Foot Ulcer Referral Pathway - sussexcommunity.nhs.uk · Ulcer Pathway Refer Urgently Within 24...
33
Foot Ulcer Referral Pathway Helen Dooley Lead Diabetes Specialist Podiatrist
Transcript of Foot Ulcer Referral Pathway - sussexcommunity.nhs.uk · Ulcer Pathway Refer Urgently Within 24...

Foot Ulcer Referral Pathway
Helen Dooley
Lead Diabetes Specialist Podiatrist

• In 2013, almost 2.9 million people in UK diagnosed with diabetes.
• 2025 estimated that in UK > 5 million people will have diabetes
• Foot complications are common in people with diabetes. (estimated 10% will have a foot ulcer at some point)
• Amputation rates are higher in patients with diabetes than patients without diabetes. 80% of amputations are preceded by foot ulcers.
• 1 in 3 people with diabetes over age of 50 are at increased risk of developing Peripheral Arterial Disease. (PAD)

Background
• Diabetic foot problems have a significant impact on patients' quality of life; for example, reduced mobility that may lead to loss of employment, depression, and damage to or loss of limbs
• In addition, Diabetic foot problems have a significant financial impact on the NHS through outpatient costs, increased bed occupancy and prolonged stays in hospital.
NICE Inpatient Guidelines 2011

How Diabetes Affects the Lower Limbs
• Diabetes is a long term condition which can cause problems as the nerves and blood vessels become damaged.
This can affect:
- The feeling in your patient’s feet (peripheral neuropathy);
- The circulation /blood flow to your patient’s feet (ischaemia)
• These changes can be gradual and may go unnoticed initially. This is why it is essential your patient has their feet screened regularly, in accordance with their stratified level of risk.
• Controlling blood sugars, cholesterol levels and blood pressure is essential to reduce the risk of limb/life threatening problems associated with diabetes.
• In addition quitting smoking, undertaking regular exercise and controlling weight will also help to reduce risks.


Screening And
Classification

• Screening is a process that categorises people into mutually exclusive groups and will give a reasonably good indication of the likelihood/risk of a person with diabetes developing a foot complications.
• Assessment is a much more intense and complex
process by which a diagnosis is reached and treatment/management is initiated
Foot screening and assessment

The aim of carrying out a foot screening is to identify the presence of risk factors for diabetic foot complications which could lead to ulceration.
Neuropathy, Peripheral Arterial
Disease, Significant structural
abnormalities, Significant callus,
previous ulceration inability to self care.
Lower Limb Assessment and Foot Screening
Assessment also includes checking for infection .
Absent pulses , Previous amputation

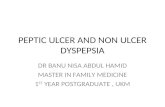
Classification of foot risk
• Active
• High Risk
• Moderate Risk
• Low Risk

Any of the following
• Ulceration • Spreading infection • Critical Limb ischaemia • Gangrene • Suspicion of an acute Charcot Arthropathy or an
unexplained hot, red, swollen foot with or without pain
Any of the following
• Previous Ulceration • Previous Amputation • On Renal replacement therapy
Any of the following
• Neuropathy plus non-critical limb ischaemia • Neuropathy plus callus and or deformity • Non-Critical Limb ischaemia plus callus and or
deformity
Any of the following • Deformity • Neuropathy • non-critical limb ischaemia
MODERATE
LOW
HIGH
HIGH
ACTIVE
No
No
No
Yes
Yes
Yes
Yes
No
Risk Stratification decision tree (based on the 2016 NICE guideline)
Risk Category
Jarl
G (
20
18
) Dec
isio
n t
ree
s fo
r ri
sk s
trat
ific
atio
n o
f th
e d
iab
etic
fo
ot.
DFJ
21
(4):
21
8-2
3

Refer all patients to Diabetes Care for You
Consider referral to Diabetes Care for You
.
Low Risk remain in Primary care for annual review.
• Ulceration • Infection • Critical ischaemia or gangrene • neuropathic pain • Unexplained red, hot, swollen foot
(Suspected Charcot or #)
Action

Related to diseases that affect circulation and sensation.
Foot ulcers
Definition Active ulceration
"a full thickness wound, i.e. a wound penetrating through the dermis, below the ankle in a diabetic patient, irrespective of duration". International Working Group on the Diabetic Foot
2005 (IWGDF)

Diabetic foot ulceration is principally associated with:
PAD and peripheral neuropathy, often in combination
Other factors associated with increased risk include:
Previous amputation
Previous ulceration
The presence of significant callus
The presence of significant structural abnormality

Impact of Neuropathy
• Signs and symptoms may be minimal
• Nevertheless pathology proceeds rapidly
• The end stage of tissue death is quickly reached
• Window of opportunity is limited

Neuropathic Ulcer

Ischaemic ulcers

Ischaemia

Critical Ischaemia

Previous Amputation

Infection Control

Infection
• Laboratory Research(In vitro) evidence suggests that in the patient with diabetes the chemicals and cells which fight infection are compromised and impaired.
• In addition PAD reduces the penetration of leukocytes(Blood cells) and antibiotics to the infected sites

Infection. Why are diabetes ulcers different
Prolonged periods of hyperglycaemia lead to impairment in immune function:
• A decrease in Chemotaxis at the site of infection.
• A decrease in the ability of the phagocytes to destroy bacteria.
• Decreased intracellular killing of bacteria.

an area that has previously been ulcerated but has subsequently healed. After ulceration the affected area never repairs itself completely and only returns to 70% of tensile strength. This area is always vulnerable to future ulcerations. Previous ulceration is the highest risk factor for future ulceration. (FRAME)
Previous ulceration

Diabetes Care For You Ulcer Pathway
Refer Urgently Within 24 hours to Level 4 (secondary care) Clinic
Ulcer With spreading infection/ Swelling / discolouration/ >2cm Cellulitis
Any Arterial Ulcer (Below Ankle) Including Gangrene / necrosis
Refer Urgently within 24 hours to Diabetes Care For you via ERS
Non –Infected , Neuropathic Ulcers
(Below Ankle)
Neuropathic Ulcers with local infection (<2cm cellulitis /no deep probe/no bone
visible/ no systemic symptoms
Take Swab Start Antibiotics

Referral Form – Essential information
HW/LH Referral form. Low Risk may be treated in B&H

Where do I refer this chap?
• Type 2 Diabetes
• 49 year old gentleman
• Extremely Painful Left hallux – trauma
• Presented GP surgery
• Ingrown toe nail /Fungal nail
• Chronic Pain Left Hallux

Palpable Pulses
All sites detected (10g monofilament)
Low risk
Pain Red infection
Active Foot Problem
MRI Left foot localised bone marrow oedema in the terminal tuft of the distal phalanx of the hallux. In the absence of fracture and disproportionate pain raises the suspicion of a deep infection, confirmed on MRI scan.

GP
Antibiotic therapy
X-ray
General Podiatry MSK Foot &Ankle
MRI
DCFY Podiatrist Ulcer under hallux nail. Osteomyelitis
Left hallux
Management
Ulcer
Antibiotic Therapy

Referral Form – Essential information
HW/LH Referral form. Low Risk may be treated in B&H

Final Points • Screen and Classify
• Refer early
• Controlling blood sugars, cholesterol levels and blood pressure is essential to reduce the risk of limb/life threatening problems associated with diabetes.
• In addition quitting smoking, undertaking regular exercise and controlling weight will also help to reduce risks.
• Provide foot health education.

Skin care
Nail care
Foot wear
Check feet
Maintain the boat to weather the storm


Questions