Focus on Intracranial Pressure (Relates to Chapter 57, “Nursing Management: Acute Intracranial...
61
Focus on Intracranial Pressure (Relates to Chapter 57, “Nursing Management: Acute Intracranial Problems,” in the textbook) Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
-
Upload
dana-felicia-gaines -
Category
Documents
-
view
222 -
download
1
Transcript of Focus on Intracranial Pressure (Relates to Chapter 57, “Nursing Management: Acute Intracranial...
Focus on Intracranial Pressure
(Relates to Chapter 57, “Nursing Management: Acute Intracranial Problems,” in the textbook)
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
Intracranial Pressure
Skull has three essential components: Brain tissue Blood Cerebrospinal fluid (CSF)
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 2

Components of the Brain
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 3
Fig. 57-1. Components of the brain.

Intracranial Pressure
Intracellular and extracellular fluids of brain tissues make up 78% of the volume. Blood makes up 12%. Remaining 10% is CSF.
Balance of these components maintains the ICP under normal conditions.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 4

Intracranial Pressure
Factors that influence ICP Arterial pressure Venous pressure Intraabdominal and intrathoracic pressure
Posture Temperature Blood gases (particularly CO2 levels)
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 5

Regulation and Maintenance
Normal intracranial pressure Modified Monro-Kellie doctrine: describes relatively constant volume within skull structure If volume in any one of the components
increases within the cranial vault, and volume from another component is displaced, the total intracranial volume will not change.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 6
Regulation and Maintenance
Normal compensatory adaptations Alteration of CSF absorption or production
Displacement of CSF into spinal subarachnoid space
Ability to compensate is limited. If volume increase continues, ICP rises.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 7

Regulation and Maintenance
Measuring ICP Can be measured in
Ventricles Subarachnoid space Epidural space Brain tissue
Measured with a pressure transducer
Normal ICP: 5 to 15 mm Hg
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 8
Cerebral Blood Flow
Definition The amount of blood in milliliters passing through 100 g of brain tissue in 1 minute
About 50 mL/min per 100 g of brain tissue
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 9
Cerebral Blood Flow
Autoregulation of cerebral blood flow Automatic alteration in diameter of cerebral blood vessels to maintain constant blood flow to brain
Ensures a consistent CBF to provide the metabolic needs of brain tissue and maintain cerebral perfusion pressure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 10
Cerebral Blood Flow
Cerebral perfusion pressure (CPP) Pressure needed to ensure blood flow to the brain
CPP = MAP – ICP Normal is 60 to 100 mm Hg. <50 mm Hg is associated with ischemia and neuronal death.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 11

Cerebral Blood Flow
Pressure changes Compliance is the expandability of the brain.
Compliance = Volume/Pressure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 12

Intracranial Volume Pressure Curve
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 13
Fig. 57-2. Intracranial pressure-volume curve. (See text for descriptions of 1, 2, 3, and 4.)
Cerebral Blood Flow
Pressure-volume curve represented by stages Stage 1: high compliance Stage 2: compliance ↓, risk for ↑ ICP
Stage 3: any small addition in volume causes a great ↑ in ICP, loss of autoregulation
Stage 4: ICP rises to lethal levels
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 14

Cerebral Blood Flow
Factors affecting cerebral blood vessel tone CO2
O2
Hydrogen ion concentration
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 15
Mechanisms of Increased ICP
Causes Mass lesion Cerebral edema Head injury Brain inflammation Metabolic insult
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 16

Increased Intracranial Pressure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 17
Fig. 57-3. Progression of increased intracranial pressure (ICP).
Mechanisms of Increased ICP
Sustained increase in ICP results in brainstem compression and herniation of brain from one compartment to another.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 18
Herniation
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 19
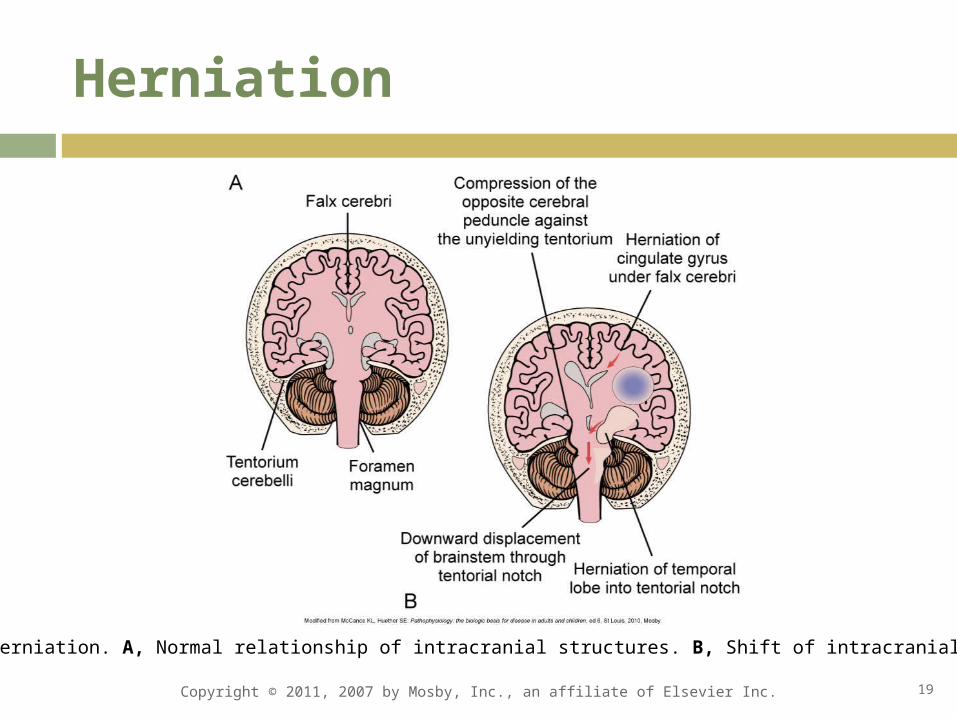
Fig. 57-4. Herniation. A, Normal relationship of intracranial structures. B, Shift of intracranial structures.
Cerebral Edema
Increased accumulation of fluid in the extravascular spaces of brain tissue
Three types of cerebral edema: Vasogenic Cytotoxic Interstitial
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 20
Cerebral Edema
Vasogenic cerebral edema Most common type Occurs mainly in white matter Associated with changes in the endothelial lining of cerebral capillaries
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 21

Cerebral Edema
Cytotoxic cerebral edema Results from local disruption of functional integrity of cell membranes
Occurs mainly in gray matter
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 22

Cerebral Edema
Interstitial cerebral edema Result of rupture of CSF brain barrier
Usually a result of obstructive or uncontrolled hydrocephalus
Can also be caused by enlargement of the extracellular space as a result of systemic water excess
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 23
Clinical Manifestations
Change in level of consciousness
Change in vital signs Cushing’s triad
Ocular signs
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 24

Clinical Manifestations
↓ In motor function Decerebrate posturing (extensor) Indicates more serious damage
Decorticate posturing (flexor)
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 25
Decorticate and Decerebrate Posturing
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 26
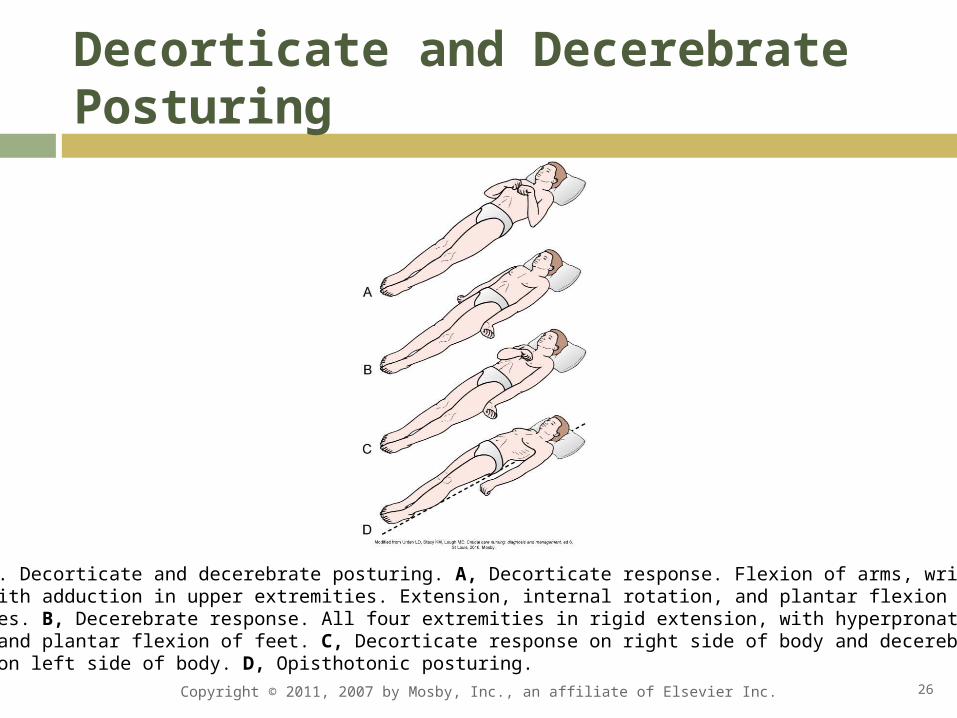
Fig. 57-5. Decorticate and decerebrate posturing. A, Decorticate response. Flexion of arms, wrists, andfingers with adduction in upper extremities. Extension, internal rotation, and plantar flexion in lower extremities. B, Decerebrate response. All four extremities in rigid extension, with hyperpronation of forearms and plantar flexion of feet. C, Decorticate response on right side of body and decerebrate response on left side of body. D, Opisthotonic posturing.
Clinical Manifestations
Headache Often continuous and worse in the morning
Vomiting Not preceded by nausea Projectile
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 27
Complications
Two major complications of uncontrolled increased ICP Inadequate cerebral perfusion Cerebral herniation
Tentorial herniation Uncal herniation Cingulate herniation
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 28
Diagnostic Studies
Aimed at identifying underlying cause MRI CT Cerebral angiography EEG Brain tissue oxygenation measurement
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 29
Diagnostic Studies
Aimed at identifying underlying cause (cont’d) ICP measurement Measurement via the LICOX catheter
Transcranial Doppler studies Evoked potential studies PET
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 30
Measurement of ICP
ICP monitoring used to guide clinical care when at risk for increased ICP Those admitted with a Glasgow Coma Scale of 8 or less
Those with abnormal CT scans or MRI
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 31

Measurement of ICP
The gold standard for ICP monitoring is the ventriculostomy. Catheter inserted into lateral ventricle
Coupled with an external transducer
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 32
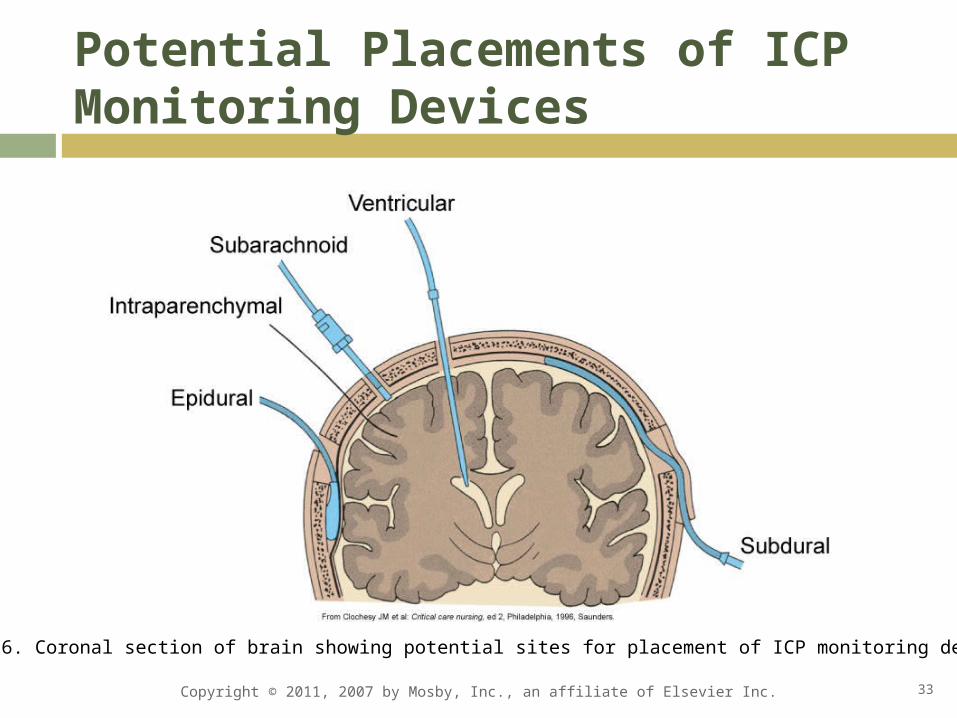
Potential Placements of ICP Monitoring Devices
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 33
Fig. 57-6. Coronal section of brain showing potential sites for placement of ICP monitoring devices.
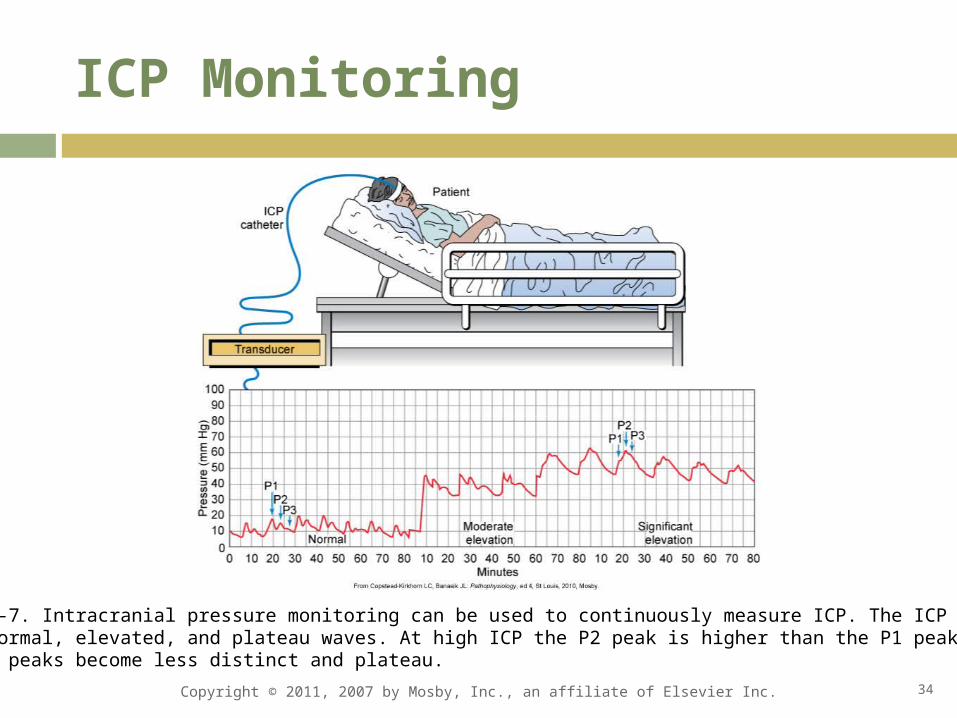
ICP Monitoring
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 34
Fig. 57-7. Intracranial pressure monitoring can be used to continuously measure ICP. The ICP tracingshows normal, elevated, and plateau waves. At high ICP the P2 peak is higher than the P1 peak, and the peaks become less distinct and plateau.
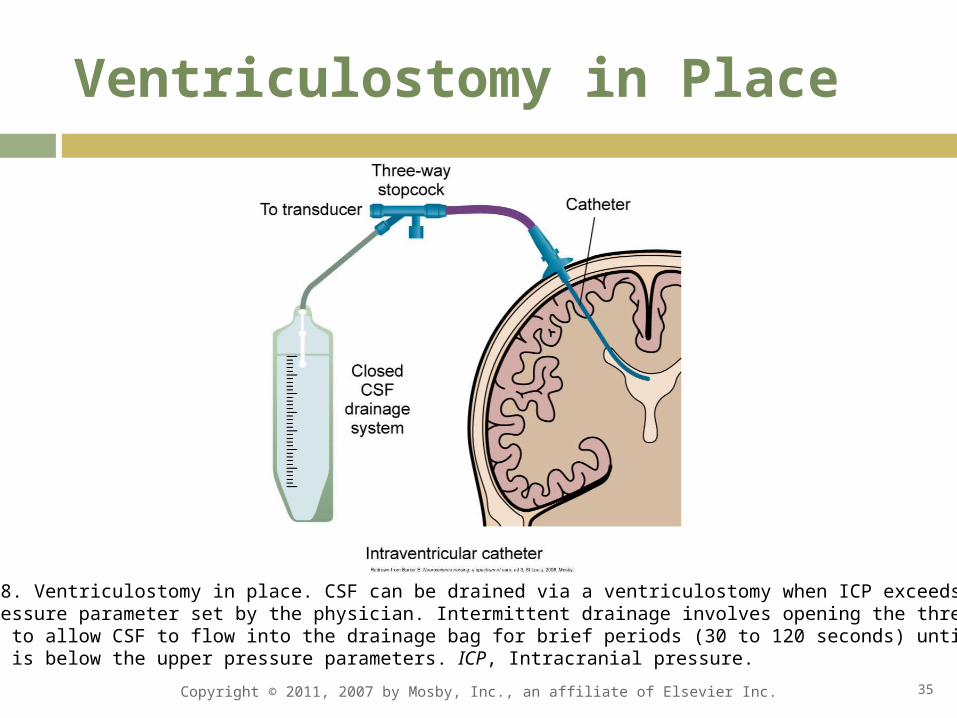
Ventriculostomy in Place
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 35
Fig. 57-8. Ventriculostomy in place. CSF can be drained via a ventriculostomy when ICP exceeds the upper pressure parameter set by the physician. Intermittent drainage involves opening the three-way stopcock to allow CSF to flow into the drainage bag for brief periods (30 to 120 seconds) until the pressure is below the upper pressure parameters. ICP, Intracranial pressure.
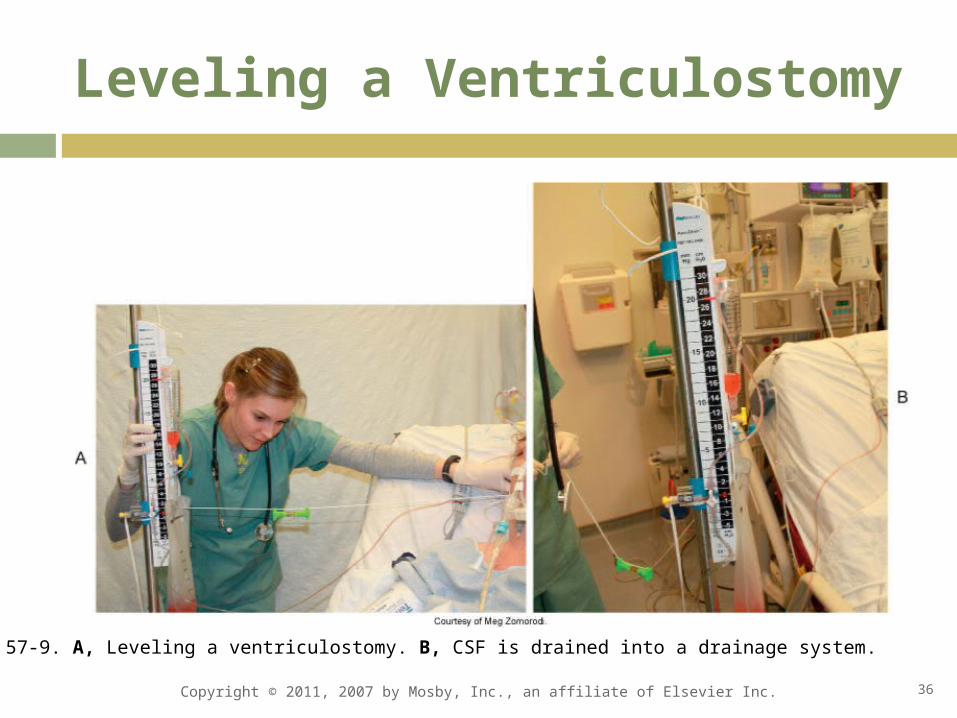
Leveling a Ventriculostomy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 36
Fig. 57-9. A, Leveling a ventriculostomy. B, CSF is drained into a drainage system.

Measurement of ICP
Fiberoptic catheter Sensor transducer located within the catheter tip
Subarachnoid bolt or screw Allows for CSF drainage Ideal for patients with mild or moderate head injury
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 37
Measurement of ICP
Infection is always a serious consideration with ICP monitoring.
ICP should be measured as mean pressure at the end of expiration.
Waveform should be recorded. Shaped similar to arterial pressure trace
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 38
Measurement of ICP
Inaccurate readings can be caused by CSF leaks Obstruction in catheter Differences in height of bolt/transducer
Kinks in tubing Incorrect height of drainage system relative to patient’s reference point
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 39
Measurement of ICP
With catheter, it is possible to control ICP by removing CSF.
Careful monitoring of the volume of CSF drained is essential.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 40

Measurement of ICP
LICOX brain tissue oxygenation catheter Provides continuous monitoring of pressure of oxygen in brain tissue
Jugular venous bulb catheter
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 41
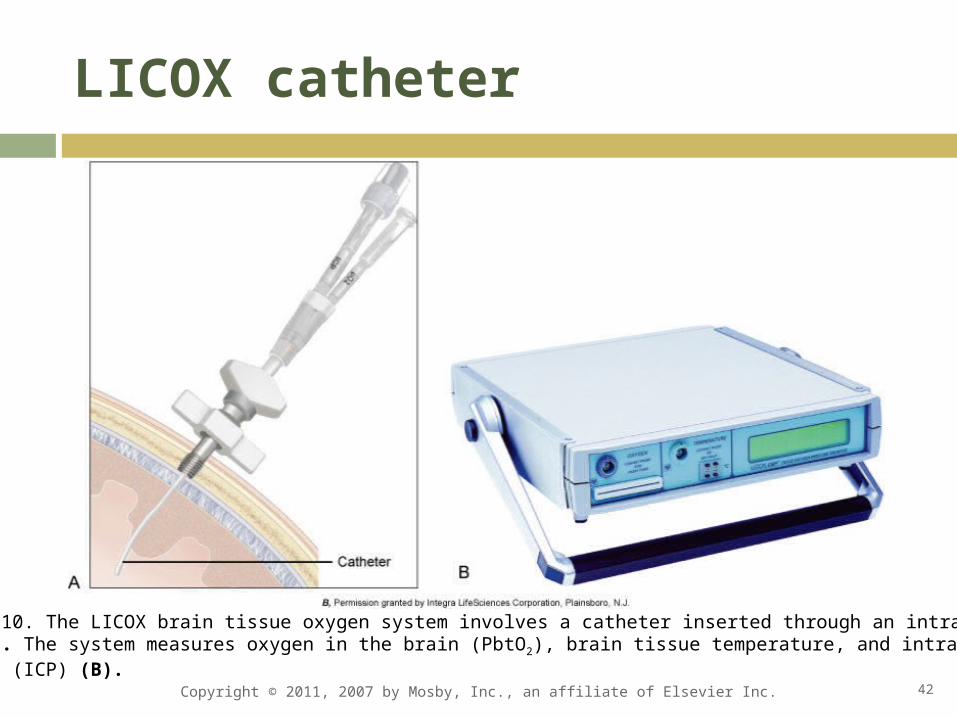
LICOX catheter
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 42
Fig. 57-10. The LICOX brain tissue oxygen system involves a catheter inserted through an intracranial bolt (A). The system measures oxygen in the brain (PbtO2), brain tissue temperature, and intracranial pressure (ICP) (B).
Collaborative Care
Adequate oxygenation PaO2 maintenance at 100 mm Hg or greater
ABG analysis guides the oxygen therapy.
May require mechanical ventilator
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 43
Collaborative Care
Drug therapy Mannitol (Osmitrol) Hypertonic saline Corticosteroids Barbiturates
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 44
Collaborative Care
Nutritional therapy Patient is in hypermetabolic and hypercatabolic state.
↑ Need for glucose Keep patient normovolemic.
IV 0.9% NaCl
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 45

Nursing Management
Nursing assessment Subjective data from patient or family members
Glasgow Coma Scale Neurologic assessment
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 46

Pupillary Check for Size and Response
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 47
Fig. 57-11. Pupillary check for size and response.

Nursing Management
Motor strength and response Vital signs
BP Pulse Respiratory rate Temperature
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 48
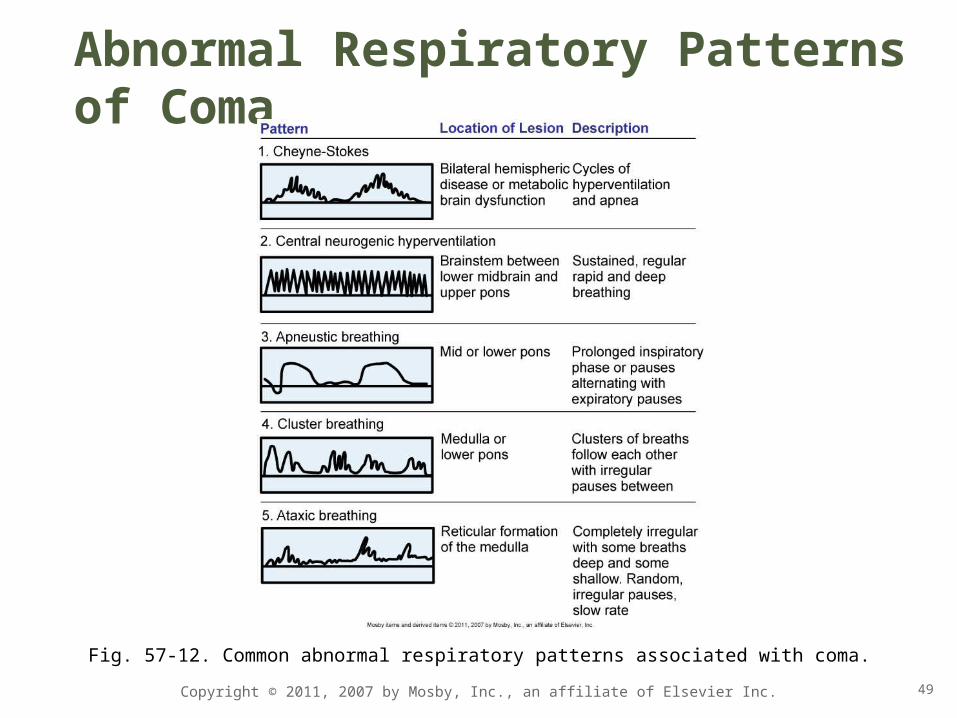
Abnormal Respiratory Patterns of Coma
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 49
Fig. 57-12. Common abnormal respiratory patterns associated with coma.

Nursing Management
Nursing diagnoses Risk for ineffective cerebral tissue perfusion
Decreased intracranial adaptive capacity
Risk for disuse syndrome Altered family process
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 50
Nursing Management
Planning Overall goals
Maintain a patent airway ICP within normal limits Normal fluid and electrolyte balance
No complications secondary to immobility and decreased LOC
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 51

Nursing Management
Nursing implementation Respiratory function Fluid and electrolyte balance Monitoring of intracranial pressure
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 52
Nursing Management
Nursing implementation Body position maintained in head-up position
Protection from injury Psychologic considerations
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 53
Intracranial pressure monitoring is instituted for a patient with a head injury. The patient’s arterial blood pressure is 92/50 mm Hg, and intracranial pressure is 18 mm Hg. Using these values to calculate the patient’s cerebral perfusion pressure (CPP), the nurse determines that:
1. The CPP is adequate for normal cerebral blood flow.2. To prevent cerebral hypoxemia, the patient’s blood pressure should be increased.3. The CPP is so low that ischemia and neuronal death are imminent.4. Lowering the patient’s blood pressure will reduce the intracranial pressure, increasing cerebral blood flow.
Audience Response Question
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 54

A patient with increased intracranial pressure is placed in a lateral position with the head of the bed elevated 30 degrees. The nurse evaluates the need for lowering the head of the bed when the patient experiences:
1. Ptosis of the eyelid.2. Unexpected vomiting.3. A decrease in motor functions.4. Decreasing level of consciousness.
Audience Response Question
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 55
Case Study
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.
56
Case Study
A son brings his 68-year-old father to ED with confusion, lethargy, and headache.
The son is concerned that the father may be developing dementia.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 57

Case Study
He was in a car accident 2 days ago where he hit his head on the windshield. He refused care. He says he “felt just fine.”
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 58

Case Study
His vital signs are BP 144/54 Heart rate 76 Respiratory rate 12 Temperature 98.9
CT indicates a subacute subdural hematoma.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 59

Discussion Questions
1.What can you tell the son about the difference between his father’s current condition and dementia?
2.What information can you give the son about the treatment his father will undergo?
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 60
Discussion Questions
3. What is the primary nursing management for the father?
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 61