
Folate and methionine metabolism in autism: a systematic ... 2010 - Folate and methionine...Folate...
24
Folate and methionine metabolism in autism: a systematic review 1,2 Penelope AE Main, Manya TAngley, Philip Thomas, Catherine E O’Doherty, and Michael Fenech ABSTRACT Background: Autism is a complex neurodevelopmental disorder that is increasingly being recognized as a public health issue. Re- cent evidence has emerged that children with autism may have altered folate or methionine metabolism, which suggests the fo- late-methionine cycle may play a key role in the etiology of autism. Objective: The objective was to conduct a systematic review to examine the evidence for the involvement of alterations in folate- methionine metabolism in the etiology of autism. Design: A systematic literature review was conducted of studies reporting data for metabolites, interventions, or genes of the fo- late-methionine pathway in autism. Eighteen studies met the inclu- sion criteria, 17 of which provided data on metabolites, 5 on interventions, and 6 on genes and their related polymorphisms. Results: The findings of the review were conflicting. The variance in results can be attributed to heterogeneity between subjects with autism, sampling issues, and the wide range of analytic techniques used. Most genetic studies were inadequately powered to provide more than an indication of likely genetic relations. Conclusions: The review concluded that further research is required with appropriately standardized and adequately powered study de- signs before any definitive conclusions can be made about the role for a dysfunctional folate-methionine pathway in the etiology of autism. There is also a need to determine whether functional bene- fits occur when correcting apparent deficits in folate-methionine metabolism in children with autism. Am J Clin Nutr 2010;91:1598–620. INTRODUCTION Autism spectrum disorders (ASDs) are increasingly recog- nized as a public health issue. ASDs are characterized by impairments in reciprocal social interaction and communication and restricted interests as well as repetitive stereotypic behaviors (1). The term autism spectrum disorder encompasses autistic disorder, Asperger disorder, and pervasive development disorders– not otherwise specified. Over the past 20 y, the number of di- agnosed cases has significantly increased. This has been partly attributed to broadening of the diagnostic criteria and increased community awareness (2). Recent well-designed studies using whole-genome scanning methods indicate a key role for genetic factors in the etiology of autism (3–5). These studies have shown that multiple genes contribute to the wide range of symptoms observed in autism (6). A common aberration is not consistently seen in all autism cases, which suggests that it is a cluster of disorders with each having a distinct pathophysiology. In addition, environmental factors, including heavy metal toxicity (7–9), subclinical viral infections (10), and gastrointestinal pathology (reviewed in references 11 and 12), have also been identified as contributing to autism. Folate and methionine metabolism and autism A dysfunctional folate-methionine pathway has been identified in many individuals with autism. This pathway is crucial for DNA synthesis (13), DNA methylation (14), and cellular redox balance (15). As shown in Figure 1, methionine, an essential amino acid, is converted to S-adenosyl-methionine (SAM), the body’s main methyl group donor, which is converted to S-adenosyl- homocysteine (SAH) during methylation reactions. Thus, plasma SAM:SAH indicates methylation status. SAH is later hydrolyzed to homocysteine in a reversible reaction releasing adenosine. Homocysteine formed from methylation reactions is metab- olized by 1 of 2 pathways. The first is the trans-sulfuration pathway, which involves the irreversible conversion of homo- cysteine to cysteine through cystathionine. Cysteine is the rate- limiting amino acid for the synthesis of glutathione, which plays a key role in detoxification processes (16). Total glutathione: oxidized glutathione in plasma is an indicator for oxidative stress (17). The second pathway involves the remethylation of homocysteine to methionine, which is carried out by methionine synthase (MS) in most tissues. A shown in Figure 2, the methyl group for MS is donated by 5-methyltetrahydrofolate (5-MTHF), which is converted to tetrahydrofolate (THF). THF is methylated to become 5,10-methylene tetrahydrofolate (5,10-MTHF) either by serine hydroxyl-methyltransferase or a series of 3 reactions catalyzed by methyltetrahydrofolate dehydrogenase (MTHFD-1). Most 5,10-MTHF is metabolized to 5-MTHF, the only form of folate used in the central nervous system (CNS) and the main form of folate in the blood, by methylene tetrahydrofolate re- ductase (MTHFR). The remaining 5,10-MTHF is converted to dihydrofolate (DHF) by thymidine synthase in the synthesis of thymidylate, which is required for DNA replication and may be converted back to THF by dihydrofolate reductase (DHFR). 1 From the Autism Research Group, Sansom Institute, University of South Australia, Adelaide, Australia (PAEM, CEO, and MTA), and Food and Nu- tritional Science, Commonwealth Scientific and Industrial Research Organi- sation, Adelaide, Australia (MF and PT). 2 Address correspondence to PAE Main, Food and Nutritional Science, CSIRO, Gate 13 Kintore Street, Adelaide, South Australia 5000. E-mail: [email protected]. Received November 30, 2009. Accepted for publication March 4, 2010. First published online April 21, 2010; doi: 10.3945/ajcn.2009.29002. 1598 Am J Clin Nutr 2010;91:1598–620. Printed in USA. Ó 2010 American Society for Nutrition by guest on May 11, 2016 ajcn.nutrition.org Downloaded from 29002.DC1.html http://ajcn.nutrition.org/content/suppl/2010/05/19/ajcn.2009. Supplemental Material can be found at: by guest on May 11, 2016 ajcn.nutrition.org Downloaded from by guest on May 11, 2016 ajcn.nutrition.org Downloaded from
Transcript of Folate and methionine metabolism in autism: a systematic ... 2010 - Folate and methionine...Folate...

Folate and methionine metabolism in autism: a systematic review1,2
Penelope AE Main, Manya T Angley, Philip Thomas, Catherine E O’Doherty, and Michael Fenech
ABSTRACTBackground: Autism is a complex neurodevelopmental disorderthat is increasingly being recognized as a public health issue. Re-cent evidence has emerged that children with autism may havealtered folate or methionine metabolism, which suggests the fo-late-methionine cycle may play a key role in the etiology of autism.Objective: The objective was to conduct a systematic review toexamine the evidence for the involvement of alterations in folate-methionine metabolism in the etiology of autism.Design: A systematic literature review was conducted of studiesreporting data for metabolites, interventions, or genes of the fo-late-methionine pathway in autism. Eighteen studies met the inclu-sion criteria, 17 of which provided data on metabolites, 5 oninterventions, and 6 on genes and their related polymorphisms.Results: The findings of the review were conflicting. The variancein results can be attributed to heterogeneity between subjects withautism, sampling issues, and the wide range of analytic techniquesused. Most genetic studies were inadequately powered to providemore than an indication of likely genetic relations.Conclusions: The review concluded that further research is requiredwith appropriately standardized and adequately powered study de-signs before any definitive conclusions can be made about the rolefor a dysfunctional folate-methionine pathway in the etiology ofautism. There is also a need to determine whether functional bene-fits occur when correcting apparent deficits in folate-methioninemetabolism in children with autism. Am J Clin Nutr2010;91:1598–620.
INTRODUCTION
Autism spectrum disorders (ASDs) are increasingly recog-nized as a public health issue. ASDs are characterized byimpairments in reciprocal social interaction and communicationand restricted interests as well as repetitive stereotypic behaviors(1). The term autism spectrum disorder encompasses autisticdisorder, Asperger disorder, and pervasive development disorders–not otherwise specified. Over the past 20 y, the number of di-agnosed cases has significantly increased. This has been partlyattributed to broadening of the diagnostic criteria and increasedcommunity awareness (2).
Recent well-designed studies using whole-genome scanningmethods indicate a key role for genetic factors in the etiology ofautism (3–5). These studies have shown that multiple genescontribute to the wide range of symptoms observed in autism (6).A common aberration is not consistently seen in all autism cases,which suggests that it is a cluster of disorders with each havinga distinct pathophysiology. In addition, environmental factors,including heavy metal toxicity (7–9), subclinical viral infections
(10), and gastrointestinal pathology (reviewed in references 11and 12), have also been identified as contributing to autism.
Folate and methionine metabolism and autism
A dysfunctional folate-methionine pathway has been identifiedin many individuals with autism. This pathway is crucial for DNAsynthesis (13), DNA methylation (14), and cellular redox balance(15). As shown in Figure 1, methionine, an essential aminoacid, is converted to S-adenosyl-methionine (SAM), the body’smain methyl group donor, which is converted to S-adenosyl-homocysteine (SAH) during methylation reactions. Thus,plasma SAM:SAH indicates methylation status. SAH is laterhydrolyzed to homocysteine in a reversible reaction releasingadenosine.
Homocysteine formed from methylation reactions is metab-olized by 1 of 2 pathways. The first is the trans-sulfurationpathway, which involves the irreversible conversion of homo-cysteine to cysteine through cystathionine. Cysteine is the rate-limiting amino acid for the synthesis of glutathione, which playsa key role in detoxification processes (16). Total glutathione:oxidized glutathione in plasma is an indicator for oxidativestress (17). The second pathway involves the remethylation ofhomocysteine to methionine, which is carried out by methioninesynthase (MS) in most tissues.
A shown in Figure 2, the methyl group for MS is donatedby 5-methyltetrahydrofolate (5-MTHF), which is convertedto tetrahydrofolate (THF). THF is methylated to become5,10-methylene tetrahydrofolate (5,10-MTHF) either by serinehydroxyl-methyltransferase or a series of 3 reactions catalyzedby methyltetrahydrofolate dehydrogenase (MTHFD-1).
Most 5,10-MTHF is metabolized to 5-MTHF, the only form offolate used in the central nervous system (CNS) and the mainform of folate in the blood, by methylene tetrahydrofolate re-ductase (MTHFR). The remaining 5,10-MTHF is converted todihydrofolate (DHF) by thymidine synthase in the synthesis ofthymidylate, which is required for DNA replication and may beconverted back to THF by dihydrofolate reductase (DHFR).
1 From the Autism Research Group, Sansom Institute, University of South
Australia, Adelaide, Australia (PAEM, CEO, and MTA), and Food and Nu-
tritional Science, Commonwealth Scientific and Industrial Research Organi-
sation, Adelaide, Australia (MF and PT).2 Address correspondence to PAE Main, Food and Nutritional Science,
CSIRO, Gate 13 Kintore Street, Adelaide, South Australia 5000. E-mail:
Received November 30, 2009. Accepted for publication March 4, 2010.
First published online April 21, 2010; doi: 10.3945/ajcn.2009.29002.
1598 Am J Clin Nutr 2010;91:1598–620. Printed in USA. � 2010 American Society for Nutrition
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from
29002.DC1.html http://ajcn.nutrition.org/content/suppl/2010/05/19/ajcn.2009.Supplemental Material can be found at:
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from
by guest on M
ay 11, 2016ajcn.nutrition.org
Dow
nloaded from

Significant cytogenetic alterations in both lymphocytes and/orbuccal cells have been found in other neurologic conditions,including Down syndrome, Parkinson disease, Alzheimer dis-ease, and schizophrenia (18–21). Although it is plausible thatfolate deficiency increases chromosomal instability (22), there iscurrently no direct evidence that chromosomal DNA damage isthe cause of neurodegenerative disease. Other plausible mech-anisms for a role of folate deficiency in neurodegenerativediseases include impaired mitochondrial function due to mito-chondrial DNA deletions, reduced availability of methyl groupsfrom folate for neurotransmitter synthesis, and reduced pro-liferative potential of regenerative cells in critical regions of thebrain caused by diminished nucleotide synthesis (23, 24).
Folate transport into the CNS
Folate transport through the choroid plexus is mainly mediatedby a family of folate receptor (FR) proteins, and the reducedfolate carrier 1 (RFC-1) (Figure 3) FR proteins located on theplasma side of the choroid plexus bind and transfer folate viaendocytosis into the intracellular compartment where it is con-centrated. The RFC-1 is located on the cerebrospinal fluid (CSF)side of the choroid plexus, where it facilitates transport of theconcentrated folate into the CSF. Defective folate transport intothe CNS has been linked with cerebral folate deficiency (CFD),a condition associated with developmental delays (with orwithout autistic features), providing plausibility for involvementof the folate-methionine pathway in autism (reviewed in refer-ence 25). This article systematically reviews the evidence fora role of the folate-methionine pathway in the etiology of au-tism, because, to our knowledge, no such article has been pub-lished to date.
METHODS
A systematic literature review was conducted to identify fo-late-methionine pathway studies in autism, including metaboliteconcentrations in blood, interventions directed at normalizinga dysfunctional pathway and genes, and related polymorphismsof the pathway. The search used the following electronic data-bases (all databases were accessed through our institution’ssubscription, with the exception of The Cochrane Library):Embase, Medline, Cinahl, Scopus, Web of Science, InternationalPharmaceutical Abstracts, and the Cochrane database (availablefrom http://www.thecochranelibrary.com). The reference lists forall obtained studies were hand-searched for additional studies.
The criteria for study inclusion were as follows: 1) studies inchildren with autistic disorder as described in the Diagnosticand Statistical Manual of Mental Disorders: Revised Text(DSM-IV-R) (1) or diagnosed by using a standard diagnosticinstrument, eg, the Childhood Autism Rating Scale (CARS)(26); and 2) studies including data for receptors, carriers, me-tabolites, cofactors or genes of the folate-methionine pathway,and/or 3) interventions using metabolites or cofactors of thefolate-methionine pathway. Only full-text English-language ar-ticles published between 1978 and October 2008 were included.
All potential studies identified were independently evaluatedfor inclusion by 2 primary reviewers (PM and MA). The primaryreviewers were not blinded to the authors, institutions or source ofpublication at any time during the selection process. Disagree-ments about the inclusion/exclusion of studies were discussedand consensus achieved. Provision was made for a third reviewerif consensus was unattainable but did not prove necessary. A levelof evidence was assigned to each study by using the Australian
FIGURE 2. Folate cycle. THF, tetrahydrofolate; 5-methyl-THF, 5-methyl-tetrahydrofolate; 5,10-MTHF, 5,10-methylene-tetrahydrofolate; DHF,dihydrofolate; 10-formyl-THF, 10-formyl-tetrahydrofolate; 5,10-methenyl-THF, 5,10-methenyl-tetrahydrofolate; dUMP, deoxy-uracil-monophosphate;dTMP, deoxy-thymidine-monophosphate; cSHMT, cyclo-serine-hydroxymethyl transferase; MTHFR, 5,10-methylene tetrahydrofolate reductase;MS, methionine synthase; MSR, methionine synthase reductase; MTHFD1,5,10-methylenetetrahydrofolate dehydrogenase/5,10-methenyl-tetrahydrofolatecyclohydrolase/10-formyl-tetrahydrofolate synthetase; DHFR, dihydrofolatereductase; TS, thymidine synthase; B6, vitamin B-6; Vit. B12, vitamin B-12.
FIGURE 3. Folate transport across the choroid plexus. 5-MTHF, 5-methyl-tetrahydrofolate; FRa and b, folate receptor a and b; RFC-1,reduced folate carrier-1; CSF, cerebral spinal fluid.
FIGURE 1. Methionine cycle and trans-sulfuration pathway. SAM,S-adenosyl-methionine; SAH, S-adenosyl-homocysteine; THF, tetrahydrofolate;5-MTHF, 5 methyl-tetrahydrofolate; R, DNA or protein; R-CH3, methylatedDNA or protein; MAT, methionine adenosine transferase; MS, methioninesynthase; BHMT, betaine homocysteine methyltransferase; CBS, cystathioneB synthase; DMG, dimethylglycine; Vit. B6, vitamin B-6; Vit. B12, vitaminB-12.
FOLATE-METHIONINE PATHWAY AND AUTISM 1599
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

National Health and Medical Research Council criteria (27)(Table 1). The large number of variables and case definitionsacross studies prohibited statistical assessment of heterogeneityand meta-analysis.
RESULTS
Forty-nine abstracts were identified via the electronic andhand-search strategy. Of these abstracts, 31 were ineligible forinclusion because they did not include data about the folate-methionine pathway, data about children with autism was notpresented separately from other disorders, and/or because theywere not written in the English language. Eighteen studies metthe inclusion criteria, of which 17 provided data on metabolites orcofactors of the folate-methionine pathway, 5 provided the resultsof interventions, and 6 included genetic data.
A summary of studies that measured metabolites and/orcofactors of the folate-methionine pathway is shown in Table 2.Three studies presented data for multiple metabolites of thefolate-methionine and trans-sulfuration pathways (28–30). Bothstudies by James et al (28, 29) showed that, with the exceptionof SAH and reduced glutathione, specific metabolites of themethionine and trans-sulfuration pathways were significantlydecreased. The metabolites measured were methionine, SAM,homocysteine, cysteine, and total glutathione. The authorsconcluded that the resultant decrease in the SAM:SAH ratioindicates a decreased capacity for methylation in children withautism, and the total glutathione:oxidized glutathione ratiosuggests that oxidative stress may play a role in the etiology ofautism. In contrast, the study by Suh et al (30) showed no sig-nificant change in plasma metabolites of the folate-methionineand trans-sulfuration pathways; lower concentrations of SAM,cysteine, and glutathione; and significantly higher homocysteineconcentrations in peripheral leukocytes when children with au-tism were compared with controls. The discrepancies may havebeen due to differences in methodology. James et al’s studies
(28, 29) used HPLC/electrocoulometric detection and the otherused liquid chromatography-linked tandem mass spectrometry.
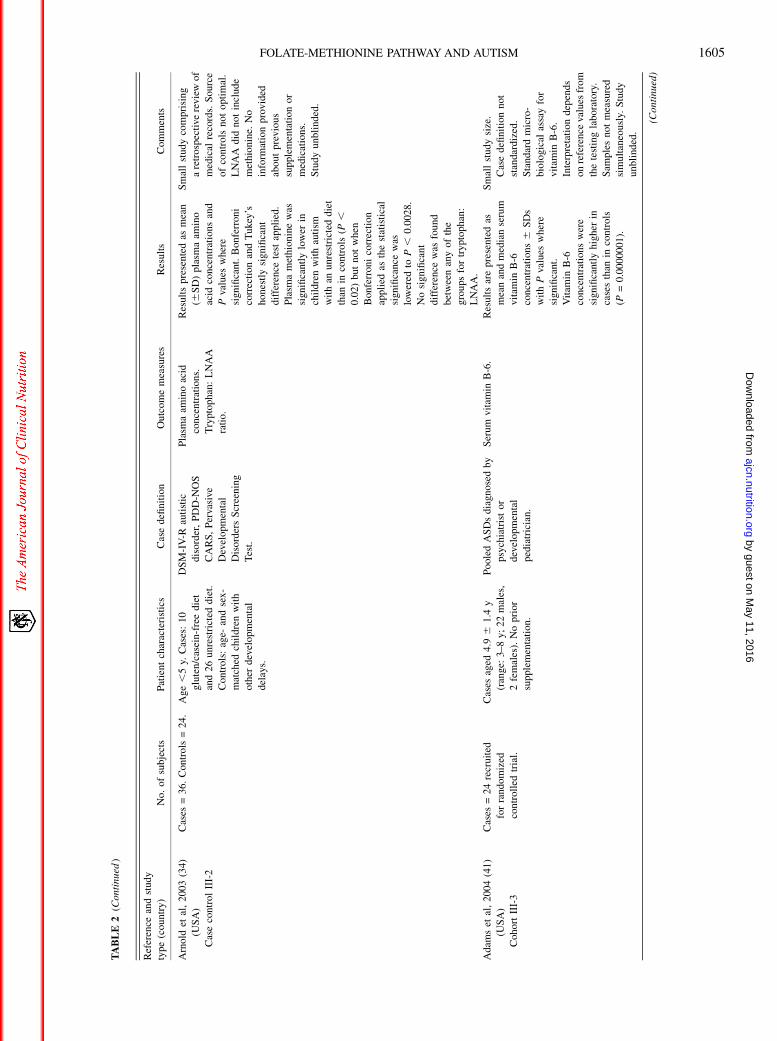
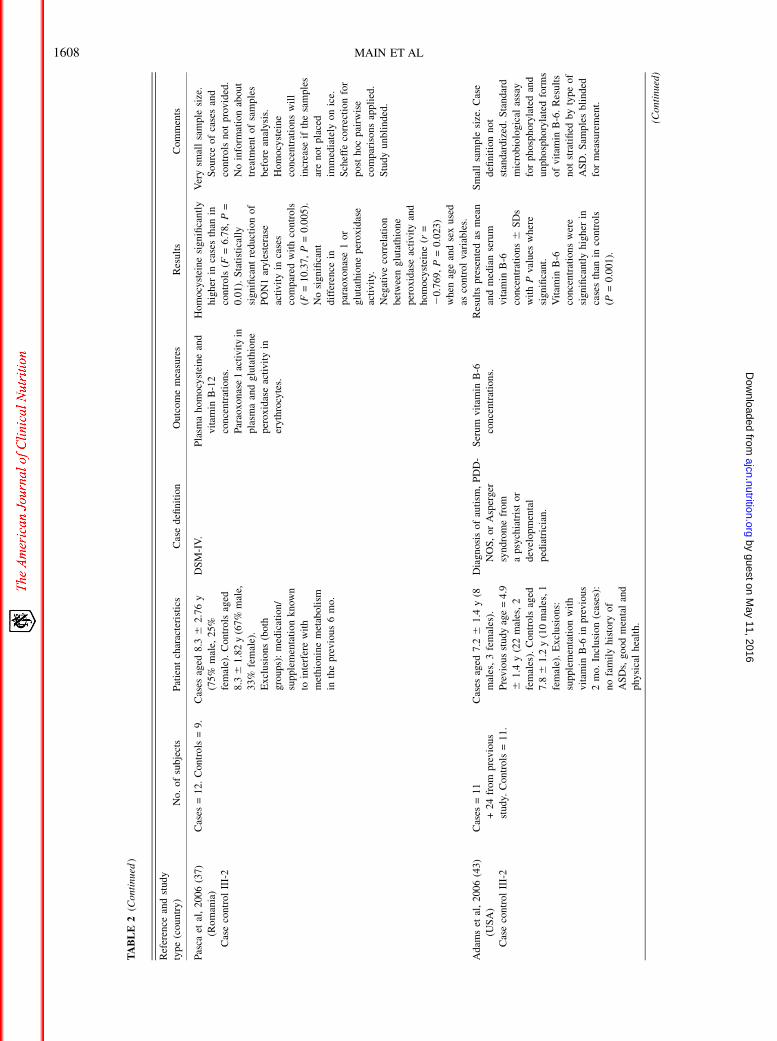
Eleven studies measured plasma concentrations of amino acidsassociated with the folate-methionine pathway (28–38). Thefindings were inconsistent between studies. For example, 3reported low methionine in plasma of children with autism (28–30), 2 others reported no association (30, 32), and anotherreported significantly increased concentrations (31). Threestudies reported low concentrations of cysteine (28, 29, 31),whereas others reported no significant differences (30, 32) and,although James et al (28, 29) reported a decreased concentrationof homocysteine, 2 later studies reported significantly increasedconcentrations of homocysteine (37, 38) and 2 reported nosignificant difference (30, 36).
Ten studies examined cofactors required for folate-methioninemetabolism (31, 35–37, 39–44). Of these, 4 studies detectedsignificantly higher serum vitamin B-6 in children with autismthan in controls (31, 39, 41, 43), of which one also found elevatedserum concentrations of riboflavin (39). In addition, a case studyreported high vitamin B-12 in a child with autism and CFD (35);however, a later study found no significant difference in vitaminB-12 between children with autism and controls (37). None of thestudies found any significant difference in serum or erythrocytefolate between children with autism and controls.
Five studies reported significantly low CSF folate concen-trations together with normal serum folate concentrations inchildren with autism (35, 38, 40, 42, 44). High titers of FR1antibodies were found in 19 of 23 children with autism and atleast one symptom of CFD (44).
The findings of the 5 studies that reported the outcome ofinterventions (28, 35, 38, 42, 44) are presented in Table 3. A pilotstudy conducted in a small group of children with autismshowed that supplementation with folinic acid and betaine for 3mo significantly normalized the methionine pathway metaboliteprofile in plasma, particularly the SAM:SAH ratio (28). Theaddition of vitamin B-12 to this regimen for an additional 1 moin a subset of participants acted mainly on the trans-sulfurationpathway, improving the total glutathione:oxidized glutathioneratio, although it also led to further normalization of methioninemetabolites. Quantitative psychometric measures were not,however, included in the study.
The remaining studies reported the effect of treatment withfolinic acid on low CSF concentrations of 5-MTHF in childrenwith autism and at least one symptom of CFD (35, 37, 42, 44).The most autism-specific of these studies showed that treatmentwith folinic acid resulted in improved autistic, motor, and otherneurologic symptoms in young children (,3.5 y) and im-provements in motor and neurologic symptoms in older chil-dren, although there was no change in autistic symptoms in theolder age group (44).
Six studies examined genes of the folate-methionine pathwayor folate transport system in children with autism, which aresummarized in Table 4. The results from these studies wereinconsistent. For example, an early study found that the T alleleof the MTHFR 677C/T polymorphism was of significantlyhigher frequency in autistic patients than in controls (P ,0.0001) (45). The homozygote MTHFR 1298A/C genotype(P = 0.0005) and compound MTHFR 677C/T/1298A/Cgenotype (P = 0.01) were also significantly associated with thecondition. A subsequent larger study, however, failed to confirm
TABLE 1
Australian National Health and Medical Research Council designated
levels of evidence1
Level of
evidence Description
I Evidence obtained from a systematic review of all relevant
randomized controlled trials.
II Evidence obtained from at least one properly designed
randomized controlled trial.
III-1 Evidence obtained from well-designed pseudo-randomized
controlled trials (alternate allocation or some other
method).
III-2 Evidence obtained from comparative studies with
concurrent controls and allocation not randomized
(cohort studies), case control studies, or interrupted time
series with control group.
III-3 Evidence obtained from comparative studies with historical
control, �2 single-arm studies, or interrupted time series
without a parallel control group.
IV Evidence obtained from a case series, either posttest or
pretest and posttest.
1 Data from reference 27.
1600 MAIN ET AL
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

TABLE2
Stu
die
sof
met
aboli
tes
or
cofa
ctors
of
the
fola
te-m
ethio
nin
epat
hway
inch
ildre
nw
ith
auti
sm1
Ref
eren
cean
dst
udy
type
(countr
y)
No
.o
fsu
bje
cts
Pat
ient
char
acte
rist
ics
Cas
edefi
nit
ion
Outc
ome
mea
sure
sR
esult
sC
omm
ents
San
kar,
19
79
(39
)(U
SA
)
Cas
eco
ntr
ol
III-
3
Cas
es=
19
.C
ontr
ols
=7
8
sch
izop
hre
nic
,6
beh
avio
ral
dis
turb
ance
,
12
psy
cho
sis,
5
met
abo
lic
defi
cien
cy.
Mal
e,ag
e=
5–
16
y,
adm
itte
dto
Chi
ld
Psy
chia
tric
Res
earc
h
Un
it,
Cre
edm
ore
Sta
te
Ho
spit
al,
US
A.
Incl
usi
on
:N
o
sup
plem
enta
tio
nfo
r3
wk
bef
ore
the
stu
dy.
On
set
from
infa
ncy
wit
h
seve
reem
otio
nal
iso
lati
on
;fa
ilu
reto
rela
teto
ob
ject
san
d
per
son
s;fa
ilu
reto
dev
elo
psp
eech
and
com
mun
icat
ion
.If
spee
chp
rese
nt,
itis
an
on
com
mu
nica
tive
typ
e.S
tere
oty
pyo
f
mo
tor
beh
avio
r.
Ser
um
foli
cac
id,r
ibo
flav
in,
vit
amin
B-6
,an
dv
itam
in
Cco
nce
ntr
atio
ns.
Res
ults
pre
sen
ted
asm
ean
seru
mco
nce
ntr
atio
ns
for
each
vit
amin
6S
D
com
par
edw
ith
conce
ntr
atio
ns
of
pu
bli
shed
no
rmal
ran
ge.
No
mea
sure
so
f
stat
isti
cal
sign
ifica
nce.
Ser
um
rib
ofl
avin
(P=
0.0
029
)an
dv
itam
inB
-6
(P,
0.0
001
)w
ere
sign
ifica
ntly
hig
her
in
case
sth
anin
con
tro
ls.
Stu
dy
was
un
der
tak
en
bef
ore
ast
anda
rdiz
ed
defi
nit
ion
of
auti
smw
as
avai
lab
le.
Sta
nd
ard
ph
oto
met
ric
and
mic
rob
iolo
gic
alas
say
s
use
d;
how
ever
,th
e
met
ho
du
sed
to
det
erm
ine
vit
amin
B-6
dif
fere
dfo
rca
ses
and
con
tro
ls.
Was
ho
utti
me
for
fola
teis
4m
o;
ther
efo
re,
the
incl
usi
on
crit
eria
do
no
tp
recl
ude
inte
rfer
ence
fro
mp
rio
r
fola
tein
ges
tio
n.
Co
nd
uct
edb
efo
re
reco
mm
enda
tio
ns
for
fola
tesu
ppl
emen
tati
on
.
Pre
vio
us
die
tary
inta
ke
and
med
icat
ions
wer
e
no
tco
nsi
der
ed.
Stu
dy
un
bli
nded
.
(Co
nti
nu
ed)
FOLATE-METHIONINE PATHWAY AND AUTISM 1601
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from
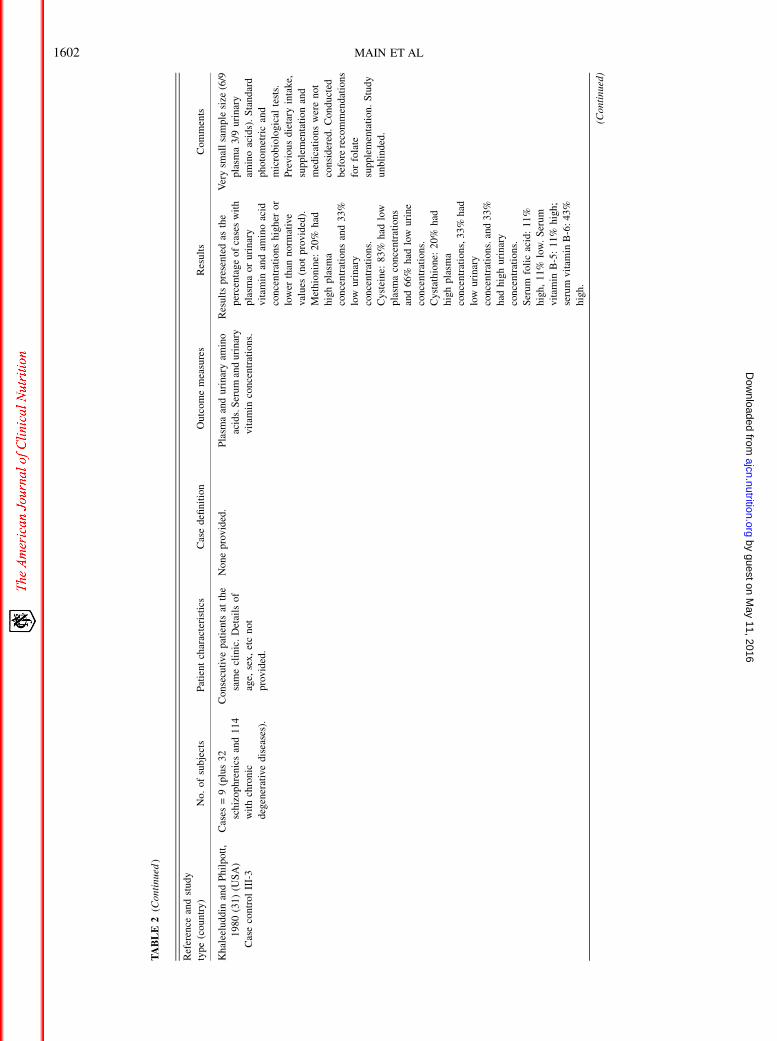
TABLE2
(Co
nti
nu
ed)
Ref
eren
cean
dst
ud
y
type
(countr
y)
No.
of
subje
cts
Pat
ient
char
acte
rist
ics
Cas
edefi
nit
ion
Outc
ome
mea
sure
sR
esult
sC
omm
ents
Kh
alee
lud
din
and
Ph
ilp
ott
,
19
80
(31
)(U
SA
)
Cas
eco
ntr
ol
III-
3
Cas
es=
9(p
lus
32
sch
izo
ph
ren
ics
and
11
4
wit
hch
ron
ic
deg
ener
ativ
edis
ease
s).
Co
nse
cuti
vep
atie
nts
atth
e
sam
ecl
inic
.D
etai
lso
f
age,
sex
,et
cn
ot
pro
vid
ed.
No
ne
pro
vid
ed.
Pla
sma
and
uri
nar
yam
ino
acid
s.S
eru
man
du
rin
ary
vit
amin
con
cen
trat
ion
s.
Res
ults
pre
sen
ted
asth
e
per
cen
tag
eo
fca
ses
wit
h
pla
sma
or
uri
nar
y
vit
amin
and
amin
oac
id
con
cen
trat
ion
sh
igh
ero
r
low
erth
ann
orm
ativ
e
valu
es(n
ot
pro
vid
ed).
Met
hio
nin
e:2
0%
had
hig
hp
lasm
a
con
cen
trat
ion
san
d3
3%
low
uri
nar
y
con
cen
trat
ion
s.
Cys
tein
e:8
3%
had
low
pla
sma
con
cen
trat
ion
s
and
66
%h
adlo
wu
rin
e
con
cen
trat
ion
s.
Cys
tath
ion
e:2
0%
had
hig
hp
lasm
a
con
cen
trat
ion
s,3
3%
had
low
uri
nar
y
con
cen
trat
ion
s.an
d3
3%
had
hig
hu
rin
ary
con
cen
trat
ion
s.
Ser
um
foli
cac
id:
11
%
hig
h,
11
%lo
w.
Ser
um
vit
amin
B-5
:1
1%
hig
h;
seru
mv
itam
inB
-6:
43
%
hig
h.
Ver
ysm
all
sam
ple
size
(6/9
pla
sma
3/9
uri
nar
y
amin
oac
ids)
.S
tan
dar
d
ph
oto
met
ric
and
mic
rob
iolo
gic
alte
sts.
Pre
vio
us
die
tary
inta
ke,
sup
plem
enta
tio
nan
d
med
icat
ions
wer
en
ot
con
sid
ered
.C
ond
uct
ed
bef
ore
reco
mm
enda
tio
ns
for
fola
te
sup
plem
enta
tio
n.
Stu
dy
un
bli
nd
ed.
(Co
ntin
ued
)
1602 MAIN ET AL
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

TABLE2
(Co
nti
nu
ed)
Ref
eren
cean
dst
ud
y
type
(cou
ntr
y)
No.
of
subje
cts
Pat
ient
char
acte
rist
ics
Cas
edefi
nit
ion
Outc
ome
mea
sure
sR
esul
tsC
om
men
ts
Low
eet
al,
19
81
(40
)
(US
A)
Cas
eco
ntr
olII
I-2
Cas
es=
43
.C
on
trol
s=
59
chil
dre
n/
ado
lesc
ents
wit
ho
ther
psy
chia
tric
or
dev
elo
pmen
tal
dis
ord
ers.
19
fam
ily
and
com
mun
ity
mem
ber
s.
Cas
esag
ed1
2.4
y(r
ange
:
4–
22
y);
con
tro
ls:
oth
er
psy
chia
tric
/
dev
elo
pm
enta
l
dis
ord
ers;
age
=1
1.4
y
(ran
ge:
2–
32
y).
Fam
ily
and
com
mun
ity
mem
ber
sag
ed2
6y
(ran
ge:
12
–4
6y
).
DS
M-I
II.
Ser
um
and
eryt
hro
cyte
fola
te,
seru
mv
itam
in
B-1
2co
nce
ntr
atio
ns.
CS
Ffo
late
and
mo
no
amin
e
con
cen
trat
ion
sin
a
sub
gro
up
com
pri
sin
g
6ca
ses
and
10
wit
h
no
nau
tist
icp
sych
iatr
ic
or
dev
elo
pm
enta
l
dis
ord
ers.
Res
ults
wer
ep
rese
nte
das
mea
nse
rum
and
ery
thro
cyte
con
cen
trat
ion
sfo
r
vit
amin
san
dC
SF
mo
no
amin
es6
SD
san
d
ran
ge.
Th
eco
rrel
atio
n
bet
wee
nse
rum
fola
te
and
vit
amin
B-1
2is
show
nb
yu
sin
g
Pea
rso
n’s
coef
fici
ent.
Ser
um
and
eryt
hro
cyte
fola
tean
dse
rum
vit
amin
B-1
2w
ere
no
rmal
com
par
edw
ith
fam
ily
and
com
mu
nit
yco
ntr
ols
.
Ther
ew
asno
corr
elat
ion
bet
wee
nth
em.
Th
ere
was
no
sign
ifica
nt
dif
fere
nce
inC
SF
fola
te
bet
wee
nch
ild
ren
wit
h
auti
sman
dth
ose
wit
h
oth
erp
sych
iatr
ic/
dev
elo
pmen
td
iso
rder
s.
Eig
ht
case
sw
ere
tak
ing
foli
cac
idsu
ppl
emen
ts.
Th
ese
chil
dre
nh
ad
hig
her
seru
man
d
eryt
hro
cyte
fola
te
con
cen
trat
ion
s.
Ser
um
and
CS
Ffo
late
con
cen
trat
ion
sw
ere
low
com
par
edw
ith
curr
ent
refe
ren
ceva
lues
[AM
H2
00
8,R
amae
ker
s
etal
(44
)].
No
info
rmat
ion
abo
ut
pre
vio
us
die
tary
inta
ke
or
med
icat
ion.
Con
du
cted
bef
ore
reco
mm
enda
tio
ns
for
fola
tesu
ppl
emen
tati
on
.
Th
ein
clu
sio
no
ffa
mil
y
mem
ber
san
dad
ult
sas
con
tro
lsw
asn
ot
app
rop
riat
e.S
tud
y
un
bli
nd
ed.
Vis
cont
iet
al1
99
4(3
2)
(Ita
ly)
Cas
eco
ntr
ol
III-
2
Cas
es=
37
.C
on
trol
s=
19
.C
ontr
ols
:m
ean
age
=7
y
(ran
ge:
3–
13
y).
No
neu
rolo
gic
/met
abol
ic/
psy
chia
tric
dis
ord
ers.
DS
M-I
II-R
.S
eru
man
du
rin
ary
amin
o
acid
con
cen
trat
ion
s.
Res
ults
pre
sen
ted
asm
ean
(6S
D)
seru
man
d
uri
nar
yco
nce
ntr
atio
ns.
Th
ere
wer
en
o
stat
isti
call
ysi
gnifi
cant
dif
fere
nce
sin
pla
sma
or
uri
nar
ym
eth
ion
ine
or
pla
sma
cyst
ein
eb
etw
een
case
san
dco
ntr
ols
or
bet
wee
nca
ses
wit
han
d
wit
ho
utn
euro
log
ic
sym
pto
ms.
Uri
nar
y
cyst
ein
eco
nce
ntr
atio
ns
wer
elo
wer
inch
ild
ren
wit
hau
tism
and
neu
rolo
gic
al
abn
orm
alit
ies
(P,
0.0
5)
than
inco
ntr
ols
.
Ag
ean
dse
xar
eid
enti
fied
asp
oss
ible
con
foun
der
s.
No
info
rmat
ion
abo
ut
pre
vio
us
die
tary
inta
ke,
med
icat
ions,
or
sup
plem
enta
tio
n.
Stu
dy
un
bli
nd
ed.
(Co
ntin
ued
)
FOLATE-METHIONINE PATHWAY AND AUTISM 1603
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

TABLE
2(C
onti
nu
ed)
Ref
eren
cean
dst
udy
type
(countr
y)
No
.o
fsu
bje
cts
Pat
ient
char
acte
rist
ics
Cas
edefi
nit
ion
Outc
ome
mea
sure
sR
esult
sC
omm
ents
D’E
ufe
mia
etal
,1
99
5(3
3)
(Ita
ly)
Cas
eco
ntr
ol
III-
2
Cas
es=
40
.C
ontr
ols
=4
6.
Cas
esag
ed1
2y
4m
o
(ran
ge:
7–
17
y;
27
mal
e,
13
fem
ale)
.M
ean
IQ=
68
.1(6
2–
78)
(Sta
nfo
rd
and
Bin
etsc
ale)
,n
o
epil
epsy
.C
on
trol
sag
ed
11
y2
mo
(ran
ge:
5–
15
y;2
7m
ales
,19
fem
ales
).
No
rmal
IQ,
no
per
son
al
or
fam
ily
his
tory
of
psy
chia
tric
or
neu
rolo
gic
dis
ord
ers,
hea
lth
y.A
ll
par
tici
pan
tso
fn
orm
al
hei
ght
and
wei
ght
rang
e
and
on
anu
nre
stri
cted
die
t.N
om
edic
atio
ns
in
the
mo
nth
bef
ore
the
stu
dy.
DS
M-I
II-R
.P
lasm
aam
ino
acid
con
cen
trat
ion
s.
Try
pto
ph
an:L
NA
A
rati
o.
Res
ults
for
pla
sma
amin
o
acid
con
cen
trat
ion
sw
ere
pre
sen
ted
asm
eans
6
SD
s.C
omp
aris
on
of
mea
nsw
asca
rrie
dout
by
usi
ng
the
Man
n-
Wh
itn
eyU
test
for
nonpa
ram
etri
cdat
a.
Sp
earm
an’s
test
was
use
dto
calc
ula
teth
e
corr
elat
ion
coef
fici
ents
bet
wee
nth
etr
yp
toph
an:
LN
AA
rati
oan
dag
e,
hei
ght,
wei
gh
t,an
dIQ
.
Th
ere
was
no
sign
ifica
nt
dif
fere
nce
inm
eth
ion
ine
or
cyst
ein
e
con
cen
trat
ion
sb
etw
een
case
san
dco
ntr
ols
.
Th
etr
yp
top
han
:LN
AA
rati
ow
assi
gnifi
cant
ly
low
erin
case
sth
anin
con
tro
ls(P
,0
.01)
.N
o
corr
elat
ion
bet
wee
n
try
pto
phan
:LN
AA
and
age,
hei
gh
t,w
eig
ht,
or
IQ.
Sm
all
stud
y.
Cas
esso
urc
edfr
om
Ital
ian
Ass
oci
atio
nof
Par
ents
of
Au
tist
ic
Ch
ild
ren
.
LN
AA
did
no
tin
clu
de
met
hio
nin
e.S
tud
y
un
bli
nded
.
(Co
nti
nu
ed)
1604 MAIN ET AL
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from
TABLE
2(C
onti
nu
ed)
Ref
eren
cean
dst
udy
type
(countr
y)
No
.o
fsu
bje
cts
Pat
ient
char
acte
rist
ics
Cas
edefi
nit
ion
Outc
ome
mea
sure
sR
esult
sC
omm
ents
Arn
old
etal
,2
00
3(3
4)
(US
A)
Cas
eco
ntr
ol
III-
2
Cas
es=
36
.C
ontr
ols
=2
4.
Ag
e,
5y.
Cas
es:
10
glu
ten
/cas
ein
-fre
ed
iet
and
26
un
rest
rict
edd
iet.
Co
ntr
ols:
age-
and
sex
-
mat
ched
chil
dre
nw
ith
oth
erd
evel
opm
enta
l
del
ays.
DS
M-I
V-R
auti
stic
dis
ord
er,
PD
D-N
OS
CA
RS
,P
erva
sive
Dev
elo
pmen
tal
Dis
ord
ers
Scr
een
ing
Tes
t.
Pla
sma
amin
oac
id
con
cen
trat
ion
s.
Try
pto
ph
an:
LN
AA
rati
o.
Res
ults
pre
sen
ted
asm
ean
(6S
D)
pla
sma
amin
o
acid
conce
ntr
atio
ns
and
Pva
lues
wh
ere
sign
ifica
nt.
Bon
ferr
oni
corr
ecti
on
and
Tu
key
’s
ho
nes
tly
sign
ifica
nt
dif
fere
nce
test
app
lied
.
Pla
sma
met
hio
nin
ew
as
sign
ifica
ntly
low
erin
chil
dre
nw
ith
auti
sm
wit
han
un
rest
rict
edd
iet
than
inco
ntr
ols
(P,
0.0
2)bu
tn
ot
wh
en
Bon
ferr
oni
corr
ecti
on
appli
edas
the
stat
isti
cal
sign
ifica
nce
was
low
ered
toP,
0.0
02
8.
No
sig
nifi
can
t
dif
fere
nce
was
fou
nd
bet
wee
nan
yo
fth
e
gro
ups
for
try
pto
phan
:
LN
AA
.
Sm
all
stud
yco
mp
risi
ng
are
trosp
ecti
vere
vie
wof
med
ical
reco
rds.
So
urce
of
con
tro
lsn
ot
op
tim
al.
LN
AA
did
no
tin
clu
de
met
hio
nin
e.N
o
info
rmat
ion
pro
vid
ed
abo
ut
pre
vio
us
sup
plem
enta
tio
no
r
med
icat
ions
.
Stu
dy
un
bli
nded
.
Ad
ams
etal
,2
00
4(4
1)
(US
A)
Coh
ort
III-
3
Cas
es=
24
recr
uit
ed
for
ran
do
miz
ed
con
tro
lled
tria
l.
Cas
esag
ed4
.96
1.4
y
(ran
ge:
3–
8y
;2
2m
ales
,
2fe
mal
es).
No
pri
or
sup
plem
enta
tio
n.
Po
oled
AS
Ds
dia
gno
sed
by
psy
chia
tris
to
r
dev
elo
pmen
tal
ped
iatr
icia
n.
Ser
um
vit
amin
B-6
.R
esul
tsar
ep
rese
nte
das
mea
nan
dm
edia
nse
rum
vit
amin
B-6
con
cen
trat
ion
s6
SD
s
wit
hP
valu
esw
her
e
sign
ifica
nt.
Vit
amin
B-6
con
cen
trat
ion
sw
ere
sign
ifica
ntly
hig
her
in
case
sth
anin
con
tro
ls
(P=
0.0
00
00
01).
Sm
all
stud
ysi
ze.
Cas
ed
efin
itio
nn
ot
stan
dard
ized
.
Sta
nd
ard
mic
ro-
bio
logi
cal
assa
yfo
r
vit
amin
B-6
.
Inte
rpre
tati
on
dep
ends
on
refe
ren
ceva
lues
fro
m
the
test
ing
lab
ora
tory
.
Sam
ple
sn
ot
mea
sure
d
sim
ult
aneo
usl
y.S
tud
y
un
bli
nded
.
(Co
nti
nu
ed)
FOLATE-METHIONINE PATHWAY AND AUTISM 1605
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

TABLE
2(C
onti
nu
ed)
Ref
eren
cean
dst
udy
type
(countr
y)
No
.o
fsu
bje
cts
Pat
ient
char
acte
rist
ics
Cas
edefi
nit
ion
Outc
ome
mea
sure
sR
esult
sC
omm
ents
Jam
eset
al,
20
04
(28
)
(US
A)
Cas
eco
ntr
ol
III-
2
Cas
es=
20
.
Con
tro
ls=
33
.
Idio
pat
hic
(14
mal
e,6
fem
ale)
.1
6/2
0:
40
0lg
foli
cac
idan
d3l
g
vit
amin
B-1
2/d
.
Co
ntr
ols
aged
7.4
61
.3
y;
age-
and
sex
-
mat
ched
.
Ex
clu
sio
ns
(bo
th
gro
ups
):m
edic
atio
ns
kn
own
toaf
fect
met
hio
nin
em
etab
oli
sm.
Dia
gno
sis
of
mal
nu
trit
ion
,ac
tive
infe
ctio
n,
or
gen
etic
dis
ease
.E
xcl
usi
on
s
(co
ntr
ols)
:ch
ron
ic
dis
ease
.
DS
M-I
V.
Met
abo
lite
so
fth
e
met
hio
nin
e/tr
an
s-
sulf
ura
tio
np
ath
way
sin
pla
sma.
Res
ults
pre
sen
ted
asm
ean
(6S
D)
met
abo
lite
con
cen
trat
ion
san
d
rang
e.P
valu
esw
ere
pro
vid
edw
her
eth
ere
wer
est
atis
tica
lly
sign
ifica
ntdif
fere
nce
s.
All
met
abo
lite
sw
ere
sign
ifica
ntly
low
erin
case
sth
anin
con
tro
ls
exce
pt
for
SA
H,
aden
osi
ne,
and
GS
SH
,
wh
ich
wer
eh
igh
er.
Th
eS
AM
:SA
Hra
tio
dec
reas
edb
y4
6%
,an
d
the
tGS
H:G
SS
Hra
tio
dec
reas
edb
y6
6%
.
Th
eso
urc
eo
fth
eco
ntr
ols
was
no
tp
rov
ided
.
No
info
rmat
ion
abo
ut
die
tary
inta
ke.
No
det
ails
pro
vid
edab
ou
tO
TC
sup
plem
enta
tio
nta
ken
by
con
tro
ls.
Stu
dy
un
bli
nded
.
Mo
rett
iet
al,
20
05
(35
)
(US
A)
Cas
ere
port
IV
Cas
es=
1.
Fem
ales
wit
hC
SF
fola
te
defi
cien
cyan
dau
tism
foll
owed
fro
mse
con
d
day
afte
rb
irth
to�6
y.
Neo
nat
alE
EG
show
ed
mu
ltif
oca
lse
izu
re
dis
char
ges;
mil
d
spas
tici
tyat
2–
3m
o;
dev
elo
pmen
tal
del
ayat
9m
oan
dre
gre
ssio
nat
3.5
yre
sult
ing
inan
inab
ilit
yto
wal
ko
rfe
ed
ora
lly.
AD
OS
,A
DI-
R,
Bai
ley
Sca
leo
fIn
fant
Dev
elo
pmen
t,V
AB
S.
Fo
late
and
vit
amin
B-1
2in
per
iph
eral
tiss
ues
.
Vit
amin
B-1
2in
seru
m.
MT
HF
Rac
tiv
ity.
CS
Ffo
late
,S
AM
,S
AH
,
and
ho
mo
cyst
ein
e.
Res
ults
pre
sen
ted
asp
oin
t
valu
esco
mp
ared
wit
h
no
rmal
ran
ge.
MT
HF
R
acti
vit
ysl
igh
tly
low
er
than
con
tro
lre
fere
nce
.
Ser
um
vit
amin
B-1
2
con
cen
trat
ion
sh
igh
but
no
rmal
inp
erip
her
al
tiss
ue.
CS
Ffo
late
and
SA
Mlo
w;h
om
ocy
stei
ne
and
SA
Hco
nce
ntr
atio
ns
hig
h.
So
urc
eo
fre
fere
nce
rang
e
no
tp
rov
ided
. (Co
nti
nu
ed)
1606 MAIN ET AL
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

TABLE
2(C
onti
nu
ed)
Ref
eren
cean
dst
udy
type
(countr
y)
No
.o
fsu
bje
cts
Pat
ient
char
acte
rist
ics
Cas
edefi
nit
ion
Outc
ome
mea
sure
sR
esult
sC
omm
ents
Ram
aek
ers
etal
,2
00
5(4
2)
(Ger
man
y)
Cas
eco
ntr
ol
III-
3
Cas
es=
5/2
8ca
ses
of
auti
smin
chil
dre
nw
ith
idio
pat
hic
CF
D.
Con
tro
ls=
28
age-
mat
ched
.4
1u
nre
late
d
CN
Sco
nd
itio
ns;
5
mot
her
s.
On
ech
ild
wit
hau
tism
and
no
rmal
IQd
iagn
ose
dat
3y.
Fo
ur
chil
dre
nw
ith
auti
sman
dm
enta
l
reta
rdat
ion
dia
gn
ose
dat
2,
3,
5,
and
12
y.T
he
yo
ung
est
also
had
intr
acta
ble
epil
epsy
.
AD
OS
.S
eru
mfo
late
and
CS
F5
-
MT
HF
con
cen
trat
ion
s.
Ser
um
and
CS
Ffo
late
con
cen
trat
ion
sw
ere
pre
sen
ted
asm
eans
and
rang
es.
Blo
ckin
g
anti
bo
die
sw
ere
pre
sen
ted
wit
hch
i-
squ
are
and
Pva
lues
.
Th
em
ean
tite
ran
d
affi
nit
yco
nst
ants
wer
e
pre
sen
ted
wit
hra
ng
es.
Ser
um
fola
te
con
cen
trat
ion
sw
ere
no
rmal
.C
SF
fola
te
con
cen
trat
ion
sin
case
s
wer
esi
gnifi
cant
lylo
w
bef
ore
trea
tmen
tan
d
no
rmal
ized
afte
r
trea
tmen
t.
So
urc
eo
fth
eag
e-m
atch
ed
con
tro
lsw
asn
ot
pro
vid
ed.
No
corr
ecti
on
for
mu
ltip
le
com
par
iso
ns.
Jam
eset
al,
20
06
(29
)
(US
A)
Cas
eco
ntr
ol
III-
2
Cas
es=
80
.C
ontr
ols
=7
3.
Su
bjec
tsfr
omth
e2
00
4
stud
yw
ere
no
tin
clu
ded
.
Cas
esag
ed7
.36
3.2
y(7
1
mal
es,
9fe
mal
es).
Co
ntr
ols
aged
10
.86
4.1
y.A
ge-
and
sex
-
mat
ched
con
tro
lsfr
om
sim
ilar
studie
s.
Ex
clu
sio
ns
(bo
th
gro
ups
):m
edic
atio
ns
and
sup
plem
ents
kn
own
toaf
fect
met
hio
nin
e
met
abo
lism
,k
now
n
gen
etic
dis
ease
,an
d
chil
dh
ood
dis
inte
gra
tive
dis
ord
ers.
Ex
clu
sio
ns
(co
ntr
ol):
chro
nic
dis
ease
,au
tism
,
or
oth
ern
euro
log
ic
dis
ord
er.
DS
M-I
V,
AD
OS
,C
AR
S.
Pla
sma
met
abo
lite
so
fth
e
met
hio
nin
ean
dtr
an
s-
sulf
ura
tio
np
ath
way
s.
Res
ults
wer
ep
rese
nte
das
mea
ns,
SD
s,an
dra
nges
for
each
met
abo
lite
wit
h
Pva
lues
for
stat
isti
call
y
sign
ifica
ntdif
fere
nce
s.
All
met
abo
lite
sw
ere
sign
ifica
ntly
low
erin
case
sth
anin
con
tro
ls
exce
pt
for
SA
H,
aden
osi
ne,
and
GS
SH
,
wh
ich
wer
eh
igh
er.
Th
eS
AM
:SA
Hra
tio
dec
reas
edb
y2
7%
,an
d
the
tGS
H:G
SS
Hra
tio
dec
reas
edb
y4
8%
.
The
pro
port
ion
of
case
s
wit
hm
ore
clin
ical
ly
seve
rem
etab
oli
c
alte
rati
on
sw
as
det
erm
ined
,an
dth
e
fin
din
gs
are
pre
sen
ted
as
per
centa
ges
.
Rel
ativ
ely
smal
lst
ud
y.N
o
corr
ecti
on
for
mu
ltip
le
com
par
iso
ns.
Th
e
auth
ors
do
no
td
efin
e
clin
ical
seve
rity
.
Un
bli
nd
ed.
(Co
nti
nu
ed)
FOLATE-METHIONINE PATHWAY AND AUTISM 1607
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from
TABLE
2(C
onti
nu
ed)
Ref
eren
cean
dst
udy
type
(countr
y)
No
.o
fsu
bje
cts
Pat
ient
char
acte
rist
ics
Cas
edefi
nit
ion
Outc
ome
mea
sure
sR
esult
sC
omm
ents
Pas
caet
al,
20
06
(37
)
(Ro
man
ia)
Cas
eco
ntr
ol
III-
2
Cas
es=
12
.C
ontr
ols
=9
.C
ases
aged
8.3
62
.76
y
(75
%m
ale,
25
%
fem
ale)
.C
ontr
ols
aged
8.36
1.8
2y
(67
%m
ale,
33
%fe
mal
e).
Ex
clu
sio
ns
(bo
th
gro
ups
):m
edic
atio
n/
sup
plem
enta
tio
nk
now
n
toin
terf
ere
wit
h
met
hio
nin
em
etab
oli
sm
inth
ep
rev
iou
s6
mo.
DS
M-I
V.
Pla
sma
ho
mo
cyst
ein
ean
d
vit
amin
B-1
2
con
cen
trat
ion
s.
Par
aoxonas
e1
acti
vit
yin
pla
sma
and
glu
tath
ion
e
per
ox
idas
eac
tiv
ity
in
eryt
hro
cyte
s.
Ho
mo
cyst
ein
esi
gn
ifica
ntl
y
hig
her
inca
ses
than
in
con
tro
ls(F
=6
.78,
P=
0.0
1).
Sta
tist
ical
ly
sign
ifica
ntre
duct
ion
of
PO
N1
aryl
este
rase
acti
vit
yin
case
s
com
par
edw
ith
con
tro
ls
(F=
10
.37
,P
=0
.00
5).
No
sig
nifi
can
t
dif
fere
nce
in
par
aox
on
ase
1o
r
glu
tath
ion
ep
ero
xid
ase
acti
vit
y.
Neg
ativ
eco
rrel
atio
n
bet
wee
ng
luta
thio
ne
per
ox
idas
eac
tiv
ity
and
ho
mo
cyst
ein
e(r
=
20
.769
,P
=0
.023
)
wh
enag
ean
dse
xu
sed
asco
ntr
ol
vari
able
s.
Ver
ysm
all
sam
ple
size
.
So
urc
eo
fca
ses
and
con
tro
lsn
ot
pro
vid
ed.
No
info
rmat
ion
abo
ut
trea
tmen
to
fsa
mp
les
bef
ore
anal
ysis
.
Ho
mo
cyst
ein
e
con
cen
trat
ion
sw
ill
incr
ease
ifth
esa
mp
les
are
no
tp
lace
d
imm
edia
tely
on
ice.
Sch
effe
corr
ecti
on
for
po
sth
oc
pai
rwis
e
com
par
iso
ns
app
lied
.
Stu
dy
un
bli
nded
.
Ad
ams
etal
,2
00
6(4
3)
(US
A)
Cas
eco
ntr
ol
III-
2
Cas
es=
11
+2
4fr
omp
rev
iou
s
stud
y.C
ontr
ols
=1
1.
Cas
esag
ed7
.26
1.4
y(8
mal
es,
3fe
mal
es).
Pre
vio
us
stud
yag
e=
4.9
61
.4y
(22
mal
es,
2
fem
ales
).C
ontr
ols
aged
7.8
61
.2y
(10
mal
es,
1
fem
ale)
.E
xcl
usi
on
s:
sup
plem
enta
tio
nw
ith
vit
amin
B-6
inp
rev
iou
s
2m
o.
Incl
usi
on
(cas
es):
no
fam
ily
his
tory
of
AS
Ds,
go
od
men
tal
and
ph
ysi
cal
hea
lth
.
Dia
gn
osi
so
fau
tism
,P
DD
-
NO
S,
or
Asp
erge
r
syn
dro
me
from
ap
sych
iatr
ist
or
dev
elo
pmen
tal
ped
iatr
icia
n.
Ser
um
vit
amin
B-6
con
cen
trat
ion
s.
Res
ults
pre
sen
ted
asm
ean
and
med
ian
seru
m
vit
amin
B-6
con
cen
trat
ion
s6
SD
s
wit
hP
valu
esw
her
e
sign
ifica
nt.
Vit
amin
B-6
con
cen
trat
ion
sw
ere
sign
ifica
ntly
hig
her
in
case
sth
anin
con
tro
ls
(P=
0.0
01
).
Sm
all
sam
ple
size
.C
ase
defi
nit
ion
no
t
stan
dard
ized
.S
tan
dar
d
mic
rob
iolo
gic
alas
say
for
ph
osp
ho
ryla
ted
and
un
pho
sph
ory
late
dfo
rms
of
vit
amin
B-6
.R
esu
lts
no
tst
rati
fied
by
typ
eo
f
AS
D.
Sam
ple
sb
lin
ded
for
mea
sure
men
t.
(Co
nti
nu
ed)
1608 MAIN ET AL
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

TABLE2
(Co
nti
nu
ed)
Ref
eren
cean
dst
ud
y
type
(cou
ntr
y)
No.
of
subje
cts
Pat
ient
char
acte
rist
ics
Cas
edefi
nit
ion
Outc
ome
mea
sure
sR
esul
tsC
om
men
ts
Ad
ams
etal
,2
00
7(3
6)
(Aus
tral
ia)
Cas
eco
ntr
olII
I-2
Cas
es=
17
.C
on
trol
s=
16
.C
ases
aged
2–
16
y.
Ex
clu
sio
ns:
PD
D-N
OS
and
Asp
erge
rsy
nd
rom
e.
DS
M-I
V,
AD
OS
,A
dap
tive
Beh
avio
ral
Ass
essm
ent
Qu
esti
on
nai
re.
Fo
late
met
abo
lite
s.R
esul
tsfo
rm
etab
oli
tes
pre
sen
ted
asm
ean
con
cen
trat
ion
s6
SD
s
and
Pva
lues
.N
o
sig
nifi
can
td
iffe
ren
ce
was
det
ecte
dfo
r
ho
mo
cyst
ein
e,se
rum
,o
r
ery
thro
cyte
fola
teo
r
vit
amin
B-1
2.
Sm
all
sam
ple
nu
mb
ers.
Sour
ceof
case
san
d
con
tro
lsn
ot
pro
vid
ed.
No
info
rmat
ion
abo
ut
die
tary
inta
ke,
sup
plem
enta
tio
n,
or
med
icat
ions.
Ho
mo
cyst
ein
e
con
cen
trat
ion
sw
ill
incr
ease
ifth
esa
mpl
es
are
no
tp
lace
d
imm
edia
tely
on
ice.
Stu
dy
un
bli
nd
ed.
Ram
aek
ers
etal
,2
00
7(4
4)
(Ger
man
y)
Cas
ese
ries
IV
Cas
es=
25
.C
ases
aged
6.8
8y
(2.8
–1
2.3
y;
18
mal
es,
7fe
mal
es).
Au
tism
plu
so
ne
or
mor
e
feat
ure
so
fC
FD
.
Con
tro
lsag
ed6
.76
y
(3.3
–1
1.4
y;
14
mal
es,
11
fem
ales
).
Ex
clu
sio
ns:
infe
ctio
ns
du
ring
pre
gn
ancy
,b
irth
/
neo
nat
alin
juri
es,
hea
rin
gd
efici
ts,
inbo
rn
erro
rso
fm
etab
oli
sm,
kn
own
gen
etic
abnorm
alit
ies,
and
def
ects
of
intr
acel
lula
r
sign
alin
g.
DS
M-I
V,
AD
OS
,A
DI,
VA
BS
.
Ser
um
fola
te
con
cen
trat
ion
s.
CS
F5
-MT
HF
con
cen
trat
ion
s.
Blo
ckin
gfo
late
rece
pto
r
auto
anti
bo
dies
inse
rum
.
Res
ults
of
the
seru
man
d
CS
Ffo
late
con
cen
trat
ion
sw
ere
pre
sen
ted
asm
ean
sw
ith
ate
stst
atis
tic
and
P
valu
e.N
osi
gn
ifica
nt
dif
fere
nce
was
fou
nd
in
seru
mfo
late
(t=
0.7
6)
bet
wee
nca
ses
and
con
tro
ls.
CS
F5
-MT
HF
was
sign
ifica
ntly
low
er
inca
ses
bef
ore
trea
tmen
t(t
=7
.77
,P,
0.0
00
1).
Itis
no
tcl
ear
wh
ethe
rth
e
case
sp
rese
nte
din
Ram
aeker
set
al(4
2)
are
incl
ud
ed.
No
info
rmat
ion
abo
ut
die
tary
or
sup
ple
men
tal
fola
tein
tak
e.
Stu
dy
un
bli
nd
ed.
Mo
rett
iet
al,
20
08
(38
)
(US
A)
Cas
ese
ries
IV
Cas
es=
7.
Pat
ien
t1
=
pre
vio
us
case
rep
ort
.
Cas
esag
ed8
,9
,8
,1
0,
7,
2,
and
15
y.
CF
Dp
lus
auti
sm
(in
clu
des
Mo
rett
iet
al;
28
);5
chil
dre
nh
ad
seve
rean
d2
had
pro
fou
nd
dev
elo
p-
men
tal
del
ays.
AD
OS
,A
DI-
R,
Bai
ley,
VA
BS
.
CS
F5
-MT
HF
con
cen
trat
ion
s.
Res
ults
for
CS
F5
-MT
HF
con
cen
trat
ion
sw
ere
pre
sen
ted
asp
oin
tval
ues
com
par
edw
ith
no
rmal
ran
ge.
CS
Ffo
late
was
sig
nifi
can
tly
low
for
all
case
sat
dia
gno
sis.
Sm
all
sam
ple
size
.
No
info
rmat
ion
abo
ut
sup
plem
ents
or
med
icat
ion.
Cas
eso
lder
than
Ram
aeker
set
al(4
2,4
4).
Pre
-an
d
po
stin
terv
enti
on
beh
avio
ral
sco
res
no
t
pre
sen
ted.
Un
bli
nded
.
(Co
ntin
ued
)
FOLATE-METHIONINE PATHWAY AND AUTISM 1609
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

TABLE
2(C
onti
nu
ed)
Ref
eren
cean
dst
udy
type
(countr
y)
No
.o
fsu
bje
cts
Pat
ient
char
acte
rist
ics
Cas
edefi
nit
ion
Outc
ome
mea
sure
sR
esult
sC
omm
ents
Su
het
al,
20
08
(30
)(U
SA
)
Cas
eco
ntr
ol
III-
2
Cas
es=
31
.C
ontr
ols
=1
1.
Cas
esag
ed4
.176
1.3
y(2
6
mal
e,4
fem
ale)
.
70
%G
Ip
rob
lem
s;
38
.5%
pic
a;4
0.7
%
del
ayed
mo
tor
dev
elo
pmen
t;6
4.3
%
del
ayed
spee
ch
dev
elo
pmen
t.
Co
ntr
ols
aged
6.9
61
.6
y(9
mal
e,2
fem
ale)
.
Ex
clu
sio
ns
(bo
th):
nu
trit
ion
alo
r
anti
ox
idan
t
sup
plem
enta
tio
nin
the
pre
vio
us
6m
o.
Excl
usi
ons
(cas
es):
chro
nic
dis
ease
;ac
ute
illn
ess
inp
rio
r2
wk
;
psy
chia
tric
,
anti
infl
amm
ato
ry,
or
chel
atio
nth
erap
y.
Ex
clu
sio
ns
(co
ntr
ols)
:
fam
ily
or
per
son
al
his
tory
of
auti
sm,
med
icat
ion
s.
AS
Ds
defi
ned
by
DS
M-I
V
plu
sA
DI-
R.
Met
hio
nin
ecy
cle
and
tra
ns-
sulf
ura
tion
pat
hw
aym
etab
oli
tes
in
leu
kocy
tes
and
pla
sma.
Leu
koc
yte
met
abo
lite
con
cen
trat
ion
sp
rese
nte
d
asa
Fo
rest
plo
tfo
rea
ch
met
abo
lite
that
incl
ud
ed
the
mea
nsc
ore
and
,
wh
ere
sign
ifica
nt,
the
Pva
lue.
Pla
sma
met
abo
lite
con
cen
trat
ion
sw
ere
pre
sen
ted
asm
eans
(6S
Ds)
for
ind
ivid
ual
met
abo
lite
san
dP
valu
esw
her
esi
gnifi
can
t.
Leu
koc
yte
SA
M
con
cen
trat
ion
sw
ere
sign
ifica
ntly
low
erin
case
sth
anin
con
tro
ls
(P=
0.0
3),
red
uci
ngth
e
SA
M:S
AH
rati
ob
y
50
%.
Leu
koc
yte
ho
mo
cyst
ein
ew
as
sign
ifica
ntly
hig
her
in
case
sth
anin
con
tro
ls
(P=
0.0
3)
and
cyst
ein
e
+cy
stei
ne
and
GS
H
sign
ifica
ntly
low
er(P
=
0.0
04an
dP
=0
.02,
resp
ecti
vely
).
Th
ere
was
no
sign
ifica
nt
dif
fere
nce
inp
lasm
a
met
abo
lite
sb
etw
een
case
san
dco
ntr
ols
exce
pt
for
cyst
einy
l-
gly
cin
e,w
hic
hw
as
hig
her
inca
ses
(P=
0.0
008
).
Sm
all
sam
ple
size
.
So
urc
eo
fca
ses
and
con
tro
lsn
ot
pro
vid
ed.
Cas
ed
efin
itio
nd
oes
no
t
dis
tin
gu
ish
bet
wee
n
dif
fere
nt
type
so
fA
SD
s.
Det
ails
of
trea
tmen
tof
blo
od
sam
ple
s
imm
edia
tely
afte
r
veni
pu
nct
ure
no
t
pro
vid
ed.
Ho
mo
cyst
ein
e
con
cen
trat
ion
sar
eli
kel
y
toin
crea
seif
the
sam
ple
s
are
no
tim
med
iate
ly
pla
ced
on
ice.
Fo
rest
plo
t
har
dto
inte
rpre
t.S
om
e
sig
nifi
can
tva
lues
wer
e
pre
sen
ted
inth
ete
xt.
Stu
dy
un
bli
nded
.
1tG
SH
,tota
lglu
tath
ione;
GS
SH
,oxid
ized
glu
tath
ione;
CF
D,c
ereb
ral
fola
tedefi
cien
cy;
GI,
gas
troin
test
inal
;C
SF,
cere
bro
spin
alfl
uid
;S
AM
,S-a
den
osy
l-m
ethio
nin
e;S
AH
,S-a
den
osy
l-h
om
ocys
tein
e;D
SM
-
III,
DS
M-I
II-R
,D
SM
-IV
,an
dD
SM
-IV
-R,
Dia
gno
stic
and
Sta
tist
ical
Man
ual
of
Men
tal
Dis
ord
ers,
3rd
edit
ion
,3
rded
itio
nre
vis
ed,
4th
edit
ion
,an
d4
thed
itio
nre
vis
ed,
resp
ecti
vely
;C
AR
S,
Chi
ldh
ood
Au
tism
Rat
ing
Sca
le;
5-M
TH
F,5-m
ethylt
etra
hydro
fola
te;
MT
HF
R,
met
hyle
ne
tetr
ahydro
fola
tere
duct
ase;
OT
C,
over
the
counte
r;C
NS
,ce
ntr
alner
vous
syst
em;
IQ,
inte
llig
ence
qu
oti
ent;
AS
D,
auti
smsp
ectr
um
dis
ord
er;
LN
AA
,la
rge
neu
tral
amin
oac
ids;
EE
G,
elec
tro
ence
ph
alo
gra
ph;
PD
D-N
OS
,p
erva
sive
dev
elo
pm
enta
ld
iso
rder
–n
oto
ther
wis
esp
ecifi
ed;
VA
BS
,V
inel
and
Ad
apti
veB
ehav
iou
rS
cale
;A
DO
S,
Au
tism
Dia
gno
stic
Ob
serv
atio
nS
ched
ule
;A
DI-
R,
Au
tism
Dia
gno
stic
Inte
rvie
w–
rev
ised
;A
MH
,A
ust
rali
anM
edic
ines
Han
db
ook
.
1610 MAIN ET AL
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

TABLE3
Stu
die
sre
port
ing
inte
rven
tions
of
the
fola
te-m
ethio
nin
epat
hway
inch
ildre
nw
ith
auti
sm1
Ref
eren
cean
d
cou
ntr
yN
o.
of
sub
ject
sP
atie
nt
char
acte
rist
ics
Inte
rven
tio
nO
utc
ome
mea
sure
Res
ults
Co
mm
ents
Jam
eset
al,
20
04
(28
)
(US
A)
Cas
es=
8M
ost
seve
rely
abn
orm
al
met
abo
lic
pro
file
fro
m
stud
yo
f2
0ch
ild
ren
(see
Tab
le1
).
Inte
rven
tio
n1
:8
00l
g
foli
nic
acid
and
10
00l
g
bet
ain
etw
ice
dai
lyfo
r3
mo.
Inte
rven
tio
n2
:
add
itio
nal
mo
nth
on
sam
ere
gim
enp
lus
an
inje
ctio
no
f7
5lg
vit
amin
B-1
2/k
gtw
ice
wee
kly
.
Met
abo
lite
so
fth
e
met
hio
nin
e/tr
an
s-
sulf
ura
tio
np
athw
ays
in
pla
sma.
Th
efi
rst
inte
rven
tio
n
no
rmal
ized
pla
sma
met
hio
nin
e,S
AM
,SA
H,
aden
osi
ne,
and
ho
mo
cyst
ein
e
con
cen
trat
ion
s.In
add
itio
n,
tGS
H,
GS
SH
,
and
tGS
H:G
SS
Hw
ere
sign
ifica
ntl
yim
pro
ved
but
no
tn
orm
aliz
ed.
Th
e
add
itio
no
fv
itam
inB
-12
no
rmal
ized
cyst
ein
e,
tGS
H,
and
GS
SH
con
cen
trat
ion
sas
wel
las
the
tGS
H:G
SS
Hra
tio.
It
also
furt
her
incr
ease
d
the
SA
M:S
AH
rati
o(P
=
0.0
4)an
dd
ecre
ased
the
con
cen
trat
ion
of
aden
osi
ne
(P=
0.0
02
).
Ver
ysm
all
sam
ple
size
for
the
inte
rven
tion.
Cri
teri
a
for
incl
usi
on
inth
e
inte
rven
tio
ng
rou
pw
ere
no
tpro
vid
ed.B
onfe
rron
i
corr
ecti
on
was
only
app
lied
toco
mp
are
indi
vid
ual
met
abo
lite
s
afte
rea
chin
terv
enti
on
.
Th
ere
sult
sw
ere
no
t
lin
ked
too
bje
ctiv
e
chan
ges
inb
ehav
ior.
Stu
dy
was
un
bli
nded
.
Mo
rett
iet
al,
20
05
(35
)
(US
A)
Cas
es=
1S
eeT
able
1.
0.5
mg
foli
nic
acid
/kg
dai
ly
for
2w
kth
en1
.0m
g/k
g
dai
lyfo
r3
mo
for
1y
beg
inn
ing
atag
e6
y.
CS
Fm
etab
oli
tes
incl
ud
ing
tho
seo
fth
em
eth
ion
ine
cycl
eb
efo
rean
daf
ter
inte
rven
tio
n.
EE
G
bef
ore
and
afte
r
inte
rven
tio
n.
Beh
avio
ral
chan
ges
.
Tre
atm
ent
wit
hfo
lin
icac
id
no
rmal
ized
CS
F
met
abo
lite
san
d
imp
rove
dm
oto
rco
ntr
ol.
Ep
ilep
tifo
rmd
isch
arg
es
ceas
ed.N
och
ange
toth
e
sym
pto
ms
asso
ciat
ed
wit
hau
tism
.
So
urce
of
no
rmal
ran
ge
no
t
pro
vid
ed.
Do
seo
f
inte
rven
tio
nb
ased
on
pre
vio
usl
yp
ub
lish
ed
repo
rts.
(Co
ntin
ued
)
FOLATE-METHIONINE PATHWAY AND AUTISM 1611
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

TABLE
3(C
onti
nu
ed)
Ref
eren
cean
d
cou
ntr
yN
o.
of
sub
ject
sP
atie
nt
char
acte
rist
ics
Inte
rven
tio
nO
utc
ome
mea
sure
Res
ults
Co
mm
ents
Ram
aek
ers
etal
,2
00
5(4
2)
(Ger
man
y)
Cas
es=
5/2
8ca
ses
of
auti
smin
chil
dre
nw
ith
idio
pat
hic
CF
D.
See
Tab
le1
.T
he
chil
dw
ith
an
orm
alIQ
wh
ow
astr
eate
dw
ith
am
ult
ivit
amin
wit
h4
00
lgfo
lin
icac
idd
aily
.
Th
ere
sto
fth
ech
ild
ren
wer
etr
eate
dw
ith
0.5
–
1.0
mg
foli
co
rfo
lin
ic
acid
/kg
dai
lyo
nan
on
goi
ng
bas
is.
CS
F5
-MT
HF
con
cen
trat
ion
sb
efo
re
and
6m
oaf
ter
the
inte
rven
tio
n.
Blo
ckin
g
fola
tere
cep
tor
anti
bo
dies
inse
rum
.
Ser
um
fola
teco
nce
ntr
atio
ns
wer
en
orm
al.
CS
Ffo
late
con
cen
trat
ion
sin
case
s
wer
esi
gnifi
cant
lylo
w
bef
ore
trea
tmen
tan
d
no
rmal
ized
afte
r
trea
tmen
t.T
he
chil
d
wit
ha
no
rmal
IQh
adn
o
blo
ckin
gF
Ran
tib
odi
es.
Th
eo
ther
case
sh
adve
ry
hig
hti
ters
of
blo
ckin
g
FR
anti
bo
dies
.T
he
chil
d
wit
ha
no
rmal
IQ
reco
vere
dco
mp
lete
ly.
Tre
atm
ent
imp
rove
d
com
mu
nic
atio
nsk
ills
and
neu
rolo
gic
abn
orm
alit
ies
inth
e2
yo
ung
erch
ild
ren
wit
h
men
tal
reta
rdat
ion
,
wh
erea
sth
eo
lder
chil
dre
nre
mai
ned
auti
stic
.E
pil
epti
c
seiz
ure
sw
ere
full
y
con
tro
lled
wit
hfo
lin
ic
acid
.
No
corr
ecti
on
for
mul
tiple
com
par
iso
ns.T
he
resu
lts
wer
en
ot
lin
ked
to
ob
ject
ive
chan
ges
in
beh
avio
r.
(Co
ntin
ued
)
1612 MAIN ET AL
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

TABLE
3(C
onti
nu
ed)
Ref
eren
cean
d
cou
ntr
yN
o.
of
sub
ject
sP
atie
nt
char
acte
rist
ics
Inte
rven
tio
nO
utc
ome
mea
sure
Res
ults
Co
mm
ents
Ram
aek
ers
etal
,2
00
7(4
4)
(Ger
man
y)
Cas
es=
25
See
Tab
le1
.1
–3
mg
foli
nic
acid
/kg
dai
ly
(sta
rtin
gd
ose
:1
mg
/kg
dai
ly).
IfC
SF
5-M
TH
F
stil
llo
waf
ter
3–
6m
o,
do
sein
crea
sed
to2
–3
mg/
kg
dai
ly.
CS
F5
-MT
HF
con
cen
trat
ion
sb
efo
re
and
afte
rin
terv
enti
on
.
Blo
ckin
gfo
late
rece
pto
r
auto
-ant
ibo
die
sin
seru
m.
CS
F5
-MT
HF
sig
nifi
can
tly
low
erin
case
sbef
ore
trea
tmen
t(t
=7
.77,
P,
0.0
001
)an
dn
orm
aliz
ed
afte
rtr
eatm
ent.
Nin
etee
no
f2
5ca
ses
had
blo
ckin
gF
Rau
to-
anti
bo
dies
inse
rum
.Th
e
tite
rw
assi
gn
ifica
ntl
y
hig
hin
thes
esu
bje
cts
(P
,0
.000
1);
17
/19
of
thes
eca
ses
also
had
neu
rolo
gic
defi
cits
.
Sp
onta
neo
us
norm
aliz
atio
nof
auto
-
anti
bo
dies
and
CF
Din
1
pat
ien
t,1
lost
tofo
llow
-
up,
no
resu
lts
avai
lable
for
3p
atie
nts
.T
wo
pat
ien
ts(d
iag
nose
dat
2
and
3.2
y)
had
com
ple
te
reco
very
of
neu
rolo
gic
sym
pto
ms
and
auti
sm.
Th
irte
enp
atie
nts
(dia
gno
sed
at3
–7
y)
had
imp
rove
dn
euro
log
yan
d
par
tial
reco
very
of
auti
sm.
Th
ree
old
er
pat
ien
ts(d
iag
nose
dat
4.9
,8
,an
d1
1.9
y)
show
edp
arti
alre
cove
ry
of
neu
rolo
gy
and
no
chan
ge
inau
tism
.
Itis
no
tcl
ear
wh
ethe
rth
e
case
sp
rese
nte
db
y
Ram
aeker
set
al(4
2)
are
incl
ud
ed.
No
info
rmat
ion
abo
ut
die
tary
or
sup
ple
men
tal
fola
tein
tak
e.U
nb
lin
ded
.
(Co
ntin
ued
)
FOLATE-METHIONINE PATHWAY AND AUTISM 1613
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

these associations (29), although a later case report of a childseverely affected with autism plus CFD showed that the childwas homozygous for the MTHFR 677C/T allele and hetero-zygous for MTHFR 1298A/C (35).
In addition, a borderline association with autism was detectedfor the 19 base pair (bp) deletion of the dihydrofolate reductase(DHFR) gene [odds ratio (OR): 2.69; 95% CI: 1.00, 7.28; P ,0.05] which is involved in folate metabolism (36). Significantassociations were also found in this study for this polymorphismin combination with MTHFR 677C/T (OR: 2.09; 95% CI:1.04, 4.18; P , 0.04), MTHFR 677C/T and MTHFR1298A/C (OR: 1.64; 95% CI: 1.0, 2.69; P , 0.05), andMTHFR 677C/T and RFC-1 80G/A (OR: 1.8; 95% CI: 1.02,3.18; P = 0.04) (25). These findings have not been confirmed todate.
The findings for genes involved in folate transport were alsoinconsistent. Although the largest study to date found a signifi-cant association between RFC-1 80G/A and autism (OR: 2.13;95% CI: 1.4, 3.4) (29), a subsequent study failed to replicate thefindings (37). On the other hand, an association was found be-tween the 19-bp deletion of DHFR and RFC-1 with autism (36).Other studies have not found any mutations in genes involved infolate transport (35, 38, 44).
DISCUSSION
Although the findings of this review indicate inconsistenciesbetween studies, they suggest that the folate-methionine pathwaymay play a role in the etiology of autism; however, further studyis necessary before any definitive conclusions can be made.
Methionine cycle
The largest studies to date that have measured concentrationsof the metabolites of the methionine cycle in plasma found thatmethionine, SAM, and homocysteine were significantly lowerand SAH was significantly higher in children with autism than incontrols (28, 29). Although a later study showed no significantdifferences between children with autism and controls, thenumber of participants was much lower, which suggests that thefindings may be less reliable (30). The same study identifieddifferences in methionine cycle metabolites from peripherallymphocytes; however, the presentation of the findings togetherwith the low sample numbers have made interpretation of the datadifficult.
Inconsistencies were found between studies in plasmaconcentrations of all amino acids associated with the methionine-transulfuration pathways. One reason for this may be meth-odologic differences between studies. For example, homocysteineis released from blood cells into plasma at ’10% h at roomtemperature (46). Samples, therefore, should be immediately puton ice and the plasma separated out or homocysteine concen-trations will be artificially high. The 3 studies that showedhigher concentrations of homocysteine in children with autismthan in controls do not provide details of how the samples werehandled immediately after they were taken (30, 36, 37). Bothpublications by James et al (28, 29), however, indicate that thesamples were immediately placed on ice, which lends credenceto their findings.T
ABLE
3(C
onti
nu
ed)
Ref
eren
cean
d
cou
ntr
yN
o.
of
sub
ject
sP
atie
nt
char
acte
rist
ics
Inte
rven
tio
nO
utc
ome
mea
sure
Res
ults
Co
mm
ents
Mo
rett
iet
al,
20
08
(38
)
(US
A)
Cas
es=
7S
eeT
able
1.
0.5
mg
foli
nic
acid
/kg
dai
ly
for
2w
kth
en1
.0m
g/k
g
dai
lyfo
r3
mo.
CS
F5
-MT
HF
con
cen
trat
ion
sb
efo
re
and
afte
rin
terv
enti
on
.
Res
ult
sfo
rC
SF
5-M
TH
F
con
cen
trat
ion
sw
ere
pre
sen
ted
asp
oin
tval
ues
com
par
edw
ith
no
rmal
rang
e.C
SF
fola
tew
as
sign
ifica
ntl
ylo
wfo
ral
l
case
sat
dia
gnosi
san
d
no
rmal
ized
afte
r
trea
tmen
tw
ith
foli
nic
acid
.T
reat
men
tle
dto
imp
rove
men
tsin
cog
nit
ion
,la
ng
uag
e,an
d
mot
or
do
mai
ns
wit
hn
o
chan
ge
inau
tist
ic
sym
pto
ms.
Imp
rove
d
seiz
ure
con
tro
lin
2/6
.
Sm
all
sam
ple
size
.N
o
info
rmat
ion
abo
ut
sup
plem
ents
or
med
icat
ion.
Cas
esold
er
than
thos
ein
the
stud
y
by
Ram
aek
ers
etal
(42
,
44
).P
re-
and
po
stin
terv
enti
on
beh
avio
ral
sco
res
no
t
pre
sen
ted.
Un
bli
nded
.
1tG
SH
,to
tal
glu
tath
ione;
GS
SH
,oxid
ized
glu
tath
ione;
CF
D,
cere
bra
lfo
late
defi
cien
cy;
CS
F,ce
rebro
spin
alfl
uid
;S
AM
,S-a
den
osy
l-m
eth
ion
ine;
SA
H,
S-a
den
osy
l-h
om
ocy
stei
ne;
5-M
TH
F,5
-met
hy
l-
tetr
ahydro
fola
te;
IQ,
inte
llig
ence
quoti
ent;
EE
G,
elec
troen
cephal
ogra
m;
FR
,fo
late
rece
pto
r.
1614 MAIN ET AL
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

TABLE4
Stu
die
so
fg
enes
of
the
fola
te-m
eth
ion
ine
pat
hway
inch
ild
ren
wit
hau
tism
1
Ref
eren
cean
dst
ud
y
type
(co
un
try
)N
o.
of
sub
ject
sP
atie
nt
char
acte
rist
ics
Cas
ed
efin
itio
nO
utc
ome
mea
sure
sR
esul
tsC
om
men
ts
Bor
iset
al,
20
04
(45
)
(US
A)
Cas
eco
ntr
ol
III-
3
Cas
es=
16
8.
14
2m
ale,
26
fem
ale.
73
.6%
auti
stic
dis
ord
er,
28
.2%
PD
D-N
OS
.
14
9re
gre
ssiv
e,1
9
idio
pat
hic
.
All
wh
ite.
DS
M-I
Vau
tist
icd
iso
rder
or
PD
D-N
OS
.
MT
HF
Rp
oly
mo
rph
ism
s
67
7C/
Tan
d
12
98
A/
C
Res
ult
sp
rese
nte
das
the
nu
mb
eran
dp
rop
orti
on
(%)
of
chil
dre
nw
ith
each
gen
oty
pe
and
P
valu
esw
her
e
stat
isti
call
ysi
gn
ifica
nt.
67
7C/
T
po
lym
orp
his
ms
wer
e
sign
ifica
ntl
yas
soci
ated
wit
hca
ses
(P,
0.0
001
).1
29
8AA
(wil
d
type
)w
asm
ore
pre
vale
nt
inca
ses
than
inco
ntr
ols
(P=
0.0
005
)
and
12
98
A/
Cw
as
mor
ep
reva
len
tin
contr
ols
than
inca
ses
(P=
0.0
4).
Co
mpo
un
d
het
ero
zyg
ote
67
7C/
T/
12
98A
/C
was
sign
ifica
ntl
ym
ore
pre
vale
nt
inca
ses
than
inco
ntr
ols
(P=
0.0
1).
Gen
oty
pin
gp
erfo
rmed
in3
dif
fere
nt
lab
ora
tori
es.
Po
pula
tion
con
cen
trat
ion
dat
afr
om
2d
iffe
ren
tst
ud
ies
use
d
for
con
tro
ls.
Har
dto
gen
eral
ize
bec
ause
of
ah
igh
deg
ree
of
vari
abil
ity
bet
wee
n
eth
nic
gro
ups
.T
he
fin
din
gs
are
no
tst
rati
fied
by
type
of
AS
Ds.
No
corr
ecti
on
for
mul
tiple
com
par
iso
ns.
Mo
rett
iet
al,
20
05
(35
)
(US
A)
Cas
ere
port
IV
Cas
es=
1.
See
Tab
le1
.A
DO
S,
AD
I-R
.M
TH
FR
po
lym
orp
his
ms
67
7C/
Tan
d
12
98
A/
C.
Mu
tati
on
s
info
late
rece
pto
rs.
Res
ult
sfo
rM
TH
FR
po
lym
orp
his
m
pre
sen
ted
asp
ho
tog
rap
h
of
elec
tro
ph
ore
sis.
Th
e
pat
ien
tw
ash
om
ozy
gou
s
for
MT
HF
R6
77
C/
T
and
het
ero
zyg
ou
sfo
r
MT
HF
R1
29
8A/
C.
MT
HF
Rac
tiv
ity
was
low
.N
om
uta
tio
ns
of
RF
C1
or
FB
P1
wer
e
det
ecte
d.
(Co
ntin
ued
)
FOLATE-METHIONINE PATHWAY AND AUTISM 1615
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

TABLE
4(C
onti
nu
ed)
Ref
eren
cean
dst
ud
y
type
(co
un
try
)N
o.
of
sub
ject
sP
atie
nt
char
acte
rist
ics
Cas
ed
efin
itio
nO
utc
ome
mea
sure
sR
esul
tsC
om
men
ts
Jam
eset
al,
20
06
(29
)
(US
A)
Cas
eco
ntr
ol
III-
2
Cas
es=
36
0.
Co
ntr
ols
=
20
5.
See
Tab
le1
;9
7%
case
san
d
10
0%
con
tro
lsw
hit
e.
DS
M-I
V-R
,A
DO
S,
CA
RS
.G
enes
of
the
met
hio
nin
e
and
tra
ns-
sulf
urat
ion
pat
hw
ays.
RF
C-1
,MT
HF
R,M
TR
R,
TC
N2,
CO
MT,
GS
TM
-1
nu
ll,
GC
PII
.
Res
ult
sp
rese
nte
das
nu
mb
ero
fsu
bje
cts,
OR
s,9
5%
CIs
,an
dP
valu
esfo
rea
chal
lele
or
gen
eco
mb
inat
ion
.R
FC
-
18
0A/
Gw
as
sign
ifica
ntl
yas
soci
ated
wit
hau
tism
(OR
:2
.13;
95
%C
I:1
.4,
3.4
).
Sig
nifi
can
tg
ene-
gen
e
inte
ract
ion
sfo
un
dfo
r:
TC
N2
77
7C/
T:
CO
MT
47
2G/
A(O
R:
7.0
;9
5%
CI:
2.3
2,
21
.2);
RF
C-1
80
A/
G:
MT
FR
67
7C/
T;
RF
C-
18
0A/
G:
GS
TM
-1
nu
ll.
Rel
ativ
ely
smal
lst
ud
y.N
o
corr
ecti
on
for
mul
tiple
com
par
iso
ns.
Un
bli
nd
ed.
(Co
ntin
ued
)
1616 MAIN ET AL
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

TABLE
4(C
onti
nu
ed)
Ref
eren
cean
dst
ud
y
type
(co
un
try
)N
o.
of
sub
ject
sP
atie
nt
char
acte
rist
ics
Cas
ed
efin
itio
nO
utc
ome
mea
sure
sR
esul
tsC
om
men
ts
Ad
ams
etal
,2
00
7(3
6)
(Au
stra
lia)
Cas
eco
ntr
ol
III-
2
Cas
es=
17
.C
on
trol
s=
16
.S
eeT
able
1.
DS
M-I
V,
AD
OS
,A
dap
tive
Beh
avio
ral
Ass
essm
ent
Qu
esti
onn
aire
.
Gen
eso
fth
efo
late
/
met
hio
nin
ep
athw
ay.
19
-bp
del
-DH
FR
,
MT
HF
R,
MS,
MS
R,
GC
PII
,R
FC
-1.
Res
ult
sp
rese
nte
das
the
nu
mb
erw
ith
the
wil
d-
type
and
mu
tan
tfo
rm
plu
sth
eO
Rs,
95
%C
Is,
and
Pva
lues
wh
ere
the
dif
fere
nce
was
stat
isti
call
ysi
gn
ifica
nt.
Ab
ord
erli
ne
asso
ciat
ion
was
det
ecte
dfo
rth
e1
9-
bp
del
–DH
FR
gen
e
(OR
:2
.69;
95
%C
I:
1.0
0,7
.28;
P,
0.0
5).
No
sign
ifica
nt
asso
ciat
ion
sw
ere
det
ecte
dfo
rR
FC
80
A/
G,
MT
HF
R
67
7C/
T,1
29
8A/
C,
MS
R7
56
A/
G,
MS
R
66
A/
G,
or
GC
PII
15
61C
/T.
Bor
der
lin
e
asso
ciat
ion
sw
ere
det
ecte
dfo
r1
9-b
p-d
el-
DH
FR
and
MT
HF
R6
77
(OR
:2
.09;
95
%C
I:
1.0
4,4
.18;
P,
0.0
4).
MT
HF
R6
77
/MT
HF
R
12
98
(OR
:1
.64
;9
5%
CI:
1.0
,2
.69
;P,
0.0
5);
and
MT
HF
67
7/R
FC
80
(OR
:1
.8;
95
%C
I:1
.02,
3.1
8;P
=0
.04
).
Sm
all
sam
ple
nu
mb
ers.
Sour
ceof
case
san
d
con
tro
lsn
ot
pro
vid
ed.
Un
bli
nd
ed.
Ram
aek
ers
etal
,2
00
7(4
4)
(Ger
man
y)
Cas
eco
ntr
ol
III-
3
Cas
es=
25
.S
eeT
able
1.
DS
M-I
V,
AD
OS
,A
DI,
VA
BS
.
Muta
tions
of
fola
tere
cepto
r
gen
es.
Co
din
gex
on
so
fF
R1
and
FR
2sh
owed
no
rmal
sequen
ces.
Sm
all
sam
ple
size
.S
tud
y
un
bli
nd
ed.
Mo
rett
iet
al,
20
08
(38
)
(US
A)
Cas
ese
ries
IV
Cas
es=
7.
See
Tab
le1
.A
DO
S,
AD
I-R
,B
aile
y,
VA
BS
.
Mu
tati
on
so
fg
enes
invo
lved
info
late
met
abo
lism
.
Th
ere
wer
en
om
uta
tio
ns
of
fola
tere
cepto
rgen
es
(RF
C-1
,F
R1,
FR
2,
PC
FT
),M
TH
FR
,
DH
FR
,o
r
form
ino
tran
sfer
ase
cycl
od
eam
inas
e.
Sm
all
sam
ple
size
.S
tud
y
un
bli
nd
ed.
1D
SM
-IV
and
DS
M-I
V-R
,D
iag
no
stic
and
Sta
tist
ical
Man
ual
of
Men
tal
Dis
ord
ers,
4th
edit
ion
,an
dD
iag
nost
ican
dS
tati
stic
alM
anua
lo
fM
enta
lD
isor
der
s,4
thed
itio
n,
rev
ised
;C
AR
S,
Ch
ild
ho
odA
uti
sm
Rat
ing
Sca
le;
OR
,o
dd
sra
tio;
PD
D-N
OS
,p
erva
sive
dev
elo
pmen
tal
dis
ord
ers–
not
oth
erw
ise
spec
ified
;A
DO
S,
Au
tism
Dia
gn
ost
icO
bse
rvat
ion
Sch
edu
le;
AD
I-R
,A
uti
smD
iag
nost
icIn
terv
iew
–re
vis
ed;
VA
BS
,
Vin
elan
dA
dap
tive
Beh
avio
ur
Sca
le.
MT
HF
R,
met
hy
len
ete
trah
yd
rofo
late
;A
SD
s,au
tism
spec
trum
dis
ord
ers;
bp
,b
ase
pai
r.
FOLATE-METHIONINE PATHWAY AND AUTISM 1617
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

In addition, James et al (29) and Adams et al (36) reportedborderline associations between some genes of the methioninepathway and autism. The power for both studies, however, wasinsufficient to provide more than an indication of possible geneassociations and neither corrected probability values for chanceeffects due to multiple comparisons.
Folate cycle
Folate metabolism is complex. 5-MTHF and vitamin B-12 arerequired for the conversion of homocysteine into methionine byMS. Low MS activity could lead to an accumulation of 5-MTHF,and intracellular folate retention may be impaired. No signifi-cant association between polymorphisms of MS and autism,however, has been shown (36). Furthermore, various studieshave reported vitamin B-12 and erythrocyte folate concentrationsare normal in children with autism (31, 36, 39, 40). Un-fortunately, these studies did not identify or control for potentialconfounders, such as age, neurologic symptoms, or supple-mentation with cofactors for the folate-methionine pathway.None of the studies reported on plasma concentrations ofmethylmalonic acid, which is the functional indicator of vitaminB-12 status.
Many biomedical interventions for treating autism have beentouted, although most lack an evidence base (47). Whereas Jameset al (28) showed that supplementation with folinic acid andbetaine normalized the plasma concentrations of metabolites inthe methionine pathway, and the addition of vitamin B-12 furtherimproved these concentrations, significant autism behavioraloutcomes were not measured or observed. On the other hand,supplementation with folinic acid led to improved CFS folatestatus and remarkable cognitive, motor, and neurologic changesin 15 of 18 children with low-functioning autism and at least onesymptom of CFD (44). This was particularly apparent in youngerchildren, which suggests that damage caused by metabolicdysfunction over time has a degree of irreversibility. The abilityto replicate this result by showing an association of neurologicbenefits with changes in CSF folate concentration is limited,however, because obtaining CSF folate is a highly invasiveprocedure.
Vitamin B-6 is required for the conversion of THF to 5,10-MTHF and homocysteine to cysteine via cystathionine. Thesignificant increases in serum vitamin B-6 observed in childrenwith autism (31, 40, 41, 43) could reflect diminished cellularuptake or inefficacy of cells to retain or store vitamin B-6. Im-paired bioavailability of vitamin B-6 may affect the nervoussystem because it is required for the synthesis of neuro-transmitters, including serotonin, dopamine, and taurine (48).
Folate metabolism can also be impaired by 2 polymorphismsof MTHFR, MTHFR 677C/T, and MTHFR 1298A/C, whichlower enzyme activity, reduce DNA methylation, and possiblyincrease chromosomal instability (49–51). MTHFR is a pivotalenzyme that catalyses the reduction of 5,10-MTHF into 5-MTHF, which is the major circulating form of folate, and acts asa methyl donor in the remethylation of homocysteine to me-thionine. Whereas Boris et al (45) reported a significant asso-ciation for the homozygote MTHFR 677C/T and thecompound heterozygote MTHFR 677C/T/1298A/C and au-tism, other studies did not confirm the association (29, 36),which may be affected by folate and riboflavin status. The role
of this enzyme in autism, therefore, remains unclear; however,again, the studies lacked the power needed to more than indicatea potential association and did not correct for multiple com-parisons. Furthermore, Boris et al (45) used genotype data from2 different sources outside of the study population as controls,which means that cases and controls were not truly matched.
No studies were found that examined the association betweenMTHFD, an enzyme that catalyses 3 sequential reactions in theinterconversion of one-carbon derivatives of tetrahydrofolate,and autism. A borderline association was, however, reportedbetween a 19-bp deletion of DHFR and autism (36). DHFRmaintains the reduced form of folate required for de novo syn-thesis of methionine and thymine; however, as noted above, thisstudy lacked power and did not correct for multiple compar-isons, which made the association tenuous.
James et al (29) reported a significant association betweenRFC-1 80G/A (OR: 2.13; 95% CI: 1.3, 3.4), and Adams et al(36) reported a borderline association between RFC-1 80G/Aand 19-bp del-DHFR (OR: 1.8; 95% CI: 1.02, 3.18) and autism.Their findings suggest that folate transport may be involved in thedevelopment of autism; however, as discussed above, both studieslacked power and did not correct for multiple comparisons.
High titers of auto-antibodies to FR1 were reported in childrenwith low-functioning autism and at least one symptom of CFD(44), although mutations in FR1 or FR2 were not found andmothers did not have the antibody, which led the authors tospeculate that it may have been formed from milk protein (38,44). The plausibility of an association of FR1 auto-antibodieswith neural deficits is supported by the observations of antibodiesagainst placental FR proteins being associated with neural tubedefects (52).
Conclusions
A better understanding of the metabolic basis of autism has thepotential to guide the development of a laboratory-based “test” todiagnose autism, predict the outcome of disease, and assign themost appropriate intervention. Although the findings of this re-view do not conclusively implicate a dysfunctional folate-me-thionine pathway in the etiology of autism, the topic clearlydeserves scrutiny. Any review of evidence will be confounded bythe heterogeneity of autism, sampling issues, and the wide rangeof analytic techniques used. Given the increase in communityawareness of autism in recent years and the consequent increasedfocus on autism research, the findings of the more recentlypublished studies are likely to be more reliable, although they arestill inconsistent. These findings suggest that changes in theconcentrations of metabolites of the methionine cycle may bedriven by abnormalities in folate transport and/or metabolism.Almost all of the genetic association studies that have examinedthe genes of this metabolic pathway were under powered. Asautism is a complex genetic disease, the relative risk conferred byeach disease-associated allele is likely to be small; therefore,large patient and control groups are required for statistical sig-nificance. Furthermore, many of the studies examined multiplepolymorphisms and their interactions without correcting formultiple comparisons may have been better analyzed by usinglogistic regression analysis.
Whereas supplementation can normalize the concentrations ofthe folate-methionine metabolites, whether or not normalization
1618 MAIN ET AL
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

affects objective behavioral measures needs to be determined toassess the clinical relevance. Supplementation has been shown tobe most effective in improving autistic behavior, motor, andneurologic symptoms in younger children (aged ,3 y) with low-functioning autism and CFD (44); however, it remains to be seenwhether this holds for children with autistic disorder withoutCFD. Large-scale studies that link normalization of metaboliteconcentrations with genetic polymorphisms and objective be-havioral measures are needed to address these issues. In addi-tion, a large-scale retrospective survey should be conducted inmothers of children with and without autism to ascertain theassociation level of folate supplementation before and duringpregnancy with the risk of having a child with autism andwhether susceptibility genes in the folate-methionine pathwaymodify such a risk if present. Overall, this review concluded thatevidence suggests a role for the folate-methionine pathway inautism and suggests some future directions for research.
The authors’ responsibilities were as follows—PAEM: planned,
researched, and drafted the manuscript; and CEO, MF, PT, and MTA:
reviewed the manuscript. There were no potential conflicts of interest.
REFERENCES1. American Psychiatric Association. Diagnostic and statistical manual of
mental disorders: text revision (DSM-IV-R). Washington, DC: AmericanPsychiatric Association, 2000.
2. Fombonne E. Epidemiological surveys of autism and other pervasive de-velopmental disorders: an update. J Autism Dev Disord 2003;33:365–82.
3. Autism Genome Project Consortium, Szatmari P, Paterson AD, et al.Mapping autism risk loci using genetic linkage and chormosomal re-arrangments. Nat Genet 2007;39:319–28.
4. Morrow EM, Yoo S-Y, Flavell SW, et al. Identifying autism loci andgenes by tracing recent shared ancestry. Science 2008;321:218–23.
5. Christian SL, Bune CW, Sudi J, et al. Novel submicroscopic abnor-malities detected in autism spectrum disorder. Biol Psychiatry 2008;63:1111–7.
6. Geschwind DH, Levitt P. Autism spectrum disorders: developmentaldisconnection syndromes. Curr Opin Neurobiol 2007;17:103–11.
7. Grandjean P, Landrigan PJ. Developmental neurotoxicity of industrialchemicals. Lancet 2006;368:2167–77.
8. Kern JK, Jones AM. Evidence of toxicity, oxidative stress and neuronalinsult in autism. J Toxicol Environ Health B Crit Rev 2006;9:485–99.
9. Slotkin TA, Vevin ED, Seidler FJ. Comparative developmental neuro-toxicity of organophsphate insecticides: effects on brain developmentare separable from systemic toxicity. Environ Health Perspect 2006;114:746–51.
10. van den Pol AN. Viral infections in the developing and mature brain.Trends Neurosci 2006;29:398–406.
11. Horvath K, Perman J. Autistic disorder and gastrointestinal disease. CurrOpin Pediatr 2002;14:583–7.
12. White JF. Intestinal pathophysiology in autism. Exp Biol Med (May-wood) 2003;228:639–49.
13. Das SK, Kunkel TA, Loeb LA. Effects of altered nucleotide concentrationson the fidelity of DNA replication. Basic Life Sci 1985;31:117–26.
14. Selhub J, Rosenberg IH. Folic acid. In: Ziegler EE, Filer LJ Jr, eds.Present knowledge in nutrition. 7th ed. Washington, DC: InternationalLife Sciences Institute Press, 1996:206–19.
15. Barbato JC, Catanescu O, Murray K, DiBello PM, Jacobsen DW. Tar-geting of metallothioneine by L-homocysteine: a novel mechanism fordisruption of zinc and redox homeostasis. Arterioscler Thromb VascBiol 2007;27:49–54.
16. Fang YZ, Yang S, Wu G. Free radicals, antioxidants and nutrition.Nutrition 2002;18:872–9.
17. Schafer FQ, Beuttner GR. Redox environment of the cell as viewedthrough the redox state of the glutathione disulfide/glutathione couple.Free Radic Biol Med 2001;30:1191–212.
18. Petrozzi L, Lucetti C, Scarpato R, et al. Cytogenetic alterations inlymphocytes of Alzheimer’s disease and Parkinson’s disease patients.Neurol Sci 2002;23(suppl):S97–8.
19. Thomas P, Hecker J, Faunt J, Fenech M. Buccal micronucleus cytomebiomarkers may be associated with Alzheimer’s disease. Mutagenesis2007;22:371–9.
20. Thomas P, Harvey S, Gruner T, Fenech M. The buccal cytome andmicronucleus frequency is substantially altered in Down’s syndrome andnormal ageing compared to young healthy controls. Mutat Res 2008;638:37–47.
21. Psimadas D, Messini-Nikolaki N, Zafiropoulou M, Fortos A, TsilimigakiS, Piperakis SM. DNA damage and repair efficiency in lymphocytesfrom schizophrenic patients. Cancer Lett 2004;204:33–40.
22. Muntjewerff JW, Van der Put N, Eskes T, et al. Homocysteine metab-olism and B-vitamins in schizophrenic patients: low plasma folate asa possible independent risk factor for schizophrenia. Psychiatry Res2003;121:1–9.
23. Chou YF, Yu C, Huan RS. Changes in mitochondrial DNA deletion,content, and biogenesis in folate-deficient tissues of young rats dependon mitochondrial folate and oxidative DNA injuries. J Nutr 2007;137:2036–42.
24. Chou YF, Huang RS. Mitochondrial DNA deletions of blood lympho-cytes as genetic markers of low folate-related mitochondrial genotox-icity in peripheral tissues. Eur J Nutr 2009;48:429–36.
25. Djukic A. Folate-responsive neurologic diseases. Pediatr Neurol 2007;37:387–97.
26. Schopler E, Reichler R, Renner B. Toward objective classification ofchildhood autism: Childhood Autism Rating Scale (CARS). J AutismDev Disord 1980;10:91–103.
27. National Health and Medical Research Council. A guide to the de-velopment, implementation and evaluation of clinical practice guidelines.Canberra, Australia: Australian Governement Publishing Service, 1999.
28. James SJ, Cutler P, Melnyk S, et al. Metabolic biomarkers of increasedoxidative stress and impaired methylation capacity in children withautism. Am J Clin Nutr 2004;80:1611–7.
29. James SJ, Melnyk S, Jernigan S, et al. Metabolic endophenotype andrelated genotypes are associated with oxidative stress in children withautism. Am J Med Genet B Neuropsychiatr Genet 2006;141:947–56.
30. Suh JH, Walsh, WJ, McGinnis WR, Lewis A, Ames BN. Altered sulfuramino acid metabolism in immune cells of children diagnosed withautism. Am J Biochem Biotech 2008;4:105–13.
31. Khaleeluddin K, Philpott WH. I. The clinical report of ecologic andnutritional disorders in chronic mental and physical degenerative dis-eases. II. The significance of B6 and methionine metabolic disorders inmental disease. J Appl Nutr 1980;32:37–52.
32. Visconti P, Piazzi S, Posar A, Santi A, Pipitone E, Rossi PG. Aminoacids and infantile autism. Dev Brain Dysfunct 1994;7:86–92.
33. D’Eufemia P, Finochhiaro R, Celli M, Viozzi L, Monteleone D, FiardiniO. Low serum tryptophan to large neutral amino acids ratio in idiopathicinfantile autism. Biomed Pharmacother 1995;49:288–92.
34. Arnold GL, Hyman SL, Mooney RA, Kirby RS. Plasma amino acidsprofiles in children with autism: potential risk of nutritional deficiencies.J Autism Dev Disord 2003;33:449–54.
35. Moretti P, Sahoo T, Hyland K, et al. Cerebral folate deficiency withdevelopmental delay, autism and response to folinic acid. Neurology2005;64:1088–90.
36. Adams M, Lucock M, Stuart J, Fardell S, Baker K, Ng X. Preliminaryevidence for involvement of the folate gene polymorphism 19-bpdeletion-DHFR in occurrence of autism. Neurosci Lett 2007;422:24–9.
37. Pasca S, Nemes B, Vlase L, et al. High levels of homocysteine and lowserum paraoxonase 1 arylesterase activity in children with autism. LifeSci 2006;78:2244–8.
38. Moretti P, Peters SU, del Gaudio D, et al. Brief report: autistic symp-toms, developmental regression, metal retardation, epilepsy and dyski-nesias in CNS folate deficiency. J Autism Dev Disord 2008;38:1170–7.
39. Siva Sankar DV. Plasma levels of folates, riboflavin, vitamin B6 and ascor-bate in severely disturbed children. J Autism Dev Disord 1979;9:73–82.
40. Lowe TL, Cohen DJ, Miller S, Young JG. Folic acid and B12 in autismand neuropsychiatric disturbances of childhood. J Am Acad ChildAdolesc Psychiatry 1981;20:104–11.
41. Adams JB, Holloway C. Pilot study of a moderate dose multi-vitamin/mineral supplement for children with autistic spectrum disorder.J Alt Complement Med 2004;10: 1033–9. (Published erratum appears inJ Alt Complement Med 2004;11.)
42. Ramaekers VT, Rothenberg S, Sequeira JM, et al. Autoantibodies tofolate receptors in the cerebral folate deficiency syndrome. N Engl JMed 2005;352:1985–90.
FOLATE-METHIONINE PATHWAY AND AUTISM 1619
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

43. Adams JB, George F, Audhya T. Abnormally high plasma levels of
vitamin B6 in children with autism not taking supplements compared to
controls not taking supplements. J Altern Complement Med 2006;12:
59–63.44. Ramaekers VT, Blau N, Sequeria JM, Nassogne MC, Quadros EV.
Folate receptor autoimmunity and cerebral folate deficiency in low-
functioning autism with neurological defects. Neuropediatrics 2007;
38:276–81.45. Boris M, Goldblatt A, Goalanko J, James SJ. Association of MTHFR
gene variants with autism. J Am Phys Surg 2004;9:106–8.46. Bolander-Gouaille C, Bottiglieri R. Homocysteine: related vitamins and
neuropsychiatric disorders. 2nd ed. Paris, France: Springer-Verlag, 2007.47. Angley M, Semple S, Hewton C, Paterson F, McKinnon R. Children and
autism: Part 2 - management with complementary medicines and dietary
interventions. Aust Fam Physician 2007;36:827–30.
48. Gerster H. The importance of vitamin B6 for development of the infant:human medical and animal experimental studies. Z Ernahrungswiss1996;35:309–17 (in German).
49. Kimura M, Umegaki K, Higuchi M, Thomas P, Fenech M. Methyl-enetetrahydrofolate reductase C677T polymorphism, folic acid and ri-boflavin are important determinants of genome stability in culturedhuman lymphocytes. J Nutr 2004;134:48–56.
50. Coppede F, Colognato R, Bonelli A, et al. Polymorphisms in folate andhomocysteine metabolizing genes and chromosome damage in mothersof Down Syndrome children. Am J Med Genet A 2006;143A:2006–15.
51. Iarmarcovai B, Bonassi S, Botta A, Baan RA, Orsie’re T. Geneticpolymorphisms and micronucleus formation: a review of the literature.Mutat Res 2008;658:215–33.
52. Rothenberg SP, Da Costa MP, Sequeira JM, et al. Autoantibodies againstfolate receptors in women with a pregnancy complicated by a neural-tubedefect. N Engl J Med 2004;350:134–42.
1620 MAIN ET AL
by guest on May 11, 2016
ajcn.nutrition.orgD
ownloaded from

Erratum
Main PAE, Angley MT, Thomas P, O’Doherty CE, Fenech M. Folate and methionine metabolism in autism: a systematicreview. Am J Clin Nutr 2010;91:1598–620.
On page 1614, in the last paragraph of Results, the second and third sentences are as follows: ‘‘Although the largest study todate found a significant association between RFC-1 80G/A and autism (OR: 2.13; 95% CI: 1.4, 3.4) (29), a subsequent studyfailed to replicate the findings (37). On the other hand, an association was found between the 19-bp deletion of DHFR andRFC-1 with autism (36).’’
These sentences should be replaced with the following: ‘‘The largest study to date found a significant association betweenRFC-1 80G/A and autism (OR: 2.13; 95% CI: 1.4, 3.4) (29), but a smaller, inadequately powered study found no associationwith this polymorphism (36).’’
doi: 10.3945/ajcn.2010.30167.
Erratum
Yang Q, Cogswell ME, Hamner HC, et al. Folic acid source, usual intake, and folate and vitamin B-12 status in US adults:National Health and Nutrition Examination Survey (NHANES) 2003–2006. Am J Clin Nutr 2010;91:64–72.
In Table 2 on page 68, the median, 25th percentile, and 75th percentile values should be changed as follows: For adult maleswho consumed ECGP1RTE1SUP, the median (interquartile range) usual folic acid intakes should be 653 (528, 801) lg/d, not687 (552,849) lg/d. For adults aged 40–59 y who consumed ECGP only, the 75th percentile of usual vitamin B-12 intakeshould be 6.9 lg/d, not 6.8 lg/d; and for all adults aged 40–49 y (‘‘Total’’), the 25th percentile of usual vitamin B-12 intakeshould be 4.5 lg/d, not 4.2 lg/d. For non-Hispanic white adults who consumed ECGP1RTE1SUP, the 75th percentile of usualfolic acid intake should be 806 lg/d, not 896 lg/d. For non-Hispanic black adults who consumed ECGP1SUP, the 75thpercentile of usual vitamin B-12 intake should be 26.0 lg/d, not 23.8 lg/d. For Mexican American adults who consumed ECGPonly, the median and 25th percentile of usual folic acid intake should be 149 and 114 lg/d, respectively, not 114 and 149 lg/d.The estimates were not adjusted for interview method. The footnote for Table 2 and for Supplemental Table 1 in the onlineissue should therefore read ‘‘. . .were adjusted for participant ID, age, sex, race-ethnicity, and day of the week.’’ Similarly onpage 66, in the third paragraph under Statistical analyses, the first sentence should read, ‘‘In PC-SIDE, all analyses wereadjusted for age, sex, race-ethnicity, and day of the week.’’ These corrections do not change the interpretation of the results orany of the results presented in the text.
doi: 10.3945/ajcn.2010.30166.
Erratum
George SM, Park Y, Leitzmann MF, et al. Fruit and vegetable intake and risk of cancer: a prospective cohort study. Am J ClinNutr 2009;89:347–53.
In Table 1 on page 349, a few values are incorrect. For ‘‘Fruit (cup equivalents/1000 kcal),’’ the value in the ‘‘Fruit/Men/Q5’’column should be 2.1 instead of 1.4. For ‘‘Vegetable (cup equivalents/1000 kcal),’’ the values in the ‘‘Vegetable/Women/Q5,’’‘‘Vegetable/Men/Q1,’’ and ‘‘Vegetable/Men/Q5’’ columns should be 1.8 instead of 1.4, 0.3 instead of 0.8, and 1.4 instead of 1.3,respectively. In addition, in the right-hand column of page 351, the second sentence of the first full paragraph contains an error:the second instance of ‘‘nonsmokers’’ should be ‘‘smokers’’ instead. The sentence should read as follows: ‘‘Also, in general,nonsmokers had higher average median intakes of fruit and vegetables than did smokers.’’
doi: 10.3945/ajcn.2010.30168.
LETTERS TO THE EDITOR 1001






![Serum Levels of Homocysteine, Vitamin B12 and Folate in ... · methyltetrahydrofolate and methyl-Vitamin-B12 are essential factors for methionine synthesis of Hcy [10]. Lacking Vitamin](https://static.fdocuments.net/doc/165x107/5ec906dfa105b02e13239827/serum-levels-of-homocysteine-vitamin-b12-and-folate-in-methyltetrahydrofolate.jpg)

![J Neurol Disord 2013, 1:1 Neurological Disorders · of two metabolic cycles: the SAM cycle and the folate cycle [1,12]. The . SAM cycle begins with influx of methionine from the diet,](https://static.fdocuments.net/doc/165x107/5c17507f09d3f29c288b598a/j-neurol-disord-2013-11-neurological-disorders-of-two-metabolic-cycles-the.jpg)









