Focus On Veraflox
12
Pyoderma Inside features... PLUS more facts about this important issue Joe Blondeau discusses the mutant prevention concentration (MPC) in relation to dermatology Paul Coward outlines the bacterial cause of pyoderma and treatment options
-
Upload
markettiers4dc-markettiers4dc -
Category
Documents
-
view
225 -
download
2
description
Focus On Veraflox
Transcript of Focus On Veraflox

Pyoderma
Inside features...
PLUS more facts about this important issue
Joe Blondeau discusses the mutant prevention concentration (MPC) in relation to dermatology
Paul Coward outlines the bacterial cause of pyoderma and treatment options

The skin from inside out is formed of the dermis and the adnexal structures, the basement membrane and the epidermis. Together these layers provide physical,
microbial and chemical barriers and form part of the skin immune system.
The dermis is a support matrix that also produces secretions to maintain the epidermis and adnexal structures. It is formed of connective tissue (collagen, elastic fibres and ground substance), blood vessels, nerves, lymphatic vessels and cellular components (fibroblasts and mast cells).
The adnexae comprise the hair follicles, the sebaceous and sweat glands. As well as its barrier functions, the hair also aids camouflage and behaviour, while the sebum produced by the sebaceous glands combines with secretions from the sweat glands to form an emulsion on the epidermal surface that also has protective and behavioural roles.
The basement membrane anchors the cells of the epidermis onto the dermis and is the interface between the two, through which nutrients, chemicals and immune cells pass.
FOCUS ON – Foreword
T his “Focus On...” brochure is the next in the series to provide key information on pyoderma, as
one of the most common skin problems seen in dogs. Dermatological problems are a daily part of veterinary practice and as such, the following pages are intended to provide a succinct overview of this common complaint in dogs.
Anita Patel provides an introduction to the skin as an organ, as well as its functions. In addition, Paul Coward, who runs a dermatology referral service, discusses pyoderma, its bacterial causes and the necessary treatment.
Dr. Joe Blondeau – a clinical microbiologist whose main research interests include the areas of antimicrobial agents and antimicrobial resistance, clinical microbiology and outcomes associated with antimicrobial therapy – focuses on Mutant Preventation Concentration, in relation to dermatology and pradofloxacin.
Veraflox® (pradofloxacin) is an innovative next-generation veterinary fluoroquinolone, licensed for the treatment of superficial and deep pyoderma in dogs.
Anita Patel BVM, DVD, MRCVS, RCVS-recognised specialist in Veterinary Dermatology
Anita Patel is a recognised RCVS specialist in Veterinary Dermatology and has been running a busy referral practice in the south-east of England for the last 12 years, prior to which she was in general practice.
Anita has co-authored the chapter on structure and function of skin in the BSAVA Small Animal Dermatology Manual. She has also published papers in journals and authored the chapter on feline pyoderma in Consultations in Feline Internal Medicine. She co-authored a case-based text book, Saunders’ “Solutions in Veterinary Practice: Small Animal Dermatology” and has written chapters in other texts.
Focus On Pyoderma
Skin and its functionBy Anita Patel

THE EPIDERMIS IS FORMED OF FOUR LAYERS: The basal layer, the innermost layer of tightly packed columnar cells, proliferates to produce daughter cells, which migrate upwards into the spinous layer.
The spinous layer, the next layer up, is composed of polygonal cells which undergo a complex chain of biochemical and structural changes. This process, referred to as differentiation, is vital for the formation of the epidermal barrier.
The granular layer is characterised by keratohyalin granules and lamellar bodies. These structures undergo biochemical changes to provide structural strength and form the epidermal lipid barrier.
The corneal layer is formed of tightly packed, flattened, anucleate keratinocytes, interspersed with epidermal lipids. This layer plays a major protective role, providing a selectively permeable barrier, mechanical strength, hydration, UV protection and immune surveillance. The cells from the surface are lost through the process of desquamation.
The skin immune system is composed of the resident and transient cells of the epidermis and dermis. These include the keratinocytes, Merkel cells, Langerhans’ cells, fibroblasts, dermal dendrocytes, mast cells, T-lymphocytes, neutrophils, eosinophils, macrophages and melanocytes. They play a role in both innate and adapted immune responses, through the secretion of cytokines, antimicrobial peptides as well as antigen presentation.
Thus the skin, the largest organ of the body, provides a homoeostatic environment for the optimal function of all other organs it encloses and is adapted to provide protection against microbial, chemical and mechanical insults.
Focus On Pyoderma
1
2
1 Corneocyte 2 Intercellular lipid lamella
Corneal layer(Stratum corneum)
Spinous layer(Stratum spinosum)
Basal layer(Stratum basale)
Granular layer(Stratum granulosum)

Pyoderma: common in small animal practice By Paul Coward
P yoderma is one of the most common skin problems seen in small animal practice but continues
to present a significant challenge. With increasing concern over resistant infections in both man and animals it is important that antibiotics are used appropriately.
Pyoderma is classified according to the depth of infection. These are surface (acute moist dermatitis and fold infections), superficial (juvenile pyoderma, superficial pyoderma and superficial folliculitis) and deep (deep folliculitis and furunculosis). Whilst a number of bacteria have been associated with pyoderma, by far the most frequent are staphylococci, particularly Staphylococcus pseudintermedius.
Systemic antibiotic therapy will be required for most superficial pyoderma and all deep pyoderma but should be avoided if possible in surface pyoderma, juvenile pyoderma and mild superficial pyoderma. The increased use of antibacterial shampoos, antibacterial skin wipes and antibacterial gels will reduce antibiotic use and should reduce the development of antibiotic-resistant strains of bacteria.
When antibiotics are indicated, consideration should be given to the appropriate choice of medication together with adequate dose and duration of therapy. In most cases, the initial antibiotic chosen will be cephalexin, amoxyclav or clindamycin. Fluoroquinolones are kept in reserve and prescribed only when culture and sensitivity indicate that they are required. Skin infections require longer courses of antibiotics than many internal infections and a minimum of three weeks should be used for superficial pyoderma that has not responded to topical therapy alone. The animal should be re-examined prior to cessation of antibiotics so that treatment can be extended until full resolution is achieved. Sampling for bacterial culture and sensitivity testing is indicated in all cases that fail to respond to initial therapy and for all cases of deep pyoderma, where an extended course of antibiotics will be required. Ideally, existing antibiotics should be stopped prior to taking samples for bacterial culture. In cases of deep pyoderma that are responding poorly to therapy it is worth considering submitting a punch biopsy to enable culture of the deeper tissue.
Treating the infection effectively is very important but is still only half of the job. Most cases of pyoderma are secondary to factors that have reduced the dog’s ability to resist infection and further investigation will be required if frequent recurrence is to be avoided.
Paul Coward, BVSc BSc CertSAD MRCVS
Paul has degrees in Physiology (1977) and Veterinary Science (1981) both from Liverpool University. He spent ten years in general practice before completing the RCVS Certificate in Small Animal Dermatology.
Paul has run a dermatology referral service based in Dorset since 1991 and now also works two days a week in the University of Bristol Small Animal Hospital where he is a member of the dermatology team. Paul is a past president of the British Veterinary Dermatology Study Group and member of the European Society of Veterinary Dermatology.
Focus On Pyoderma
5
4
3
2
1
1 Demodex mite
2 Bacteria
3 Macrophage
4 Deep pyoderma
5 Furunculosis

1 Demodex mite
2 Bacteria
3 Macrophage
4 Deep pyoderma
5 Furunculosis
There are many causes of pyoderma in cats and dogs – including parasites:
FLEAS AND FLEA ALLERGY DERMATITIS (FAD)Hypersensitivity to antigenic material contained in flea saliva not only causes itching and irritation after a flea bite but it is also the major cause of FAD.
In dogs, FAD typically occurs as hot spots; in cats it takes the form of miliary dermatitis. It is the most common allergic skin disease of dogs and cats and is most prevalent in the summer months. All breeds and ages are susceptible.
The clinical signs of flea allergy in the dog and cat, such as lesions, seborrhoea and alopecia, are the result of pruritus and self-trauma. The classic primary skin lesion in the hypersensitive dog or cat is a small pruritic, erythematous wheal noted at the site of the flea bite.
With prolonged exposure to fleas, the acute primary lesions are rapidly replaced by chronic secondary lesions that result from pruritus and repeated self-trauma.
Dermatitis in the dog is typically confined to the dorsal lumbosacral area, but sometimes affects the caudomedial thighs, ventral abdomen and flank.
DEMODEX CANIS Many dogs carry Demodex canis mites as part of their normal skin flora without showing any signs of skin disease. However, in some individuals, the mite numbers increase, and cause visible signs of disease. The reasons for this are varied; some individuals are thought to be genetically predisposed to the disease, and initiating factors such as alterations in the immune system (e.g. from underlying disease, hormonal changes or immunosuppressive therapy, amongst others) may contribute to a flare-up of disease. Two types of demodectic mange are clinically recognised, depending on the extent of the lesions: a localised and a generalised type. The generalised type is further subdivided into juvenile-onset and adult-onset demodectic mange.
Localised demodicosis is usually characterised by small patches of hair loss and inflammation of the skin. The most common areas affected are the face (especially around the eyes and mouth) and the front legs. Cases usually occur in young dogs and the disease is often mild, with many cases resolving without the need for treatment, although the symptoms can last for several months.
Generalised demodicosis involves similar skin lesions, but affects a much larger area of the skin, and can be classed as either juvenile-onset or adult-onset depending on the age of presentation. Generally, if the condition presents in animals over 4 years old, where no previous history of demodicosis exists, this is classed as adult onset demodicosis. Generalised demodicosis can be a difficult condition to treat, with true adult-onset disease being especially problematic, as these animals often have some kind of underlying disease which has precipitated the increase in mite numbers.
For more information on parasites and parasite protection plans for your clients, please visit jungleforvets.co.uk
Focus On Pyoderma

An introduction to Veraflox®
The only next generation FQ licensed in veterinary medicine
• Veraflox®rapidlyfightsbacteriawithhigh-activitydualmoleculartargeting1
• Veraflox®offersanenhancedspectrumofantimicrobialactivitywhencomparedtootherfluoroquinolones2,3
• WiththelowestavailableMICandMPCvalues*comparedtootherlicensedveterinaryfluoroquinolones,Veraflox®canbeexpectedtodeliversuperiorperformance4andtherebyhelpreducetheriskoffluoroquinoloneresistance5
• Indogs,Veraflox®provideseffectivetreatmentinaonce-daily,flavouredtablet
*refers to licensed indications
Dual Molecular Targeting
DNA gyrase
Topoisomerase IV
High dual binding affinity blocks DNA replication
Pradofloxacin
Focus On Pyoderma
A data sheet for each formulation is supplied at the back of this brochure
Pradofloxacin

Serum 1.6Skin 2.34
VERAFLOX®
: HIGH TISSUE PENETRATION
Focus On Pyoderma
Veraflox®demonstrateshighactivityagainstrelevantveterinarypathogens,withenhancedefficacyagainstGram-positivebacteria,suchastheStaphylococcus intermedius group
IN VITRO ACTIVITY AGAINST CANINE AND FELINE STAPHYLOCOCCI6
Pathogen Fluoroquinolone
MIC parameter (µg/ml)
MICrange(µg/ml)
MIC50
(µg/ml)MIC90
(µg/ml)MIC90S
(µg/ml)Geo.Mean
MIC
Staphylococcusintermediusgroup
(includingS.pseudintermedius)
(n=988)
pradofloxacin 0.016–8.0 0.06 0.06 0.06 0.052
marbofloxacin 0.03–64.0 0.25 0.5 0.5 0.300
ibafloxacin 0.016–128.0 0.12 0.25 N/A 0.150
MIC = minimum inhibitory concentration MIC90S = MIC90 of the susceptible population

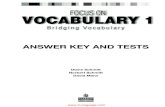
Deep Pyoderma
100
90
80
70
60
50
40
30
20
10
0Pradofloxacin Amoxicillin-
clavulanic acid
Per
cent
age
Clinical Remission Rates
73%
86%
12
10
8
6
4
2
0Pradofloxacin
Relapse Rates
Amoxicillin-clavulanic acid
0%*
*P=0.0082
Per
cent
age
11%
• 86%ofdogstreatedforthedifficultconditionofdeeppyodermadisplayedrapidclinicalremission7
• Veraflox®provedsignificantlymoreeffectivethanamoxicillin-clavulanicacidatpreventingtherelapseofpyoderma;twoweeksaftercessationoftherapy,norelapsesofdeeppyodermawereobserved,followingtreatmentwithVeraflox®7
Focus On Pyoderma
Deep pyoderma with cellulitis on dog‘s chin Electron-microscopic image of Staphylococci colonising skin surface

Focus On Pyoderma
Clinical Case Study: 1.5 Year Old Male Lurcher (23 kg) BelowisarecentcasestudythatdemonstrateshowVeraflox®wasusedtoresolveaproblematicinfection.
CASE STUDY
CONCLUSION
Superficial pyoderma secondary to atopic dermatitis
EXAMINER
Clinician Mr Paul S. Coward
Specialisation Veterinary Dermatology
Clinic name Mr. Paul S. Coward Veterinary Dermatology
Address Verwood, Dorset BH31 6BL, United Kingdom
CASE HISTORY
Species Canine
Age 1.5 years
Breed Lurcher
Gender Male neutered
Weight 23 kg
INITIAL VISIT
Patient history; Pruritus and recurrent ventral pyoderma
– Treated with repeated courses of antibiotics and a hypoallergenic diet trial
– Diagnosis of superficial pyoderma secondary to atopy
– Intradermal allergy testing: multiple positive results
Treatment with extended course of oral cephalexin and allergen-specific immunotherapy. Dog otherwise well.
Physical examination;
– Ventral pruritus
– Papular rash ventral abdomen and groin despite extended course of cephalexin (49 days) at appropriate dose and twice weekly washes with chlorhexidine-based shampoo
Bacterial culture; 1. Staphylococcus pseudintermedius 2. Bacillus species
Antibiogram Bacillus spp.
Amoxicillin/clavulanic acid S I RCephalexin S I REnrofloxacin S I RMarbofloxacin S I ROxacillin S I RPradofloxacin S I R
Diagnosis; Superficial pyoderma secondary to atopic dermatitis
Treatment;
– Veraflox® 60 mg tablets: 1.5 tablets once daily
– Chlorhexidine-based wash twice weekly continued
– Allergen-specific immunotherapy commenced
Follow-up visit 1 | Day 35
– Pyoderma lesions resolved
– Pruritus reduced but still present
– Continue immunotherapy and twice weekly chlorhexidine-based washes
COMMENTS
Number of days of Veraflox® treatment until cure = 27 days
Whilst the culture results suggested the S pseudintermedius was sensitive to cephalexin, the response to therapy was poor. The bacillus was resistant so the antibiotic was changed to Veraflox® and a good response was seen.•Secondarysuperficial
pyodermarefractorytoconventionaltreatment.
•CausedbyresistantBacillusspp.
•Completecureafter27daysofpradofloxacintreatment.

MPC and Dermatology in Companion Animals Dr. Joe Blondeau
Clinicians prescribe antimicrobial agents to effect clinical cure of infectious diseases. The
premise is based on the observation that in a patient presenting with signs suggested or proven to have pathogenic organisms causing infection, the use of an antimicrobial agent will inhibit/kill the bacteria thereby facilitating resolution and clinical cure.
Antimicrobial therapy is most often prescribed empirically, meaning that the specific aetiology is unknown but the drug chosen is expected to have a spectrum of activity to cover the most probable pathogens and have a pharmacological profile to allow the drug to reach the site of infection and accumulate in concentrations sufficient to inhibit or kill the pathogen.
Over the past three decades, there has been an increasing realisation and escalation of antimicrobial resistance. Where do drug resistant organisms come from or how do they arise? Whilst unclear in some circumstances, new research has provided some clear insights into antimicrobial use and resistance selection. Clinicians now are faced with the reality that the drugs they are prescribing to effect a clinical cure may, in fact, be the same drugs that allow for the selection of antimicrobial resistance. In effect, treatment for clinical cure may select for drug resistance.
It has been argued that during infection, bacterial densities fluctuate and for some infections, the densities of bacteria present during acute infection may exceed the number of bacteria used for routine in vitro susceptibility testing. Such an observation identifies that the true “bug-drug” interactions that occur when high bacterial densities are present during infection may not be adequately determined by routine susceptibility testing using a relatively low bacterial density (Blondeau, 2009); this may have an impact on selection and amplification of drug-resistant bacteria.
The mutant prevention concentration (MPC) is a novel in vitro measurement that defines the antimicrobial drug
concentration blocking the growth of the least susceptible cells present in bacterial densities of >109 colony forming units (Blondeau, 2009; Blondeau et al., 2004; Dong et al., 1999). The MPC is the upper boundary of the Mutant Selection Window (MSW), with the MIC being the lower boundary. Therapeutic drug concentrations persisting between these two drug concentrations (i.e. in the MSW) are argued to selectively amplify (allow growth of) mutant bacterial cells with reduced susceptibility to the antimicrobial agent used for therapy. Mutant cells conferring drug resistance may arise spontaneously when bacterial cell densities exceed 107 bacterial cells and published reports suggest spontaneous mutants arise in bacterial densities between 107-109 bacterial cells (Blondeau et al., 2001); such densities have been reported to occur in human medicine, in acute respiratory and urinary tract infections and in meningitis. (Bingen et al., 1990; Fagon et al., 2000; Feldman, 1976; McVey and Kuszak, 2010).
Measuring the MPC provides a drug concentration which, if clinically achievable and sustainable, would block mutant growth and resistance selection. Resistance prevention, in addition to a successful clinical outcome, is a laudable goal and one commented on in therapeutic guidelines. (Mandell et al., 2007). Indeed, the World Health Organization (WHO) suggested the best strategy for antimicrobial resistance was to “defeat resistance before it starts”.(World Health Organisation, 2000). As such, dosing to prevent resistance without compromising clinical outcome should be the aim of therapy.
Drug pharmacology plays an important role in optimising therapy (Schentag et al., 2001). Concentration-dependent agents (i.e. fluoroquinolones, aminoglycosides) are characterised by two relationships:
- area under the drug concentration curve (AUC) to MIC ratio
- maximum serum or tissue concentration (Cmax) to MIC ratio
Past research suggests AUC/MIC ratios >100 (possibly less for Gram-
positive organisms) and Cmax/MIC ratios of 8-10 or higher correlated with clinical improvement and resistance prevention. Time-dependent agents (i.e. beta-lactams) are characterised by the time drug concentrations exceed the MIC over the dosage interval and literature suggests that if the levels of drug exceed the MIC for 40-60% of the dosage interval, this correlates with a satisfactory clinical outcome (Roberts and Lipman, 2009).
Limited data exists for antibiotics used in dermatology – particularly, achievable and sustainable skin drug concentrations. Tissue drug concentrations are often expressed in absolute values where available, or as a ratio or percentage of serum drug concentrations. For example, with beta-lactam agents, tissue drug concentrations may be less than serum drug concentrations (Honeybourne, 1994). One additional consideration is protein binding and conventional thinking suggests that only the free unbound fraction contributes to antimicrobial activity. Singhvi et al. (1978) showed that protein binding >60% decreased antimicrobial activity in vitro (MIC values were increased) as compared to drugs where the protein binding was <60%. Additionally, disease severity impacts tissue distribution as does the route and method of parenteral administration (i.e. higher concentrations with continuous versus bolus infusion) (Roberts and Lipman, 2009). For fluoroquinolones, tissue drug concentrations often exceed serum values (Blondeau et al., 2001).
Pradofloxacin is the newest of the veterinary fluoroquinolones to be approved for clinical use. It has activity against both Staphylococcus pseudintermedius and E. coli – important pathogens in companion animal medicine. Additionally, pradofloxacin is a dual targeting compound, meaning that it simultaneously targets the two intracellular fluoroquinolone targets – DNA gyrase (topoisomerase II) and topoisomerase IV – enzymes essential for DNA replication. This is a lethal bactericidal effect and dual targeting has a lower propensity for resistance selection
Focus On Pyoderma

Tools for Vets and Clients
Focus On Pyoderma
don’t forget to complete the fUll coUrse of treatment
treatment record
2 3 4 5 6 7 8
9 10 11 12 13 14 15
16 17 18 19 20 21 22
23 24 25 26 27 28 29
30 31 32 33 34 35
1 Treatment start date
Make a note of the date the first dose is given, and use the stickers
provided to mark one box each day until the course is finished.your pet has been
prescribed
Do I have to give Veraflox® at a specific time of day?
No, but you should choose a time of day most convenient to you and ensure it is administered at this time, each day, for the duration of treatment.
What happens if I miss a dose?
If you miss a dose, but remember soon afterwards, give the dose as normal, otherwise contact your veterinary practice for advice.
If my pet improves should I stop the treatment?
No – it is very important that you complete the course as directed by your veterinary surgeon, even if you think that your pet’s condition has improved.
if you have any queries relating to the use of this product, please speak to your prescribing veterinary surgeon.
Use medicines responsibly. www.noah.co.uk/responsible Veraflox® 15 mg tablets contain 15 mg Pradofloxacin. Veraflox® 60 mg tablets contain 60 mg Pradofloxacin. Veraflox® 120 mg tablets contain 120 mg Pradofloxacin. Veraflox® 25 mg/ml oral suspension for cats contains 25 mg/ml Pradofloxacin. Please refer to the appropriate datasheet, further information is available on request. Advice on the use of this or other medicines must be sought from the medicine provider. This information has been brought to you by Bayer, manufacturers of Veraflox®.
® Registered Trade Mark of Bayer AG. Bayer plc, Animal Health Division, Bayer House, Strawberry Hill, Newbury, Berkshire RG14 1JA. Tel: 01635 563000 POM-V Bayer Ltd, Animal Health Division, The Atrium, Blackthorn Road, Dublin 18, Ireland. Tel: 01 299 9313 POM VERA2/0711/ZONE/150000 EU/2/10/107/003 EU/2/10/107/007 EU/2/10/107/011 EU/2/10/107/013
Frequently askedquestions
2357_4 Veraflox Client Compliance Leaflet_OUTPUT.indd 1-2 30/08/2011 15:18
CLIENT POST PRESCRIPTION LEAFLET
CLIENT TREATMENT RECORD FRIDGE MAGNET – WITH STICKER PACK
For illustration purposes only.Design,sizesandspecificationsofallitemsmaychangeatproduction.
FREE WEBINARYOU ARE INVITED
TO ATTEND
Prepare your practice and order your materials today.
Call 0845 2574798ororderitemsfromtheBayerLeafletLinewebsite;www.bayer-leaflet-line.co.ukUsername:bayervetsPassword:bayervets1
Alternatively, please speak to your territory manager
✔✔✔✔✔✔✔✔✔
✔✔✔✔✔✔✔✔✔
✔✔✔✔✔✔✔✔✔
✔✔✔✔✔✔✔✔✔
✔✔✔✔✔✔✔✔✔
✔✔✔✔✔✔✔✔✔
✔✔✔✔✔✔✔✔✔
as compared to agents that preferentially target one intracellular target.
Ganiere et al (2005) reported an MIC90 value of 0.063 µg/ml for fifty S. intermedius strains collected from canine pyoderma cases; in addition, MIC90 values reported for E. coli strains ranged from 0.031 to 0.063 µg/ml. In the dog, pradofloxacin Cmax is 1.60 µg/ml; the AUC0-24 is 13 µg*h/ml and skin drug concentrations are 1.2-3.0 x (1.92-4.8 µg/ml) serum concentrations. MPC90 measurements for pradofloxacin tested against S. pseudintermedius and E. coli strains were reported to be 0.125 µg/ml for both pathogens (Blondeau, 2009). In considering tissue Cmax/MIC ratios for S. pseudintermedius, those values would range from 30.4-76.2 and the same or higher for E. coli, based on the above MIC values of 0.031 to 0.063 µg/ml.
The tissue Cmax/MPC ratios for S. pseudintermedius and E. coli would range from 15.36-38.4.
S. pseudintermedius is a much more common cause of pyoderma than is E. coli and both organisms are common companion animal pathogens. As MPC values determine drug concentrations necessary to block mutant cell growth and thereby reduce the likelihood for resistance selection, the low MIC and MPC values reported for pradofloxacin against these key pathogens show a narrow MSW and high tissue Cmax/MIC or Cmax/MPC ratios. Resistance prevention without compromising clinical efficacy seems attainable with pradofloxacin in the treatment of pyoderma.
your pet has been prescribed
Do I have to give Veraflox® at a specific time of day?No, but you should choose a time of day most convenient to you and ensure it is administered at this time, each day, for the duration of treatment.What happens if I miss a dose?If you miss a dose, but remember soon afterwards, give the dose as normal, otherwise contact your veterinary practice for advice.
If my pet improves should I stop the treatment?No – it is very important that you complete the course as directed by your veterinary surgeon, even if you think that your pet’s condition has improved.
if you have any queries relating to the use of this product, please speak to your prescribing veterinary surgeon.
Use medicines responsibly. www.noah.co.uk/responsible Veraflox® 15 mg tablets contain 15 mg Pradofloxacin. Veraflox® 60 mg tablets
contain 60 mg Pradofloxacin. Veraflox® 120 mg tablets contain 120 mg Pradofloxacin.
Veraflox® 25 mg/ml oral suspension for cats contains 25 mg/ml Pradofloxacin.
Please refer to the appropriate datasheet, further information is available on request.
Advice on the use of this or other medicines must be sought from the medicine provider.
This information has been brought to you by Bayer, manufacturers of Veraflox®. ® Registered Trade Mark of Bayer AG. Bayer plc, Animal Health Division, Bayer House, Strawberry Hill, Newbury, Berkshire RG14 1JA. Tel: 01635 563000 POM-V
Bayer Ltd, Animal Health Division, The Atrium, Blackthorn Road, Dublin 18, Ireland.
Tel: 01 299 9313 POM VERA2/0711/ZONE/150000 EU/2/10/107/003 EU/2/10/107/007 EU/2/10/107/011 EU/2/10/107/013
Frequently askedquestions
ReferencesBingen, E., Lambert-Zechovsky, N., Mariani-Kurkdjian, P., Doit, C., Aujard, Y., Fournerie, F., Mathieu, H., 1990. Bacterial counts in cerebrospinal fluid of children with meningitis. Eur. J. Clin. Microbiol. Infect. Dis. 9, 278-281.Blondeau, J.M., 2009. New concepts in antimicrobial susceptibility testing: the mutant prevention concentration and mutant selection window approach. Vet. Dermatol. 20, 383-396.Blondeau, J.M., Hansen, G., Metzler, K.L., Hedlin, P., 2004. The role of PK/PD parameters to avoid selection and increase of resistance: mutant prevention concentration. J. Chemother. 16, 1-19.Blondeau, J.M., Zhao, X., Hansen, G.T., Drlica, K., 2001. Mutant prevention concentrations (MPC) of fluoroquinolones for clinical isolates of Streptococcus pneumoniae. Antimicrob. Agents Chemother. 45, 433-438.Dong, Y., Zhao, X., Domagala, J., Drlica, K., 1999. Effect of fluoroquinolone concentration on selection of resistant mutants of Mycobacterium bovis BCG and Staphylococcus aureus. Antimicrob. Agents Chemother. 43, 1756-1758.Fagon, J., Patrick, H., Haas, D.W., Torres, A., Gilbert, C., Cheadle, W.G., Falcone, R.E., Paganin, F., Fabian, T.C., Lilienthal, F., 2000. Treatment of gram-positive nosocomial pneumonia: prospective random comparison of quinupristin/dalfopristin versus vancomycin. Am. J. Respir. Crit. Care Med. 161, 753-762.Feldman, W., 1976. Concentrations of bacteria in cerebrospinal fluid of patients with bacterial meningitis. J. Pediatr. 88, 549-552.Ganiere, J.P., Medaille, C., Mangion, C., 2005. Antimicrobial drug susceptibility of Staphylococcus intermedius clinical isolates from canine pyoderma. J Vet Med B Infect Dis Vet Public Health 52, 25-31.Honeybourne, D., 1994. Antibiotic penetration into lung tissues. Thorax 49, 104-106.Mandell, L.A., Wunderink, R.G., Anzueto, A., Bartlett, J.G., Campbell, G.D., Dean, N.C., Dowell, S.F., File Jr., T.M., Musher, D.M., Niederman, M.S., Torres, A., Whitney, C.G., 2007. Infectious Disease Society of America/American Thoracic Society Consensus Guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 44, S27-S72.McVey, D.S., Kuszak, J., 2010. Bacterial isolates from the lungs of beef calves with bronchopneumonia associated with acute bovine respiratory disease. In: Conference on Research Workers in Animal Diseases (CRWAD), Chicago, IL, December 4-5.Roberts, J.A., Lipman, J., 2009. Tissue distribution of beta-lactam antibiotics: continuous versus bolus dosing. J. Pharm. Pract. Res. 39, 219-222.Schentag, J.J., Gilliland, K.K., Paladino, J.A., 2001. What have we learned from pharmacokinetic and pharmacodynamic theories? Clin. Infect. Dis. 32, S39-46.Singhvi, S.M., Heald, A.F., Schreiber, E.C., 1978. Pharmacokinetics of cephalosporin antibiotics: protein-binding considerations. Chemotherapy 24, 121-133.World Health Organization. World Health Organization Report on Infectious Diseases (2000). http://www.who.int/infectiousdisease-report/2000 (April 9, 2013, date last accessed).
To view Dr. Joe Blondeau discussing the Mutant Prevention Concentration and any up coming webinars, or for further information, please visit www.animalhealthwebinars.bayer.co.uk to register.

VERAFLOX® 25 MG/ML ORAL SUSPENSION FOR CATSPresentation: Veraflox® 25 mg/ml oral suspension for cats is a yellowish to beige suspension containing 25 mg/ml Pradofloxacin with 2 mg/ml Sorbic acid (E200) as a preservative. Uses: Indicated for the use in cats for the treatment of: acute infections of the upper respiratory tract caused by susceptible strains of Pasteurella multocida, Escherichia coli and the Staphylococcus intermedius group (including S. pseudintermedius), wound infections and abscesses caused by susceptible strains of Pasteurella multocida and the Staphylococcus intermedius group (including S. pseudintermedius). Dosage and administration: Administration is by the oral route. Dosages The recommended dose is 5.0 mg/kg bodyweight of pradofloxacin once daily. Due to the graduation of the syringe the resulting dose range is 5.0 to 7.5 mg/kg bodyweight according to the following table:
Bodyweight of Cat (kg)
Dose of oral suspension to be given (ml)
Pradofloxacin dose (mg/kg bw)
> 0.67 – 1 0.2 5 – 7.5
1 – 1.5 0.3 5 – 7.5
1.5 – 2 0.4 5 – 6.7
2 – 2.5 0.5 5 – 6.3
2.5 – 3 0.6 5 – 6
3 – 3.5 0.7 5 – 5.8
3.5 – 4 0.8 5 – 5.7
4 – 5 1.0 5 – 6.3
5 – 6 1.2 5 – 6
6 – 7 1.4 5 – 5.8
7 – 8 1.6 5 – 5.7
8 – 9 1.8 5 – 5.6
9 – 10 2.0 5 – 5.6
To ensure a correct dosage, bodyweight should be determined as accurately as possible to avoid underdosing. To facilitate accurate dosing, the 15 ml bottle of Veraflox® oral suspension is supplied together with a 3 ml oral dosing syringe (graduation: 0.1 to 2 ml). The duration of the treatment depends on the nature and severity of the infection and on the response to treatment. For most infections the following treatment courses will be sufficient:
The treatment should be reconsidered if no improvement of the clinical condition is observed within 3 days after starting the treatment. Method of Administration:
Shake well before use. Draw out the equivalent dosage into the syringe.
Administer directly into the mouth.
In order to avoid cross-contamination, the same syringe should not be used for different animals. Thus, one syringe should only be used for one animal. After administration, the syringe should be cleaned with tap water and stored in the carton box together with the veterinary medicinal product. Use during pregnancy and lactation: The safety of this veterinary medicinal product has not been established in queens during pregnancy and lactation. Pregnancy: Do not use during pregnancy. Pradofloxacin induced eye malformations at foetal and maternal toxic dosages in rats. Lactation: Do not use during lactation since there are no data on pradofloxacin in kittens aged less than 6 weeks. Fluoroquinolones are known to cross the placenta and to be distributed into milk. Fertility: Pradofloxacin has been shown to have no effects on fertility in breeding animals. Contra-indications, warnings, etc: Do not use in cats with known hypersensitivity to fluoroquinolones. Due to the lack of data, pradofloxacin should not be used in kittens aged less than 6 weeks. Pradofloxacin has no effects on the developing cartilage of kittens of 6 weeks of age and older. However the product should not be used in cats with persisting articular cartilage lesions, as these lesions may worsen during treatment with fluoroquinolones. Do not use in cats with central nervous system (CNS) disorders, such as epilepsy, as fluoroquinolones could potentially cause seizures in predisposed animals. Do not use in cats during pregnancy and lactation. Whenever possible, the veterinary medicinal product should only be used based on susceptibility testing. Official and local antimicrobial policies should be taken into account when the veterinary medicinal product is used. Fluoroquinolones should be reserved for the treatment of clinical conditions which have responded poorly, or are expected to respond poorly, to other classes of antimicrobials. Use of the veterinary medicinal product deviating from instructions given in the SPC may increase the prevalence of bacteria resistant to the fluoroquinolones and may decrease the effectiveness of treatment with other fluoroquinolones due to the potential for cross-resistance. Pradofloxacin may increase sensitivity of the skin to sunlight. During treatment, animals should therefore not be exposed to excessive sunlight. Mild transient gastrointestinal disturbances including vomiting have been observed in rare cases. Concurrent administration with metal cations such as those contained in antacids or sucralfate made with magnesium hydroxide or aluminium hydroxide, or multivitamins containing iron or zinc, and dairy products containing calcium, has been reported to decrease the bioavailability of fluoroquinolones. Therefore, Veraflox® should not be administered concurrently with antacids, sucralfate, multivitamins or dairy products, as absorption of Veraflox® may be decreased. Further, fluoroquinolones should not be used in combination with nonsteroidal antiinflammatory drugs (NSAIDs) in animals with a history of seizures because of potential pharmacodynamic interactions in the CNS. The combination of fluoroquinolones with theophylline could increase the plasma levels of theophylline by altering its metabolism and thus should be avoided. The combined use of fluoroquinolones with digoxin should also be avoided because of potentially increased oral bioavailability of digoxin. No specific antidotes for pradofloxacin (or other fluoroquinolones) are known, therefore, in case of overdose, symptomatic treatment should be given. Intermittent vomiting was observed after repeated oral administration of 1.6 times the maximum recommended dose. User Safety: Due to potential harmful effects, the bottles and the filled syringes must be kept out of the reach and sight of children. People with known hypersensitivity to quinolones should avoid any contact with the veterinary medicinal product. Avoid skin and eye contact with the veterinary medicinal product. Wash hands after use. In case of accidental contact with the eyes, wash immediately with water. In case of contact with the skin, rinse off with water. Environmental Safety: Any unused veterinary medicinal product or waste materials derived from such veterinary medicinal products should be disposed of in accordance with local requirements. Pharmaceutical precautions: In the absence of compatibility studies, this veterinary medicinal product must not be mixed with other veterinary medicinal products. Store in the original container. Keep the bottle tightly closed. Shelf life of the veterinary medicinal product as packaged for sale: 3 years Shelf life after first opening the bottle: 3 months Legal category: POM-V
VERAFLOX® TABLETSPresentation: Veraflox® 15 mg tablets are brownish single scored tablets for oral administration to cats and dogs, they contain 15 mg Pradofloxacin and have been marked with “P15” on one side. Veraflox® 60 mg tablets are brownish single scored tablets for oral administration to dogs, they contain 60 mg Pradofloxacin and have been marked with “P60” on one side. Veraflox® 120 mg tablets are brownish single scored tablets for oral ad-ministration to dogs, they contain 120 mg Pradofloxacin and have been marked with “P120” on one side. Uses: Cats: Treatment of acute infections of the upper respiratory tract caused by susceptible strains of Pasteurella multocida, Escherichia coli and the Staphylococcus intermedius group (including S. pseudintermedius). Dogs: Treatment of: wound infections caused by susceptible strains of the Staphylococcus intermedius group (includ-ing S. pseudintermedius), superficial and deep pyoderma caused by susceptible strains of the Staphylococcus intermedius group (including S. pseudintermedius), acute urinary tract infections caused by susceptible strains of Escherichia coli and the Staphylococcus intermedius group (including S. pseudintermedius) and as adjunctive treatment to mechanical or surgical periodontal therapy in the treatment of severe infections of the gingiva and
periodontal tissues caused by susceptible strains of anaerobic organisms, for example Porphyromonas spp. and Prevotella spp. Dosage and administration: Administration is via the oral route. The recommended dose is 3.0 mg/kg bodyweight of pradofloxacin once daily. Due to the available tablet sizes the resulting dose range is 3.0 to 4.5 mg/kg bodyweight according to the following tables. To ensure a correct dosage, bodyweight should be determined as accurately as possible to avoid underdosing.
Cats:
Bodyweight of Cat (kg)
Number of Tablets Pradofloxacin dose (mg/kg bw)15 mg
> 3.4 – 5 1 3.0 – 4.4
5 – 7.5 1.5 3.0 – 4.5
7.5 – 10 2 3.0 – 4.0
Dogs:
Bodyweight of Dog (kg)
Number of Tablets Pradofloxacin dose (mg/kg bw)15 mg 60 mg 120 mg
> 3.4 – 5 1 3.0 – 4.4
5 – 7.5 1.5 3.0 – 4.5
7.5 – 10 2 3.0 – 4.0
10 – 15 3 3.0 – 4.5
15 – 20 1 3.0 – 4.0
20 – 30 1.5 3.0 – 4.5
30 – 40 1 3.0 – 4.0
40 – 60 1.5 3.0 – 4.5
60 – 80 2 3.0 – 4.0
Duration of treatment The duration of the treatment depends on the nature and severity of the infection and on the response to treatment. For most infections the following treatment courses will be sufficient:
Cats:
Indication Duration of treatment (days)
Acute infections of the upper respiratory tract 5
The treatment should be reconsidered if no improvement of the clinical condition is observed within 3 days after starting the treatment.
Dogs:
Indication Duration of treatment (days)
Infections of the skin:
Superficial pyoderma 14 – 21
Deep pyoderma 14 – 35
Wound infections 7
Acute infections of the urinary tract 7 – 21
Severe infections of the gingiva and periodontal tissues 7
The treatment should be reconsidered if no improvement of the clinical conditions is observed within 3 days, or in cases of superficial pyoderma 7 days, and in cases of deep pyoderma 14 days, after starting the treatment. Use during pregnancy and lactation: The safety of this veterinary medicinal product has not been established during pregnancy and lactation in cats and dogs. Pregnancy: Do not use during pregnancy. Pradofloxacin induced eye malformations at foetal and maternal toxic dosages in rats. Lactation: Do not use during lactation. Labora-tory studies in puppies have shown evidence of arthropathy after systemic administration of fluoroquinolones. Fluoroquinolones are known to cross the placenta and to be distributed into milk. Fertility: Pradofloxacin has been shown to have no effects on fertility in breeding animals. Contra-indications, warnings, etc: Do not use in animals with known hypersensitivity to fluoroquinolones. Cats: Due to the lack of data, pradofloxacin should not be used in kittens aged less than 6 weeks. Pradofloxacin has no effects on the developing cartilage of kittens of 6 weeks of age and older. However, the product should not be used in cats with persisting articular cartilage lesions, as these lesions may worsen during treatment with fluoroquinolones. Do not use in cats with central nervous system (CNS) disorders, such as epilepsy, as fluoroquinolones could potentially cause seizures in predisposed animals. Do not use in cats during pregnancy and lactation. Dogs: Do not use in dogs during the period of growth as developing articular cartilage may be affected. The period of growth depends on the breed. For the majority of breeds, pradofloxacin containing veterinary medicinal products must not be used in dogs of less than 12 months of age and in giant breeds less than 18 months. Do not use in dogs with persist-ing articular cartilage lesions, since lesions may worsen during treatment with fluoroquinolones. Do not use in dogs with central nervous system (CNS) disorders, such as epilepsy, as fluoroquinolones could possibly cause seizures in predisposed animals. Do not use in dogs during pregnancy and lactation. Whenever possible, the veterinary medicinal product should only be used based on susceptibility testing. Official and local antimicrobial policies should be taken into account when the veterinary medicinal product is used. Fluoroquinolones should be reserved for the treatment of clinical conditions which have responded poorly, or are expected to respond poorly, to other classes of antimicrobials. Use of the veterinary medicinal product deviating from instructions given in the SPC may increase the prevalence of bacteria resistant to the fluoroquinolones and may decrease the effectiveness of treatment with other fluoroquinolones due to the potential for cross-resistance. Pyoderma occurs mostly secondary to an underlying disease, thus, it is advisable to determine the underlying cause and to treat the animal accordingly. This veterinary medicinal product should only be used in severe cases of periodontal disease. Mechanical cleaning of teeth and removal of plaque and calculus or extraction of teeth are prerequisites for a persistent therapeutic effect. In case of gingivitis and periodontitis, the veterinary medicinal product should only be used as an adjunct to mechanical or surgical periodontal therapy. Only those dogs for which periodontal treatment goals cannot be achieved by mechanical treatment alone should be treated with this veterinary medicinal product. Pradofloxacin may increase sensitivity of the skin to sunlight. During treatment, animals should therefore not be exposed to excessive sunlight. Excretion via kidneys is an important elimination route for pradofloxacin in dogs. As for other fluoroquinolones, the renal excretion rate of pradofloxacin may be decreased in dogs with impaired kidney function and, therefore, pradofloxacin should be used with caution in such animals. Mild transient gastrointestinal disturbances including vomiting have been observed in rare cases in dogs and cats. Concurrent administration with metal cations such as those contained in antacids or sucralfate made with magnesium hydroxide or aluminium hydroxide, or multivitamins containing iron or zinc, and dairy products containing calcium, has been reported to decrease the bioavailability of fluoroquinolones. Therefore, Veraflox® should not be administered concurrently with antacids, sucralfate, multivitamins or dairy products, as absorption of Veraflox® may be decreased. Further, fluoroquinolones should not be used in combination with nonsteroidal antiinflammatory drugs (NSAIDs) in animals with a history of seizures because of potential pharmacodynamic interactions in the CNS. The combination of fluoroquinolones with theophylline could increase the plasma levels of theophylline by altering its metabolism and thus should be avoided. The combined use of fluoroquinolones with digoxin should also be avoided because of potentially increased oral bioavailability of digoxin. No specific antidotes for pradofloxacin (or other fluoroquinolones) are known, therefore, in case of overdose, symptomatic treatment should be given. Intermittent vomiting and soft faeces were observed in dogs after repeated oral administration of 2.7 times the maximum recommended dose. Infrequent vomiting was observed in cats after repeated oral administration of 2.7 times the maximum recommended dose. User Safety: Due to potential harmful effects, the tablets must be kept out of the reach and sight of children. People with known hypersensitivity to quinolones should avoid any contact with the veterinary medicinal product. Avoid skin and eye contact with the veterinary medicinal product. Wash hands after use. Do not eat, drink or smoke while handling the veterinary medicinal product. In case of accidental ingestion, seek medical advice and show the package leaflet or the label to the physician. Environmental Safety: Any unused veterinary medicinal product or waste materials derived from such veterinary medicinal products should be disposed of in accordance with local requirements. Pharmaceutical precautions: This veterinary medicinal product does not require any special storage conditions. Shelf life of the veterinary medicinal product as packaged for sale: 3 years. Legal category: POM-V
Indication Duration of treatment (days)
Wound infections and abscesses 7
Acute infections of the upper respiratory tract 5
Pleaserefertoappropriatedatasheet,furtherinformationisavailableonrequest.®RegisteredTradeMarkofBayerAG.Bayerplc,AnimalHealthDivision,BayerHouse,StrawberryHill,NewburyRG141JA.Tel:01635563000.BayerLtd.,AnimalHealthDivision,TheAtrium,BlackthornRoad,Dublin18.Tel:(01)2999313.EU/2/10/107/003 EU/2/10/107/007 EU/2/10/107/011 EU/2/10/107/013 VERA.0413.DE.ZO.2.References:1.Koerber,B.,et al.,Bactericidalmechanismsofpradofloxacin,anovel8-cyanofluoroquinolone.In:42ndInterscienceConferenceonAntimicrobialAgentsandChemotherapy.SanDiego,CA:2002.AbstractF-567:188.2.Himmler,T.,et al.,Synthesisandinvitroactivityofpradofloxacin,anovel8-cyanofluoroquinolone.In:42ndInterscienceConferenceonAntimicrobialAgentsandChemotherapy.SanDiego,CA:2002.AbstractF-566:42.3.EuropeanMedicinesAgencywebsite.4.Silley,P.,et al.,Comparativeactivityofpradofloxacinagainstanaerobicbacteriaisolatedfromdogsandcats.JAntimicrob.Chemother.2007;60(5):999-1003.5.Wetzstein,H.G.,Comparativemutantpreventionconcentrationsofpradofloxacinandotherveterinaryfluoroquinolonesindicatedifferingpotentialsinpreventingselectionofresistance.Antimicrob.AgentsChemother.2005;49(10):4166-4173.6.BayerStudyNumber147.348.7.Mueller,R.S.,Stephan,B.,Pradofloxacininthetreatmentofcaninedeeppyoderma:amulticentered,blinded,randomisedparalleltrial.VetDermatol.2007;18(3):144-151.
UseMedicinesResponsibly(www.noah.co.uk/responsible)