 22,455$ 269,460$ 201,000$

CMS Requirements for CCM
Health Network Holdings Inc.43
Patient Provider
2 or more chronic conditions
Must use a certified EHRtechnology
24/7 access to care team for urgent needs
Serious health risk 20 minutes per patient per month of care coordination services
Care plan is updated as needed to remain current
Must consent to receive services, and consent is documented
Qualifying activity time must be documented: date, staff, description
Continuity of care with care team for successive routine appointments
May only consent with one provider at a time
Comprehensive patient-centered care plan congruent with patient’s goals and values
Care plan is created and managed within a technology platform
May have a co-pay Shared with patient Service period is one calendar month

The Next Most Important Questions
1. Does our organization have the capacity to take it on?
2. Do we have a senior clinical manager or team to lead it?
Health Network Holdings Inc. 44

• How to identify eligible patients and track enrollment requirements?
• How to create the protocols and processes for following up with patients with various chronic conditions?
• How to compliantly and efficiently manage and document services provided for 100s of patients?
CCM Implementation Challenges
• Who is going to train and manage the staff to enroll patients, create care plans and deliver services efficiently?
• Who will cover for sick days, vacation time, turnover, etc?
• Who is going to monitor patients in the program to ensure that enrolled patients receive the full scope of services?
DOCUMENTATION & TIME MGMT STAFFING & RESOURCES TO EXECUTE
Processes, Technology and Staff to Meet the CMS Requirements
Health Network Holdings Inc. 45
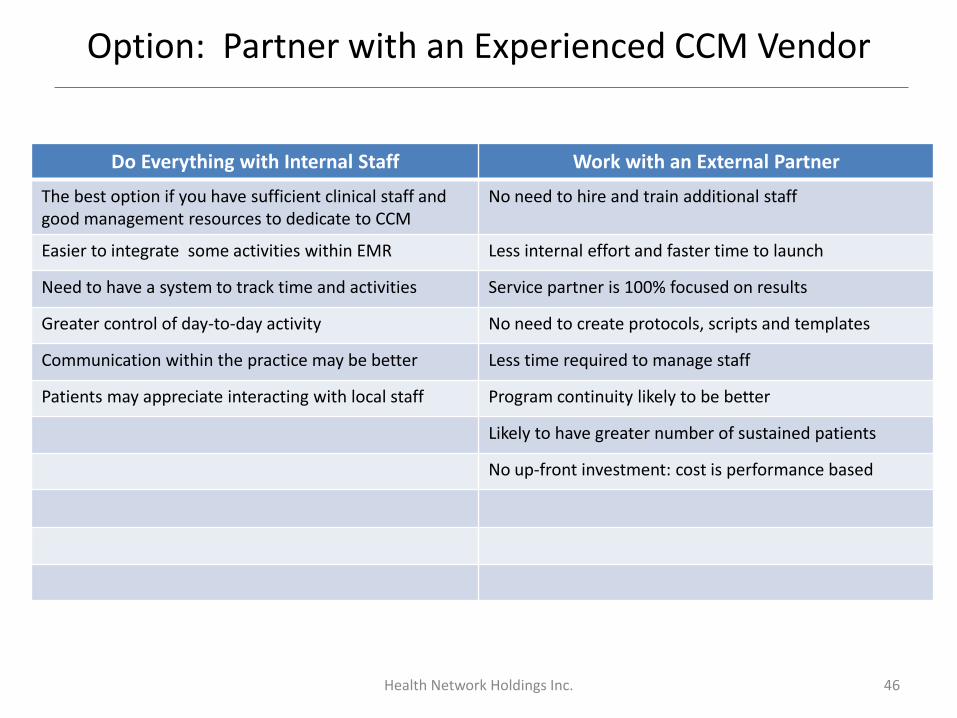
Option: Partner with an Experienced CCM Vendor
Do Everything with Internal Staff Work with an External Partner
The best option if you have sufficient clinical staff and good management resources to dedicate to CCM
No need to hire and train additional staff
Easier to integrate some activities within EMR Less internal effort and faster time to launch
Need to have a system to track time and activities Service partner is 100% focused on results
Greater control of day-to-day activity No need to create protocols, scripts and templates
Communication within the practice may be better Less time required to manage staff
Patients may appreciate interacting with local staff Program continuity likely to be better
Likely to have greater number of sustained patients
No up-front investment: cost is performance based
Health Network Holdings Inc. 46
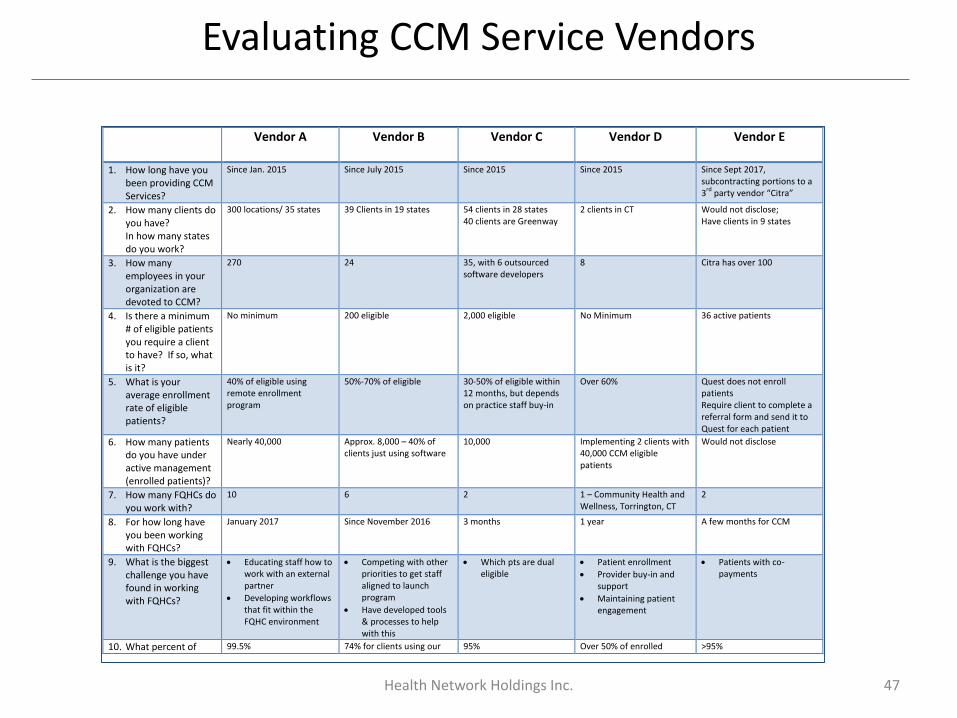
Evaluating CCM Service Vendors
Health Network Holdings Inc. 47
Vendor A Vendor B Vendor C Vendor D
Vendor E
1. How long have you been providing CCM Services?
Since Jan. 2015 Since July 2015 Since 2015 Since 2015 Since Sept 2017, subcontracting portions to a 3
rd party vendor “Citra”
2. How many clients do you have? In how many states do you work?
300 locations/ 35 states 39 Clients in 19 states 54 clients in 28 states 40 clients are Greenway
2 clients in CT Would not disclose; Have clients in 9 states
3. How many employees in your organization are devoted to CCM?
270 24 35, with 6 outsourced software developers
8 Citra has over 100
4. Is there a minimum # of eligible patients you require a client to have? If so, what is it?
No minimum 200 eligible 2,000 eligible No Minimum 36 active patients
5. What is your average enrollment rate of eligible patients?
40% of eligible using remote enrollment program
50%-70% of eligible 30-50% of eligible within 12 months, but depends on practice staff buy-in
Over 60% Quest does not enroll patients Require client to complete a referral form and send it to Quest for each patient
6. How many patients do you have under active management (enrolled patients)?
Nearly 40,000 Approx. 8,000 – 40% of clients just using software
10,000 Implementing 2 clients with 40,000 CCM eligible patients
Would not disclose
7. How many FQHCs do you work with?
10 6 2 1 – Community Health and Wellness, Torrington, CT
2
8. For how long have you been working with FQHCs?
January 2017 Since November 2016 3 months 1 year A few months for CCM
9. What is the biggest challenge you have found in working with FQHCs?
Educating staff how to work with an external partner
Developing workflows that fit within the FQHC environment
Competing with other priorities to get staff aligned to launch program
Have developed tools & processes to help with this
Which pts are dual eligible
Patient enrollment
Provider buy-in and support
Maintaining patient engagement
Patients with co-payments
10. What percent of 99.5% 74% for clients using our 95% Over 50% of enrolled >95%
How We Implemented
Health Network Holdings Inc. 48

Our Implementation Models
Health Network Holdings Inc. 49
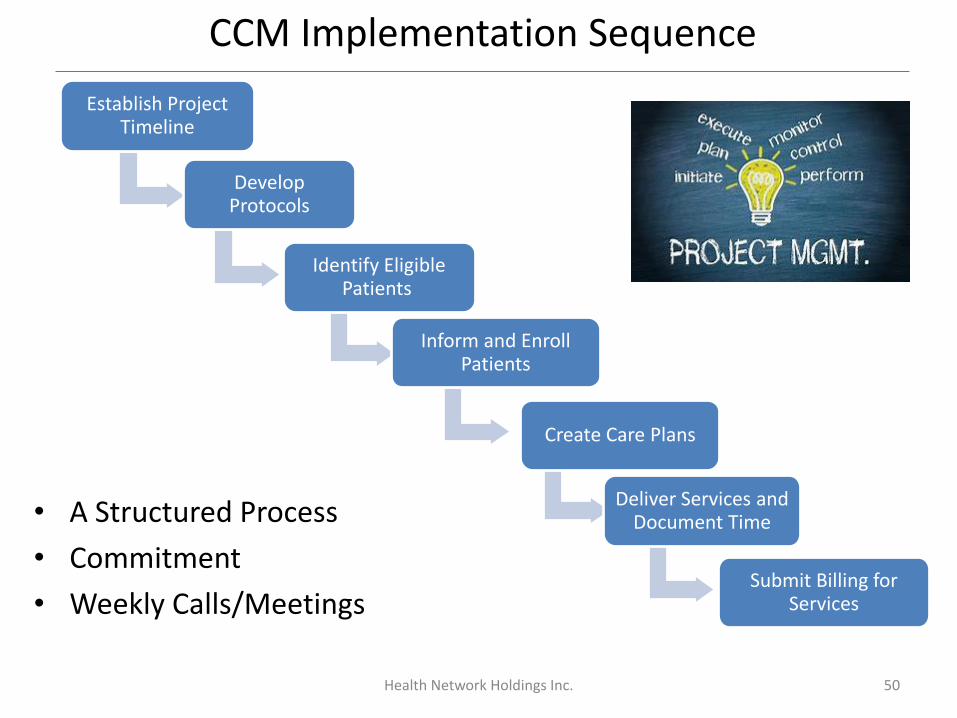
CCM Implementation Sequence
• A Structured Process
• Commitment
• Weekly Calls/Meetings
Health Network Holdings Inc. 50
Establish Project Timeline
Develop Protocols
Identify Eligible Patients
Inform and Enroll Patients
Create Care Plans
Deliver Services and Document Time
Submit Billing for Services

First 1-2 months
Explain program & obtain
patient consent
Create CCM care plan & share with
patient
StaffDocument Qualifying Activities
PATIENT ONBOARDING ONGOING, MONTHLY
Health Network Holdings Inc. 51
What to Expect

1. By Mail: Typical patient information sheet mailed to CCM-eligible patients.
This was printed in Spanish on the reverse side.
2. At the next scheduled office visit.
Health Network Holdings Inc. 52
Informing Eligible Patients

Monthly Care Outreach Activities
Health Network Holdings Inc. 53
Patient Centered Care Plan Care Plan reviewed and utilized as guide for discussions with patients and updated with any relevant changes.
Medication Oversight Medication reconciliation, treatment adherence, & prescription renewal assistance
Monitoring & Assessment Ongoing monitoring and assessment of patients medical, functional, and psychosocial needs, in accordance with Care Plan
Appointments & Community Services
Help patients schedule and attend appointments. Assist with barriers and follow up after appointments; Coordinate with community and home based services
NotifyNotify providers and nurses of any changes or updates with the patients’ health
Lessons and Results
Health Network Holdings Inc. 54
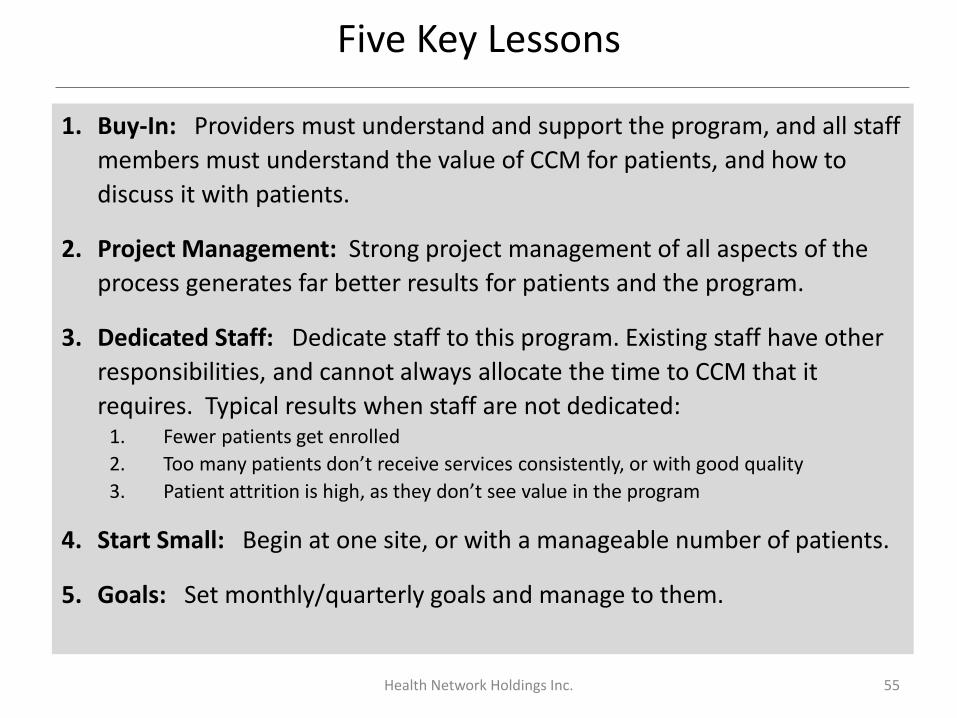
Five Key Lessons
Health Network Holdings Inc. 55
1. Buy-In: Providers must understand and support the program, and all staff
members must understand the value of CCM for patients, and how to
discuss it with patients.
2. Project Management: Strong project management of all aspects of the
process generates far better results for patients and the program.
3. Dedicated Staff: Dedicate staff to this program. Existing staff have other
responsibilities, and cannot always allocate the time to CCM that it
requires. Typical results when staff are not dedicated:1. Fewer patients get enrolled
2. Too many patients don’t receive services consistently, or with good quality
3. Patient attrition is high, as they don’t see value in the program
4. Start Small: Begin at one site, or with a manageable number of patients.
5. Goals: Set monthly/quarterly goals and manage to them.

Results to Date
• Over 2,500 patients receiving CCM services
• Incredible anecdotes from patients and care managers– Helped a patient keep her housing
– Improving medication management, refills and adherence
– Appointment assistance (PCP visits up 11%)
– Arranging for social services
– Improved continuity in patient record
– Patient engagement in health goals
• Phase 2– Assisting with AWVs
– Targeted preventative screenings for quality measurements
– Care transition follow-up
Health Network Holdings Inc. 56

Questions & Discussion
Health Network Holdings Inc. 57
Richard [email protected]
Office: (203)949-4032Mobile: (860)810-8599
linkedin.com/in/ralbrecht08
Thank you!
Look out for more information on Part 2 of our FQHC Webinar Series.
Interested in more webinars? Subscribe here.
Please remember to fill out our survey: https://www.surveymonkey.com/r/FH33FR9
58
Kathy Hsu Wibberly, PhD
Director, Mid-Atlantic
Telehealth Resource Center
UVA Center for Telehealth
Email: [email protected]
Phone: (434) 906-4960
Richard Albrecht
Director, Telehealth
Network, Health Network
Holdings, Inc.
Email: [email protected]
Office: (203) 949-4032
Mobile: (860) 810-8599
Howard Chapman, Jr.
Director of Programs and
Development
Email:
Telephone: (276) 398-2292
ext. 2221
Cell: (276) 494-1143


















