
FORMULARY ADDITIONS UPDATE: United … MedicareRx (PDP) plan FORMULARY ADDITIONS UPDATE: Brand Name...
39
United MedicareRx (PDP) plan FORMULARY ADDITIONS UPDATE: Brand Name Generic Name Dosage Form Strength Description of Change Effective Date of Change Tier Utilization Management Notes ACETASOL HC acetic acid/hydrocortisone Solution 2%, 1% Formulary Additions 03/01/09 Tier 1 ACTONEL risedronate sodium Tablet 150mg Removal of Utilization Management 03/01/09 Tier 2 QL (1 per 31 days), ST Removed ACTONEL risedronate sodium Tablet 30mg Removal of Utilization Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed ACTONEL risedronate sodium Tablet 35mg Removal of Utilization Management 03/01/09 Tier 2 QL (5 per 31 days), ST Removed ACTONEL risedronate sodium Tablet 5mg Removal of Utilization Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed ACTONEL risedronate sodium Tablet 75mg Removal of Utilization Management 03/01/09 Tier 2 QL (2 per 31 days), ST Removed ACTONEL WITH CALCIUM calcium carbonate/ risedronate sodium Tablet 1,250mg, 35mg Removal of Utilization Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed APRISO mesalamine (5-aspirin) 24-Hour Capsule 0.375gm Formulary Additions 03/01/09 Tier 3 QL (124 per 31 days) ASTEPRO azelastine hcl Solution 137mcg/spray Formulary Additions 03/01/09 Tier 3 QL (62 per 31 days) ATACAND candesartan cilexetil Tablet 16mg Removal of Utilization Management 03/01/09 Tier 3 QL (62 per 31 days), ST Removed The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009. FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS, OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold. 1 9/22/2009
Transcript of FORMULARY ADDITIONS UPDATE: United … MedicareRx (PDP) plan FORMULARY ADDITIONS UPDATE: Brand Name...

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
ACETASOL HC acetic acid/hydrocortisone Solution 2%, 1% Formulary Additions 03/01/09 Tier 1
ACTONEL risedronate sodium Tablet 150mg Removal of Utilization Management 03/01/09 Tier 2 QL (1 per 31 days), ST Removed
ACTONEL risedronate sodium Tablet 30mg Removal of Utilization Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed
ACTONEL risedronate sodium Tablet 35mg Removal of Utilization Management 03/01/09 Tier 2 QL (5 per 31 days), ST Removed
ACTONEL risedronate sodium Tablet 5mg Removal of Utilization Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed
ACTONEL risedronate sodium Tablet 75mg Removal of Utilization Management 03/01/09 Tier 2 QL (2 per 31 days), ST Removed
ACTONEL WITH CALCIUM calcium carbonate/risedronate sodium Tablet 1,250mg, 35mg Removal of Utilization
Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed
APRISO mesalamine (5-aspirin) 24-Hour Capsule 0.375gm Formulary Additions 03/01/09 Tier 3 QL (124 per 31 days)
ASTEPRO azelastine hcl Solution 137mcg/spray Formulary Additions 03/01/09 Tier 3 QL (62 per 31 days)
ATACAND candesartan cilexetil Tablet 16mg Removal of Utilization Management 03/01/09 Tier 3 QL (62 per 31 days), ST Removed
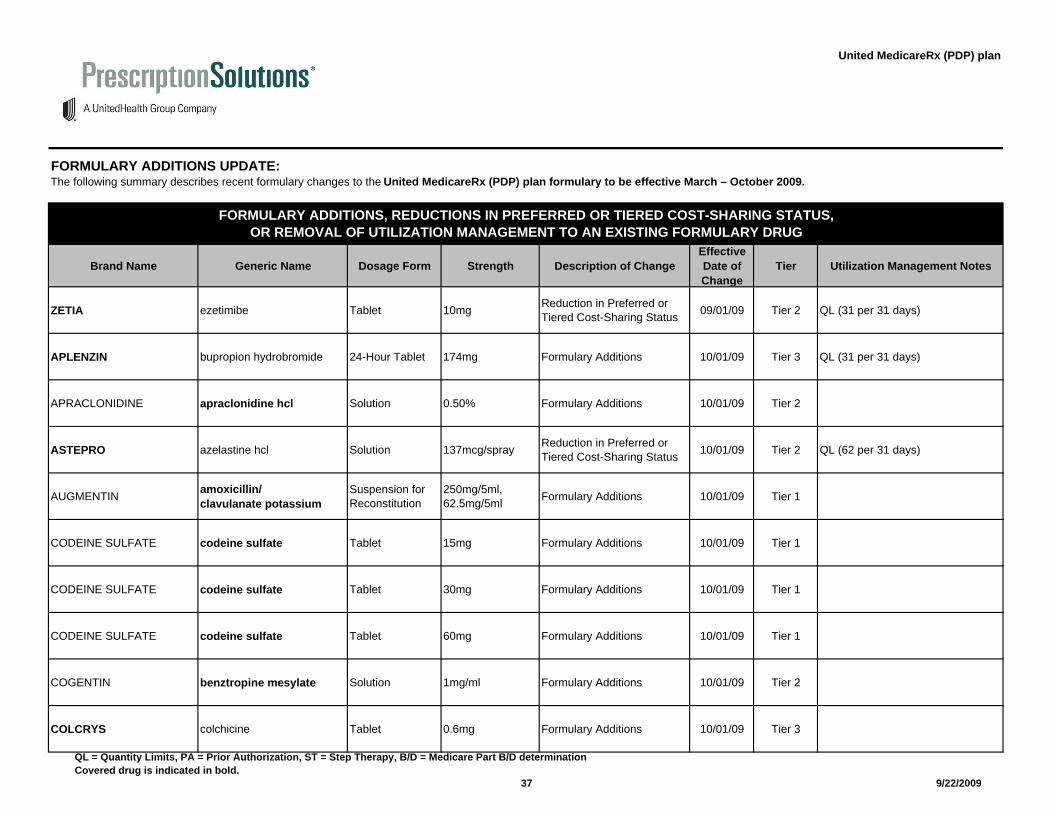
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
1
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
ATACAND candesartan cilexetil Tablet 32mg Removal of Utilization Management 03/01/09 Tier 3 QL (31 per 31 days), ST Removed
ATACAND candesartan cilexetil Tablet 4mg Removal of Utilization Management 03/01/09 Tier 3 QL (31 per 31 days), ST Removed
ATACAND candesartan cilexetil Tablet 8mg Removal of Utilization Management 03/01/09 Tier 3 QL (93 per 31 days), ST Removed
ATACAND HCT candesartan cilexetil/hydrochlorothiazide Tablet 16mg, 12.5mg Removal of Utilization
Management 03/01/09 Tier 3 QL (62 per 31 days), ST Removed
ATACAND HCT candesartan cilexetil/hydrochlorothiazide Tablet 32mg, 25mg Formulary Additions 03/01/09 Tier 3 QL (31 per 31 days)
ATACAND HCT candesartan cilexetil/hydrochlorothiazide Tablet 32mg, 12.5mg Removal of Utilization
Management 03/01/09 Tier 3 QL (31 per 31 days), ST Removed
BANZEL rufinamide Tablet 200mg Formulary Additions 03/01/09 Tier 3 QL (248 per 31 days)
BANZEL rufinamide Tablet 400mg Formulary Additions 03/01/09 Tier 3 QL (248 per 31 days)
BENICAR olmesartan medoxomil Tablet 20mg Removal of Utilization Management 03/01/09 Tier 2 QL (62 per 31 days), ST Removed
BENICAR olmesartan medoxomil Tablet 40mg Removal of Utilization Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
2
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
BENICAR olmesartan medoxomil Tablet 5mg Removal of Utilization Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed
BENICAR HCT hydrochlorothiazide/olmesartan medoxomil Tablet 12.5mg, 20mg Removal of Utilization
Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed
BENICAR HCT hydrochlorothiazide/olmesartan medoxomil Tablet 12.5mg, 40mg Removal of Utilization
Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed
BENICAR HCT hydrochlorothiazide/olmesartan medoxomil Tablet 25mg, 40mg Removal of Utilization
Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed
BONIVA ibandronate sodium Tablet 150mg Removal of Utilization Management 03/01/09 Tier 2 QL (1 per 31 days), ST Removed
BONIVA ibandronate sodium Tablet 2.5mg Removal of Utilization Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed
BYETTA exenatide Solution 10mcg/0.04ml Removal of Utilization Management 03/01/09 Tier 2 PA removed, ST
BYETTA exenatide Solution 5mcg/0.02ml Removal of Utilization Management 03/01/09 Tier 2 PA removed, ST
CLARINEX desloratadine Syrup 0.5mg/ml Removal of Utilization Management 03/01/09 Tier 3 QL (310 per 31 days), ST Removed
CLARINEX desloratadine Tablet 5mg Removal of Utilization Management 03/01/09 Tier 3 QL (31 per 31 days), ST Removed
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
3
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
CLARINEX REDITABS desloratadine Dispersible Tablet 2.5mg Removal of Utilization
Management 03/01/09 Tier 3 QL (31 per 31 days), ST Removed
CLARINEX REDITABS desloratadine Dispersible Tablet 5mg Removal of Utilization
Management 03/01/09 Tier 3 QL (31 per 31 days), ST Removed
COSOPT dorzolamide hcl/timolol maleate Solution 2%, 0.5% Formulary Additions 03/01/09 Tier 1
DAZIDOX oxycodone hcl Tablet 10mg Formulary Additions 03/01/09 Tier 1
DAZIDOX oxycodone hcl Tablet 20mg Formulary Additions 03/01/09 Tier 1
DIAMOX acetazolamide 12-Hour Capsule 500mg Formulary Additions 03/01/09 Tier 1
DIOVAN valsartan Tablet 160mg Removal of Utilization Management 03/01/09 Tier 2 QL (62 per 31 days), ST Removed
DIOVAN valsartan Tablet 320mg Removal of Utilization Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed
DIOVAN valsartan Tablet 40mg Removal of Utilization Management 03/01/09 Tier 2 QL (62 per 31 days), ST Removed
DIOVAN valsartan Tablet 80mg Removal of Utilization Management 03/01/09 Tier 2 QL (62 per 31 days), ST Removed
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
4
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
DIOVAN HCT hydrochlorothiazide/valsartan Tablet 12.5mg, 160mg Removal of Utilization
Management 03/01/09 Tier 2 QL (62 per 31 days), ST Removed
DIOVAN HCT hydrochlorothiazide/valsartan Tablet 12.5mg, 320mg Removal of Utilization
Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed
DIOVAN HCT hydrochlorothiazide/valsartan Tablet 12.5mg, 80mg Removal of Utilization
Management 03/01/09 Tier 2 QL (62 per 31 days), ST Removed
DIOVAN HCT hydrochlorothiazide/valsartan Tablet 25mg, 160mg Removal of Utilization
Management 03/01/09 Tier 2 QL (62 per 31 days), ST Removed
DIOVAN HCT hydrochlorothiazide/ valsartan Tablet 25mg, 320mg Removal of Utilization
Management 03/01/09 Tier 2 QL (31 per 31 days), ST Removed
DITROPAN oxybutynin chloride Syrup 5mg/5ml Formulary Additions 03/01/09 Tier 3
DORYX doxycycline hyclate Delayed Release Tablet 150mg Formulary Additions 03/01/09 Tier 3
DUREZOL difluprednate Emulsion 0.05% Formulary Additions 03/01/09 Tier 3
EPIDUO adapalene/benzoyl peroxide Gel 0.1%, 2.5% Formulary Additions 03/01/09 Tier 3 ST
FORTEO teriparatide Solution 600mcg/2.4ml Formulary Additions 03/01/09 Tier 3 PA, B/D
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
5
9/22/2009
United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
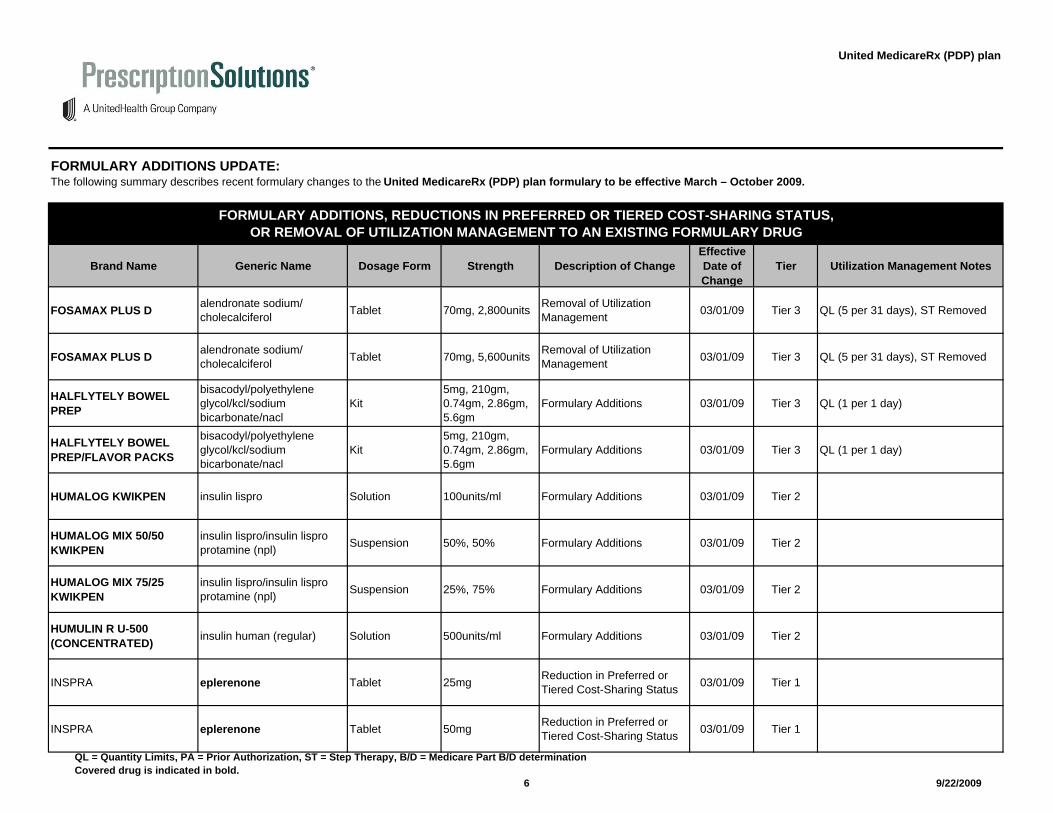
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
FOSAMAX PLUS D alendronate sodium/cholecalciferol Tablet 70mg, 2,800units Removal of Utilization
Management 03/01/09 Tier 3 QL (5 per 31 days), ST Removed
FOSAMAX PLUS D alendronate sodium/cholecalciferol Tablet 70mg, 5,600units Removal of Utilization
Management 03/01/09 Tier 3 QL (5 per 31 days), ST Removed
HALFLYTELY BOWEL PREP
bisacodyl/polyethylene glycol/kcl/sodium bicarbonate/nacl
Kit5mg, 210gm, 0.74gm, 2.86gm, 5.6gm
Formulary Additions 03/01/09 Tier 3 QL (1 per 1 day)
HALFLYTELY BOWEL PREP/FLAVOR PACKS
bisacodyl/polyethylene glycol/kcl/sodium bicarbonate/nacl
Kit5mg, 210gm, 0.74gm, 2.86gm, 5.6gm
Formulary Additions 03/01/09 Tier 3 QL (1 per 1 day)
HUMALOG KWIKPEN insulin lispro Solution 100units/ml Formulary Additions 03/01/09 Tier 2
HUMALOG MIX 50/50 KWIKPEN
insulin lispro/insulin lispro protamine (npl) Suspension 50%, 50% Formulary Additions 03/01/09 Tier 2
HUMALOG MIX 75/25 KWIKPEN
insulin lispro/insulin lispro protamine (npl) Suspension 25%, 75% Formulary Additions 03/01/09 Tier 2
HUMULIN R U-500 (CONCENTRATED) insulin human (regular) Solution 500units/ml Formulary Additions 03/01/09 Tier 2
INSPRA eplerenone Tablet 25mg Reduction in Preferred or Tiered Cost-Sharing Status 03/01/09 Tier 1
INSPRA eplerenone Tablet 50mg Reduction in Preferred or Tiered Cost-Sharing Status 03/01/09 Tier 1
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
6
9/22/2009
United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
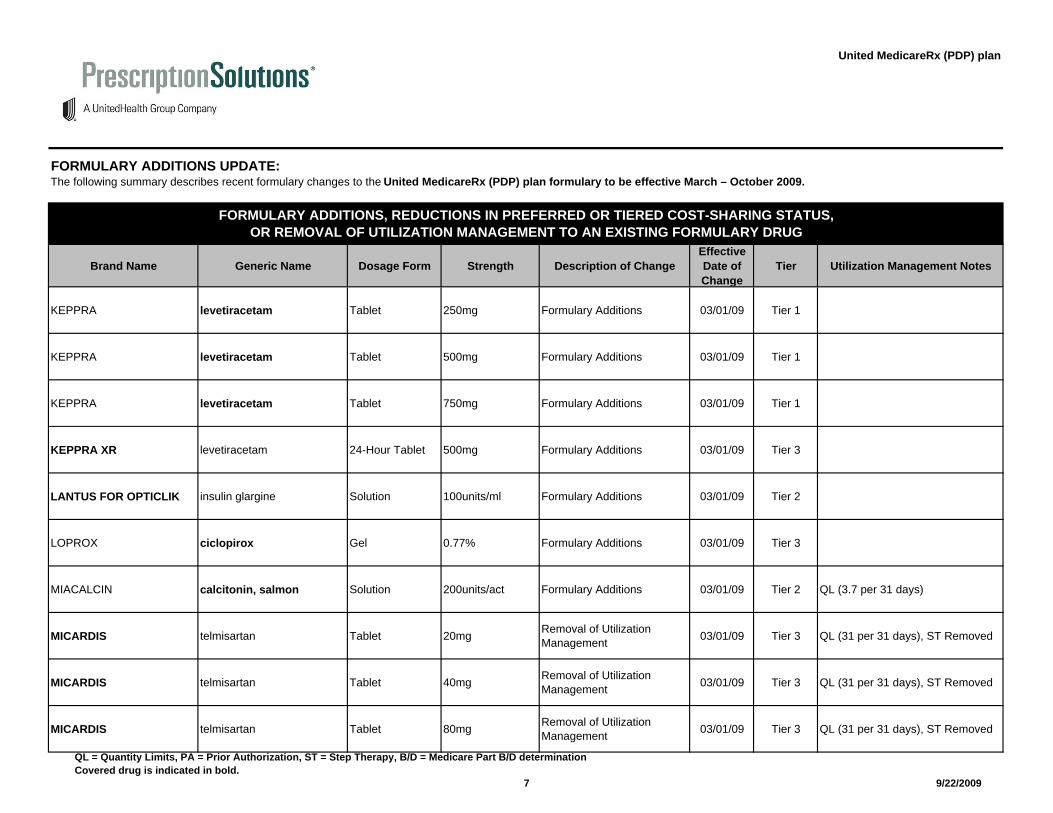
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
KEPPRA levetiracetam Tablet 250mg Formulary Additions 03/01/09 Tier 1
KEPPRA levetiracetam Tablet 500mg Formulary Additions 03/01/09 Tier 1
KEPPRA levetiracetam Tablet 750mg Formulary Additions 03/01/09 Tier 1
KEPPRA XR levetiracetam 24-Hour Tablet 500mg Formulary Additions 03/01/09 Tier 3
LANTUS FOR OPTICLIK insulin glargine Solution 100units/ml Formulary Additions 03/01/09 Tier 2
LOPROX ciclopirox Gel 0.77% Formulary Additions 03/01/09 Tier 3
MIACALCIN calcitonin, salmon Solution 200units/act Formulary Additions 03/01/09 Tier 2 QL (3.7 per 31 days)
MICARDIS telmisartan Tablet 20mg Removal of Utilization Management 03/01/09 Tier 3 QL (31 per 31 days), ST Removed
MICARDIS telmisartan Tablet 40mg Removal of Utilization Management 03/01/09 Tier 3 QL (31 per 31 days), ST Removed
MICARDIS telmisartan Tablet 80mg Removal of Utilization Management 03/01/09 Tier 3 QL (31 per 31 days), ST Removed
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
7
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
MICARDIS HCT hydrochlorothiazide/telmisartan Tablet 12.5mg, 40mg Removal of Utilization
Management 03/01/09 Tier 3 QL (62 per 31 days), ST Removed
MICARDIS HCT hydrochlorothiazide/telmisartan Tablet 12.5mg, 80mg Removal of Utilization
Management 03/01/09 Tier 3 QL (62 per 31 days), ST Removed
MICARDIS HCT hydrochlorothiazide/telmisartan Tablet 25mg, 80mg Removal of Utilization
Management 03/01/09 Tier 3 QL (62 per 31 days), ST Removed
MILLIPRED prednisolone sodium phosphate Solution 10mg/5ml Formulary Additions 03/01/09 Tier 3
MORPHINE SULFATE morphine sulfate Solution 10mg/5ml Formulary Additions 03/01/09 Tier 1
MORPHINE SULFATE morphine sulfate Solution 20mg/5ml Formulary Additions 03/01/09 Tier 1
MOXATAG amoxicillin 24-Hour Tablet 775mg Formulary Additions 03/01/09 Tier 3
NORDITROPIN NORDIFLEX PEN somatropin Solution 10mg/1.5ml Formulary Additions 03/01/09 Tier 4 PA
NULYTELY/FLAVOR PACKS
polyethylene glycol/kcl/sodium bicarbonate/nacl
Solution for Reconstitution
420gm, 1.48gm, 5.72gm, 11.2gm Formulary Additions 03/01/09 Tier 2 QL (1 per 1 day)
OMNITROPE somatropin Solution 10mg/1.5ml Formulary Additions 03/01/09 Tier 4 PA
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
8
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
OMNITROPE somatropin Solution 5mg/1.5ml Formulary Additions 03/01/09 Tier 4 PA
OXYCONTIN oxycodone hcl 12-Hour Tablet 10mg Formulary Additions 03/01/09 Tier 3 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 20mg Formulary Additions 03/01/09 Tier 3 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 40mg Formulary Additions 03/01/09 Tier 3 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 80mg Formulary Additions 03/01/09 Tier 3 QL (186 per 31 days)
PARCOPA carbidopa anhydrous/levodopa
Dispersible Tablet 10mg, 100mg Formulary Additions 03/01/09 Tier 3 ST
PARCOPA carbidopa anhydrous/levodopa
Dispersible Tablet 25mg, 250mg Formulary Additions 03/01/09 Tier 3 ST
PARCOPA carbidopa monohydrate/levodopa
Dispersible Tablet 25mg, 100mg Formulary Additions 03/01/09 Tier 3 ST
PATANASE olopatadine hcl Solution 0.6% Reduction in Preferred or Tiered Cost-Sharing Status 03/01/09 Tier 2 QL (30.5 per 31 days)
PHOSLO calcium acetate Capsule 667mg Formulary Additions 03/01/09 Tier 1
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
9
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
PRANDIMET metformin hcl/repaglinide Tablet 500mg, 1mg Formulary Additions 03/01/09 Tier 3 QL (155 per 31 days), ST
PRANDIMET metformin hcl/repaglinide Tablet 500mg, 2mg Formulary Additions 03/01/09 Tier 3 QL (155 per 31 days), ST
PREZISTA darunavir ethanolate Tablet 600mg Formulary Additions 03/01/09 Tier 4
PREZISTA darunavir ethanolate Tablet 400mg Formulary Additions 03/01/09 Tier 4
PRILOSEC omeprazole Delayed Release Capsule 40mg Formulary Additions 03/01/09 Tier 3
PROMACTA eltrombopag olamine Tablet 25mg Formulary Additions 03/01/09 Tier 4 PA
PROMACTA eltrombopag olamine Tablet 50mg Formulary Additions 03/01/09 Tier 4 PA
RAZADYNE ER galantamine hydrobromide 24-Hour Capsule 16mg Formulary Additions 03/01/09 Tier 1
RAZADYNE ER galantamine hydrobromide 24-Hour Capsule 24mg Formulary Additions 03/01/09 Tier 1
RAZADYNE ER galantamine hydrobromide 24-Hour Capsule 8mg Formulary Additions 03/01/09 Tier 1
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
10
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
RELISTOR methylnaltrexone bromide Kit 12mg/0.6ml Formulary Additions 03/01/09 Tier 4 PA
RELISTOR methylnaltrexone bromide Solution 12mg/0.6ml Formulary Additions 03/01/09 Tier 4 PA
REPREXAIN hydrocodone bitartrate/ibuprofen Tablet 10mg, 200mg Formulary Additions 03/01/09 Tier 3
REPREXAIN hydrocodone bitartrate/ibuprofen Tablet 2.5mg, 200mg Formulary Additions 03/01/09 Tier 3
REQUIP XL ropinirole hcl 24-Hour Tablet 12mg Formulary Additions 03/01/09 Tier 3
SANCTURA trospium chloride Tablet 20mg Removal of Utilization Management 03/01/09 Tier 3 QL (62 per 31 days), ST Removed
SANCTURA XR trospium chloride 24-Hour Capsule 60mg Removal of Utilization Management 03/01/09 Tier 3 QL (31 per 31 days), ST Removed
SANCUSO granisetron Patch 3.1mg/24hr Formulary Additions 03/01/09 Tier 4 QL (1 per 1 day)
SPECTRACEF cefditoren pivoxil Tablet 400mg Formulary Additions 03/01/09 Tier 2
STALEVO 125 carbidopa monohydrate/entacapone/levodopa Tablet 31.25mg, 200mg,
125mg Formulary Additions 03/01/09 Tier 2 ST
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
11
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
STALEVO 75 carbidopa monohydrate/entacapone/levodopa Tablet 18.75mg, 200mg,
75mg Formulary Additions 03/01/09 Tier 2 ST
SULAR nisoldipine 24-Hour Tablet 17mg Reduction in Preferred or Tiered Cost-Sharing Status 03/01/09 Tier 2 QL (31 per 31 days)
SULAR nisoldipine 24-Hour Tablet 25.5mg Reduction in Preferred or Tiered Cost-Sharing Status 03/01/09 Tier 2 QL (31 per 31 days)
SULAR nisoldipine 24-Hour Tablet 34mg Reduction in Preferred or Tiered Cost-Sharing Status 03/01/09 Tier 2 QL (31 per 31 days)
SULAR nisoldipine 24-Hour Tablet 8.5mg Reduction in Preferred or Tiered Cost-Sharing Status 03/01/09 Tier 2 QL (31 per 31 days)
TOBRAMYCIN/DEXAMETHASONE
dexamethasone/tobramycin sulfate Suspension 0.1%, 0.3% Formulary Additions 03/01/09 Tier 1
TRILIPIX choline fenofibrate Delayed Release Capsule 135mg Formulary Additions 03/01/09 Tier 3 PA
TRILIPIX choline fenofibrate Delayed Release Capsule 45mg Formulary Additions 03/01/09 Tier 3 PA
TRUSOPT dorzolamide hcl Solution 2% Formulary Additions 03/01/09 Tier 1
UNITHROID levothyroxine sodium Tablet 137mcg Formulary Additions 03/01/09 Tier 1
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
12
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
VENLAFAXINE HCL ER venlafaxine hcl 24-Hour Tablet 150mg Formulary Additions 03/01/09 Tier 3 QL (62 per 31 days)
VENLAFAXINE HCL ER venlafaxine hcl 24-Hour Tablet 225mg Formulary Additions 03/01/09 Tier 3 QL (31 per 31 days)
VENLAFAXINE HCL ER venlafaxine hcl 24-Hour Tablet 37.5mg Formulary Additions 03/01/09 Tier 3 QL (93 per 31 days)
VENLAFAXINE HCL ER venlafaxine hcl 24-Hour Tablet 75mg Formulary Additions 03/01/09 Tier 3 QL (93 per 31 days)
VERIPRED 20 prednisolone sodium phosphate Solution 20mg/5ml Formulary Additions 03/01/09 Tier 3
VIDEX EC didanosine Delayed Release Capsule 125mg Formulary Additions 03/01/09 Tier 1
VIVACTIL protriptyline hcl Tablet 10mg Formulary Additions 03/01/09 Tier 1
VIVACTIL protriptyline hcl Tablet 5mg Formulary Additions 03/01/09 Tier 1
XALATAN latanoprost Solution 0.005% Removal of Utilization Management 03/01/09 Tier 3 QL (2.5 per 31 days), ST Removed
XENAZINE tetrabenazine Tablet 12.5mg Formulary Additions 03/01/09 Tier 4 PA
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
13
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
XENAZINE tetrabenazine Tablet 25mg Formulary Additions 03/01/09 Tier 4 PA
XYZAL levocetirizine dihydrochloride Solution 2.5mg/5ml Removal of Utilization Management 03/01/09 Tier 3 QL (310 per 31 days), ST Removed
XYZAL levocetirizine dihydrochloride Tablet 5mg Removal of Utilization Management 03/01/09 Tier 3 QL (31 per 31 days), ST Removed
ZERIT stavudine Capsule 15mg Formulary Additions 03/01/09 Tier 1
ZERIT stavudine Capsule 20mg Formulary Additions 03/01/09 Tier 1
ZERIT stavudine Capsule 30mg Formulary Additions 03/01/09 Tier 1
ZERIT stavudine Capsule 40mg Formulary Additions 03/01/09 Tier 1
ZETIA ezetimibe Tablet 10mg Removal of Utilization Management 03/01/09 Tier 3 QL (31 per 31 days), ST Removed
ZOLOFT sertraline hcl Tablet 50mg Formulary Additions 03/01/09 Tier 3
ADOXA PAK 1/150 doxycycline monohydrate Tablet 150mg Formulary Additions 04/01/09 Tier 3
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
14
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
ALTACE ramipril Tablet 1.25mg Formulary Additions 04/01/09 Tier 3
ALTACE ramipril Tablet 10mg Formulary Additions 04/01/09 Tier 3
ALTACE ramipril Tablet 2.5mg Formulary Additions 04/01/09 Tier 3
ALTACE ramipril Tablet 5mg Formulary Additions 04/01/09 Tier 3
AVINZA morphine sulfate 24-Hour Capsule 45mg Formulary Additions 04/01/09 Tier 2 QL (120 per 31 days)
AVINZA morphine sulfate 24-Hour Capsule 75mg Formulary Additions 04/01/09 Tier 2 QL (120 per 31 days)
BLEPH-10 sulfacetamide sodium Solution 10% Formulary Additions 04/01/09 Tier 1
BUDEPRION XL bupropion hcl 24-Hour Tablet 300mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 1 QL (31 per 31 days)
BYETTA exenatide Solution 10mcg/0.04ml Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2 ST
BYETTA exenatide Solution 5mcg/0.02ml Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2 ST
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
15
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
CAPOTEN captopril Tablet 100mg Formulary Additions 04/01/09 Tier 3
CARBINOXAMINE MALEATE carbinoxamine maleate Tablet 4mg Formulary Additions 04/01/09 Tier 2
DEPAKOTE ER divalproex sodium 24-Hour Tablet 250mg Formulary Additions 04/01/09 Tier 1
DEPAKOTE ER divalproex sodium 24-Hour Tablet 500mg Formulary Additions 04/01/09 Tier 1
DEPAKOTE SPRINKLES divalproex sodium Sprinkle Capsule 125mg Formulary Additions 04/01/09 Tier 1
ENDOCET acetaminophen/oxycodone hcl Tablet 325mg, 10mg Formulary Additions 04/01/09 Tier 1
ENDOCET acetaminophen/oxycodone hcl Tablet 325mg, 7.5mg Formulary Additions 04/01/09 Tier 1
ENDOCET acetaminophen/oxycodone hcl Tablet 500mg, 7.5mg Formulary Additions 04/01/09 Tier 1
ENDOCET acetaminophen/oxycodone hcl Tablet 650mg, 10mg Formulary Additions 04/01/09 Tier 1
FLOVENT DISKUS fluticasone propionate Aerosol Powder 100mcg/blist Formulary Additions 04/01/09 Tier 3 ST
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
16
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
FLOVENT DISKUS fluticasone propionate Aerosol Powder 250mcg/blist Formulary Additions 04/01/09 Tier 3 ST
FLOVENT DISKUS fluticasone propionate Aerosol Powder 50mcg/blist Formulary Additions 04/01/09 Tier 3 ST
GENERLAC lactulose Solution 10gm/15ml Formulary Additions 04/01/09 Tier 1
IMITREX sumatriptan succinate Solution 6mg/0.5ml Formulary Additions 04/01/09 Tier 1 QL (4 per 31 days)
IMITREX sumatriptan succinate Tablet 100mg Formulary Additions 04/01/09 Tier 1 QL (18 per 31 days)
IMITREX sumatriptan succinate Tablet 25mg Formulary Additions 04/01/09 Tier 1 QL (18 per 31 days)
IMITREX sumatriptan succinate Tablet 50mg Formulary Additions 04/01/09 Tier 1 QL (18 per 31 days)
JANUMET metformin hcl/sitagliptin phosphate Tablet 1,000mg, 50mg Reduction in Preferred or
Tiered Cost-Sharing Status 04/01/09 Tier 2 ST
JANUMET metformin hcl/sitagliptin phosphate Tablet 500mg, 50mg Reduction in Preferred or
Tiered Cost-Sharing Status 04/01/09 Tier 2 ST
JANUVIA sitagliptin phosphate Tablet 100mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2 ST
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
17
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
JANUVIA sitagliptin phosphate Tablet 25mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2 ST
JANUVIA sitagliptin phosphate Tablet 50mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2 ST
KAPIDEX dexlansoprazole Delayed Release Capsule 30mg Formulary Additions 04/01/09 Tier 3 ST
KAPIDEX dexlansoprazole Delayed Release Capsule 60mg Formulary Additions 04/01/09 Tier 3 ST
KEPPRA levetiracetam Solution 100mg/ml Formulary Additions 04/01/09 Tier 1
KEPPRA levetiracetam Tablet 1,000mg Formulary Additions 04/01/09 Tier 1
LAMICTAL lamotrigine Tablet 100mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2
LAMICTAL lamotrigine Tablet 150mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2
LAMICTAL lamotrigine Tablet 200mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2
LAMICTAL lamotrigine Tablet 25mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
18
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
METROGEL-VAGINAL metronidazole Gel 0.75% Formulary Additions 04/01/09 Tier 3
PALGIC carbinoxamine maleate Liquid 4mg/5ml Formulary Additions 04/01/09 Tier 2
PREZISTA darunavir ethanolate Tablet 75mg Formulary Additions 04/01/09 Tier 4
RANEXA ranolazine 12-Hour Tablet 1,000mg Removal of Utilization Management 04/01/09 Tier 2 PA removed, ST
RANEXA ranolazine 12-Hour Tablet 500mg Removal of Utilization Management 04/01/09 Tier 2 PA removed, ST
REQUIP ropinirole hcl Tablet 0.25mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2
REQUIP ropinirole hcl Tablet 0.5mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2
REQUIP ropinirole hcl Tablet 1mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2
REQUIP ropinirole hcl Tablet 2mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2
REQUIP ropinirole hcl Tablet 3mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
19
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
REQUIP ropinirole hcl Tablet 4mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2
REQUIP ropinirole hcl Tablet 5mg Reduction in Preferred or Tiered Cost-Sharing Status 04/01/09 Tier 2
RESERPINE reserpine Tablet 0.1mg Formulary Additions 04/01/09 Tier 1
RISPERDAL risperidone Solution 1mg/ml Formulary Additions 04/01/09 Tier 3
SARAFEM fluoxetine hcl Tablet 10mg Formulary Additions 04/01/09 Tier 3 QL (31 per 31 days), ST
SARAFEM fluoxetine hcl Tablet 20mg Formulary Additions 04/01/09 Tier 3 QL (62 per 31 days), ST
SELFEMRA fluoxetine hcl Capsule 10mg Formulary Additions 04/01/09 Tier 3 QL (31 per 31 days), ST
SELFEMRA fluoxetine hcl Capsule 20mg Formulary Additions 04/01/09 Tier 3 QL (62 per 31 days), ST
TEKTURNA HCT aliskiren fumarate/hydrochlorothiazide Tablet 150mg, 12.5mg Reduction in Preferred or
Tiered Cost-Sharing Status 04/01/09 Tier 2 QL (31 per 31 days), ST
TEKTURNA HCT aliskiren fumarate/hydrochlorothiazide Tablet 150mg, 25mg Reduction in Preferred or
Tiered Cost-Sharing Status 04/01/09 Tier 2 QL (31 per 31 days), ST
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
20
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
TEKTURNA HCT aliskiren fumarate/hydrochlorothiazide Tablet 300mg, 12.5mg Reduction in Preferred or
Tiered Cost-Sharing Status 04/01/09 Tier 2 QL (31 per 31 days), ST
TEKTURNA HCT aliskiren fumarate/hydrochlorothiazide Tablet 300mg, 25mg Reduction in Preferred or
Tiered Cost-Sharing Status 04/01/09 Tier 2 QL (31 per 31 days), ST
TERAZOL 3 terconazole Cream 0.80% Formulary Additions 04/01/09 Tier 3
ACANYA benzoyl peroxide/clindamycin phosphate Gel 2.5%, 1.2% Formulary Additions 06/01/09 Tier 3 ST
AFINITOR everolimus Tablet 10mg Formulary Additions 06/01/09 Tier 4 PA
AFINITOR everolimus Tablet 5mg Formulary Additions 06/01/09 Tier 4 PA
APLENZIN bupropion hydrobromide 24-Hour Tablet 348mg Formulary Additions 06/01/09 Tier 3 QL (31 per 31 days)
APLENZIN bupropion hydrobromide 24-Hour Tablet 522mg Formulary Additions 06/01/09 Tier 3 QL (31 per 31 days)
COLESTID, COLESTID FLAVORED colestipol hcl Granules 5gm Reduction in Preferred or
Tiered Cost-Sharing Status 06/01/09 Tier 1
COLESTID, COLESTID FLAVORED colestipol hcl Pack 5gm Formulary Additions 06/01/09 Tier 1
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
21
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
DEGARELIX degarelix acetate Solution for Reconstitution 120mg Formulary Additions 06/01/09 Tier 4 PA
DEGARELIX degarelix acetate Solution for Reconstitution 80mg Formulary Additions 06/01/09 Tier 4 PA
DILTZAC diltiazem hcl 24-Hour Capsule 120mg Formulary Additions 06/01/09 Tier 1
DILTZAC diltiazem hcl 24-Hour Capsule 180mg Formulary Additions 06/01/09 Tier 1
DILTZAC diltiazem hcl 24-Hour Capsule 240mg Formulary Additions 06/01/09 Tier 1
DILTZAC diltiazem hcl 24-Hour Capsule 300mg Formulary Additions 06/01/09 Tier 1
DILTZAC diltiazem hcl 24-Hour Capsule 360mg Formulary Additions 06/01/09 Tier 1
FLOVENT DISKUS fluticasone propionate Aerosol Powder 100mcg/blist Reduction in Preferred or Tiered Cost-Sharing Status 06/01/09 Tier 2 ST Removed
FLOVENT DISKUS fluticasone propionate Aerosol Powder 250mcg/blist Reduction in Preferred or Tiered Cost-Sharing Status 06/01/09 Tier 2 ST Removed
FLOVENT DISKUS fluticasone propionate Aerosol Powder 50mcg/blist Reduction in Preferred or Tiered Cost-Sharing Status 06/01/09 Tier 2 ST Removed
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
22
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
IMITREX STATDOSE SYSTEM sumatriptan succinate Kit 4mg/0.5ml Formulary Additions 06/01/09 Tier 2 QL (4 per 31 days)
IMITREX STATDOSE SYSTEM sumatriptan succinate Kit 6mg/0.5ml Formulary Additions 06/01/09 Tier 2 QL (4 per 31 days)
KEPPRA XR levetiracetam 24-Hour Tablet 750mg Formulary Additions 06/01/09 Tier 3
OXYCONTIN oxycodone hcl 12-Hour Tablet 10mg Less Restrictive Utilization Management 06/01/09 Tier 3 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 15mg Less Restrictive Utilization Management 06/01/09 Tier 3 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 20mg Less Restrictive Utilization Management 06/01/09 Tier 3 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 30mg Less Restrictive Utilization Management 06/01/09 Tier 3 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 40mg Less Restrictive Utilization Management 06/01/09 Tier 3 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 60mg Less Restrictive Utilization Management 06/01/09 Tier 3 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 80mg Less Restrictive Utilization Management 06/01/09 Tier 3 QL (186 per 31 days)
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
23
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
PRILOSEC omeprazole Delayed Release Capsule 40mg Reduction in Preferred or
Tiered Cost-Sharing Status 06/01/09 Tier 1
RAPAFLO silodosin Capsule 4mg Formulary Additions 06/01/09 Tier 3 QL (31 per 31 days), ST
RAPAFLO silodosin Capsule 8mg Formulary Additions 06/01/09 Tier 3 QL (31 per 31 days), ST
SPRYCEL dasatinib Tablet 100mg Formulary Additions 06/01/09 Tier 4 PA
SUMATRIPTAN SUCCINATE sumatriptan succinate Solution 4mg/0.5ml Formulary Additions 06/01/09 Tier 1 QL (4 per 31 days)
SUPRAX cefixime Tablet 400mg Formulary Additions 06/01/09 Tier 3
TOVIAZ fesoterodine fumarate 24-Hour Tablet 4mg Formulary Additions 06/01/09 Tier 3 QL (31 per 31 days), ST
TOVIAZ fesoterodine fumarate 24-Hour Tablet 8mg Formulary Additions 06/01/09 Tier 3 QL (31 per 31 days), ST
ULORIC febuxostat Tablet 40mg Formulary Additions 06/01/09 Tier 3 QL (31 per 31 days), ST
ULORIC febuxostat Tablet 80mg Formulary Additions 06/01/09 Tier 3 QL (31 per 31 days), ST
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
24
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
VECTICAL calcitriol Ointment 3mcg/gm Formulary Additions 06/01/09 Tier 3 ST
VIMPAT lacosamide Tablet 100mg Formulary Additions 06/01/09 Tier 3 QL (62 per 31 days), PA
VIMPAT lacosamide Tablet 150mg Formulary Additions 06/01/09 Tier 3 QL (62 per 31 days), PA
VIMPAT lacosamide Tablet 200mg Formulary Additions 06/01/09 Tier 3 QL (62 per 31 days), PA
VIMPAT lacosamide Tablet 50mg Formulary Additions 06/01/09 Tier 3 QL (62 per 31 days), PA
ZEMPLAR paricalcitol Capsule 1mcg Reduction in Preferred or Tiered Cost-Sharing Status 06/01/09 Tier 2
ZEMPLAR paricalcitol Capsule 2mcg Reduction in Preferred or Tiered Cost-Sharing Status 06/01/09 Tier 2
ZEMPLAR paricalcitol Capsule 4mcg Reduction in Preferred or Tiered Cost-Sharing Status 06/01/09 Tier 2
BYSTOLIC nebivolol hcl Tablet 10mg Reduction in Preferred or Tiered Cost-Sharing Status 07/01/09 Tier 2 QL (124 per 31 days), ST Removed
BYSTOLIC nebivolol hcl Tablet 2.5mg Reduction in Preferred or Tiered Cost-Sharing Status 07/01/09 Tier 2 QL (31 per 31 days), ST Removed
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
25
9/22/2009
United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
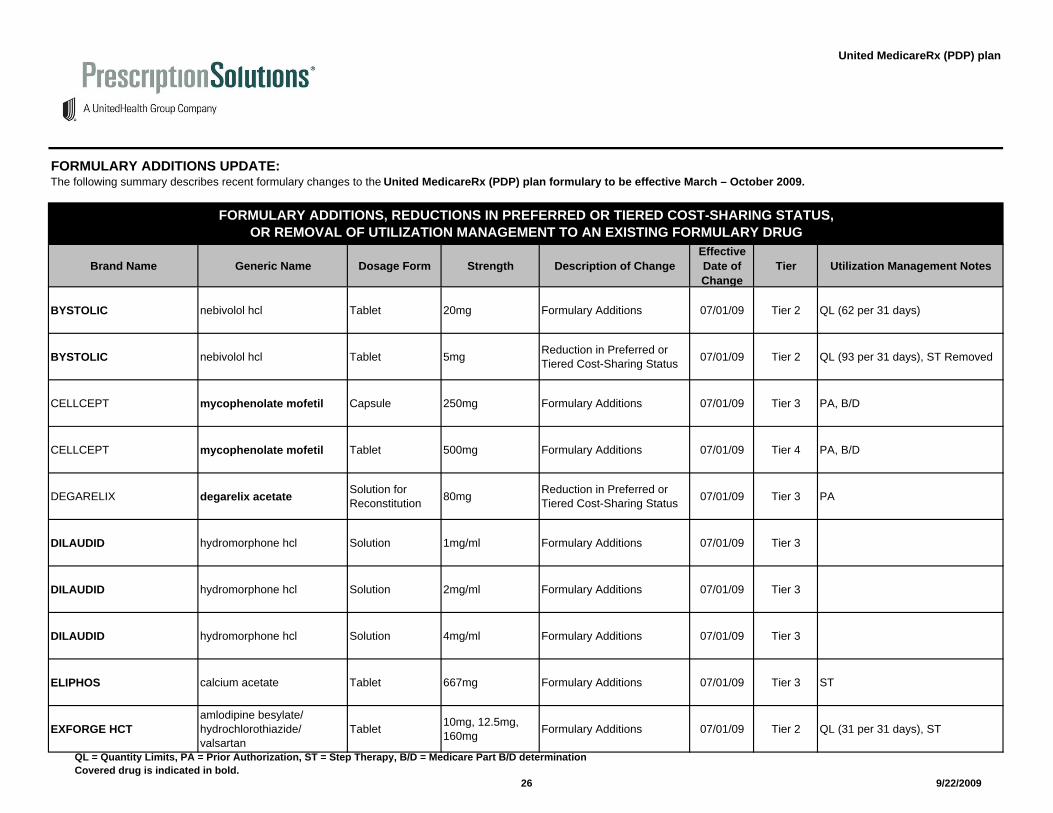
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
BYSTOLIC nebivolol hcl Tablet 20mg Formulary Additions 07/01/09 Tier 2 QL (62 per 31 days)
BYSTOLIC nebivolol hcl Tablet 5mg Reduction in Preferred or Tiered Cost-Sharing Status 07/01/09 Tier 2 QL (93 per 31 days), ST Removed
CELLCEPT mycophenolate mofetil Capsule 250mg Formulary Additions 07/01/09 Tier 3 PA, B/D
CELLCEPT mycophenolate mofetil Tablet 500mg Formulary Additions 07/01/09 Tier 4 PA, B/D
DEGARELIX degarelix acetate Solution for Reconstitution 80mg Reduction in Preferred or
Tiered Cost-Sharing Status 07/01/09 Tier 3 PA
DILAUDID hydromorphone hcl Solution 1mg/ml Formulary Additions 07/01/09 Tier 3
DILAUDID hydromorphone hcl Solution 2mg/ml Formulary Additions 07/01/09 Tier 3
DILAUDID hydromorphone hcl Solution 4mg/ml Formulary Additions 07/01/09 Tier 3
ELIPHOS calcium acetate Tablet 667mg Formulary Additions 07/01/09 Tier 3 ST
EXFORGE HCTamlodipine besylate/hydrochlorothiazide/valsartan
Tablet 10mg, 12.5mg, 160mg Formulary Additions 07/01/09 Tier 2 QL (31 per 31 days), ST
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
26
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
EXFORGE HCTamlodipine besylate/hydrochlorothiazide/valsartan
Tablet 10mg, 25mg, 160mg Formulary Additions 07/01/09 Tier 2 QL (31 per 31 days), ST
EXFORGE HCTamlodipine besylate/hydrochlorothiazide/valsartan
Tablet 10mg, 25mg, 320mg Formulary Additions 07/01/09 Tier 2 QL (31 per 31 days), ST
EXFORGE HCTamlodipine besylate/hydrochlorothiazide/valsartan
Tablet 5mg, 12.5mg, 160mg Formulary Additions 07/01/09 Tier 2 QL (31 per 31 days), ST
EXFORGE HCTamlodipine besylate/hydrochlorothiazide/valsartan
Tablet 5mg, 25mg, 160mg Formulary Additions 07/01/09 Tier 2 QL (31 per 31 days), ST
GELNIQUE oxybutynin chloride Gel 10% Formulary Additions 07/01/09 Tier 3 QL (31 per 31 days), ST
PERCOCET acetaminophen/oxycodone hcl Tablet 325mg, 2.5mg Formulary Additions 07/01/09 Tier 1
REQUIP XL ropinirole hcl 24-Hour Tablet 6mg Formulary Additions 07/01/09 Tier 3
RISPERDAL M-TAB risperidone Dispersible Tablet 0.5mg Formulary Additions 07/01/09 Tier 2
RISPERDAL M-TAB risperidone Dispersible Tablet 2mg Formulary Additions 07/01/09 Tier 2
RYZOLT tramadol hcl 24-Hour Tablet 100mg Formulary Additions 07/01/09 Tier 3 QL (31 per 31 days), PA
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
27
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
RYZOLT tramadol hcl 24-Hour Tablet 200mg Formulary Additions 07/01/09 Tier 3 QL (31 per 31 days), PA
RYZOLT tramadol hcl 24-Hour Tablet 300mg Formulary Additions 07/01/09 Tier 3 QL (31 per 31 days), PA
SAVELLA milnacipran hcl Tablet 100mg Formulary Additions 07/01/09 Tier 3 QL (62 per 31 days), PA
SAVELLA milnacipran hcl Tablet 12.5mg Formulary Additions 07/01/09 Tier 3 QL (62 per 31 days), PA
SAVELLA milnacipran hcl Tablet 25mg Formulary Additions 07/01/09 Tier 3 QL (62 per 31 days), PA
SAVELLA milnacipran hcl Tablet 50mg Formulary Additions 07/01/09 Tier 3 QL (62 per 31 days), PA
SAVELLA TITRATION PACK milnacipran hcl Miscellaneous 0 Formulary Additions 07/01/09 Tier 3 QL (55 per 31 days), PA
SIMPONI golimumab Solution 50mg/0.5ml Formulary Additions 07/01/09 Tier 4 PA
STAVUDINE stavudine Solution for Reconstitution 1mg/ml Formulary Additions 07/01/09 Tier 1
TEGRETOL-XR carbamazepine 12-Hour Tablet 200mg Formulary Additions 07/01/09 Tier 1
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
28
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
TEGRETOL-XR carbamazepine 12-Hour Tablet 400mg Formulary Additions 07/01/09 Tier 1
TOPAMAX topiramate Tablet 100mg Formulary Additions 07/01/09 Tier 1
TOPAMAX topiramate Tablet 100mg Removal of Utilization Management 07/01/09 Tier 2 PA removed
TOPAMAX topiramate Tablet 200mg Formulary Additions 07/01/09 Tier 1
TOPAMAX topiramate Tablet 200mg Removal of Utilization Management 07/01/09 Tier 2 PA removed
TOPAMAX topiramate Tablet 25mg Formulary Additions 07/01/09 Tier 1
TOPAMAX topiramate Tablet 25mg Removal of Utilization Management 07/01/09 Tier 2 PA removed
TOPAMAX topiramate Tablet 50mg Formulary Additions 07/01/09 Tier 1
TOPAMAX topiramate Tablet 50mg Removal of Utilization Management 07/01/09 Tier 2 PA removed
TOPAMAX SPRINKLE topiramate Sprinkle Capsule 15mg Formulary Additions 07/01/09 Tier 1
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
29
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
TOPAMAX SPRINKLE topiramate Sprinkle Capsule 25mg Formulary Additions 07/01/09 Tier 1
TRILIPIX choline fenofibrate Delayed Release Capsule 135mg Reduction in Preferred or
Tiered Cost-Sharing Status 07/01/09 Tier 2 PA removed
TRILIPIX choline fenofibrate Delayed Release Capsule 45mg Reduction in Preferred or
Tiered Cost-Sharing Status 07/01/09 Tier 2 PA removed
VIMPAT lacosamide Solution 200mg/20ml Formulary Additions 07/01/09 Tier 3 QL (1,240 per 31 days), PA
ADVAIR DISKUS fluticasone propionate/salmeterol xinafoate Miscellaneous 100mcg/dose,
50mcg/doseRemoval of Utilization Management 08/01/09 Tier 2 ST Removed
ADVAIR DISKUS fluticasone propionate/salmeterol xinafoate Miscellaneous 250mcg/dose,
50mcg/doseRemoval of Utilization Management 08/01/09 Tier 2 ST Removed
ADVAIR DISKUS fluticasone propionate/salmeterol xinafoate Miscellaneous 500mcg/dose,
50mcg/doseRemoval of Utilization Management 08/01/09 Tier 2 ST Removed
ADVAIR HFA fluticasone propionate/salmeterol xinafoate Aerosol 115mcg/act,
21mcg/actRemoval of Utilization Management 08/01/09 Tier 2 ST Removed
ADVAIR HFA fluticasone propionate/salmeterol xinafoate Aerosol 230mcg/act,
21mcg/actRemoval of Utilization Management 08/01/09 Tier 2 ST Removed
ADVAIR HFA fluticasone propionate/salmeterol xinafoate Aerosol 45mcg/act,
21mcg/actRemoval of Utilization Management 08/01/09 Tier 2 ST Removed
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
30
9/22/2009
United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
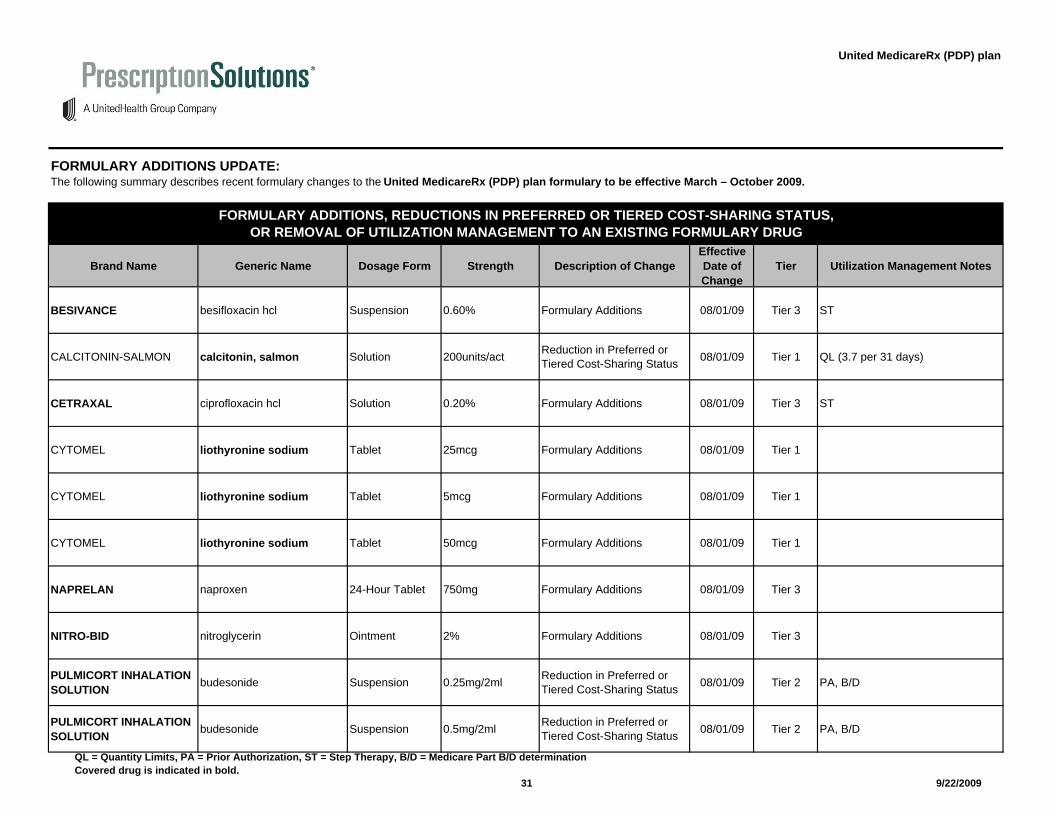
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
BESIVANCE besifloxacin hcl Suspension 0.60% Formulary Additions 08/01/09 Tier 3 ST
CALCITONIN-SALMON calcitonin, salmon Solution 200units/act Reduction in Preferred or Tiered Cost-Sharing Status 08/01/09 Tier 1 QL (3.7 per 31 days)
CETRAXAL ciprofloxacin hcl Solution 0.20% Formulary Additions 08/01/09 Tier 3 ST
CYTOMEL liothyronine sodium Tablet 25mcg Formulary Additions 08/01/09 Tier 1
CYTOMEL liothyronine sodium Tablet 5mcg Formulary Additions 08/01/09 Tier 1
CYTOMEL liothyronine sodium Tablet 50mcg Formulary Additions 08/01/09 Tier 1
NAPRELAN naproxen 24-Hour Tablet 750mg Formulary Additions 08/01/09 Tier 3
NITRO-BID nitroglycerin Ointment 2% Formulary Additions 08/01/09 Tier 3
PULMICORT INHALATION SOLUTION budesonide Suspension 0.25mg/2ml Reduction in Preferred or
Tiered Cost-Sharing Status 08/01/09 Tier 2 PA, B/D
PULMICORT INHALATION SOLUTION budesonide Suspension 0.5mg/2ml Reduction in Preferred or
Tiered Cost-Sharing Status 08/01/09 Tier 2 PA, B/D
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
31
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
SINGULAIR montelukast sodium Chewable Tablet 4mg Removal of Utilization Management 08/01/09 Tier 2 QL (31 per 31 days), ST Removed
SINGULAIR montelukast sodium Chewable Tablet 5mg Removal of Utilization Management 08/01/09 Tier 2 QL (31 per 31 days), ST Removed
SINGULAIR montelukast sodium Pack 4mg Removal of Utilization Management 08/01/09 Tier 2 QL (31 per 31 days), ST Removed
SINGULAIR montelukast sodium Tablet 10mg Removal of Utilization Management 08/01/09 Tier 2 QL (31 per 31 days), ST Removed
SONATA zaleplon Capsule 10mg Reduction in Preferred or Tiered Cost-Sharing Status 08/01/09 Tier 1 QL (62 per 31 days)
SONATA zaleplon Capsule 5mg Reduction in Preferred or Tiered Cost-Sharing Status 08/01/09 Tier 1 QL (31 per 31 days)
SYMBICORT budesonide/formoterol fumarate dihydrate Aerosol 160mcg/act,
4.5mcg/actRemoval of Utilization Management 08/01/09 Tier 2 ST Removed
SYMBICORT budesonide/formoterol fumarate dihydrate Aerosol 80mcg/act,
4.5mcg/actRemoval of Utilization Management 08/01/09 Tier 2 ST Removed
URSO 250 ursodiol Tablet 250mg Formulary Additions 08/01/09 Tier 1
URSO FORTE ursodiol Tablet 500mg Formulary Additions 08/01/09 Tier 1
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
32
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
VYVANSE lisdexamfetamine dimesylate Capsule 20mg Formulary Additions 08/01/09 Tier 3 QL (31 per 31 days)
VYVANSE lisdexamfetamine dimesylate Capsule 40mg Formulary Additions 08/01/09 Tier 3 QL (31 per 31 days)
VYVANSE lisdexamfetamine dimesylate Capsule 60mg Formulary Additions 08/01/09 Tier 3 QL (31 per 31 days)
ADCIRCA tadalafil Tablet 20mg Formulary Additions 09/01/09 Tier 4 QL (62 per 31 days), PA
APTIVUS tipranavir Solution 100mg/ml Formulary Additions 09/01/09 Tier 4
ASACOL HD mesalamine (5-aspirin) Delayed Release Tablet 800mg Formulary Additions 09/01/09 Tier 3 PA
CASODEX bicalutamide Tablet 50mg Formulary Additions 09/01/09 Tier 2
CREON amylase (diastase)/lipase (as pancrelipase)/protease
Extended Release Capsule
120,000units, 24,000units, 76,000units
Formulary Additions 09/01/09 Tier 2
CREON amylase (diastase)/lipase (as pancrelipase)/protease
Extended Release Capsule
30,000units, 6,000units, 19,000units
Formulary Additions 09/01/09 Tier 2
CREON amylase (diastase)/lipase (as pancrelipase)/protease
Extended Release Capsule
60,000units, 12,000units, 38,000units
Formulary Additions 09/01/09 Tier 2
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
33
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
EDLUAR zolpidem tartrate Sublingual Tablet 10mg Formulary Additions 09/01/09 Tier 3 QL (31 per 31 days), PA
EDLUAR zolpidem tartrate Sublingual Tablet 5mg Formulary Additions 09/01/09 Tier 3 QL (31 per 31 days), PA
ELIPHOS calcium acetate Tablet 667mg Removal of Utilization Management 09/01/09 Tier 3 ST Removed
GAVILYTE-Gpolyethylene glycol/kcl/sodium bicarbonate/nacl/sodium sulfate
Solution for Reconstitution
236gm, 2.97gm, 6.74gm, 5.86gm, 22.74gm
Formulary Additions 09/01/09 Tier 1
KIONEX sodium polystyrene sulfonate Powder 454gm Reduction in Preferred or
Tiered Cost-Sharing Status 09/01/09 Tier 1
LAMICTAL ODT lamotrigine Dispersible Tablet 100mg Formulary Additions 09/01/09 Tier 3 QL (93 per 31 days)
LAMICTAL ODT lamotrigine Dispersible Tablet 200mg Formulary Additions 09/01/09 Tier 3 QL (93 per 31 days)
LAMICTAL ODT lamotrigine Dispersible Tablet 25mg Formulary Additions 09/01/09 Tier 3 QL (31 per 31 days)
LAMICTAL ODT lamotrigine Dispersible Tablet 50mg Formulary Additions 09/01/09 Tier 3 QL (31 per 31 days)
MULTAQ dronedarone hcl Tablet 400mg Formulary Additions 09/01/09 Tier 3 PA
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
34
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
OXYCODONE HCL ER oxycodone hcl 12-Hour Tablet 10mg Reduction in Preferred or Tiered Cost-Sharing Status 09/01/09 Tier 2 QL (124 per 31 days)
OXYCODONE HCL ER oxycodone hcl 12-Hour Tablet 80mg Reduction in Preferred or Tiered Cost-Sharing Status 09/01/09 Tier 2 QL (186 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 10mg Reduction in Preferred or Tiered Cost-Sharing Status 09/01/09 Tier 2 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 15mg Reduction in Preferred or Tiered Cost-Sharing Status 09/01/09 Tier 2 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 20mg Reduction in Preferred or Tiered Cost-Sharing Status 09/01/09 Tier 2 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 20mg Reduction in Preferred or Tiered Cost-Sharing Status 09/01/09 Tier 2 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 30mg Reduction in Preferred or Tiered Cost-Sharing Status 09/01/09 Tier 2 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 40mg Reduction in Preferred or Tiered Cost-Sharing Status 09/01/09 Tier 2 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 40mg Reduction in Preferred or Tiered Cost-Sharing Status 09/01/09 Tier 2 QL (124 per 31 days)
OXYCONTIN oxycodone hcl 12-Hour Tablet 60mg Reduction in Preferred or Tiered Cost-Sharing Status 09/01/09 Tier 2 QL (124 per 31 days)
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
35
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
OXYCONTIN oxycodone hcl 12-Hour Tablet 80mg Reduction in Preferred or Tiered Cost-Sharing Status 09/01/09 Tier 2 QL (186 per 31 days)
RISPERDAL M-TAB risperidone Dispersible Tablet 3mg Formulary Additions 09/01/09 Tier 2
RISPERDAL M-TAB risperidone Dispersible Tablet 4mg Formulary Additions 09/01/09 Tier 2
RISPERIDONE ODT risperidone Dispersible Tablet 0.25mg Formulary Additions 09/01/09 Tier 2
SEROQUEL XR quetiapine fumarate 24-Hour Tablet 150mg Formulary Additions 09/01/09 Tier 2
SEROQUEL XR quetiapine fumarate 24-Hour Tablet 50mg Formulary Additions 09/01/09 Tier 2
TOPAMAX SPRINKLE topiramate Sprinkle Capsule 15mg Removal of Utilization Management 09/01/09 Tier 2 PA removed
TOPAMAX SPRINKLE topiramate Sprinkle Capsule 25mg Removal of Utilization Management 09/01/09 Tier 2 PA removed
TRI-LO-SPRINTEC ethinyl estradiol/norgestimate Tablet 0 Formulary Additions 09/01/09 Tier 1
VOLTAREN diclofenac sodium Gel 1% Reduction in Preferred or Tiered Cost-Sharing Status 09/01/09 Tier 2
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
36
9/22/2009
United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
ZETIA ezetimibe Tablet 10mg Reduction in Preferred or Tiered Cost-Sharing Status 09/01/09 Tier 2 QL (31 per 31 days)
APLENZIN bupropion hydrobromide 24-Hour Tablet 174mg Formulary Additions 10/01/09 Tier 3 QL (31 per 31 days)
APRACLONIDINE apraclonidine hcl Solution 0.50% Formulary Additions 10/01/09 Tier 2
ASTEPRO azelastine hcl Solution 137mcg/spray Reduction in Preferred or Tiered Cost-Sharing Status 10/01/09 Tier 2 QL (62 per 31 days)
AUGMENTIN amoxicillin/clavulanate potassium
Suspension for Reconstitution
250mg/5ml, 62.5mg/5ml Formulary Additions 10/01/09 Tier 1
CODEINE SULFATE codeine sulfate Tablet 15mg Formulary Additions 10/01/09 Tier 1
CODEINE SULFATE codeine sulfate Tablet 30mg Formulary Additions 10/01/09 Tier 1
CODEINE SULFATE codeine sulfate Tablet 60mg Formulary Additions 10/01/09 Tier 1
COGENTIN benztropine mesylate Solution 1mg/ml Formulary Additions 10/01/09 Tier 2
COLCRYS colchicine Tablet 0.6mg Formulary Additions 10/01/09 Tier 3
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
37
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
EFFIENT prasugrel hcl Tablet 10mg Formulary Additions 10/01/09 Tier 3 QL (36 per 31 days), PA
EFFIENT prasugrel hcl Tablet 5mg Formulary Additions 10/01/09 Tier 3 QL (31 per 31 days), PA
ELOXATIN oxaliplatin Solution 100mg/20ml Formulary Additions 10/01/09 Tier 4
ELOXATIN oxaliplatin Solution 50mg/10ml Formulary Additions 10/01/09 Tier 4
HECTOROL doxercalciferol Capsule 1mcg Formulary Additions 10/01/09 Tier 2
LAMICTAL XR lamotrigine 24-Hour Tablet 100mg Formulary Additions 10/01/09 Tier 3 QL (93 per 31 days)
LAMICTAL XR lamotrigine 24-Hour Tablet 200mg Formulary Additions 10/01/09 Tier 3 QL (93 per 31 days)
LAMICTAL XR lamotrigine 24-Hour Tablet 25mg Formulary Additions 10/01/09 Tier 3 QL (31 per 31 days)
LAMICTAL XR lamotrigine 24-Hour Tablet 50mg Formulary Additions 10/01/09 Tier 3 QL (31 per 31 days)
NEXT CHOICE levonorgestrel Tablet 0.75mg Formulary Additions 10/01/09 Tier 1
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
38
9/22/2009

United MedicareRx (PDP) plan
FORMULARY ADDITIONS UPDATE:
Brand Name Generic Name Dosage Form Strength Description of ChangeEffective Date of Change
Tier Utilization Management Notes
The following summary describes recent formulary changes to the United MedicareRx (PDP) plan formulary to be effective March – October 2009.
FORMULARY ADDITIONS, REDUCTIONS IN PREFERRED OR TIERED COST-SHARING STATUS,OR REMOVAL OF UTILIZATION MANAGEMENT TO AN EXISTING FORMULARY DRUG
NUCYNTA tapentadol hcl Tablet 100mg Formulary Additions 10/01/09 Tier 3 QL (217 per 31 days), PA
NUCYNTA tapentadol hcl Tablet 50mg Formulary Additions 10/01/09 Tier 3 QL (186 per 31 days), PA
NUCYNTA tapentadol hcl Tablet 75mg Formulary Additions 10/01/09 Tier 3 QL (186 per 31 days), PA
ONGLYZA saxagliptin hcl Tablet 2.5mg Formulary Additions 10/01/09 Tier 3 QL (31 per 31 days), ST
ONGLYZA saxagliptin hcl Tablet 5mg Formulary Additions 10/01/09 Tier 3 QL (31 per 31 days), ST
PROGRAF tacrolimus Capsule 0.5mg Formulary Additions 10/01/09 Tier 2 PA, B/D
PROGRAF tacrolimus Capsule 1mg Formulary Additions 10/01/09 Tier 2 PA, B/D
PROGRAF tacrolimus Capsule 5mg Formulary Additions 10/01/09 Tier 4 PA, B/D
ZIPSOR diclofenac potassium Capsule 25mg Formulary Additions 10/01/09 Tier 3 QL (124 per 31 days), ST
QL = Quantity Limits, PA = Prior Authorization, ST = Step Therapy, B/D = Medicare Part B/D determination Covered drug is indicated in bold.
39
9/22/2009


















