(Fluoro)quinolones - University of...
15
(Fluoro)quinolones • Quinolones were originally brought to market in the 1960’s • Gram- only • Short half-lives • Poor tissue penetration • Currently used only for Gram- UTI (renal clearance) Nalidixic acid Fluoroquinolones • Came into use in the 1980’s. • Widely used: oral and parenteral. • Increasing resistance due to widespread use. • Early generations (e.g. Naladixic acid) had exclusively Gram- spectra of activity, newer generations extend to cover Pseudomonas and some Gram+ Nalidixic acid Ciprofloxacin Moxifloxacin Levofloxacin Gemifloxacin
Transcript of (Fluoro)quinolones - University of...
(Fluoro)quinolones
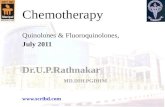
•Quinolones were originally brought to market in the 1960’s
•Gram- only• Short half-lives
• Poor tissue penetration
• Currently used only for Gram- UTI (renal clearance)
Nalidixic acid
Fluoroquinolones
•Came into use in the 1980’s.• Widely used: oral and parenteral.
• Increasing resistance due to widespread use.
•Early generations (e.g. Naladixic acid) had exclusively Gram- spectra of activity, newer generations extend to cover Pseudomonas and some Gram+
Nalidixic acid
Ciprofloxacin
Moxifloxacin
Levofloxacin
Gemifloxacin
•Disrupts bacterial DNA replication
• Bactericidal
• Concentration-dependent killing: increasing concentrations increases rate and extent of bacterial death (AUC/MIC)• Similar to aminoglycosides, for some FQ, can opt for a single, high concentration dose
vs multiple
• Strong post-antibiotic effect (PAE):• Persistent inhibition of bacterial growth even after systemic drug is cleared
• PAE gets stronger for higher concentrations, up to a point
•A number of newer fluoroquinolones have been withdrawn due to toxicities• Grepafloxacin: cardiac events• Trovafloxacin: hepatotoxicity• Gatifloxacin: hypo and hyperglycemia
•Well-absorbed, highly bioavailable through oral administration, good tissue penetration
•Not generally used in children or pregnant women due to adverse effects
Fluoroquinolone properties
MOA: Fluoroquinolones target DNA replication
•During DNA replication, helicases and DNA polymerase introduce supercoiling into DNA. Gyrase, a topoisomerase, and the target for FQ’s, relieves that strain, allowing replication to proceed.
• Topoisomerases II, “gyrase”, primary target in Gram-: responsible for relieving supercoiling
• Topoisomerase IV primary target in Gram+: responsible for separation of interlinked, replicated chromosomes during cell division. “Gyrase” is a secondary target.
•Fluoroquinolones bind to the topoisomerase/DNA complexes and inhibit the enzyme’s function. They stabilize the DNA/topisomerase complex, leading to damaged DNA. Leads to cell death.
•Some evidence that FQ also act on mammalian enzymes, possibly resulting in observed adverse effects

Spectrum of activity•Gram- aerobes:
•Broad coverage of most Gram- aerobes:• E.g. Haemophlius spp., M. catarrhalis, Neisseria spp.
•Including Pseudomonas, at least later generation FQs, cipro-, (levo-, moxi-)
•Enterobacteriaceae:• Klebsiella, Proteus, Enterobacter, Serratia, Providencia...
• Moxi- may exhibit somewhat lower activity against some of these
•Gram+ aerobes: later generation
•Organisms vary in sensitivity
•Newer generations cover Streptococcus, including PRSP
•Staphylococcus: MSSA sensitive, but MRSA not sensitive
•Anaerobes: only Moxifloxacin
•Atypicals:•M. tuberculosis
•But activity against MAC poor
•Mycoplasma pneumoniae
•Chlamydia
Uses
•UTI:
•Especially for complicated UTI involving Klebsiella, Providencia, Pseudomonas, Proteus, etc. I.e. most of the likely pathogens for UTI.
•Gut infections:•Good coverage of Salmonella, Shigella, E. coli
•But since Ciprofloxacin and Levofloxacin are not active against anaerobes, the gut anaerobic flora is not perturbed as much. (Moxifloxacin is active against anaerobes)
•Respiratory infections:•S. pneumoniae, H. influenzae, M. catarrhalis
•Pseudomonas for cystic fibrosis patients
•Osteomyelitis: good bone penetration
•Complicated multi-Gram- infections exhibiting beta-lactam resistance
•STDs:•N. gonorrhoeae: increasing resistance, and azithromycin (single dose) preferable
•Chlamydia
Resistance•Increasingly a problem due to widespread use (humans and agriculture)
•A class effect: evolve resistance to one FQ, and the others also are inactive
•A function of duration and intensity of bacterial exposure to drug: the longer and more intense, the more likely resistance emerges
•Mutations in targets (chromosomally encoded topoisomerase genes) prevent FQ activity
•Plasmid-encoded protection proteins
•Observed in Enterobacteriaciae
•Alone, fairly low-level resistance
•These plasmids frequently encode R-factors for multiple classes of drugs
•Efflux pumps
•Still fairly rare
•Enzymatic modification of the drug
•An aminoglycoside acetyltransferase gained the ability to inactivate fluoroquinolones.
Resistance
•Examples:
•Staph. and Pseudomonas are particularly problematic
•N. gonorrhoeae increasing
•S. pneumoniae resistance also emerging
•Campylobacter jejuni: traveler’s diarrhea

Resistance
Ciprofloxacin-resistant campylobacteriosis in the UK
The Lancet 2010; 376:1987 (DOI:10.1016/S0140-6736(10)62261-1)
Resistance
source: CDC
Gonococcal Isolate Surveillance Project (GISP)—Percent of Neisseria gonorrhoeae isolates
with resistance or intermediate resistance to ciprofloxacin, 1990–2008
NOTE: Resistant isolates have ciprofloxacin MICs !1 "g/ml. Isolates with intermediate resistance have ciprofloxacin MICs of 0.125–0.5 "g/ml. Susceptibility to ciprofloxacin was first measured in GISP in 1990.
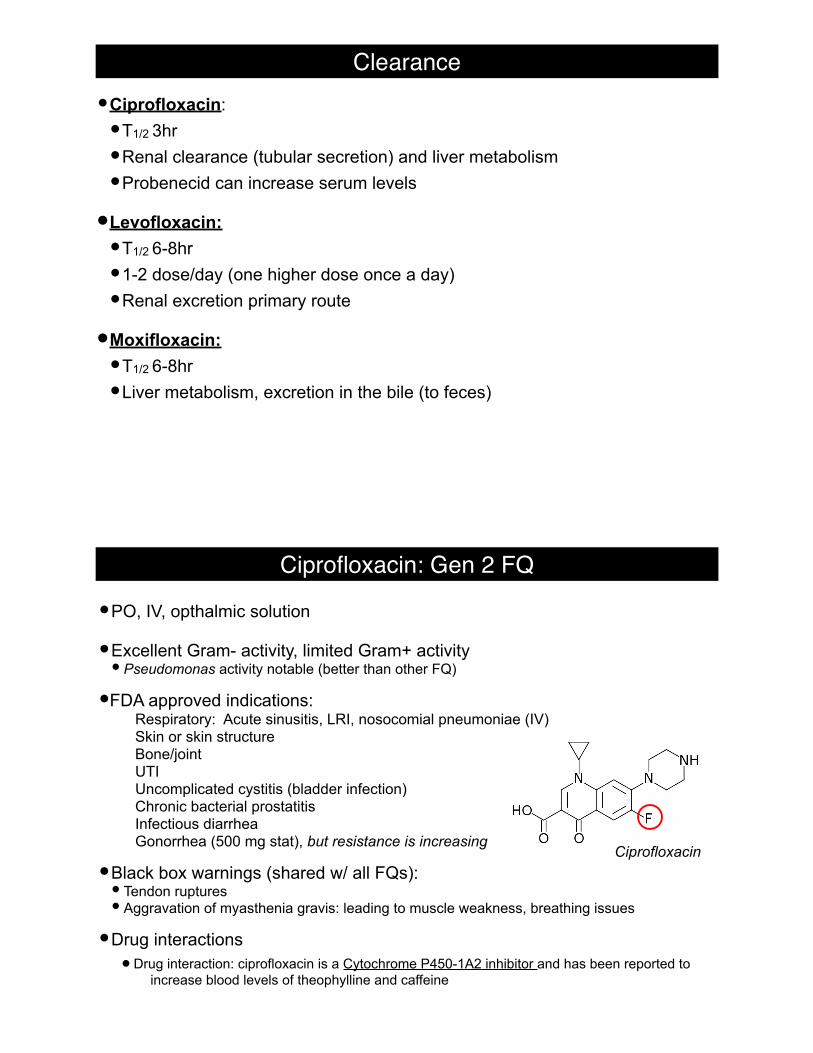
•Ciprofloxacin:
•T1/2 3hr
•Renal clearance (tubular secretion) and liver metabolism
•Probenecid can increase serum levels
•Levofloxacin:
•T1/2 6-8hr
•1-2 dose/day (one higher dose once a day)
•Renal excretion primary route
•Moxifloxacin:
•T1/2 6-8hr
•Liver metabolism, excretion in the bile (to feces)
Clearance
•PO, IV, opthalmic solution
•Excellent Gram- activity, limited Gram+ activity• Pseudomonas activity notable (better than other FQ)
•FDA approved indications: Respiratory: Acute sinusitis, LRI, nosocomial pneumoniae (IV) Skin or skin structure Bone/joint UTI Uncomplicated cystitis (bladder infection) Chronic bacterial prostatitis Infectious diarrhea Gonorrhea (500 mg stat), but resistance is increasing
•Black box warnings (shared w/ all FQs):• Tendon ruptures• Aggravation of myasthenia gravis: leading to muscle weakness, breathing issues
•Drug interactions• Drug interaction: ciprofloxacin is a Cytochrome P450-1A2 inhibitor and has been reported to
increase blood levels of theophylline and caffeine
Ciprofloxacin: Gen 2 FQ
Ciprofloxacin
•PO, IV, opthalmic solution
•Excellent Gram- activity, improved Gram+ activity vs Ciprofloxacin.• S. aureus• S. epidermidis• S. pneumoniae• H. influenzae• Klebsiella spp.•M. catarrhalis• Enterobacter spp.•Mycobacteria• Bacillus anthrasis
•Same compound as ofloxacin, but racemically homogeneous (oflox- has both)
•FDA approved indications (reserved for more serious, life-threating cases):Respiratory: acute sinusitis, acute exacerbation of chronic bronchitis, nosocomial pneumonia,
community acquired pneumoniaComplicated and uncomplicated skin and skin structureComplicated and uncomplicated UTIAcute pyelonephitisProstatitis
•Black box warnings as w/ Cipro.
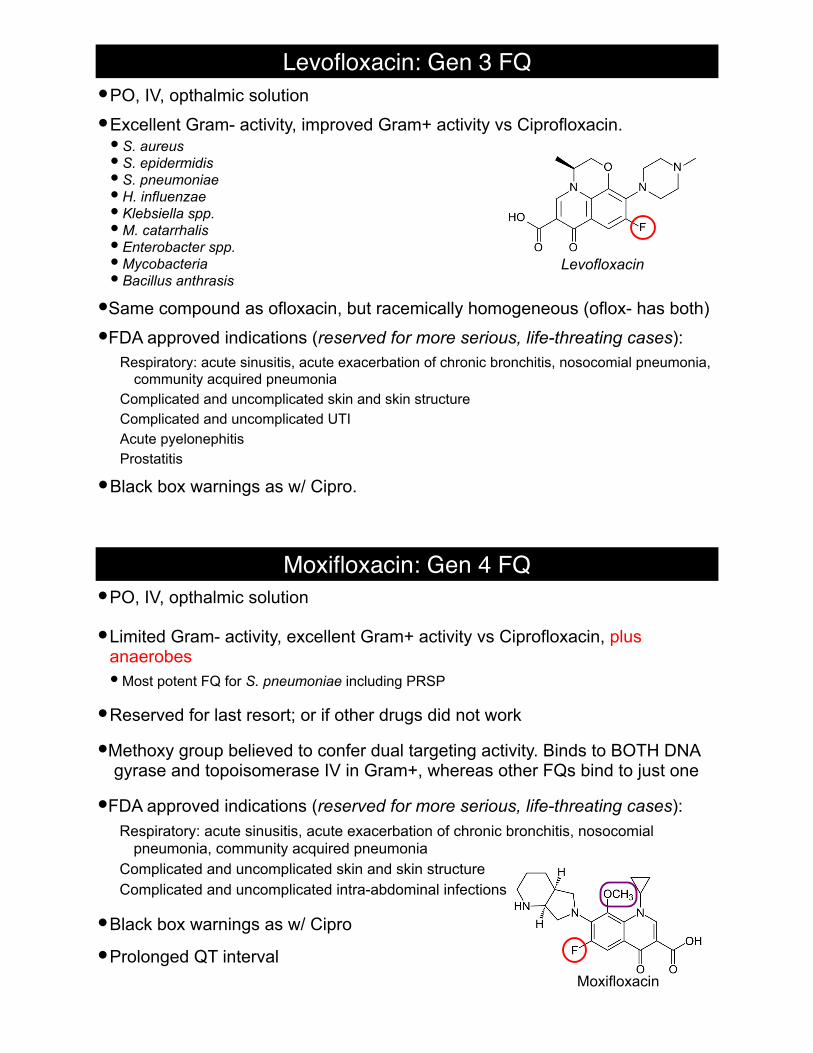
Levofloxacin: Gen 3 FQ
Levofloxacin
•PO, IV, opthalmic solution
•Limited Gram- activity, excellent Gram+ activity vs Ciprofloxacin, plus anaerobes• Most potent FQ for S. pneumoniae including PRSP
•Reserved for last resort; or if other drugs did not work
•Methoxy group believed to confer dual targeting activity. Binds to BOTH DNA gyrase and topoisomerase IV in Gram+, whereas other FQs bind to just one
•FDA approved indications (reserved for more serious, life-threating cases):Respiratory: acute sinusitis, acute exacerbation of chronic bronchitis, nosocomial
pneumonia, community acquired pneumoniaComplicated and uncomplicated skin and skin structureComplicated and uncomplicated intra-abdominal infections
•Black box warnings as w/ Cipro
•Prolonged QT interval
Moxifloxacin: Gen 4 FQ
Moxifloxacin
Fluoroquinolones: Pregnancy and Children
•Generally avoid for pregant women and breast feeding mothers(category C)• Risk not established; concerns over risk of fetal distress, prematurity, spontaneous
abortion
• Passes to fetus through placenta
• Passes to infant through breast milk
•Generally avoid for children < 18 y.o.• Arthropathy (damage to joints) and erosion of cartilage
• Potentially permanent damage
• Exception: FDA approved usage in children for complicated UTA, pyelonephritis
Fluoroquinolones: Adverse Reactions
•Fluoroquinolones form insoluble complexes with divalent cations (aluminum, magnesium, calcium, iron):•Reduced absorption•Avoid taking with dairy, antacid, iron products for 2 hours
•Gastrointestinal (3-17%): nausea, vomiting, discomfort
•0.9-11% headache, dizziness
•Drug interactions:• Ciprofloxacin: inhibition of CP1A2 liver enzyme: leads to caffeine, theophylline elevation• Possible effect with NSAIDs
•Prolonged QT interval• (Sparfloxacin, Grepafloxacin) > Moxifloxacin, Levofloxacin > Ciprofloxacin
Black box warning:• Aggravation of myasthenia gravis: (rare) auto-immune disorder leading to blockage of
signaling at neuromuscular junctions: muscle weakenss, loss of control, breathing difficulties, potentially life threatening (paralysis of respiratory muscles)
• Spontaneous rupture of tendons, tendinopathy: 0.14-0.4% incidence. Higher risk in patients > 60 y.o., or taking glucocorticoids (e.g. prednisone)
•Congenital issues or drugs can lead to “blockage” of cardiac ion currents • Polarization/depolarization of cardiac cells becomes out of register
• This can lead to arrhythmias and ventricular fibrulation
•More of an issue with now off-market FQs (sparfloxacin, grepafloxacin)
Prolonged QT interval
•Widespread usage, especially ciprofloxacin
•Spectrum•Gram- aerobes
• Levofloxacin, Moxifloxacin have more coverage of Gram+
•Ciprofloxacin has better potency against Pseudomonas
•Moxifloxacin covers some anaerobes (similar to penicillins: pip+tazo and amox+clav)
•Disrupts bacterial DNA replication by jamming the topoisomerase (II and IV) enzymes leading to bactericidal effect
•Multiple modes of resistance documented: most common is mutation of the target enzyme to reduce drug binding/activity
•Cautions•Pregant women, and children < 18 y.o.
• FDA boxed warnings: myasthenia gravis aggravation, tendinopathy/rupture
• In some cases, potential for QT interval elongation
Fluoroquinolone summary

Drugs for resistant infections

transpeptidase cannot bind to D-Ala-D-Ala, thus crosslinking does not take place
L-Ala
D-Glu
L-Lys Gly Gly Gly Gly Gly
L-Ala
D-Glu
L-Lys Gly Gly Gly Gly Gly
ONAM NAGO NAM NAGO
D-Ala
D-Ala
D-Ala
D-Ala
Gly
5Gly
5
L-Ala
D-Glu
L-Lys
L-Ala
D-Glu
L-Lys
Gly Gly Gly Gly
L-Ala
D-Glu
L-Lys
L-Ala
D-Glu
L-LysGly
5
ONAM NAGO NAM NAGO
ONAM NAG
ONAM NAG
O
D-Ala
D-Ala
D-Ala
D-Ala
D-Ala
glycopeptide
Glycopeptides: M.O.A.
• Isolated from Actinobacteria Amycolatopsis orientalis in 1957
•Cyclic glycosylated peptide
• Prevents peptidoglycan formation in Gram+
•Bacteria by binding to the D-Ala-D-Ala;
• Inhibits transpeptidase (peptide crosslinking)
• No cross-resistance with beta-lactams
• Bactericidal
• Poor oral absorption, does not penetrate CNS
•Renally cleared, must adjust dose for renal dysfunction
• Synergistic with aminoglycosides
Glycopeptides: Vancomycin
• Indicated uses:• MRSA, S. epidermidis
• E. faecalis (10% resistant), E. faecium (88% resistant)
• Altered terminal dipeptide in peptidoglycan polypeptide (VanA)
• VanB and VanC lead to intermediate resistance
• C. difficile (take orally)
• Resistance is emerging
• Metronidazole alternative treatment
• PRSP
• Endocarditis or other infection by S. pneumoniae
Glycopeptides: Vancomycin
Glycopeptides: Vancomycin
• Older preparations contained more impurities, possibly responsible for reports of nephrotoxicity and ototoxicity; newer contain 85-95% “Factor B”, active drug.
• Adverse effects:
• Must introduce through IV slowly:
• Hypersensitivity (3%)
• Phlebitis (13%)
• Red man/neck syndrome: associated with too rapid infusion (<<60min)
• Nephrotoxicity
• Reversible, also associated with aminoglycoside use. Becomes more problematic as dose is pushed higher (e.g. to overcome intermediate-resistance)
Lipoglycopeptides: Telavancin
DL Higgins, et al., Antimicrob. Agents Chemo. (2005) 49: 1127
•Vibativ® (Theravance) FDA approved 2009•Blocks cell wall synthesis (like vanco) and induces membrane
depolarization• More potent than vancomycin
•Complicated skin and skin structure infections• MRSA
•Adverse effects:• Greater frequency of nephrotoxicity than w/ vancomycin (15% vs 7%)
• QT prolongation
•Cubicin® (Cubist)
• From Streptomyces roseosporus
• Treat Gram+ infections: complicated skin/skin structure infections, bacteremia
• MRSA
• Enterococcus faecalis and faecium
• Streptococcus pyogenes (if pen. allergic)
• NOT for pneumonia; daptomycin binds to pulmonary surfactant, antibiotic activity inhibited
• Depolarizes cellular membrane, shutting down essential functions in the cytoplasm
• Bactericidal
Lipopeptide: Daptomycin
Lipopeptide: Polymixins
Polymyxin E (Colistin)• From Bacillus polymyxa
• Binds to lipopolysaccharide of outer membrane
• Acts like a detergent and destroys membranes
• Bactericidal
• Broad Gram- spectrum• Except N. gonorrhoeae, N. meningitidis• Gram+ resistant
• Indicated uses:• P. aeruginosa• Enterobacteriaceae exhibiting carbapenemase production• E. coli UTI• K. pneumoniae bacteremia• H. influenzae meningitis (intrathecal injection, into the spinal canal)
• Black box warnings about nephrotoxicity and neurotoxicity
Glycylcycline: Tigecycline
• Tygacil® (Wyeth); FDA approved 2005
• A derivative of the tetracycline class of antimicrobials; inhibits protein synthesis
• Bacteriostatic
• Broad spectrum: Gram+ and Gram- coverage
• MRSA
• H. influenzae
• N. gonorrhoeae
• Acinetobacter baumanii
• Enterobacteriaceae bearing NDM-1 are susceptible
• Complicated skin and skin structure infections, intra-abdominal infections
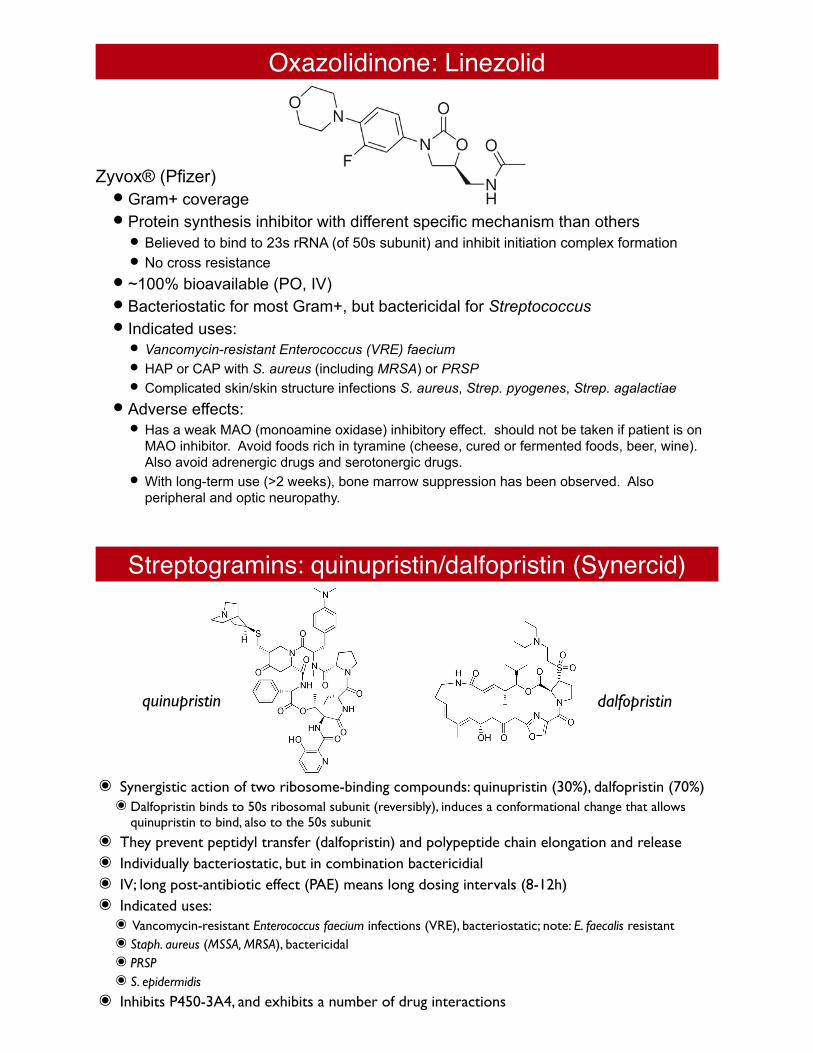
Oxazolidinone: Linezolid
Zyvox® (Pfizer)• Gram+ coverage• Protein synthesis inhibitor with different specific mechanism than others
• Believed to bind to 23s rRNA (of 50s subunit) and inhibit initiation complex formation• No cross resistance
• ~100% bioavailable (PO, IV)• Bacteriostatic for most Gram+, but bactericidal for Streptococcus• Indicated uses:
• Vancomycin-resistant Enterococcus (VRE) faecium
• HAP or CAP with S. aureus (including MRSA) or PRSP
• Complicated skin/skin structure infections S. aureus, Strep. pyogenes, Strep. agalactiae
• Adverse effects:• Has a weak MAO (monoamine oxidase) inhibitory effect. should not be taken if patient is on
MAO inhibitor. Avoid foods rich in tyramine (cheese, cured or fermented foods, beer, wine). Also avoid adrenergic drugs and serotonergic drugs.
• With long-term use (>2 weeks), bone marrow suppression has been observed. Also peripheral and optic neuropathy.
Streptogramins: quinupristin/dalfopristin (Synercid)
๏ Synergistic action of two ribosome-binding compounds: quinupristin (30%), dalfopristin (70%)๏Dalfopristin binds to 50s ribosomal subunit (reversibly), induces a conformational change that allows
quinupristin to bind, also to the 50s subunit๏ They prevent peptidyl transfer (dalfopristin) and polypeptide chain elongation and release๏ Individually bacteriostatic, but in combination bactericidial๏ IV; long post-antibiotic effect (PAE) means long dosing intervals (8-12h)๏ Indicated uses:๏ Vancomycin-resistant Enterococcus faecium infections (VRE), bacteriostatic; note: E. faecalis resistant๏ Staph. aureus (MSSA, MRSA), bactericidal๏ PRSP๏ S. epidermidis
๏ Inhibits P450-3A4, and exhibits a number of drug interactions
quinupristin dalfopristin