Pediatric Type 1 Diabetes Mellitus Chelsea Stegman and Kelly Davis.

DOI: 10.1542/pir.31-12-5062010;31;506Pediatrics in Review
Kelly M. ClaytonFocus on Diagnosis : Pediatric Abdominal Imaging
http://pedsinreview.aappublications.org/content/31/12/506located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Pediatrics. All rights reserved. Print ISSN: 0191-9601. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2010 by the American Academy of published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1979. Pediatrics in Review is owned, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from

Author Disclosure
Dr Clayton has disclosed no financial
relationships relevant to this article.
This commentary does not contain a
discussion of an unapproved/
investigative use of a commercial
product/device.
Pediatric Abdominal ImagingKelly M. Clayton, MD*
IntroductionWhen evaluating acute abdominalpain in children, the most importantinitial step is to perform a thoroughhistory and physical examination.Only after, if necessary for diagnosticpurposes, should specific laboratoryand radiographic studies be obtained.Imaging can provide additional evi-dence to support a questionable di-agnosis. A wide variety of abdominalimaging modalities is available to prac-titioners, although availability is highlydependent on the institution and localresources. We discuss the classic find-ings indicative of abdominal disordersfound on plain radiography, ultra-sonography (US), computed tomog-raphy (CT) scan, magnetic resonanceimaging (MRI), and nuclear medicinestudies.
RadiographyAbdominal radiography often is anecessary preliminary study and isthe most commonly requested studyfor a child complaining of abdominalpain. Its availability, lesser cost, andlower radiation exposure comparedwith other imaging modalities makeit attractive. Abdominal radiographyis highly sensitive (almost 100%) fordiagnosing free intraperitoneal airand bowel obstruction. (1) It maydetect abdominal calcifications andforeign body ingestions. Plain radi-ography for diagnosing intussuscep-tion is controversial due to a less than50% accuracy rate. However, a rightupper quadrant soft-tissue mass with-out right colonic gas is almost patho-gnomonic for intussusception. (2)Abdominal radiography should notbe used to quantify the amount of
stool, measure the liver size, or eval-uate a child who has chronic vagueabdominal pain. (3) It is importantto remember that negative findingson abdominal radiography shouldprompt the physician to order addi-tional, more specific studies whenclinical suspicion is high.
Fluoroscopy is used with plain ra-diography to evaluate the pediatricabdomen. For example, upper gastro-intestinal radiographic studies dem-onstrate both the anatomy and func-tion of the esophagus, stomach, andduodenum. This technique is helpfulin diagnosing malrotation, duodenalweb, achalasia, and hypertrophic py-loric stenosis. Furthermore, an aircontrast enema is not only diagnosticbut also the treatment for intussus-ception.
UltrasonographyUS is a more specific study thatshould be one of the initial choiceswhen evaluating a child for abdomi-nal pain. It is noninvasive, does notuse ionizing radiation, and is rela-tively inexpensive. US employs high-frequency sound waves to producereal-time images. Its use is easier andmore reliable in children than adultsbecause of their small size and dimin-ished fat planes. (4) Higher-frequencytransducers also can be used in smallchildren compared with adults, im-proving the image resolution. (3)
In neonates and younger infants,US is the method of choice to diag-nose pyloric stenosis. Its sensitivityand specificity approaches 100% whenthe pyloric muscle is seen directly. Apyloric muscle thickness of greaterthan 3 mm is considered positive(Fig. 1), although transient pyloro-spasm may provide false-positive re-sults. False-negative results also mayoccur due to an overfilled stomach*University of Alabama, Birmingham, Ala.
focus on diagnosis
506 Pediatrics in Review Vol.31 No.12 December 2010
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from

obscuring the antrum, an inexperi-enced operator, or a child presentingearly in the disease process. (5)
US in older infants and children isuseful in diagnosing intussusception,appendicitis, ovarian torsion, andcholelithiasis. It is 100% sensitive and88% specific for diagnosing intussus-ception. (6) A hypoechoic thick rimencasing a hyperechoic central core isseen on the transverse section and isthe classic “doughnut sign” (Fig. 2).The “sandwich sign” appears on thelongitudinal section and is tubularwith a hyperechoic lumen and a sur-rounding hypoechoic layer. Both ofthese findings on US are diagnosticfor intussusception. (7) Additionalevaluation and treatment continueswith an air contrast enema.
The accuracy of diagnosing acuteappendicitis with US varies substan-tially, depending on the technique ofthe ultrasonographer. In children, thesensitivity ranges from 44% to 94%,with the specificity between 47% and95%. (2)(6)(8)(9)(10) Centers expe-rienced in US achieve a sensitivityand specificity of greater than 90%.(11) Demonstrating a noncompress-ible, aperistaltic, blind-ending tubu-lar structure arising from the cecumon US is diagnostic of acute appen-dicitis (Fig. 3). Additional criteriainclude the presence of an appendi-colith; periappendiceal fluid; an ap-pendix that has discrete walls, targetappearance, or a diameter of greaterthan 6 mm; and pericecal fat strand-ing. (10) The one major limitation of
US is the inability to see the appendixin up to 20% of cases. (11)
US is the diagnostic test of choicefor evaluating pelvic disease. Whenovarian torsion is suspected, an en-larged ovary is the most commonfinding. The ovary usually containsimmature follicles on the peripheryand may have echogenic areas withinthat represent stromal edema or hem-orrhage. A twisted ovarian vascularpedicle viewed on US is very specificfor ovarian torsion. (12) Color Dopp-ler US initially shows decreased orno intraovarian venous flow and pro-gresses to cessation of intraovarianarterial flow when there is a completetorsion.
Finally, cholelithiasis can be diag-nosed with the assistance of US. Thismodality allows for localizing stones,evaluating the gallbladder wall foredema and thickening, and identi-fying sludge. (13) A Murphy signalso can be elicited with the trans-ducer. Optimal gallbladder examina-tions have a sensitivity and specificityof greater than 95% for diagnosingcholelithiasis.
In pediatric trauma, the focused as-sessment with sonography for trauma(FAST) examination is becomingmore widely accepted. The FASTexamination has a large sensitivityrange of 40% to 93% and specificityof 79% to 100%. The FAST exami-nation is used to detect free abdom-inal fluid that appears anechoic orblack. However, the test should notbe relied on to detect liver or spleniclacerations. Unfortunately, childrenhave a higher incidence of solid or-gan damage in the absence of freefluid, and, therefore, a negative FASTstudy result does not exclude a signif-icant injury. (14)
Overall, US is helpful when eval-uating the liver, biliary tract, pan-creas, mass lesions, pylorus, and smallbowel wall. It is extremely useful indetecting ascites and differentiating
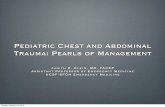
Figure 1. A 4-week-old boy who has had projectile emesis and poor weight gain.Ultrasonography demonstrates a thickened (stars) and elongated pyloric channel,classic findings for pyloric stenosis. Courtesy of Doernbecher Children’s Hospital,Portland, Ore.
focus on diagnosis
Pediatrics in Review Vol.31 No.12 December 2010 507
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from

between solid and cystic structures.However, US is one of the few imag-ing modalities that is critically depen-dent on operator skills for high-quality images. Other limiting factorsinclude large body habitus and thepresence of bowel gas, which reducethe image quality.
Computed Tomography ScanCT scan should be used only afterother imaging modalities, such asUS, have failed to make a definitivediagnosis. CT scan is helpful in rec-ognizing specific disease processes,including nephrolithiasis, appendici-tis, intra-abdominal abscesses, andpancreatitis. CT scan allows for mea-suring and discriminating betweentissue densities, is quick to perform,is operator-independent, and pre-
sents images in various planes. How-ever, CT scanning can be an invasiveprocedure that requires intravenous,oral, rectal, or intravaginal contrast.Other disadvantages are the increasedamount of radiation when comparedwith plain radiography. Children aremore susceptible to radiation becauseof the multiple cells in mitosis andthey probably will have additional CTscans throughout their lifetimes. (2)Also, there is a possible need for se-dation during imaging to decreasemotion artifact. Finally, unlike US,a child’s small size and lack of fatplanes can result in image degrada-tion. (15)
The gold standard imaging mo-dality for diagnosing suspected ap-pendicitis is CT scan. Although dif-ferent scanning techniques may be
used (eg, standard CT with or with-out intravenous and oral contrast ora focused helical appendiceal CTwith or without rectal contrast), thesensitivity, specificity, and accuracyremain greater than 95% for diag-nosing appendicitis in children. Sur-rounding intra-abdominal structuresalso are visible, allowing recognitionof an alternative diagnosis if the ap-pendix appears normal. (10)(11)(16)Key CT scan findings associated withacute appendicitis include an enlargedappendix, a thickened and enhancedappendiceal wall, and periappendicealfat stranding (Fig. 4). CT scan also mayaid in directing percutaneous fluiddrainage if an abscess is present.
A nonenhanced helical CT scan isthe most sensitive test for diagnosingnephrolithiasis. Contrast should beavoided because of its tendency toconceal stones in the collecting sys-tem. CT scan may not only depictcalculi and their location, but also canreveal urinary anomalies and complica-tions of ureteral stones. (17)
CT scanning also can be used todiagnose inflammatory bowel le-sions, abdominal masses, abdominaltrauma, biliary tree or pancreas calci-fications, and splenic cysts. Overall,its use should be limited to problemsthat cannot be detected with less in-vasive methods, such as US.
Magnetic Resonance ImagingMRI is another abdominal imagingmodality that is noninvasive and doesnot use ionizing radiation. MRI usesmagnets and radio waves to createa magnetic field that is more than10,000 times that of the earth. How-ever, it is more costly than otherimaging modalities, and sedation of-ten is required due to the duration ofthe study and the need to decreasemotion artifact.
A wide range of abdominal disor-ders can be evaluated by abdominalMRI, which is optimal for viewing
Figure 2. A 9-month-old girl who has had intermittent episodes of lethargy withemesis. Ultrasonography reveals the “doughnut sign,” commonly seen with intussus-ception. Courtesy of Doernbecher Children’s Hospital, Portland, Ore.
focus on diagnosis
508 Pediatrics in Review Vol.31 No.12 December 2010
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from

the liver and is used to assess hepaticmasses. The pancreas, spleen, andkidney also are fairly visible by ab-dominal MRI. Other uses include
demonstrating cystic structures, suchas a choledochal cyst; detecting in-flammatory lesions; and clarifyingfindings on abdominal radiographs,
US, or CT scan. The bowel is theleast well-seen organ on abdominalMRI because of movement degrada-tion caused by peristalsis. However,MRI of the bowel is indicated inpatients who require multiplefollow-up images and in whom radi-ation exposure is a concern, as inthose who have inflammatory boweldisease. (18) As more studies are per-formed to improve imaging tech-nique, the indications for abdominalMRI will continue to expand.(3)(15)
Nuclear MedicineNuclear medicine techniques areunique because of their ability toprovide both functional and quanti-fiable data. These procedures areused for evaluating biliary disease,gastroesophageal reflux, and Meckeldiverticula.
The primary indication for hepa-tobiliary scintigraphy (hepatic 2,6-dimethyliminodiacetic acid or hepa-toiminodiacetic acid [HIDA] scan)is obstructive jaundice in a neonateor an older child who has cholestaticjaundice. Hepatocytes take up thesubstance labeled with technetium99m, which is injected intravenouslyand excreted into the biliary tract.Gallbladder filling and biliary tractfunctioning can be evaluated. Simi-larly, the radionucleotide in a Meckelscan is absorbed and taken up abnor-mally by the ectopic gastric mucosa.(2) Nuclear medicine modalities canhelp quantify gastroesophageal refluxas well as locate the source of occultblood loss from the gastrointestinaltract. (3)(15)
ConclusionThe first step in evaluating abdomi-nal pain in children is performing ahistory and physical examination.Only after those evaluations shouldimaging be undertaken to assist theclinician with making and confirming
Figure 3. A 15-year-old girl who has had right lower quadrant pain, emesis, and fever.The appendix is unable to be compressed and measures 8 mm in diameter, which is anultrasonographic sign positive for appendicitis. Courtesy of The Children’s Hospital ofAlabama, Birmingham, Ala.
Figure 4. An 11-year-old girl who has acute appendicitis and probably rupture.Computed tomography scan shows focal loss of mucosal enhancement at the tip of theappendix (arrow), concerning for wall discontinuity and rupture. Courtesy of Doern-becher Children’s Hospital, Portland, Ore.
focus on diagnosis
Pediatrics in Review Vol.31 No.12 December 2010 509
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from

a clinical diagnosis. The indicationsfor plain radiographs, US, CT scan,MRI, and nuclear medicine studies inspecific abdominal disorders in thepediatric population are summarizedin the Table. Additional informationmay be found in the resources. Fur-ther investigational uses should helpexpand the knowledge and use ofimaging modalities in the future.
ACKNOWLEDGMENTS. Dr Clay-ton would like to thank Drs DanielYoung and Marjorie Lee White fortheir help.
EDITOR’S NOTE: Dr Clayton wrotethis article while serving as a fellow atThe University of Alabama, Birming-ham, Ala.
References1. Kellow ZS, MacInnes M, Kurzencwg D,et al.The role of abdominal radiography inthe evaluation of the nontrauma emergencypatient. Radiology. 2008;248:887–893
2. Louie JP. Essential diagnosis of ab-dominal emergencies in the first year oflife. Emerg Med Clin North Am. 2007;25:1009–10403. Simon K, Franken E. Gastrointestinalimaging. In: Wyllie R, Hyams J, eds. Pedi-atric Gastrointestinal Disease. Philadelphia,Pa: WB Saunders Co; 1993:1039–10564. Cremin B. Real time ultrasonic evalua-tion of the paediatric abdomen: techniqueand anatomical variations. A personal view.Br J Radiol. 1985;58:859–8685. Hemnanz-Schulman M, Sells L, Am-brosino M, Helter R, Stein S, Neblett W III.Hypertrophic pyloric stenosis in the infantwithout a palpable olive: accuracy of sono-graphic diagnosis. Radiology. 1994;193:771–7766. Miller C. Ultrasound in the assessmentof the acute abdomen in children: its advan-tages and its limitations. Ultrasound Clin.2007;2:525–5407. Verschelden P, Filiatrault D, Garel L,et al. Intussusception in children: reliabilityof US in diagnosis–a prospective study.Radiology. 1992;184:741–7448. Vignault F, Filiatrault D, Brandt M,Garel L, Grignon A, Ouimet A. Acute ap-pendicitis in children: evaluation with US.Radiology. 1990;176:501–504
9. Garcia Pena BM, Mandl KD, Kraus SJ,et al. US and limited computed tomographyin the diagnosis and management of ap-pendicitis in children. JAMA. 1999;282:1041–104610. Sivit CJ, Siegel MJ, Applegate KE,Newman KD. When appendicitis is sus-pected in children. Radiographics. 2001;21:247–26211. Aiken JJ, Oldham K. Acute appen-dicitis. In: Kliegman RM, Behrman RE,Jenson HB, Stanton BM, eds. NelsonTextbook of Pediatrics. 18th ed. Philadel-phia, PA: Saunders Elsevier; 2007:1628–163412. Lee EJ, Kwon HC, Joo HJ, Suh JH,Fleischer AC. Diagnosis of ovarian torsionwith color Doppler sonography: depictionof twisted vascular pedicle. J UltrasoundMed. 1998;17:83–8913. Greenberg M, Kangarloo H, Coch-ran S, Fred W. The ultrasonographicdiagnosis of cholecystitis and cholelith-iasis in children. Radiology. 1980;137:745–74914. Levy JA, Noble VE. Bedside ultra-sound in pediatric emergency medicine.Pediatrics. 2008;121:1404–141215. Stringer DA, Nadel H. Techniquesfor investigation of the pediatric gastro-intestinal tract. In: Stringer DA, BabynPS, eds. Pediatric Gastrointestional Imag-ing and Intervention. 2nd ed. Hamilton,Ontario, Canada: BC Decker Inc; 2000:15–5316. Leite NP, Pereira JM, Cunha R, PintoP, Sirlin C. CT evaluation of appendicitisand its complications: imaging techniquesand key diagnostic findings. AJR Am JRoentgenol. 2005;185:406–41717. Elder JS. Urinary lithiasis. In: KliegmanRM, Behrman RE, Jenson HB, StantonBM, eds. Nelson Textbook of Pediatrics. 18thed. Philadelphia, PA: Saunders Elsevier;2007:2267–227218. Fidler JL, Guimaraes L, Einstein DM.MR imaging of the small bowel. Radio-graphics. 2009;29:1811–1825
Table. Comparison of Imaging Modalities inGastrointestinal Disease
Disease Determining the Diagnosis
Intussusception Left lateral decubitus radiographs USAppendicitis US CTGall Bladder/Biliary Disorders USOvarian Torsion USNephrolithiasis Nonenhanced CTPyloric Stenosis US UGIPancreatitis CTUncertain of Diagnosis CT
CT!computed tomography scan, US!ultrasonography, UGI!upper gastrointestinal radiographicseries
HealthyChildren.org Parent Resources from AAP
Imaging Testshttp://www.healthychildren.org/English/health-issues/conditions/treatments/Pages/Imaging-Tests.aspx
focus on diagnosis
510 Pediatrics in Review Vol.31 No.12 December 2010
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from

DOI: 10.1542/pir.31-12-5062010;31;506Pediatrics in Review
Kelly M. ClaytonFocus on Diagnosis : Pediatric Abdominal Imaging
ServicesUpdated Information &
http://pedsinreview.aappublications.org/content/31/12/506including high resolution figures, can be found at:
References
Lhttp://pedsinreview.aappublications.org/content/31/12/506#BIBat: This article cites 14 articles, 11 of which you can access for free
Subspecialty Collections
stinal_disordershttp://pedsinreview.aappublications.org/cgi/collection/gastrointeGastrointestinal Disordersfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
/site/misc/Permissions.xhtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by Rachel Boykan on November 9, 2011http://pedsinreview.aappublications.org/Downloaded from