Fluid therapy
67
FLUID THERAPY MODERATOR : PROF. ANITA MALIK PRESENTED BY: DR. SWAPNIL DR. KANIKA DR. AJAY KR YADAV
-
Upload
kanika-rustagi -
Category
Health & Medicine
-
view
157 -
download
3
Transcript of Fluid therapy

FLUID THERAPY
MODERATOR : PROF. ANITA MALIKPRESENTED BY:
DR. SWAPNILDR. KANIKA
DR. AJAY KR YADAV

Body Fluid Compartments:
ICF:55%~75%
Intravascularplasma
ExtravascularInterstitial
fluidECF
3/4
1/4
• TBW=X 50-70% lean body weight• ICF=0.4xBW• ECF=0.2xBW TBW affected by:• Age : decreases with increasing age.• Sex: females<males• Body composition: adipose tissue .
2/3
1/3

ECF subdivided into:• Interstitial fluid : lymphatic fluid and protein poor fluid
occupying cellular spaces.• Intravascular fluid: plasma & fluid in subglycocalyx.• Transcellular fluid: GI Tract, CSF, bile, urine, aqueous
humor, pleural peritoneal, pericardial fluid.• Water in bone and dense connective tissue. These compartments vary in size & composition.

Composition of GI Secretions:
Source Volume (ml/24h) Na+* K+ Cl- HCO3
-
Salivary 1500 (500~2000) 10 (2~10) 26
(20~30) 10 (8~18) 30
Stomach 1500 (100~4000) 60 (9~116) 10
(0~32)130 (8~154) 0
Duodenum 100~2000 140 5 80 0
Ileum 3000 140 (80~150) 5 (2~8) 104
(43~137) 30
Colon 100-9000 60 30 40 0
Pancreas 100-800 140 (113~185) 5 (3~7) 75 (54~95) 115
Bile 50-800 145 (131~164) 5 (3~12) 100
(89~180) 35* Average concentration: mmol/L

Composition of Body Fluids:
Ca 2+
Mg 2+
K+
Na+
Cl-
PO43-
Organic anion
HCO3-
Protein
0
50
50
100
150
100
150
Cations Anions
EC
FICF
Units : meq/l

PHYSICOCHEMICAL LAWS FOR FLUID MOVEMENT
• DIFFUSION: movement of solute particles along concentration gradient.
• OSMOSIS: movement of solvent across a semipermeable membrane into regions of higher solute concentration.
Osmolarity = solute/(solute+solvent) (normal 280-310mosm/L)

OSMOLALITY: = solute/solvent (285-290mosm/kg)Plasma osmolality= 2x(Na) + (Glucose/18) + (Urea/2.8)
•TONICITY: effective osmolality with respect to a semipermeable membrane.Plasma tonicity = 2 x (Na) + (Glucose/18)Important in determining distribution of fluids across a cell membrane and sensed by hypothalamic osmoreceptors.
•ONCOTIC PRESSURE

Regulation of Fluids:
Renal sympathetic nerves
Renin-angiotensin-
aldosterone system
Atrial natriuretic peptide (ANP)

COLLOIDS
• Fluids containing molecules sufficiently large enough to prevent transfer across capillary membranes.
• Solutions stay in the space into which they are infused.
• SEMISYNTHETIC COLLOID:– GELATINS– HYDROXYETHYL STARCHES– DEXTRANS
• HUMAN PLASMA DERIVATIVES

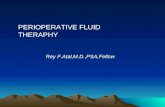
CRYSTALLOIDS• Combination of water and
electrolytes- Balanced salt solution:
electrolyte composition and osmolality similar to plasma; example: lactated Ringer’s, Plasmlyte.
- Hypotonic salt solution: electrolyte composition lower than that of plasma; example:D5W
- Hypertonic salt solution: 2.7% NaCl.
- Dextrose containing fluids



PATHOPHYSIOLOGIC FLUID ALTERATION IN PERIOPERATIVE PHASE
• PREOPERATIVE:– DIRECT INTRAVASCULAR DEPLETION– LOSS FROM GI TRACT– INFLAMMATION RELATED REDISTRIBUTION– FLUID SEQUESTRATION IN THIRD SPACE LOSSES
• INTRAOPERATIVE:– ALTERED DISTRIBUTION OF INTRAVASCULAR VOLUME.– DIRECT LOSS OF INTRAVASCULAR VOLUME.– INSENSIBLE LOSSES.

– INFLAMMATION RELATED REDISTRIBUTION.– RENAL OUTPUT
• POSTOPERATIVE :– INFLAMMATION AND IMMUNE RESPONSE (IL1,
TNF ALPHA, IL6, SIRS)– CATABOLIC METABOLISM– REGULATION OF SALT AND WATER BALANCE WITH
ADH RELEASE

PRACTICAL MANAGEMENT OF FLUID THERAPY
• QUANTITY OF FLUID :– TARGETTING OVERALL FLUID BALANCE– GOAL DIRECTED THERAPY: based on
measurements as follows• pulmonary arterial catheter,• esophageal doppler monitoring and• other targets like arterial waveform analysis, cvp,
lactate, echocardiography, oxygen extraction &venous saturation or central venous saturation etc.

Clinical Evaluation of Fluid Replacement
1. Urine Output: at least 1.0 ml/kg/hr2. Vital Signs: BP and HR normal.3. Physical Assessment: Skin and mucous membranes
no dry; no thirst in an awake patient.. Laboratory tests: periodic monitoring of hemoglobin
and hematocrit.

Perioperative Fluid Requirements
The following factors must be taken into account:
1- Maintenance fluid requirements2- NPO and other deficits: NG suction, bowel
prep3- Third space losses4- Replacement of blood loss5- Special additional losses: diarrhea

1- Maintenance Fluid Requirements
• “4-2-1 Rule” HOLIDAY SEGAR FORMULA- 4 ml/kg/hr for the first 10 kg of body weight- 2 ml/kg/hr for the second 10 kg body weight- 1 ml/kg/hr subsequent kg body weight- Extra fluid for fever, tracheotomy, denuded surfaces

2- NPO and other deficits
• NPO deficit = number of hours NPO x maintenance fluid requirement.
• Bowel prep may result in up to 1 L fluid loss.• Measurable fluid losses, e.g. NG suctioning,
vomiting, ostomy output, biliary fistula and tube.

3- Third Space Losses• Isotonic transfer of ECF from functional body fluid
compartments to non-functional compartments.• Depends on location and duration of surgical
procedure, amount of tissue trauma, ambient temperature, room ventilation• Superficial surgical trauma: 1-2 ml/kg/hr• Minimal Surgical Trauma: 3-4 ml/kg/hr
- head and neck, hernia, knee surgery• Moderate Surgical Trauma: 5-6 ml/kg/hr
- hysterectomy, chest surgery• Severe surgical trauma: 8-10 ml/kg/hr (or more)
- Nehprectomy

Blood Loss
• Replace 3 cc of crystalloid solution per cc of blood loss (crystalloid solutions leave the intravascular space)
• When using blood products or colloids replace blood loss volume per volume

SPECIAL CONSIDERATION
• PAEDIATRIC:– Modification in preoperative fasting ( allowing
carbohydrate containing fluids upto 2 hours).– Glucose free balanced crystalloid solutions to be
used intraoperatively. – Avoid hypotonic fluids.– Maintenance fluid using ½ to 2/3 of calculated 4-2-
1 formula– Return to oral fluids as soon as possible.– Maintenance and ongoing losses to be replaced
seperately.

GERIATRIC:
• Decrease in total body water • Decrease in GFR • Decrease in urinary concentrating ability • Increase in antidiuretic hormone (ADH) • Increase in atrial natriuretic peptide (ANP) • Decrease in aldosterone • Decrease in thirst mechanism • Decrease in free-water clearance

– The British Consensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patients (GIFTASUP) for fluid management recommends that “when crystalloid resuscitation or replacement is indicated balanced salt solution Ringer’s lactate/acetate or Hartmann’s solution should replace 0.9% normal saline, except in cases of hypochloremia for example from vomiting or gastric drainage.”
– If colloids are indicated and used, lower-molecular-weight colloids that can maintain adequate oncotic pressure should be considered.

NEUROSURGERY PATIENTS :
Goals : – maintaining baseline blood volume and cerebral
perfusion– avoid significant decrease in serum sodium and
osmolality and oncotic pressure.• Situations requiring specific management:– Raised ICP- increasing serum osmolarity with
mannitol, hypertonic saline.– Cerebral vasospasm – triple H( hypervolemia,
hemodilution, hypertension).– Intacranial pathologic condition associated with
cerebral salt wasting, diabetes insipidus, SIADH.

• ORGAN FAILURE:– HEART FAILURE: goals –• Preserve cardiac output with limited preload.• Minimise cardiac work . Avoid hypovolemia.• Optimisation of electrolyte and fluid disturbances.
– Renal failure:• Avoid both hypo- and hypervolemia.• Dialysis day before surgery for euvolemia.• Avoid large boluses of isotonic saline.• Fluids available- potassium free HCO3- buffered dialysis
solution>potassium containing balanced crystalloids.• Colloids- volume effect and potential toxicities
exaggerated.
– HEPATIC FAILURERELATIVE intravascular volume depletion with salt and water
retention.– Careful assesement of volume status along with cardiac
output monitoring.– Replace losses with isotonic crystalloids, colloids or blood.– Avoid salt and water retention due to excessive volumes of
saline. – Metabolism of lactates and other buffered solutions is
slowed.– Hypertonic saline may be used in hepatic encephalopathy.

SEPSIS AND ACUTE LUNG INJURY
• INITIAL RESUSCITATION (<6 HRS) with targets-– CVP8-12 mm hg– MAP >65 mm hg– u/o >0.5 ml/kg/hr– Scvo2 >70% or mixed venous o2 saturation> 65%.
• Prefer crystalloids over colloids.

TRAUMA:
– APPROACH- permissive hypovolemia with fluids targetted to achieve cerebration rather than normotension.
– Early replacement with blood and blood products.– After Clot stabilisation, now restore normal circulating
volume and tissue perfusion.

• BURNS : – I.V. FLUIDSinstituted for burns >15% BSA(adults), >10%
BSA( children)– Prefer crystalloids over colloids.– Based on PARKLAND FORMULA: • 1ST 8hrs- 2ml/kg * % TBSA( RL )• Next 16hrs - 2ml/kg * % TBSA( RL)• Next 24 hrs – 0.8ml/kg %TBSA (5%DEXTROSE) +
0.015ML/KG *%TBSA ( 5% ALBUMIN)

OBSTETRICS; PREECLAMPSIA• Reduced plasma volume in contrast to volume
expansion as in normal pregnancy.• Hypoalbuminemia and endothelial dysfunction.• Management– Restricted volume of crystalloid including drug
diluents.– Blood loss in peripartum or perioperative period to be
replaced with appropriate volumes of blood, colloids & crystalloids.
– Invasive monitoring required.– Oliguria in presence of normal renal function not to
be treated with fluid boluses.

UPPER GI LOSS
• Fluid and electrolyte abnormalities: dehydration, hypochloremic metabolic alkalosis with paradoxically acid urine and hypocalcaemia.
• Correction: gradual rehydration with normal saline and potassium supplementation.
• Surgery to treat gastric outlet obstruction to be scheduled after correction of acid base status.

References
• Miller’s anesthesia 8th edition. MARK R. EDWARDS, MICHEAL P. W. GROCOTT
• Lippincott’s ANESTHESIA REVIEW2015; PAUL SIKKA .
• British Consensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patients GIFTASUP 2011 REVISED
• SITES http://ceaccp.oxfordjournals.org/content• http://www.ncbi.nlm.nih.gov/pubmed/19302633

1. All of the following are signs of dehydration except:
A. Progressive metabolic acidosis.B. Urinary specific gravity >1.010C. Urine osmolality <300mOsm/kgD. Urine sodium <10 meq/l

C. When dehydrated, patients with normal renal function will retain sodium and produce a concentrated urine. Urine osmolality is typically greater than 450 mOsm/kg in this setting. Urine sodium will be low, and specific gravity will be high.

2. Regarding central venous pressure monitoring:A. Low values of <5mm hg may be considered normal
in the absence of other signs of hypovolemia.B. CVP readings can be interpretated independently
of clinical setting.C. CVP monitoring is never indicated in patients with
normal cardiac & pulmonary function.D. In a patient with right ventricular dysfunction, a
CVP of 10 mm hg should be considered elevated.

• A. CVP measurements must be evaluated in context of the clinical setting. Factors such as underlying cardiopulmonary disease, patient position, and anatomy can affect the values. A CVP of <5 mm Hg can be normal in a healthy patient without signs of hypovolemia. For surgical cases during which large fluid shifts are expected, placement of a CVP monitor may be indicated. Patients with compromised right ventricular function generally have high CVPs, and thus, a CVP of 10 mm Hg should be considered normal to low depending on the degree of dysfunction.

3. In healthy patients, the lactate in lactated ringer solution:
1. Causes lactic acidosis.2. Is converted to bicarbonate by the liver.3. Is rapidly bound by albumin.4. Causes a hyperchloremic metabolic acidosis.

B. In healthy patients the lactate in lactated Ringers solution is rapidly converted to bicarbonate by the liver and does not cause a lactic acidosis. Administration of a large volume of normal saline can cause a hyperchloremic metabolic acidosis. Lactate is not bound by albumin.

4. All of the following fluids are generally considered to be isotonic except:
1. Lactated ringer solution2. Normal saline3. D5 normal saline4. D5+1/4normal saline

• C. An intravenous solution’s effect on fluid movement depends in part on its tonicity. This term is sometimes used interchangeably with osmolarity, although they are subtly different. Osmolarity is the number of osmoles or moles of solute per liter of solution. Tonicity is the effective osmolality and is equal to the sum of the concentrations of the solutes which have the capacity to exert an osmotic force across the membrane. A solution is isotonic if its tonicity falls within (or near) the normal range for blood serum—from 275 to 295 mOsm/kg. A hypotonic solution has lower osmolarity (<250), and a hypertonic solution has higher osmolarity (>350).

5. All of the following statements regarding dextran solution are true except:
A. Dextran 40 may improve blood flow through microcirculation.
B. Dextrans may have antiplatelet effect.C. Large volume infusion of dextrans have been
associated with renal failure.D. Dextran 40 is better volume expander.

D. While dextran 40 has a molecular weight of 40,000, dextran 70 has a molecular weight of 70,000, and therefore, the latter is broken down more slowly, lasts longer, and is a better volume expander. Dextran 40 appears to improve blood flow through the microcirculation, and all dextrans may have antiplatelet effects. Infusion of large volume of dextran (>20 mL/kg/day) has been associated with renal failure.

6. Which of the following statement is true regarding fluid loss:
A. Substantial evaporative losses can be associated with large wounds & are directly proportionated with surface area exposed.
B. Internal redistribution of fluids ,”third spacing” cannot cause massive fluid shifts.
C. Traumatised inflammed or infected tissues can only sequester minimal amount of fluid in interstitial space
D. Cellular dysfunction as a result of hypoxia usually produces a decrease in intracellular fluid volume

A. Substantial evaporative losses can be associated with large wounds and are directly proportionate to the surface area exposed. Third spacing can cause massive fluid shifts, and traumatized, inflamed, or infected tissue can sequester large amounts of fluid. Cellular dysfunction as a result of hypoxia usually produces an increase in intracellular fluid volume.

7. All of the following are advantages of crystalloid solution except:
A. NontoxicB. Reaction freeC. Relatively inexpensiveD. Ability to remain in intravascular space

D. Advantages of crystalloid solutions are that they are nontoxic, reaction-free, and inexpensive. Colloid solutions are composed of large-molecular-weight substances that remain in the intravascular space longer than crystalloids, and typically, the initial volume of distribution is equivalent to the plasma volume. The synthetic colloids and processed albumin have minimal or no risks of infection. Colloids are more expensive than crystalloids, but have fewer risks than blood products.

8. Administration of large volumes of saline can lead to:
A. Metabolic acidosisB. Hyperchloremic induced nongap metabolic
acidosisC. Anion gap metabolic lactic acidosisD. None of the above.

B.Normal saline (0.9% NaCl) is slightly hypertonic and contains more chloride than extracellular fluid. Administration of large volumes of normal saline solution can lead to a hyperchloremic non–anion gap metabolic acidosis. Administration of large amounts of lactated Ringer solution may result in a metabolic alkalosis because of increased bicarbonate production from the metabolism of lactate.

9. All of the following contains potassium except:
A. Lactated ringer solutionB. Plasmalyte C. HespanD. Packed RBCs

C. Hespan is colloid containing starch and saline. All of the other options contain potassium. Many patients with hyperkalemia, including patients with renal failure, routinely receive normal saline because it contains no potassium.

10. All are true for normal saline except :A. Osmolarity higher than plasma.B. Osmolality similar to plasma.C. Isotonic to plasma.D. Slightly alkaline.

11. Maximum tolerated amount of blood loss without any hemodynamic alteration:
A. 20%B. 25%C. 30%D. 35%
12. Parkland fluid resuscitation is for:A. BurnsB. Trauma C. SepsisD. Organ failure

13. Triple H therapy for cerebral vasospasm after subarachnoid hemorrhage include:
A. Hypoxia , Hypervolemia, hemodilutionB. Hypervolemia, hemodilution, hypertension.C. Hypocarbia, hemodilution, hypertension.D. Hypervolemia, hypercarbia, hypotension.

14. Upper GI losses to be replaced with:A. Lactated ringer solution.B. Normal saline.C. Normal saline with K+ supplementation.D. D5+ ½ NS
Dehydration occurs as a result of water loss, reduced total body Cl−content, and alkalosis
caused by proton loss, with raised serum HCO3.Theinitial renal response is formation of urine with low Cl−and high HCO3− content. However, progressive dehydrationleads to increased aldosterone secretion, aimed atretaining Na+ and water. Na+ is retained at the expenseof K+ and H+ ions, leading to hypokalemia, and worseningmetabolic alkalosis with a paradoxically acid urine.The alkalosis also reduces the circulating ionized fractionof Ca2+.

15.Maintenance requirements in postoperative period include all except:
A. 1500-2500 ml in 24 hrs or 1 to 1.2 ml/kg/hrB. 50–100 meq sodiumC. 40-80 meq potassiumD. 60 meq calcium

16. The following ion concentrations are corrects:
A. 0.9% saline= sodium 131 mmol/LB. Albumin 4.5% =calcium 2mmol/LC. Hartmann’s solution = 154 mmol/LD. gelofuscine = calcium 5.1 mmol/LE. Dextrose 4% Saline 0.18% = sodium 30
mmol/L

17. Concerning the use of hydroxylethyl starch as an intravenous fluid:
A. Glomerular filteration is the major route of eliminationB. About 48% of the total dose is deposited in the
reticuloendothelial system.C. Large volumes may alter coagulation by lowering
factor X concentration.D. Incidence of allergic reactions is similar to that of the
gelatinsE. Serum amylase concentrations may be elevated .
18. Perioperative fluids:A. Should not be given orally within 4 hrs of
anaesthesia.B. Need to replace unmeasured losses of up to 5
mlkg−1 hr−1 during abdominal surgery.C. Are a frequent cause of left ventricular failure and
pulmonary oedema.D. Should be restricted in the first 24 hrs post-op due to
inappropriate ADH secretion.E. Should be included in day of surgery fluid balance.

19. What regulates water homeostasisA. Thirst B. Arginine vasopressinC. KidneysD. All of the above

19. What regulates water homeostasis:A. Thirst [ Fluid homeostasis depends on proper water intake
(regulated by thirst mechanism) and on urinary excretion of free water (regulated by AVP).]
B. Arginine vasopressinC. KidneysD. All of the above [ The serum sodium concentration and thus
serum osmolality are controlled by water homeostasis. Water homeostasis is mediated by thirst, arginine vasopressin, and the kidneys. Abnormal water balance manifests as an abnormality in the serum sodium concentration (hypernatremia or hyponatremia).

20. ECF volume contraction results inA. Hypotension B. Stimulation of baroreceptors C. Stimulation of sympathetic nervous systemD. Stimulation of renin secretionE. All of the above.
ECF volume contraction results inA. Hypotension [ Clinically ECF volume contraction manifest as a
decreased plasma volume and hypotension. Hypotension is due to decreased venous return (preload) and diminished cardiac output.]
B. Stimulation of baroreceptors [ Hypotension stimulates baroreceptors inthe carotid sinus and aortic arch.].
C. Stimulation of sympathetic nervous system[ Hypotension activates the sympathetic nervous system and the renin-angiotensin system.]
D. Stimulation of renin secretionE. All of the above T [ The net effect is to maintain mean arterial
pressure and cerebral and coronary perfusion. In contrast to this cardiovascular response, the renal response attempts to restore the ECF volume.